Hybrid Resiliency-Stressor Conceptual Framework for Informing Decision Support Tools and Addressing Environmental Injustice and Health Inequities



{kind=link}
Abstract
:1. Introduction
1.1. Cumulative Risk Assessment Background
1.2. Challenges of Operating in Cumulative Risk Assessment Silos
1.3. Resilience in the Context of Environmental Justice
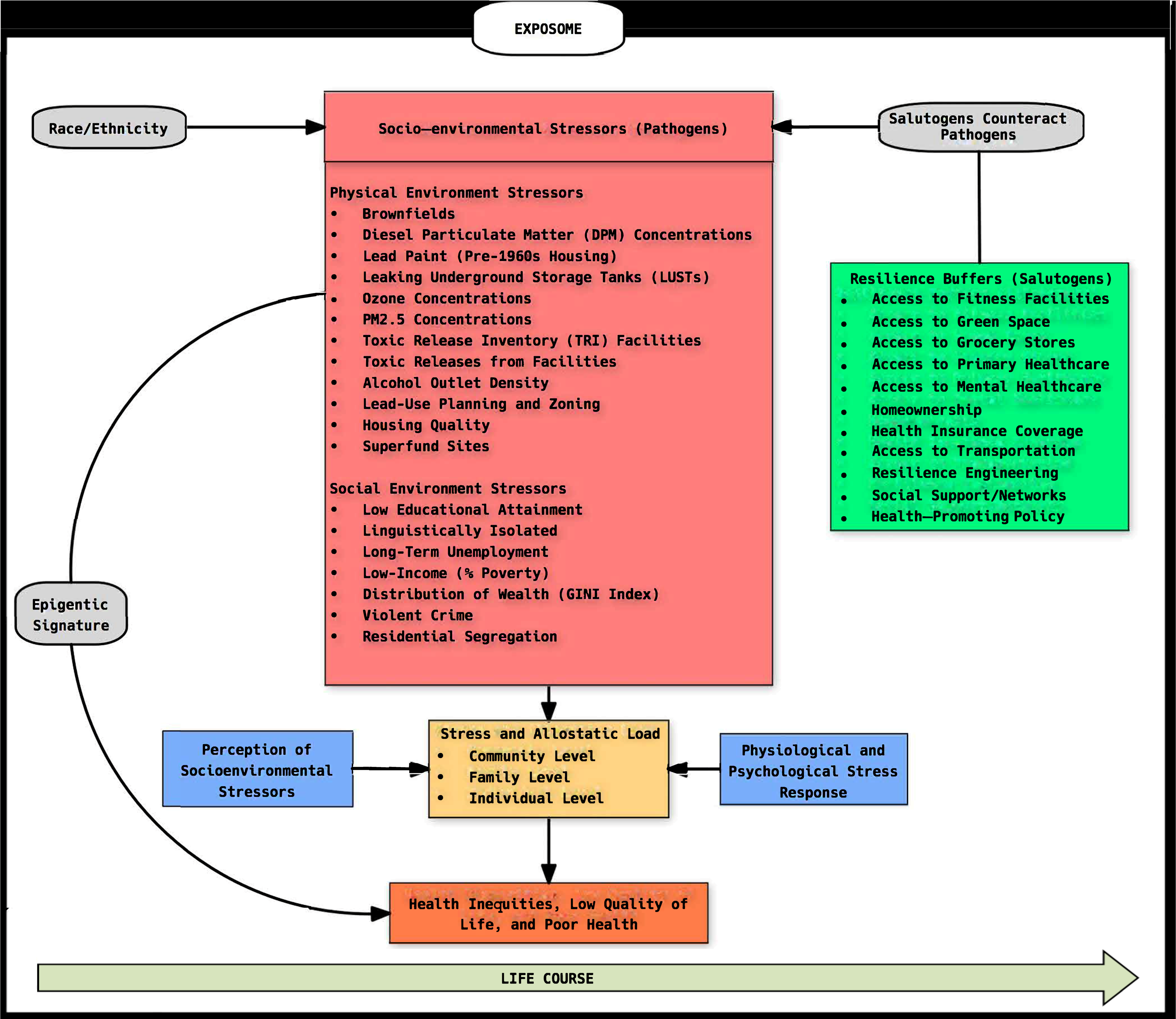
1.4. Resiliency-Stressor Conceptual Framework Overview
2. Resiliency-Stressor Conceptual Framework Components
2.1. Exposome
2.2. Stress and Allostatic Load
2.3. Actual Socio-Environmental Stressors
2.4. Perceptions of Stressors and Stress Response
2.5. Resilience Buffers
3. Challenges of Integrating Resilience into Cumulative Risk Assessment Screening
4. Public Health Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. What is the Environment in the Context of Health? Available online: http://www.who.int/quantifying_ehimpacts/publications/preventingdisease2.pdf (accessed on 1 January 2018).
