Prevalence and Risk Factors for Anemia in Non-pregnant Childbearing Women from the Chinese Fifth National Health and Nutrition Survey

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
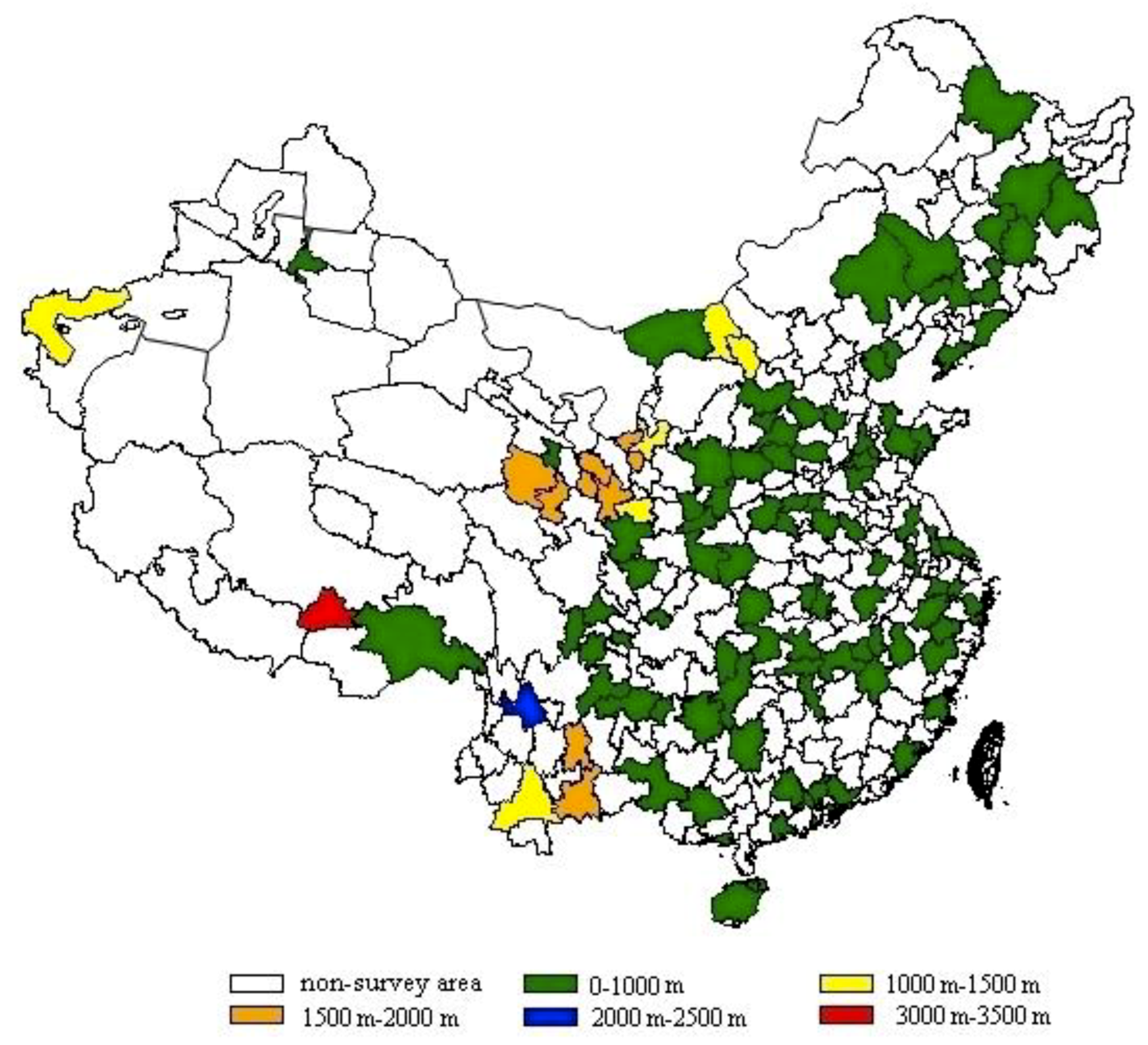
2.1. Subjects and Ethics
2.2. Blood Samples and Hemoglobin Measurement
2.3. Criteria of Anemia
2.4. Variables
2.5. Data Check and Analyses
3. Results
3.1. Participant Characteristics
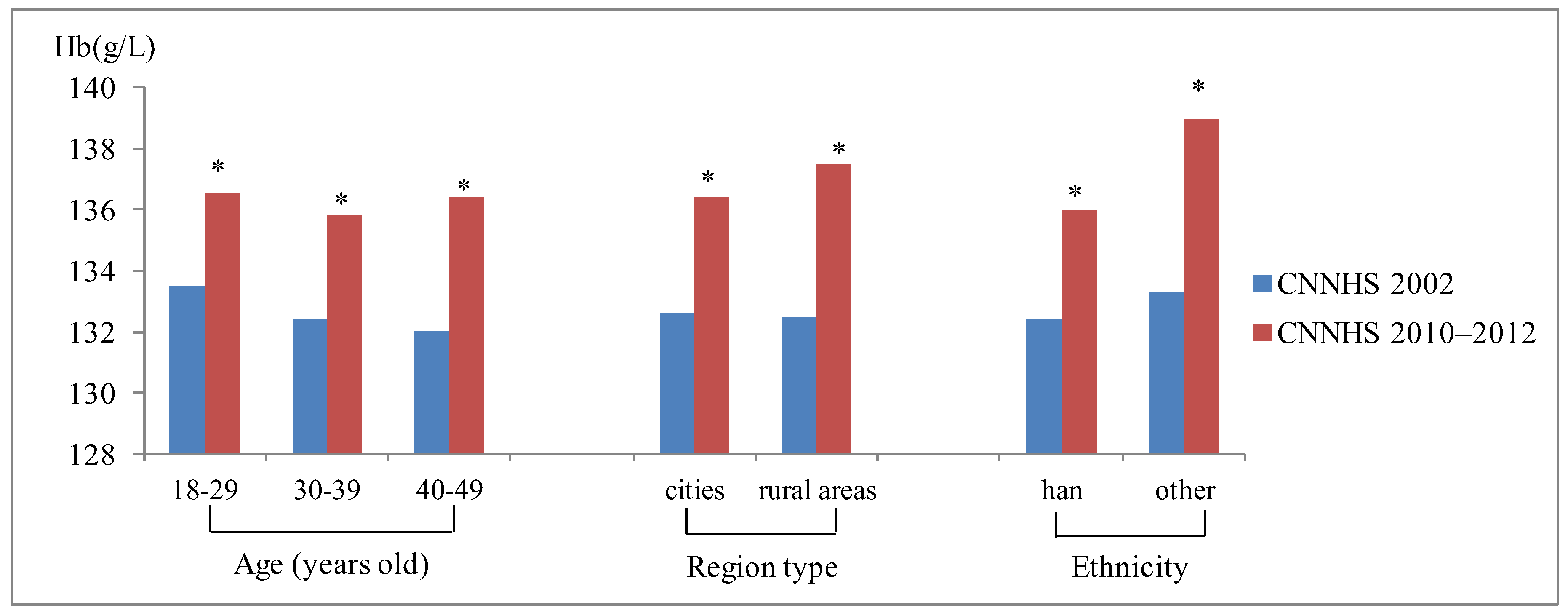
3.2. Blood Hemoglobin of Chinese Childbearing Women
