1. Introduction
Hospitalized patients, especially the elderly, are at risk of “hospitalization syndrome”, a condition associated with staying long-term in hospital. Symptoms comprise of gradual loss of orientation and cognition, loss of patient’s interest in their surroundings, and unwillingness to participate in group therapy or maintain contact with others [
1]. Typically, activities that had provided joy in the past are discontinued, the individual wishes to stay in bed and prefers to spend the entire day in their room or sleeps. Indeed, a person becomes increasingly lethargic until they lose all interest in matters. This syndrome has many causes, the most common being medication, infection, response to surgery, isolation, and dehydration [
2]. Another factor that can contribute to the development of hospitalization syndrome is the routine and stereotypical course of the days [
3].
Consequences can be both psychological and physical in nature, and a permanent change in cognitive function may occur. Nevertheless, sufficient appropriate external stimuli could prevent against its onset. However, it is crucial that any such motivations are of interest to the patient. During the process of rehabilitation, frequent family visits and patient support services are particularly important. The presence of an animal supplements these strategies, since a large number of hospitalized patients have pets, and contact with the animal reminds them of home and the stimuli they received in their own environment [
4].
Social and healthcare facilities already run a number of activity programs, such as music or art therapy, cooking, cognitive training, and memory training. It would be possible to introduce an animal into such activities or separately, whether they are put on for a group or an individual. That kind of initiative might prove to be of assistance to those with pets of their own, effectively acting as a bridge between their lives outside the establishment and their present circumstances. Indeed, the efficacy of other therapies may be increased if the patient is motivated and interested in the participation and the content of the therapy [
5]. In fact, studies have confirmed that some individuals who had previously refused to join in group therapy actually came along to sessions if they knew a dog would be present. Additionally, the duration of treatment was longer in sessions with the dog in attendance [
6].
Furthermore, hospital settings often lack opportunities to engage in meaningful communication, which is an essential part of human life, as well as crucial for motivation and the desire to make progress. A dog can constitute a good mediator of communication, acting as a catalyst for building relationships and providing a common topic for conversation [
7]. In this context, people gain a sense of inner calmness and contentment, in addition to being better able to manage social interactions and take in information from the environment [
8].
Rodin and Langer [
9] stated that an option for supporting long-term hospitalized patients would allow the patients to decide how they wished to spend their time, which would consequently make them feel healthier and better than they would otherwise. The importance of this research lies in the fact that such patients would be encouraged to take small steps to make their own choices and personal commitments. Animal assisted therapy (AAT) might then act as a supportive measure, permitting the patient to opt for the therapies they wish to partake in, a distinct benefit over receiving physiotherapy.
The aim of this study was to determine whether AAT has a positive effect on patients in long-term care and whether these treatments affect parameters such as blood pressure, heart rate, and Barthel index. To this end, the hypothesis was that a positive influence would be exerted, pertaining to the general mood and Barthel index of the patients, thanks to the dog helping to initiate and mediate pleasant experiences for the long-term care patients. We expected the blood pressure and heart rate to be the same in both groups; that the values would remain at the physiological level; and that therapy would not lead to any pathological increase or decrease.
2. Methods
2.1. Participants
A total of 72 patients participated in this study. The experimental group comprised 33 patients (8 males, 25 females), whereas the control group was made up of 39 patients (11 men, 28 women). The participants in the experimental group were aged between 51 and 95 years (84.5 ± 12, mean ± standard deviation); the control group contained persons between 58 and 100 years of age (87 ± 10.2, mean ± standard deviation). The experimental cohort received rehabilitation supplemented with the assistance of the dog, while the control group was given rehabilitation treatment in a standard way.
This study involved inpatients that were expected to be housed in a long-term care unit for at least three months. The diseases that affected patients were stroke, mild dementia or mild cognitive disease, or cancer. However, the goal was not to overcome the symptoms of such diseases, but to enhance the general condition and well-being of the patients. For this reason, the specific illness was not taken into account as a negative factor for the overall study. Research was conducted under conditions corresponding to real practice. Patients displaying happiness during an encounter with the dog, and who agreed to engage with him in therapy, were deemed suitable candidates. The cohort of patients was randomly assigned into either the control or experimental groups, utilizing envelopes for such randomization. The project was approved by the Ethics Committee of the Central Military Hospital in Prague (Military University Hospital) and evaluated as a non-invasive observational study. It was also approved by the Ethics Committee of the Czech University of Life Sciences in Prague. The study and its methodological procedure adhered with the requirements of European Union and Czech legislation (Act no. 246/1992 coll. on animal protection as amended by Act no. 162/1993 coll.).