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Wilson, S. An ecologic framework to study and address environmental justice and community health issues. Environ. Justice 2009, 2, 15–24. [Google Scholar] [CrossRef]
- Davis, R.; Cook, D.; Cohen, L. A community resilience approach to reducing ethnic and racial disparities in health. Am. J. Public Health 2005, 95, 2168–2173. [Google Scholar] [CrossRef] [PubMed]
- Longstaff, P.H.; Armstrong, N.J.; Perrin, K.; Parker, W.M.; Hidek, M.A. Building resilient communities: A preliminary framework for assessment. Homel. Secur. Aff. 2010, 6, 1–23. [Google Scholar]
- Olden, K.; Freudenberg, N.; Dowd, J.; Shields, A.E. Discovering how environmental exposures alter genes could lead to new treatments for chronic illnesses. Health Aff. 2011, 30, 833–841. [Google Scholar] [CrossRef]
- Burwell-Naney, K.; Zhang, H.; Samantapudi, A.; Jiang, C.; Dalemarre, L.; Rice, L.; Williams, E.; Wilson, S. Spatial disparity in the distribution of superfund sites in South Carolina: An ecological study. Environ. Health 2013, 12, 96. [Google Scholar] [CrossRef]
- Rice, L.J.; Jiang, C.; Wilson, S.M.; Burwell-Naney, K.; Samantapudi, A.; Zhang, H. Use of segregation indices, Townsend Index, and air toxics data to assess lifetime cancer risk disparities in Metropolitan Charleston, South Carolina, USA. Int. J. Environ. Res. Public Health 2014, 11, 5510–5526. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.M.; Fraser-Rahim, H.; Williams, E.; Zhang, H.; Rice, L.; Svendsen, E.; Abara, W. Assessment of the distribution of toxic release inventory facilities in Metropolitan Charleston: An environmental justice case study. Am. J. Public Health 2012, 102, 1974–1980. [Google Scholar] [CrossRef]
- Wilson, S.; Zhang, H.; Burwell, K.; Samantapudi, A.; Dalemarre, L.; Jiang, C.; Rice, L.; Williams, E.; Naney, C. Leaking underground storage tanks and environmental injustice: Is there a hidden and unequal threat to public health in South Carolina? Environ. Justice 2013, 6, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.; Zhang, H.; Jiang, C.; Burwell, K.; Rehr, R.; Murray, R.; Dalemarre, L.; Naney, C. Being overburdened and medically underserved: Assessment of this double disparity for populations in the state of Maryland. Environ. Health 2014, 13, 26. [Google Scholar] [CrossRef]
- Tufts University Global Development and Environment Institute Website. Environmental Justice: Income, Race, and Health. Available online: http://www.ase.tufts.edu/gdae/education_materials/modules/Environmental_Justice.pdf (accessed on 3 January 2018).
- Morello-Frosch, R.; Zuk, M.; Jerrett, M.; Shamasunder, B.; Kyle, A.D. Understanding the cumulative impacts of inequalities in environmental health: Implications for policy. Health Aff. 2011, 30, 879–887. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency Website. Framework for Cumulative Risk Assessment. Available online: https://www.epa.gov/sites/production/files/2014-11/documents/frmwrk_cum_risk_assmnt.pdf (accessed on 3 January 2018).
- Rhodes, E.L. Environmental Justice in America: A New Paradigm; Indiana University Press: Bloomington, IN, USA, 2003. [Google Scholar]
- Sexton, K. Cumulative risk assessment: An overview of methodological approaches for evaluating combined health effects from exposure to multiple environmental stressors. Int. J. Environ. Res. Public Health 2012, 9, 370–390. [Google Scholar] [CrossRef]
- Sexton, K.; Linder, S.H. The role of cumulative risk assessment in decisions about environmental justice. Int. J. Environ. Res. Public Health 2010, 7, 4037–4049. [Google Scholar] [CrossRef]
- National Environmental Justice Advisory Council. U.S. Environmental Protection Agency Website. Ensuring Risk Reduction in Communities with Multiple Stressors: Environmental Justice and Cumulative Risks/Impacts. Available online: https://www.epa.gov/sites/production/files/2015-04/documents/ensuringriskreducationnejac.pdf (accessed on 17 January 2018).
- MacDonell, M.M.; Haroun, L.A.; Teuschler, L.K.; Rice, G.E.; Hertzberg, R.C.; Butler, J.P.; Chang, Y.-S.; Clark, S.L.; Johns, A.P.; Perry, C.S.; et al. Cumulative risk assessment toolbox: Methods and approaches for the practitioner. J. Toxicol. 2013, 2013, 310904. [Google Scholar] [CrossRef]
- Israel, B.D. An environmental justice critique of risk assessment. NYU Environ. Law J. 1995, 3, 469–522. [Google Scholar]
- Williams, P.R.D.; Dotson, G.S.; Maier, A. Cumulative risk assessment (CRA): Transforming the way we assess health risks. Environ. Sci. Technol. 2012, 46, 10868–10874. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.S.; Sax, S.N.; Wason, S.C.; Campleman, S.L. Non-chemical stressors and cumulative risk assessment: An overview of current initiatives and potential air pollutant interactions. Int. J. Environ. Res. Public Health 2011, 8, 2020–2073. [Google Scholar] [CrossRef] [PubMed]