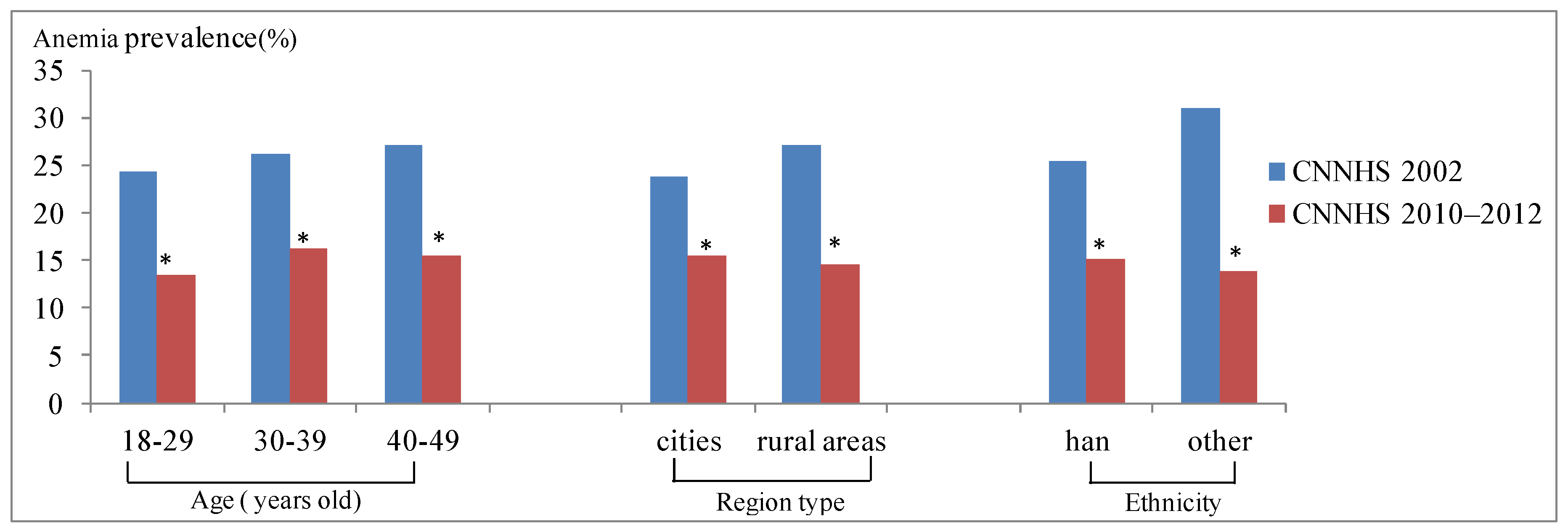
3.3. Anemia Prevalence of Chinese Childbearing Women
3.4. Risk Factors for Anemia in Chinese Childbearing Women
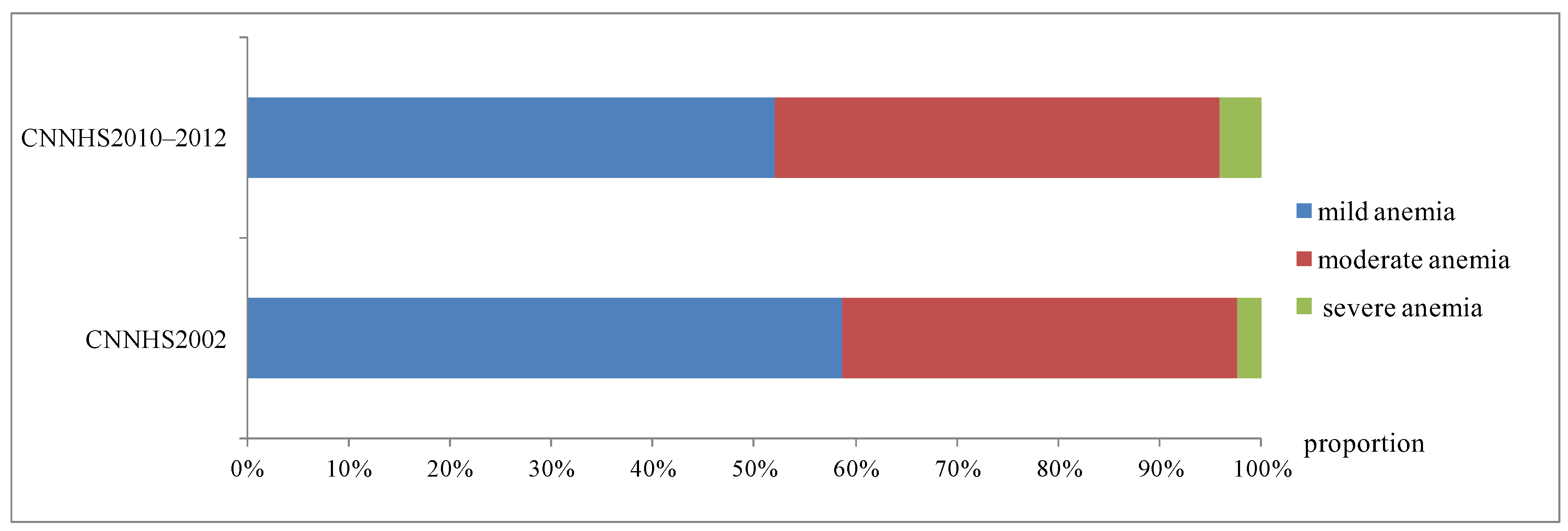
3.5. Comparison of anemia status over ten years
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Data Cleaning Principles
- (1)
- Connect the Hb database to the basic information base. If there was duplicate information, then we reported to the provincial CDC and requested them to submit the data after rechecking the original records.
- (2)
- Check whether the Hb value was in the range of 40–200 g/L, if not we reported to the provincial CDC and requested them to submit the data after rechecking the original records.
- (3)
- Check whether the Hb values of parallel samples were correctly entered by calculating the difference between the Hb values of two parallel samples. If the difference was greater than 20%, we reported to the provincial CDC and requested them to submit the data after rechecking the original records.
