A Pilot Study to Test the Feasibility of a Home Mobility Monitoring System in Community-Dwelling Older Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
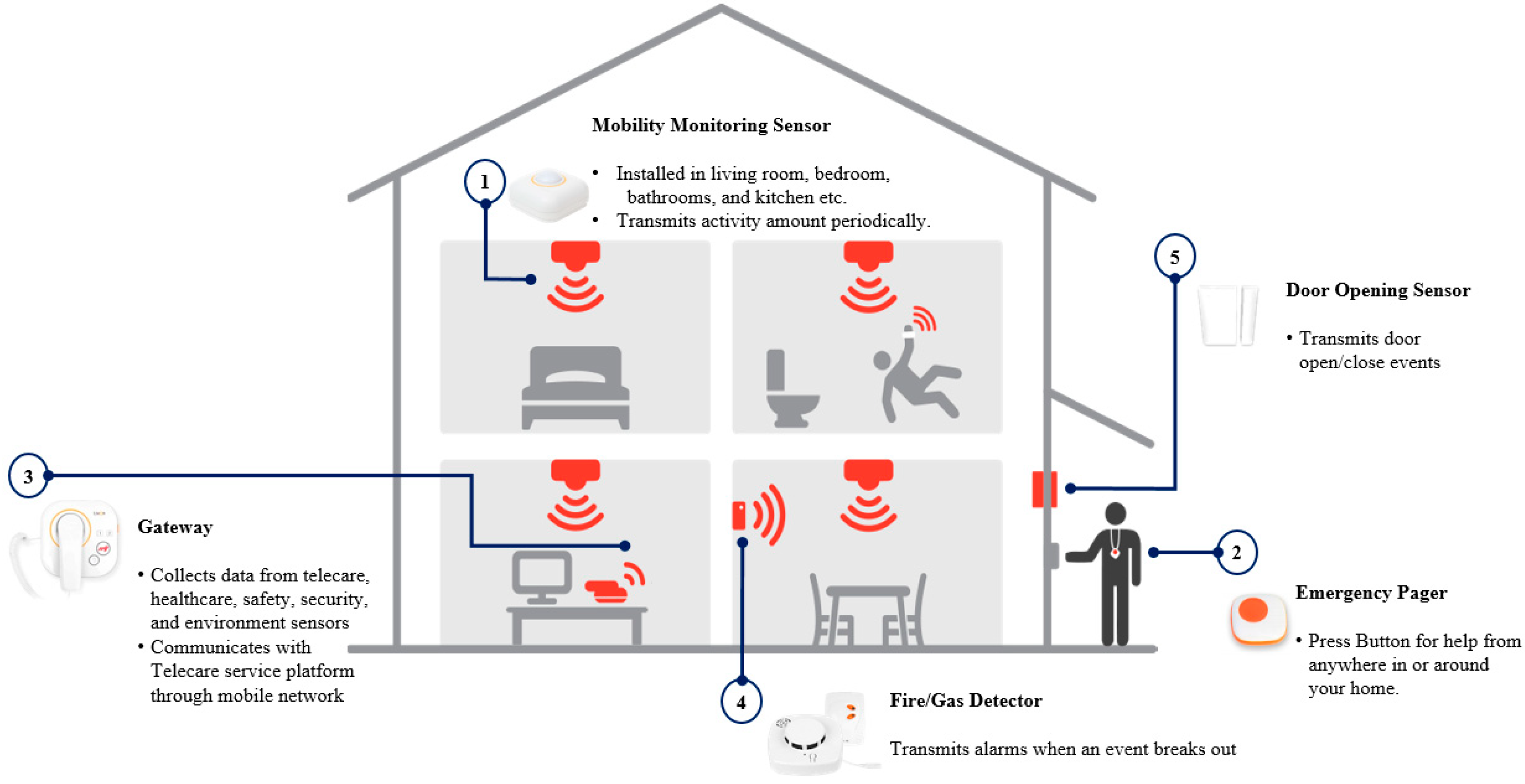