- Barzyk, T.M.; Wilson, S.; Wilson, A. Community, state, and federal approaches to cumulative risk assessment: Challenges and opportunities for integration. Int. J. Environ. Res. Public Health 2015, 12, 4546–4571. [Google Scholar] [CrossRef]
- Jordan, R.C.; Sorensen, A.E.; Biehler, D.; Wilson, S.M.; LaDeau, S. Citizen science and civic ecology: Merging paths to stewardship. J. Environ. Stud. Sci. 2019, 9, 133–143. [Google Scholar] [CrossRef]
- Sorensen, A.E.; Jordan, R.C.; LaDeau, S.L.; Biehler, D.; Wilson, S.M.; Pitas, J.H.; Leisnham, P.T. Reflecting on efforts to design an inclusive citizen science project in West Baltimore. Citiz. Sci. Theory Pract. 2019, 4. [Google Scholar] [CrossRef]
- Commodore, A.; Wilson, S.; Muhammad, O.; Svendsen, E.; Pearce, J. Community-based participatory research for the study of air pollution: A review of motivations, approaches, and outcomes. Environ. Monit. Assess. 2017, 189, 378. [Google Scholar] [CrossRef]
- Brandt, H.M.; Haynes, V.E.; Rice, L.J.; Campbell, D.; Williams, E.; Wilson, S.M.; Glover, S. Using photovoice as a tool for community engagement to assess the environment and explore environmental health disparities. J. Health Disparities Res. Pract. 2017, 10, 68–86. [Google Scholar]
- Wilson, S.; Aber, A.; Ravichandran, V.; Wright, L.; Muhammad, O. Soil contamination in urban communities impacted by industrial pollution and goods movement activities. Environ. Justice 2017, 10, 16–22. [Google Scholar] [CrossRef]
- Burwell-Naney, K.; Wilson, S.M.; Tarver, S.L.; Svendsen, E.; Jiang, C.; Ogunsakin, O.A.; Zhang, H.; Campbell, D.; Fraser-Rahim, H. Baseline air quality assessment of goods movement activities before the Port of Charleston expansion: A community–university collaborative. Environ. Justice 2017, 10, 1–10. [Google Scholar] [CrossRef]
- Wilson, S.; Campbell, D.; Dalemarre, L.; Fraser-Rahim, H.; Williams, E. A critical review of an authentic and transformative community-university partnership. Int. J. Environ. Res. Public Health 2014, 11, 12817–12834. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.L.; Caldwell, D.; Hopkins, B.; Heaney, C.D.; Wing, S.; Wilson, S.M.; O’Shea, S.; Yeatts, K. Integrating research and community organizing to address water and sanitation concerns in a community bordering a landfill. J. Environ. Health 2013, 75, 48–50. [Google Scholar]
- Olvera Alvares, H.A.; Appleton, A.A.; Fuller, C.H.; Belcourt, A.; Kubzansky, L.D. An integrated socio-environmental model of health and well-being: A conceptual framework exploring the joint contribution of environmental and social exposures to health and disease over the life span. Curr. Environ. Health Rep. 2018, 5, 233–243. [Google Scholar] [CrossRef]
- Huang, G.; London, J.K. Cumulative environmental vulnerability and environmental justice in California’s San Joaquin Valley. Int. J. Environ. Res. Public Health 2012, 9, 1593–1608. [Google Scholar] [CrossRef]
- OEHHA. Update to the California Communities Environmental Health Screening Tool. Available online: https://oehha.ca.gov/media/downloads/calenviroscreen/report/ces3report.pdf (accessed on 1 February 2018).
- Su, J.G.; Morello-Frosch, R.; Jesdale, B.M.; Kyle, A.D.; Shamasunder, B.; Jerrett, M. An index for assessing demographic inequalities in cumulative environmental hazards with application to Los Angeles, California. Environ. Sci. Technol. 2009, 43, 7626–7634. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services Community Resilience. Available online: http://www.phe.gov/Preparedness/planning/abc/Pages/community-resilience.aspx (accessed on 12 January 2018).
- Community & Regional Resilience Institute. Definitions of Community Resilience: An Analysis. Available online: http://www.resilientus.org/wp-content/uploads/2013/08/definitions-of-community-resilience.pdf (accessed on 12 January 2018).
- Chandra, A.; Williams, M.; Plough, A.; Stayton, A.; Wells, K.B.; Horta, M.; Tang, J. Getting actionable about community resilience: The Los Angeles County Community Disaster Resilience project. Am. J. Public Health 2013, 103, 1181–1189. [Google Scholar] [CrossRef]
- Wulff, K.; Donato, D.; Lurie, N. What is health resilience and how can we build it? Annu. Rev. Public Health 2015, 36, 361–374. [Google Scholar] [CrossRef]
- Bryant, B. Environmental Justice: Issues, Policies and Solutions; Island Press: Washington, DC, USA, 1995. [Google Scholar]
- Theall, K.P.; Drury, S.S.; Shirtcliff, E.A. Cumulative neighborhood risk of psychosocial stress and allostatic load in adolescents. Am. J. Epidemiol. 2012, 176, S164–S174. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K.; Linder, S.H. Cumulative risk assessment for combined health effects from chemical and nonchemical stressors. Am. J. Public Health 2011, 101, S81–S88. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization. Resilience Index Measurement and Analysis Model. Available online: http://www.fao.org/3/a-i1402e.pdf (accessed on 12 January 2018).