- (4)
- Calculate the Hb values based on the standard of the same test batch with the sample. If the difference value between the calculated Hb and the reported Hb was over 10 g/L, we reported to the provincial CDC and requested them to submit the data after rechecking the original records.
References
- World Health Organisation. Iron Deficiency Anaemia: Assessment, Prevention and Control. A Guide for Programme Managers; WHO/NHD/01.3; World Health Organisation: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. The Global Prevalence of Anaemia in 2011; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; John, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014, 123, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Anemia and iron deficiency: effects on pregnancy outcome. Am. J. Clin. Nutr. 2000, 71, S1280–S1284. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. What Is Malnutrition? Available online: http://www.who.int/features/qa/malnutrition/en/ (accessed on 8 July 2016).
- Global Burden of Disease (GBD) 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- Wang, L.D. Report on Nutrition and Health Status of Chinese Residents: Synthesis Report; People’s Medical Publishing House: Beijing, China, 2005; pp. 39–41. ISBN 7-117-06373-4. [Google Scholar]
- Chang, J.L.; Wang, Y. Report on Chinese Residents’ Nutrition and Health Survey; Peking University Medical Press: Beijing, China, 2016; pp. 3–4. ISBN 978-7-5659-1460-7. [Google Scholar]
- Hu, Y.C.; Chen, J.; Wang, R.; Li, M.; Yun, C.F.; Li, W.D.; Yang, Y.H.; Yang, X.G.; Yang, L.C. Vitamin D Nutritional Status and Its Related Factors for Chinese Children and Adolescents in 2010–2012. Nutrients 2017, 9, 1024. [Google Scholar] [CrossRef] [PubMed]
- Zwart, A.; van Assendelft, O.W.; Bull, B.S.; England, J.M.; Lewis, S.M.; Zijlstra, W.G. Recommendations for reference method for haemoglobinmetry in human blood (ISCH standard 1995) and specifications for international haemiglobinocyanide standard (4th edition). J. Clin. Pathol. 1996, 49, 271–274. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Management of Nutrition in Major Emergencies; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.O.; Lee, J.H.; Ahn, S.; Kim, J.W.; Chang, H.; Kim, Y.J.; Lee, K.W.; Kim, J.H.; Bang, S.M.; Lee, J.S. Prevalence and Risk Factors for Iron Defciency Anemia in the Korean Population: Results of the Fifth Korea National Health and Nutrition Examination Survey. J. Korean Med. Sci. 2014, 29, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.; Greene-Finestone, L.; Lowell, H.; Levesque, J.; Robinson, S. Iron Sufficiency of Canadians. Health Rep. 2012, 23, 41–48. [Google Scholar] [PubMed]
- Li, C.H.H. The Prevalence of Anemia and Moderate Severe Anemia in the US Population (NHANES 2003–2012). PLoS ONE 2016, 1, 166635. [Google Scholar] [CrossRef]
- The Central People’s Government of the People’s Republic of China. General Office of the State Council on Printing and Distributing Chinese Food and Nutrition Notification of the Development Programme (2001 to 2010). Available online: http://www.gov.cn/zhengce/content/2016-10/11/content_5117329.htm (accessed on 3 November 2001).
- Yu, X.D. Chinese national public nutrition improvement action: A major opportunity for the development of the nutrition industry. Available online: http://g.wanfangdata.com.cn/details/detail.do?_type=conference&id=6685024 (accessed on 8 December 2008).