2.2. Measurements
Diagnosis, rehabilitation, and testing were carried out at the Department of Long-term Care. Data collection and inclusion of patients in the study were carried out shortly after the patients had been admitted to hospital for long-term care.
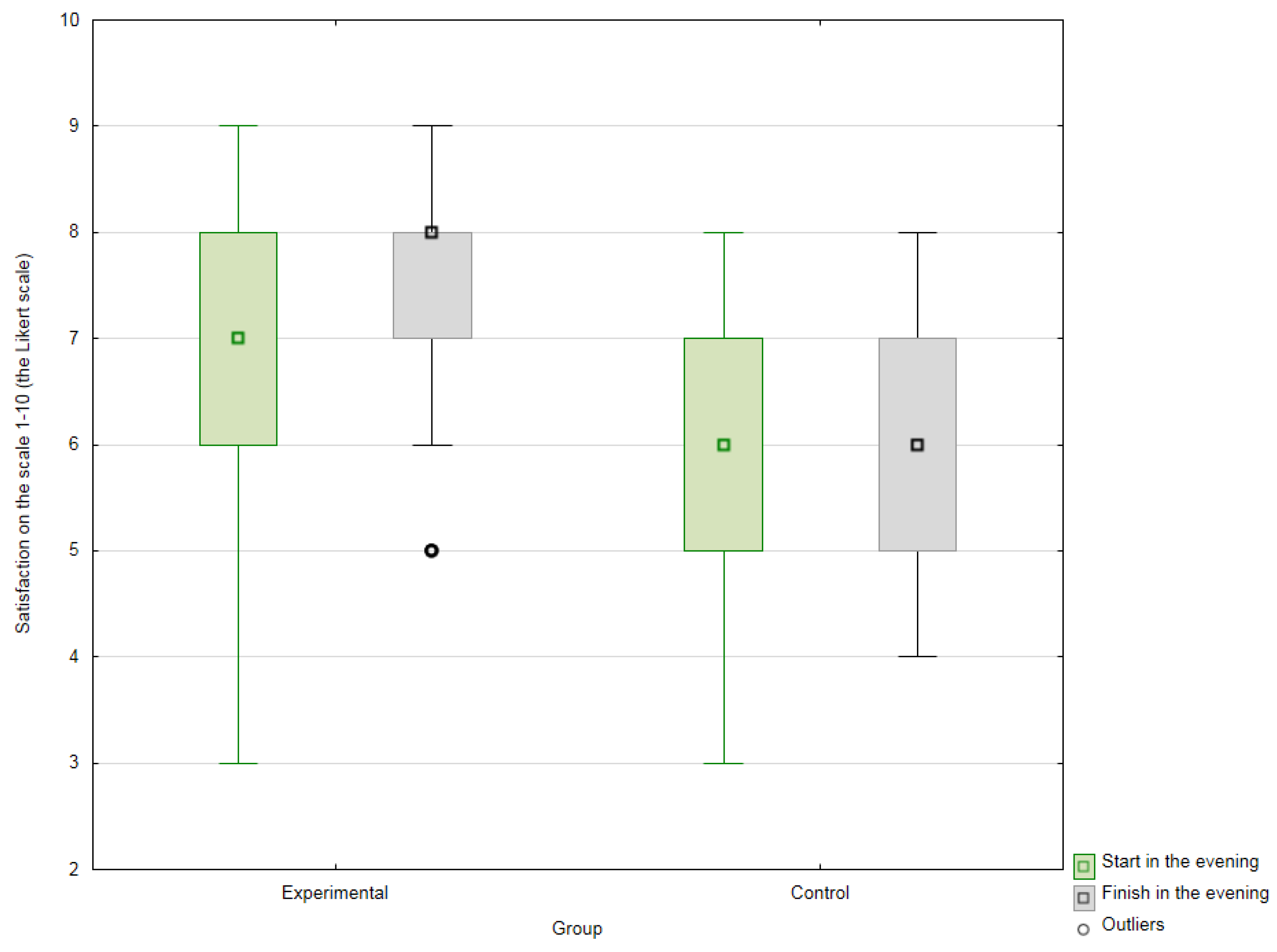
Mood was evaluated by a Likert scale that allowed patients to rate their general mood on a scale of 1 to 10 [
10,
11] on every day of therapy. The people in the experimental and control groups were asked by the same therapist to evaluate how they felt. The instruction received by patients was as follows: rate the mood you have right now on a scale of 1 to 10, with 1 being the worst mood and 10 being the best mood. The 10-point scale was chosen in order to improve patients’ understanding compared to a 5-point scale, since patients may have otherwise been confused with using a 5-point scale due to grading at school, where 1 is the best classification. Those in the experimental group were interviewed once a week before and after therapy sessions. For the control group, two measurements were reported from the same day in the morning and after a one-hour interval once a week as well (on the same days as patients in the experimental group) at times they were involved in the normal regime of the hospital.