- Miller, F.; Osbahr, H.; Boyd, E.; Thomalla, F.; Bharawani, S.; Ziervogel, G.; Walker, B.; Birkmann, J.; van der Leeuw, S.; Rockström, J.; et al. Resilience and vulnerability: Complementary or conflicting concepts. Ecol. Soc. 2010, 15, 11. [Google Scholar] [CrossRef]
- Bergstrand, K.; Mayer, B.; Brumback, B.; Zhang, Y. Assessing the relationship between social vulnerability and community resilience to hazards. Soc. Indic. Res. 2015, 122, 391–409. [Google Scholar] [CrossRef]
- Adler, T. A complex relationship: Psychosocial stress, pollution, and health. Environ. Health Persp. 2009, 117, A407. [Google Scholar] [CrossRef]
- Crowder, K.; Downey, L. Inter-neighborhood migration, race, and environmental hazards: Modeling micro-level processes of environmental inequality. AJS 2010, 115, 1110–1141. [Google Scholar] [PubMed]
- Perera, F.; Herbstman, J. Prenatal environmental exposures, epigenetics, and disease. Reprod. Toxicol. 2011, 31, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Wild, C.P. Complementing the genome with an “exposome”: The outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidem. Biomar. 2005, 14, 1847–1850. [Google Scholar] [CrossRef]
- Cui, Y.; Balshaw, D.M.; Kwok, R.K.; Thompson, C.L.; Collman, G.W.; Birnbaum, L.S. The exposome: Embracing the complexity for discovery in environmental health. Environ. Health Persp. 2016, 124, A137–A140. [Google Scholar] [CrossRef] [PubMed]
- Juarez, P.; Matthews-Juarez, P.; Hood, D.; Im, W.; Levine, R.S.; Kilbourne, B.J.; Langston, M.A.; Al-Hamdan, M.Z.; Crosson, W.L.; Estes, M.G.; et al. The public health exposome: A population-based, exposure science approach to health disparities research. Int. J. Environ. Res. Public Health 2014, 11, 12866–12894. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.T.; de la Rosa, R.; Daniels, S.I. Using exposomics to assess cumulative risks and promote health. Environ. Mol. Mutagen. 2015, 56, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P. The exposome: From concept to utility. Int. J. Epidemiol. 2012, 41, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Beckie, T.M. A systematic review of allostatic load, health, and health disparities. Biol. Res. Nurs. 2012, 14, 311–346. [Google Scholar] [CrossRef] [PubMed]
- Clougherty, J.E.; Kubzansky, L.D. A framework for examining social stress and susceptibility to air pollution in respiratory health. Environ. Health Perspect. 2009, 117, 1351–1358. [Google Scholar] [CrossRef]
- Gee, G.C.; Payne-Sturges, D.C. Environmental health disparities: A framework integrating psychosocial and environmental concepts. Environ. Health Perspect. 2004, 112, 1645–1653. [Google Scholar] [CrossRef]
- Logan, J.G.; Barksdale, D.J. Allostatis and allostatic load: Expanding the discourse on stress and cardiovascular disease. J. Clin. Nurs. 2008, 17, 201–208. [Google Scholar] [CrossRef]
- Morello-Frosch, R.; Shenassa, E.D. The environmental “riskscape” and social inequality: Implications for explaining maternal and child health disparities. Environ. Health Perspect. 2006, 114, 1150–1153. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Ann. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef]
- Torpy, J.M.; Lynm, C.; Glass, R.M. Chronic stress and the heart. JAMA 2007, 298, 1722. [Google Scholar] [CrossRef]
- Davis, M.T.; Holmes, S.E.; Pietrzak, R.H.; Esterlis, I. Neurobiology of chronic stress-related psychiatric disorders. Chronic Stress 2017, 1, 1–21. [Google Scholar] [CrossRef]
- Austin, K.W.; Ameringer, S.W.; Cloud, L.J. An integrated review of psychological stress in Parkinson’s disease: Biological mechanisms and symptom and health outcomes. Parkinsons Dis. 2016, 2016, 9869712. [Google Scholar] [CrossRef]
- Machado, A.; Herrera, A.J.; de Pablos, R.M.; Espinosa-Oliva, A.M.; Sarmiento, M.; Ayala, A.; Venero, J.L.; Santiago, M.; Villarán, R.F.; Delgado-Cortés, M.J.; et al. Chronic stress as a risk factor for Alzheimer’s disease. Rev. Neurosci. 2014, 25, 785–804. [Google Scholar] [CrossRef]
- Mohr, D.C.; Hart, S.L.; Julian, L.; Cox, D.; Pelletier, D. Association between stressful life events and exacerbation in multiple sclerosis: A meta-analysis. BMJ 2004, 328, 731. [Google Scholar] [CrossRef] [PubMed]
- Yau, Y.H.C.; Potenza, M.N. Stress and eating behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar] [PubMed]
- Sinha, R. How does stress increase risk of drug abuse and relapse? Psychopharmacology 2001, 158, 343–349. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, A.C. The long-term costs of traumatic stress: Intertwined physical and psychological consequences. World Psychiatry 2010, 9, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Oken, B.S.; Chamine, I.; Wakeland, W. A systems approach to stress, stressors and resilience in humans. Behav. Brain Res. 2015, 282, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.I.; Weekley, C.C.; Chen, S.-C.; Li, S.; Tamura, M.K.; Norris, K.C.; Shlipak, M.G. Association of educational attainment with chronic disease and mortality: The Kidney Early Evaluation Program (KEEP). Am. J. Kidney Dis. 2011, 58, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic disparities in health behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Tsai, J.; Higgins, P.C.; Lebrun, L.A. Racial/ethnic and socioeconomic disparities in access to care and quality of care for US health center patients compared with non-health center patients. J. Ambul. Care Manag. 2009, 32, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Gee, G.C.; Ponce, N. Associations between racial discrimination, limited English proficiency, and health-related quality of life among 6 Asian ethnic groups in California. Am. J. Public Health 2010, 100, 888–895. [Google Scholar] [CrossRef]