- Ronnenberg, A.G.; Goldman, M.B.; Aitken, I.W.; Xu, X. Anemia and deficiencies of folate and vitamin B-6 are common and vary with season in Chinese women of childbearing age. J. Nutr. 2000, 130, 2703. [Google Scholar] [CrossRef] [PubMed]
- Nordenberg, D.; Yip, R.; Binkin, N. The effect of cigarette smoking on hemoglobin levels an d anemia screening. JAMA 1990, 264, 1556–1559. [Google Scholar] [CrossRef] [PubMed]
- Mast, A.E.; Steele, W.R.; Johnson, B.; Wright, D.J.; Cable, R.G.; Carey, P.; Gottschall, J.L.; Kiss, J.E.; Simon, T.L.; Murphy, E.L. Population-based screening for anemia using first-time blood donors. Am. J. Hematol. 2012, 87, 496–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Zhang, J. Research Progress on Thalassemia in Southern China. J. Exp. Hematol. 2017, 25, 276–280. [Google Scholar]
- Xu, Y.; Luo, J.M. Research status of gene mutation of G6PD deficiency in China. J. China Pediatr. Blood Cancer 2009, 14, 143–145. [Google Scholar]
- The Central People’s Government of the People’s Republic of China. General Office of the State Council on Printing and Distributing Chinese Food and Nutrition Notification of the Development Programme (2014 to 2020). Available online: http://www.gov.cn/zwgk/2014-02/10/content_2581766.htm (accessed on 28 January 2014).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N(%) | Weighted Hemoglobin (g/L)1 | P2 | Weighted prevalence (%, 95%CI) | P3 |
|---|---|---|---|---|---|
| Total | 28,289 | 136.2(126.6–145.0) | 15.0(14.3–15.7) | ||
| Age group | <0.0001 χ2 = 19.21 | 0.001 F = 6.62 | |||
| 18–29 years old | 5370(19.0) | 136.5(127.4–145.2)a | 13.4(12.0–14.8)b | ||
| 30–39 years old | 9034(31.9) | 135.8(126.0–144.2)b | 16.3(15.2–17.4)a | ||
| 40–49 years old | 13,885(49.1) | 136.4(126.4–145.3)a | 15.5(14.6–16.4)a | ||
| Region type | <0.0001 χ2 = 125.29 | 0.058 F = 2.49 | |||
| Large cities | 5607(19.8) | 137.6(127.4–145.6)a | 13.3(11.8–14.7)b | ||
| Small and medium-sized cities | 7962(28.1) | 134.7(125.6–142.9)b | 15.8(14.6–17.0)a | ||
| Ordinary rural areas | 8895(31.5) | 137.4(127.7–146.4)a | 14.3(13.3–15.4)a | ||
| Poor rural areas | 5825(20.6) | 138.5(128.5–148.5)c | 14.9(13.4–16.4)a | ||
| Ethnicity | <0.0001 χ2 = 116.96 | 0.208 F = 1.59 | |||
| Han | 24,596(86.9) | 136.0(126.3–144.6) | 15.1(14.4–15.8) | ||
| Other | 3693(13.1) | 139.0(129.4–148.1) | 13.8(12.1–15.6) | ||
| Latitude | <0.0001 χ2 = 162.18 | 0.057 F = 3.62 | |||
| North | 12,872(45.5) | 136.4(126.3–145.9) | 15.8(14.6–16.9) | ||
| South | 15,417(54.5) | 136.0(126.8–144.3) | 14.4(13.6–15.2) | ||
| Season | <0.0001 χ2 = 56.03 | <0.0001 F = 29.40 | |||
| Spring | 1236(4.4) | 130.9(116.7–142.4)a | 30.3(25.4–35.2)a | ||
| Summer | 3098(11.0) | 135.2(125.0–144.4)b | 17.9(15.7–20.2)b | ||
| Autumn | 19,314(68.3) | 136.8(127.6–145.4)c | 13.5(12.7–14.3)c | ||
| Winter | 4641(16.4) | 135.0(125.5–143.5)b | 16.5(14.7–18.3)b | ||
| BMI4 level | <0.0001 χ2=108.37 | 0.957 F = 0.04 | |||
| BMI < 24 | 17161(60.6) | 135.8(126.4–144.4)a | 15.0(14.1–15.9) | ||
| 24 ≤ BMI < 28 | 8196(29.0) | 137.0(126.9–146.0)b | 14.8(13.6–16.0) | ||
| BMI ≥ 28 | 2932(10.4) | 137.0(127.6–146.9)b | 15.2(13.0–17.3) | ||
| Education | <0.0001 χ2=49.63 | 0.002 F = 6.49 | |||
| Primary school | 8709(30.8) | 136.6(126.8–146.2)a | 15.7(14.5–16.8)a | ||
| Middle school | 16,280(57.5) | 136.1(126.3–144.8)b | 15.3(14.4–16.2)a | ||
| College and above | 3300(11.7) | 136.2(127.6–143.7)b | 11.8(10.0–13.5)b | ||
| Smoke habits | <0.0001 χ2=19.63 | 0.048 F = 3.91 | |||