Methods for evaluating physiological functions and scoring the Barthel index were based on requirements demanded by the nursing documentation; both were carried out at the commencement of the study, repeatedly over the following three months (every three days) and at the end of the test period. Blood pressure and heart rate were measured using pressure gauge. The Barthel index, which assesses self-sufficiency, was incorporated and gauged within the nursing documentation [
12,
13].
The patients were all housed in one department. Participation in the study was voluntary, and any individual could quit at any time, although no one chose to do so. In addition, everyone gave their permission for the results of the study to be published and for photographs taken during the course of their therapy to be used.
2.3. The Therapy Dog
The therapy of the experimental group was conducted with the participation of a five-year-old border collie named Mia. Prior to her joining the therapy sessions, Mia undertook AAT certification. Her training was focused on obedience, even under special circumstances, on her ability to cope with stressful situations, and on her handler’s ability to gauge her behavior during unusual situations. The characteristic feature of Mia is her constant interest in people and working with them. She has no problem being close to strangers, or playing or interacting with them. Notably, Mia shows no aggression towards humans or animals.
The long-term inclusion of Mia in AAT is possible due to careful monitoring of her welfare and respect for her needs. Herein, the content of her “work day” varied, thereby preventing any sense of burnout. She was always given plenty of time to rest, had permanent access to water and she only received kibbles in limited quantities as treats to avoid any overfeeding.
2.4. General Procedures
All patients received standard nursing care, therapy, and patient activation under the auspices of rehabilitation nursing. The sessions for members of the experimental group were attended by the therapy dog Mia. Her visits took place once a week over a period of 12 weeks, and the individuals in question also came across her at random either in the department or in group activities. Each individual therapeutic session lasted approximately twenty minutes. Prior to every such visitation, the therapist consulted the condition of the patient with a physician, occupational therapist, physiotherapist, or the nursing staff, and together they evaluated the objective of the upcoming therapeutic session. The aims of sessions were cognitive function training, relaxation, basal stimulation, gross or fine motor skills training, co-operation within the treatment regimen, and prevention of hospitalization syndrome. The therapies selected were based on the needs of the given patient and on his or her current state of mind. Mia accompanied clients on outdoor walks, played fetch with a ball, or did short obedience exercises. She was able to interact positively with patients and generate conversations just through her presence.
2.5. Statistical Analysis
The Statistica 13.2 program (Informer Technologies, Inc., Palo Alto, CA, USA) was used to evaluate the data obtained. Initially, exploratory data analysis was performed on the file to verify the independence of sampling, as well as homogeneity of the samples and the normality of their distribution. After carrying out the Shapiro–Wilk test, the data were evaluated via histograms and standardized probability charts.
Pearson’s chi-squared test was employed to test variances in the subjective perception of the patients regarding their mood before and after therapy, as well as to generalize the proof of variance. The strength of dependence was judged on the basis of Pearson’s contingency coefficient (C). The coefficient of association was utilized to assess strength of association. Regarding the four-way contingency table, the chi-squared test confirmed the statistically significant dependence of the qualitative parameters under evaluation. Subsequently, odds ratios were acquired and interpreted, allowing for a relationship to be discerned between the associated frequencies in the four-way table.
For measuring the heart rate and blood pressure, the baseline (the input of the study) was selected as the median of the first five measurements, while the final value (upon completion of the therapeutic cycle) equaled the median of the last five measurements.
The frequencies of the measured data proved different for the individual patients. The data analyzed mostly showed a normal Gaussian distribution. In order to test differences in measured values at the beginning and end of the therapy, a paired-samples t-test for frequency-dependent selections was applied. A two-sample t-test was employed to assess variances in the results of the experimental and control groups.
A more detailed assessment was conducted for the Barthel index, which showed the greatest variability and improvement. In order to assess the period prior to the first signs of improvement in the experimental and control groups on the Barthel index, the Shapiro–Wilk test was applied to verify the normality of distribution, and the differences were then checked by a two-sample t-test for independent samples.