- McKee-Ryan, F.; Song, Z.; Wanberg, C.R.; Kinicki, A.J. Psychological and physical well-being during unemployment: A meta-analytic study. J. Appl. Psychol. 2005, 90, 53–76. [Google Scholar] [CrossRef] [PubMed]
- Pharr, J.R.; Moonie, S.; Bungum, T.J. The impact of unemployment on mental and physical health, access to health care and health risk behaviors. ISRN 2011, 2012, 483432. [Google Scholar] [CrossRef]
- Saunders, P. The Direct and Indirect Effects of Unemployment on Poverty and Inequality; The Social Policy Research Centre: Sydney, Australia, 2002. [Google Scholar]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, C.; Novick, L.F. Poverty and health: Focus on North Carolina. N. C. Med. J. 2012, 73, 366–373. [Google Scholar] [PubMed]
- Brunner, E.; Marmot, M. Social organization, stress and health. In Social Determinants of Health, 2nd ed.; Marmot, M., Ed.; Oxford University Press: New York, NY, USA, 2005; pp. 7–30. [Google Scholar]
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: A causal review. Soc. Sci. Med. 2015, 128, 316–326. [Google Scholar] [CrossRef]
- Enamorado, T.; Lopez-Calva, L.-F.; Rodriguez-Castelan, C.; Winkler, H. Income inequality and violent crime: Evidence from Mexico’s drug war. J. Dev. Econ. 2016, 120, 128–143. [Google Scholar] [CrossRef]
- Curry, A.; Latkin, C.; Davey-Rothwell, M. Pathways to depression: The impact of neighborhood violent crime on inner-city residents in Baltimore, Maryland, USA. Soc. Sci. Med. 2008, 67, 23–30. [Google Scholar] [CrossRef]
- Masi, C.M.; Hawkley, L.C.; Piotrowski, Z.H.; Pickett, K.E. Neighborhood economic disadvantage, violent crime, group density, and pregnancy outcomes in a diverse, population. Soc. Sci. Med. 2007, 65, 2440–2457. [Google Scholar] [CrossRef]
- Messer, L.C.; Kaufman, J.S.; Dole, N.; Herring, A.; Laraia, B.A. Violent crime exposure classification and adverse birth outcomes: A geographically-defined cohort study. Int. J. Health Geogr. 2006, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Messer, L.C.; Kaufman, J.S.; Dole, N.; Herring, A.; Laraia, B.A. Neighborhood crime, deprivation, and preterm birth. Ann. Epidemiol. 2006, 16, 455–462. [Google Scholar] [CrossRef]
- Morello-Frosch, R.; Jesdale, B.M. Separate and unequal: Residential segregation and estimated cancer risks associated with ambient air toxics in US Metropolitan areas. Environ. Health Perspect. 2006, 114, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.E. Environmental health disparities in housing. Am. J. Public Health 2011, 101, S115–S122. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.R.; Hogue, C.R. Is segregation bad for your health? Epidemiol. Rev. 2009, 31, 178–194. [Google Scholar] [CrossRef] [PubMed]
- Morello-Frosch, R.; Lopez, R. The riskscape and the color line: Examining the role of segregation in environmental health disparities. Environ. Res. 2006, 102, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Landrine, H.; Corral, I. Separate and unequal: Residential segregation and black health disparities. Ethn. Dis. 2009, 19, 179–184. [Google Scholar]
- Yang, T.C.; Matthews, S.A. Death by segregation: Does the dimension of racial segregation matter? PLoS ONE 2015, 10, e0138489. [Google Scholar] [CrossRef] [PubMed]
- Messer, L.C.; Laraia, B.A.; Mendola, P. Segregation and preterm birth: The effects of neighborhood racial composition in North Carolina. Health Place 2009, 15, 1–9. [Google Scholar]
- Debbink, M.P.; Bader, M.D.M. Racial residential segregation and low birth weight in Michigan’s Metropolitan areas. Am. J. Public Health 2011, 101, 1714–1720. [Google Scholar] [CrossRef]
- Pearlman, D.N.; Zierler, S.; Meersman, S.; Kim, H.K.; Viner-Brown, S.I.; Caron, C. Race disparities in childhood asthma: Does where you live matter? J. Natl. Med. Assoc. 2006, 98, 239–247. [Google Scholar]
- Kershaw, K.N.; Albrecht, S.S. Racial/ethnic residential segregation and cardiovascular disease risk. Curr. Cardiovasc. Risk Rep. 2015, 9, 10. [Google Scholar] [CrossRef]
- Bambra, C.; Robertson, S.; Kasim, A.; Smith, J.; Cairns-Nagi, J.M.; Copeland, A.; Finlay, N.; Johnson, K. Healthy land? An examination of the area-level association between brownfield land and morbidity and mortality in England. Environ. Plan. A 2014, 46, 433–454. [Google Scholar] [CrossRef]
- Wilson, S.M.; Fraser-Rahim, H.; Zhang, H.; Williams, E.M.; Samantapudi, A.V.; Ortiz, K.; Abara, W.; Sakati, W. The spatial distribution of leaking underground storage tanks in Charleston, South Carolina: An environmental justice analysis. Environ. Justice 2012, 5, 198–205. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Benzene. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp3.pdf (accessed on 19 January 2018).