| Smoke daily | 513(1.8) | 139.7(129.0–150.4) | 10.8(7.2–14.4) | ||
| No or occasionally | 27,776(98.2) | 136.2(126.5–145.0) | 15.0(14.4–15.7) | ||
| Annual family income (yuan) | <0.0001 χ2=34.91 | 0.005 F = 3.34 | |||
| <10000 | 13,637(48.2) | 136.2(126.3–145.3)b | 16.2(15.1–17.2)a | ||
| 10,000–19,999 | 8156(28.8) | 136.5(126.9–145.0)a | 13.6(12.5–14.8)b | ||
| 20,000–29,999 | 2770(9.8) | 136.1(127.8–143.8)ac | 13.1(11.1–15.1)b | ||
| 30,000–39,999 | 978(3.5) | 134.2(125.2–142.2)ac | 16.2(12.5–19.8)ab | ||
| 40,000– | 1026(3.6) | 136.5(127.0–144.4)a | 13.0(10.0–16.0)ab | ||
| Not answer | 1722(6.1) | 136.8(126.0–145.0) 4 | 15.0(12.2–17.7)4 | ||
| Variables | Total (n = 14473) odds ratio | P |
|---|---|---|
| Age group | ||
| 18–29 years old | ref | |
| 30–39 years old | 1.260(1.087–1.461) | 0.004 |
| 40–49 years old | 1.459(1.002–1.339) | 0.552 |
| Region type | ||
| Large cities | ref | |
| Small and medium-sized cities | 1.167(0.999–1.364) | 0.044 |
| Ordinary rural areas | 1.003(0.848–1.187) | 0.157 |
| Poor rural areas | 1.125(0.917–1.380) | 0.417 |
| Ethnicity | ||
| Other | ref | |
| Han | 1.148(0.967–1.362) | 0.115 |
| Latitude | ||
| South | ref | |
| North | 1.043(0.930–1.169) | 0.474 |
| Season | ||
| Autumn | ref | |
| Spring | 2.659(2.070–3.417) | <0.0001 |
| Summer | 1.478(1.229–1.779) | 0.907 |
| Winter | 1.258(1.090–1.452) | 0.006 |
| BMI level | ||
| BMI < 24 | ref | |
| 24 ≤ BMI < 28 | 0.925(0.821–1.042) | 0.514 |
| BMI ≥ 28 | 0.934(0.821–1.042) | 0.747 |
| Education | ||
| College and above | ref | |
| Primary school | 1.286(1.027–1.610) | 0.117 |
| Middle school | 1.300(1.065–1.585) | 0.027 |
| Annual family income (yuan) | ||
| 40,000– | ref | |
| <10,000 | 1.173(0.881–1.562) | 0.077 |
| 10,000–19,999 | 0.958(0.718–1.278) | 0.078 |
| 20,000–29,999 | 0.945(0.687–1.301) | 0.160 |
| 30,000–39,999 | 1.241(0.851–1.811) | 0.188 |
| Smoke habits | ||
| Smoke daily | ref | |
| No or occasionally | 1.484(1.016–2.167) | 0.041 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Li, M.; Wu, J.; Wang, R.; Mao, D.; Chen, J.; Li, W.; Yang, Y.; Piao, J.; Yang, L.; et al. Prevalence and Risk Factors for Anemia in Non-pregnant Childbearing Women from the Chinese Fifth National Health and Nutrition Survey. Int. J. Environ. Res. Public Health 2019, 16, 1290. https://doi.org/10.3390/ijerph16071290
Hu Y, Li M, Wu J, Wang R, Mao D, Chen J, Li W, Yang Y, Piao J, Yang L, et al. Prevalence and Risk Factors for Anemia in Non-pregnant Childbearing Women from the Chinese Fifth National Health and Nutrition Survey. International Journal of Environmental Research and Public Health. 2019; 16(7):1290. https://doi.org/10.3390/ijerph16071290
Chicago/Turabian StyleHu, Yichun, Min Li, Jinghuan Wu, Rui Wang, Deqian Mao, Jing Chen, Weidong Li, Yanhua Yang, Jianhua Piao, Lichen Yang, and et al. 2019. "Prevalence and Risk Factors for Anemia in Non-pregnant Childbearing Women from the Chinese Fifth National Health and Nutrition Survey" International Journal of Environmental Research and Public Health 16, no. 7: 1290. https://doi.org/10.3390/ijerph16071290
APA StyleHu, Y., Li, M., Wu, J., Wang, R., Mao, D., Chen, J., Li, W., Yang, Y., Piao, J., Yang, L., & Yang, X. (2019). Prevalence and Risk Factors for Anemia in Non-pregnant Childbearing Women from the Chinese Fifth National Health and Nutrition Survey. International Journal of Environmental Research and Public Health, 16(7), 1290. https://doi.org/10.3390/ijerph16071290