4. Discussion
The aim of this study was to evaluate the influence of a therapy dog on the health status of patients accommodated in the long-term care department at a hospital. This study also evaluated parameters that formed part of standard nursing documentation, building up a general picture of the health of the patient. Said parameters comprised assessment of heart rate, blood pressure, the Barthel index, and general mood.
No difference was discerned between the experimental and the control groups in heart rate and blood pressure. This study did not reveal any tendency for variation in these parameters. Odendaal and Meintjes [
14], Cole et al. [
15], Allen et al. [
16], Allen et al. [
17], and Allen [
18] unequivocally demonstrated that interacting with animals resulted in lower blood pressure and a reduced heart rate. Indeed, Odendaal and Meintjes [
14] and Cole et al. [
15] highlighted such a change of this nature after merely a few minutes of such interaction. In a study by Allen [
18], the participants of the study adopted the animals, so long-term measurements were involved. Allen et al. [
17] reported that blood pressure was measured as part of the therapy, later demonstrating that it was also reduced. Said study, however, involved dogs being assigned to a number of households, whose members remained in daily contact with the animals. All the studies were working with patients or participants with pathological levels of blood pressure, cardiovascular disease, or who were under acute stress. From the perspective of changes in blood pressure after treatment accompanied by animals, the results reported therein are rather unclear. Therefore, reduction in blood pressure would not appear to be completely evident, although it seems that claims made in support of it have been commonplace. The question remains as to whether the daily presence of a dog would actually diminish the effect of said presence, should the dog become part of daily life at a hospital. Any further study would benefit from optimal frequency of AAT and appropriate measurements, including gauging long-term effects.
Even in relation to ADL (activities of daily living, as assessed by the Barthel Index), no statistically significant shift was discerned in either group. Indeed, no statistically significant differences in input and output values were observed between the control or experimental groups. However, it is important to consider that these were individuals at around the age of 90 years; since these patients were hospitalized with chronic illnesses, it is understandable that any significant shift in their ADL would be exceptional.
Importantly, though, the patients seemed to have benefited from the visits by the dog through signs of improvement in general mood. The patients would anticipate seeing the dog in the department. Said people would link the regular visits by the dog to their room with particular days; such visits lent some kind of meaning to their otherwise drawn-out daily routine. Their reactions to the presence of the dog certainly were not neutral. Such emotions are revealed, as Francis and Pennebaker [
19] put it, and it could appear that the animal helped the patients experience such high emotions or let them go to the surface. The presence of the animal additionally formed a subject of conversation amongst fellow patients, in the room or elsewhere, and the attending staff, as well as with members of the patients’ families. Furthermore, elders frequently do not wish to complain or bother anyone, but they can express their feelings to a dog. Similar studies on autism in children have also revealed that sufferers display a sense of contentment and smile more [
7,
8].
Therefore, it could be hypothesized that the presence of a dog allows other thoughts to enter the minds of the patients. Herein, patients put aside worries about their health, instead starting conversations on ordinary subjects or choosing to remain quiet [
20]. Some patients simply sat quietly when petting the dog, while others chatted away when stroking it. The possibility of direct physical contact granted them the pleasant sensation that they could relax and calm down [
21].
Another important aspect observed was the readiness by the patient to see the animal. Often the patients had family members or friends bring snacks for it and the dog was the common subject for the visitors and the patients. Interestingly, patients frequently uttered the words “I can finally be useful”. This finding was consistent with a study by Clark et al. [
5], which also highlighted the importance in therapy of inherent interest and a sense of meaning as a person.
Some studies describe that the presence of an animal distracts the attention of participants from pain and from thinking about problems [
22,
23,
24,
25]; instead, it directs the thoughts of the patient towards the dog and the activities associated with the therapy in question. Naturally, the option exists to move such activities to outdoor areas, beyond the confinements of the healing facility, giving the patients the opportunity to stay outside in the sun and in the company of others, perhaps after spending a few months inside, to choose to dress themselves, do their hair, and to walk the dog, thus exerting a positive influence on their well-being [
6,
26].
Limitations
Several questions remain unanswered. One of the limits of this study may be the variety of illnesses suffered by the patients and the different lengths of time that had passed since their initial hospitalization. Another potential limit is the factor of the given therapist or dog. Indeed, the study was conducted with the participation of just one therapist and one dog, hence the personality of the former or the character and temperament of the latter may have impinged upon the outcome of therapy. Lastly, the medication the individual received could have affected the blood pressure measured; this is important with respect to chronically ill patients such as these, since their blood pressure is managed to keep it as stable as possible. Nevertheless, the positive aspect of this study was the fact that research did not take place under laboratory conditions but in a real environment.





{kind=link}
{kind=link}