- Currie, J.; Greenstone, M.; Moretti, E. Superfund cleanups and infant health. Am. Econ. Rev. 2011, 101, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Kouznetsova, M.; Huang, X.; Ma, J.; Lessner, L.; Carpenter, D.O. Increased rate of hospitalization for diabetes and residential proximity of hazardous waste sites. Environ. Health Perspect. 2007, 115, 75–79. [Google Scholar] [CrossRef]
- Lybarger, J.A.; Lee, R.; Vogt, D.P.; Perhac, R.M.; Spengler, R.F.; Brown, D.R. Medical costs and lost productivity from health conditions at volatile organic compound-contaminated superfund sites. Environ. Res. 1998, 79, 9–19. [Google Scholar] [CrossRef]
- Sergeev, A.V.; Carpenter, D.O. Increased hospitalizations for ischemic stroke with comorbid diabetes and residential proximity to sources of organic pollutants: A 12-year population-based study. Neuroepidemiology 2010, 35, 196–201. [Google Scholar] [CrossRef]
- Currie, J.; Schmieder, J.F. Fetal exposure to toxic releases and infant health. Am. Econ. Rev. 2009, 99, 177–183. [Google Scholar] [CrossRef]
- Legot, C.; London, B.; Shandra, J.; Rosofsky, A. Proximity to Industrial Releases of Toxins and Childhood Respiratory, Developmental, and Neurological Diseases: Environmental Ascription in East Baton Rouge Parish; Political Economy Research Institute: Amherst, MA, USA, 2011. [Google Scholar]
- Luo, J.; Hendryx, M.; Ducatman, A. Association between six environmental chemicals and lung cancer incidence in the United States. J. Environ. Public Health 2011, 2011, 463701. [Google Scholar] [CrossRef]
- Xing, Y.-F.; Xu, Y.-H.; Shi, M.-H.; Lian, Y.-X. The impact of PM2.5 on the human respiratory system. J. Thorac. Dis. 2016, 8, E69–E74. [Google Scholar]
- Scheers, H.; Jacobs, L.; Casas, L.; Nemery, B.; Nawrot, T.S. Long-term exposure to particulate matter air pollution is a risk factor for stroke: Meta-analytical evidence. Stroke 2015, 46, 3058–3066. [Google Scholar] [CrossRef]
- Ebisu, K.; Bell, M.L. Airborne PM2.5 chemical components and low birth weight in the Northeastern and Mid-Atlantic regions of the United States. Environ. Health Perspect. 2012, 120, 1746–1752. [Google Scholar] [CrossRef]
- Wang, J.; Xing, J.; Mathur, R.; Pleim, J.E.; Wang, S.; Hogrefe, C.; Gan, C.M.; Wong, D.C.; Hao, J. Historical trends in PM2.5-related premature mortality during 1990–2010 across the Northern Hemisphere. Environ. Health Perspect. 2017, 125, 400–408. [Google Scholar] [CrossRef]
- Kloog, I.; Coull, B.A.; Zanobetti, A.; Koutrakis, P.; Schwartz, J.D. Acute and chronic effects of particles on hospital admissions in New-England. PLoS ONE 2012, 7, e34664. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Health Assessment Document for Diesel Engine Exhaust; U.S. Environmental Protection Agency, Office of Research and Development, National Center for Environmental Assessment, Washington Office: Washington, DC, USA, 2002; EPA/600/8-90/057F.
- Xu, Y.; Barregard, L.; Nielsen, J.; Gudmundsson, A.; Wierzbicka, A.; Axmon, A.; Jönsson, B.A.; Kåredal, M.; Albin, M. Effects of diesel exposure on lung function and inflammation biomarkers from airway and peripheral blood of healthy volunteers in a chamber study. Part. Fibre Toxicol. 2013, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- McEntee, J.C.; Ogneva-Himmelberger, Y. Diesel particulate matter, lung cancer, and asthma incidences along major traffic corridors in MA, USA: A GIS analysis. Health Place 2008, 14, 817–828. [Google Scholar] [CrossRef]
- Silverman, D.T. Diesel exhaust causes lung cancer—Now what? Occup. Environ. Med. 2017, 74, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Kilbum, K.H. Effects of diesel exhaust on neurobehavioral and pulmonary functions. Arch. Environ. Health 2000, 55, 11–17. [Google Scholar]
- Brown, M.S.; Sarnat, S.E.; DeMuth, K.A.; Brown, L.A.S.; Whitlock, D.R.; Brown, S.W.; Tolbert, P.E.; Fitzpatrick, A.M. Residential proximity to a major roadway is associated with features of asthma control in children. PLoS ONE 2012, 7, e37044. [Google Scholar] [CrossRef]
- Brugge, D.; Durant, J.L.; Rioux, C. Near-highway pollutants in motor vehicle exhaust: A review of epidemiologic evidence of cardiac and pulmonary health risks. Environ. Health 2007, 6, 23. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.G.; deVos, A.J.B.M.; Pereira, G.; Jardine, A.; Weinstein, P. Use of a total traffic count metric to investigate the impact of roadways on asthma severity: A case-control study. Environ. Health 2011, 10, 52. [Google Scholar] [CrossRef]
- Hood, E. Dwelling disparities: How poor housing leads to poor health. Environ. Health Perspect. 2005, 113, A310–A317. [Google Scholar] [CrossRef]
- Agency for Toxic Substances & Disease Registry. Lead toxicity: Where is lead found? Available online: https://www.atsdr.cdc.gov/csem/csem.asp?csem=34&po=5 (accessed on 1 February 2018).
- Sanborn, M.D.; Abelsohn, A.; Campbell, M.; Weir, E. Identifying and managing adverse environmental health effects: 3. Lead exposure. Can. Med. Assoc. J. 2002, 166, 1287–1292. [Google Scholar]
- Maantay, J. Zoning, equity, and public health. Am. J. Public Health 2001, 91, 1033–1041. [Google Scholar] [Green Version]
- Wilson, S.; Hutson, M.; Mujahid, M. How planning and zoning contribute to inequitable development, neighborhood health, and environmental injustice. Environ. Justice 2008, 1, 211–216. [Google Scholar] [CrossRef]
- Wilson, S.M.; Heaney, C.D.; Cooper, J.; Wilson, O. Built environment issues in unserved and underserved African-American neighborhoods in North Carolina. Environ. Justice 2008, 1, 63–72. [Google Scholar] [CrossRef]
- Morenoff, J.D.; House, J.S.; Hansen, B.B.; Williams, D.R.; Kaplan, G.A.; Hunte, H.E. Understanding social disparities in hypertension prevalence, awareness, treatment, and control: The role of neighborhood context. Soc. Sci. Med. 2007, 65, 1853–1866. [Google Scholar] [CrossRef]
- Burdette, H.L.; Wadden, T.A.; Whitaker, R.C. Neighborhood safety, collective efficacy, and obesity in women with young children. Obesity 2006, 14, 518–525. [Google Scholar] [CrossRef]
- Mmari, K.; Lantos, H.; Blum, R.; Brahmbhatt, H.; Sangowawa, A.; Yu, C.; Delany-Moretlwe, S. A global study on the influence of neighborhood contextual factors on adolescent health. J. Adolesc. Health 2014, 55, S13–S20. [Google Scholar] [CrossRef]
- Pereira, G.; Wood, L.; Foster, S.; Haggar, F. Access to alcohol outlets, alcohol consumption and mental health. PLoS ONE 2013, 8, e53461. [Google Scholar] [CrossRef] [PubMed]
- Richardon, E.A.; Hill, S.E.; Mitchell, R.; Pearce, J.; Shortt, N.K. Is local alcohol outlet density related to alcohol-related morbidity and mortality in Scottish cities? Health Place 2015, 33, 172–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, C.A.; Hahn, R.A.; Elder, R.; Brewer, R.; Chattopadhyay, S.; Fielding, J.; Naimi, T.S.; Toomey, T.; Lawrence, B.; Middleton, J.C.; et al. The effectiveness of limiting alcohol density as a means of reducing excessive alcohol consumption and alcohol-related harms. Am. J. Prev. Med. 2009, 37, 556–569. [Google Scholar] [CrossRef]
- Oeder, S.; Kanashova, T.; Sippula, O.; Sapcariu, S.C.; Streibel, T.; Arteaga-Salas, J.M.; Passig, J.; Dilger, M.; Paur, H.R.; Schlager, C.; et al. Particulate matter from both heavy fuel oil and diesel fuel shipping emissions show strong biological effects on human lung cells at realistic and comparable in vitro exposure conditions. PLoS ONE 2015. [Google Scholar] [CrossRef]
- Peek, M.K.; Cutchin, M.P.; Freeman, D.; Stowe, R.P.; Goodwin, J.S. Environmental hazard and stress: Evidence from the Texax City Stress and Health Study. J. Epidemiol. Commun. Health 2009, 63, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Goldman, N.; Glei, D.A.; Seplaki, C.; Liu, I.W.; Weinstein, M. Perceived stress and phsyiological dysregulation in older adults. Stress 2005, 8, 95–105. [Google Scholar] [CrossRef]
- Chakraborty, J.; Collins, T.W.; Grineski, S.E.; Maldonado, A. Racial differences in perceptions of air pollution health risk: Does environmental exposure matter? Int. J. Environ. Res. Public Health 2017, 14, 116. [Google Scholar] [CrossRef] [PubMed]
- Harrell, J.P.; Hall, S.; Taliaferro, J. Physiological responses to racism and discrimination: An assessment of the evidence. Am. J. Public Health 2003, 93, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.; Anderson, N.B.; Clark, V.R.; Williams, D.R. Racism as a stressor for African Americans. Am. Psychol. 1999, 54, 805–816. [Google Scholar] [CrossRef]
- Hutson, M.A.; Wilson, S. The role of community-based strategies in addressing metropolitan segrgation and racial health disparities. Community Dev. J. 2011, 42, 476–493. [Google Scholar] [CrossRef]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of physical activity in the relationship between urban green space and health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization-Europe. Urban Green Spaces and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Lee, A.C.K.; Jordan, H.C.; Horsley, J. Value of urban green spaces in promoting healthy living and wellbeing: Prospects for planning. Risk Manag. Healthc. Policy 2015, 8, 131–137. [Google Scholar] [CrossRef]
- Astell-Bur, T.; Feng, X.; Kolt, G.S. Green space is associated with walking and moderate-to-vigorous physical activity (MVPA) in middle-to-older-aged-adults: Findings from 203 883 Australians in the 45 and up study. Br. J. Sport Med. 2014, 48, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Manson, J.E.; Lee, I.-M.; Cole, S.R.; Hennekens, C.H.; Willett, W.C.; Buring, J.E. Fruit and vegetable intake and risk of cardiovascular disease: The women’s health study. Am. J. Clin. Nutr. 2000, 72, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, E.B.; Forman, J.P. Fruit and vegetable consumption and the incidence of hypertension in three prospective cohort studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef]
- Rohe, W.M.; Lindblad, M. Reexamining the Social Benefits of Homeownership after the Housing Crisis; Brookings Institution Press: Washington, DC, USA, 2014. [Google Scholar]
- Ni, J.; Decker, C. The impact of homeownership on criminal activity: Empirical evidence from United States’ county level data. Econ. Bus. J. Inq. Perspect. 2009, 2, 17–37. [Google Scholar]
- Chang, C.-H.; Stukel, T.A.; Flood, A.B.; Goodman, D.C. Primary care physician workforce and medicare beneficiaries’ health outcomes. JAMA 2011, 305, 2096–2104. [Google Scholar] [CrossRef] [PubMed]
- Shi, L. The impact of primary care: A focused review. Scientifica 2012, 2012, 432892. [Google Scholar] [CrossRef]
- World Health Organization. Promoting Mental Health. Available online: http://www.who.int/mental_health/evidence/en/promoting_mhh.pdf (accessed on 1 February 2018).
- Sommers, B.D.; Gawande, A.A.; Baicker, K. Health insurance coverage and health—What the recent evidence tells us. N. Engl. J. Med. 2017, 377, 586–593. [Google Scholar] [CrossRef]
- Woolhandler, S.; Himmelstein, D.U. The relationship of health insurance and mortality: Is lack of insurance deadly? Ann. Intern. Med. 2017, 167, 424–431. [Google Scholar] [CrossRef]
- Ozbay, F.; Johnson, D.C.; Dimoulas, E.; Morgan, C.A., III; Charney, D.; Southwick, S. Social support and resilience to stress: From neurobiology to clinical practice. Psychiatry 2007, 4, 35–40. [Google Scholar] [PubMed]
- Dalton, A.M.; Jones, A.P.; Panter, J.R.; Ogilvie, D. Neighbourhood, route and workplace-related environmental characteristics predict adults’ mode of travel to work. PLoS ONE 2013, 8, e67575. [Google Scholar] [CrossRef] [PubMed]
- Victoria Transport Policy Institute. Evaluating Public Transportation Health Benefits. Available online: http://www.apta.com/resources/reportsandpublications/Documents/APTA_Health_Benefits_Litman.pdf (accessed on 1 February 2018).
- Litman, T. Transportation and public health. Annu. Rev. Public Health 2013, 34, 217–233. [Google Scholar] [CrossRef] [PubMed]
- The National Academies. Disaster Resilience. A National Imperative; The National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Burwell-Naney, K.; Wilson, S.M.; He, X.; Sapkota, A.; Puett, R. Development of a cumulative stressors and resiliency index to ecamine environmental health risk: A South Carolina assessment. Environ. Justice 2018, 11, 165–175. [Google Scholar] [CrossRef]
- Bromley, E.; Eisenman, D.P.; Magana, A.; Williams, M.; Kim, B.; McCreary, M.; Chandra, A.; Wells, K.B. How do communities use a participatory public health approach to build resilience? The Los Angeles County community disaster resilience project. Int. J. Environ. Res. Public Health 2017, 14, 1267. [Google Scholar] [CrossRef]
- Keegan, R.; Grover, L.T.; Patron, D.; Sugarman, O.K.; Griffith, K.; Sonnier, S.; Springgate, B.F.; Jumonville, L.C.; Gardner, S.; Massey, W.; et al. Case study of resilient Baton Rouge: Applying depression collaborative care and community planning to disaster recovery. Int. J. Environ. Res. Public Health 2018, 15, 1208. [Google Scholar] [CrossRef]
- Kennedy, M.; Gonick, S.; Meischke, H.; Rios, J.; Errett, N.A. Building back better: Local health department engagement and integration of health promotion and Hurricane Harvey recovery planning and implementation. Int. J. Environ. Res. Public Health 2019, 16, 299. [Google Scholar] [CrossRef]
- California Environmental Justice Alliance. Green Zones. Available online: https://caleja.org/what-we-do/greenzones/ (accessed on 4 February 2018).

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burwell-Naney, K.; Wilson, S.M.; Whitlock, S.T.; Puett, R. Hybrid Resiliency-Stressor Conceptual Framework for Informing Decision Support Tools and Addressing Environmental Injustice and Health Inequities. Int. J. Environ. Res. Public Health 2019, 16, 1466. https://doi.org/10.3390/ijerph16081466
Burwell-Naney K, Wilson SM, Whitlock ST, Puett R. Hybrid Resiliency-Stressor Conceptual Framework for Informing Decision Support Tools and Addressing Environmental Injustice and Health Inequities. International Journal of Environmental Research and Public Health. 2019; 16(8):1466. https://doi.org/10.3390/ijerph16081466
Chicago/Turabian StyleBurwell-Naney, Kristen, Sacoby M. Wilson, Siobhan T. Whitlock, and Robin Puett. 2019. "Hybrid Resiliency-Stressor Conceptual Framework for Informing Decision Support Tools and Addressing Environmental Injustice and Health Inequities" International Journal of Environmental Research and Public Health 16, no. 8: 1466. https://doi.org/10.3390/ijerph16081466
APA StyleBurwell-Naney, K., Wilson, S. M., Whitlock, S. T., & Puett, R. (2019). Hybrid Resiliency-Stressor Conceptual Framework for Informing Decision Support Tools and Addressing Environmental Injustice and Health Inequities. International Journal of Environmental Research and Public Health, 16(8), 1466. https://doi.org/10.3390/ijerph16081466