2.2. Data Collection Via the Home Mobility Monitoring System
2.3. Data Analysis
2.4. Evaluation of Adaptability
3. Results
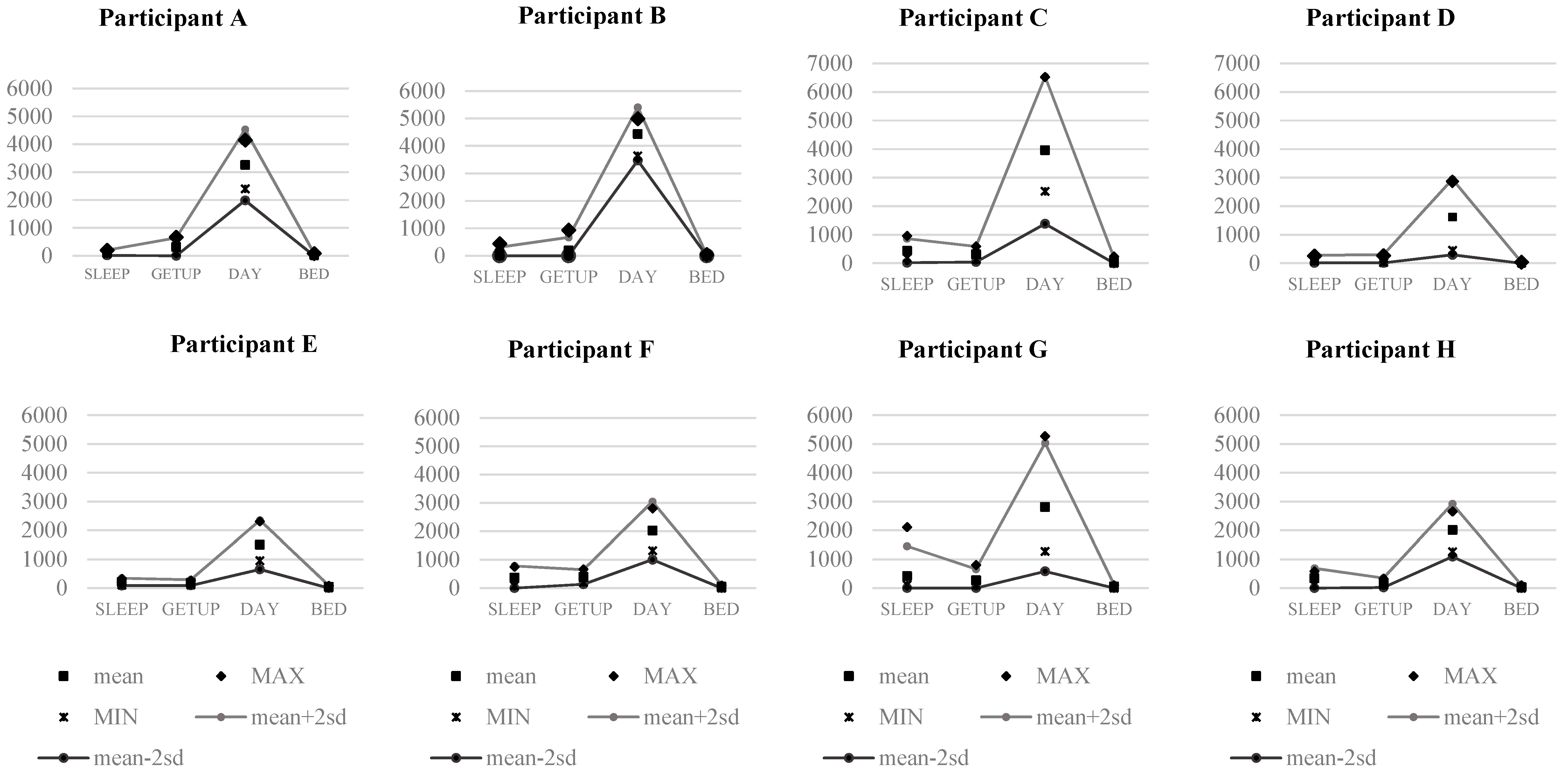
3.1. Identification of Daily Indoor Activity
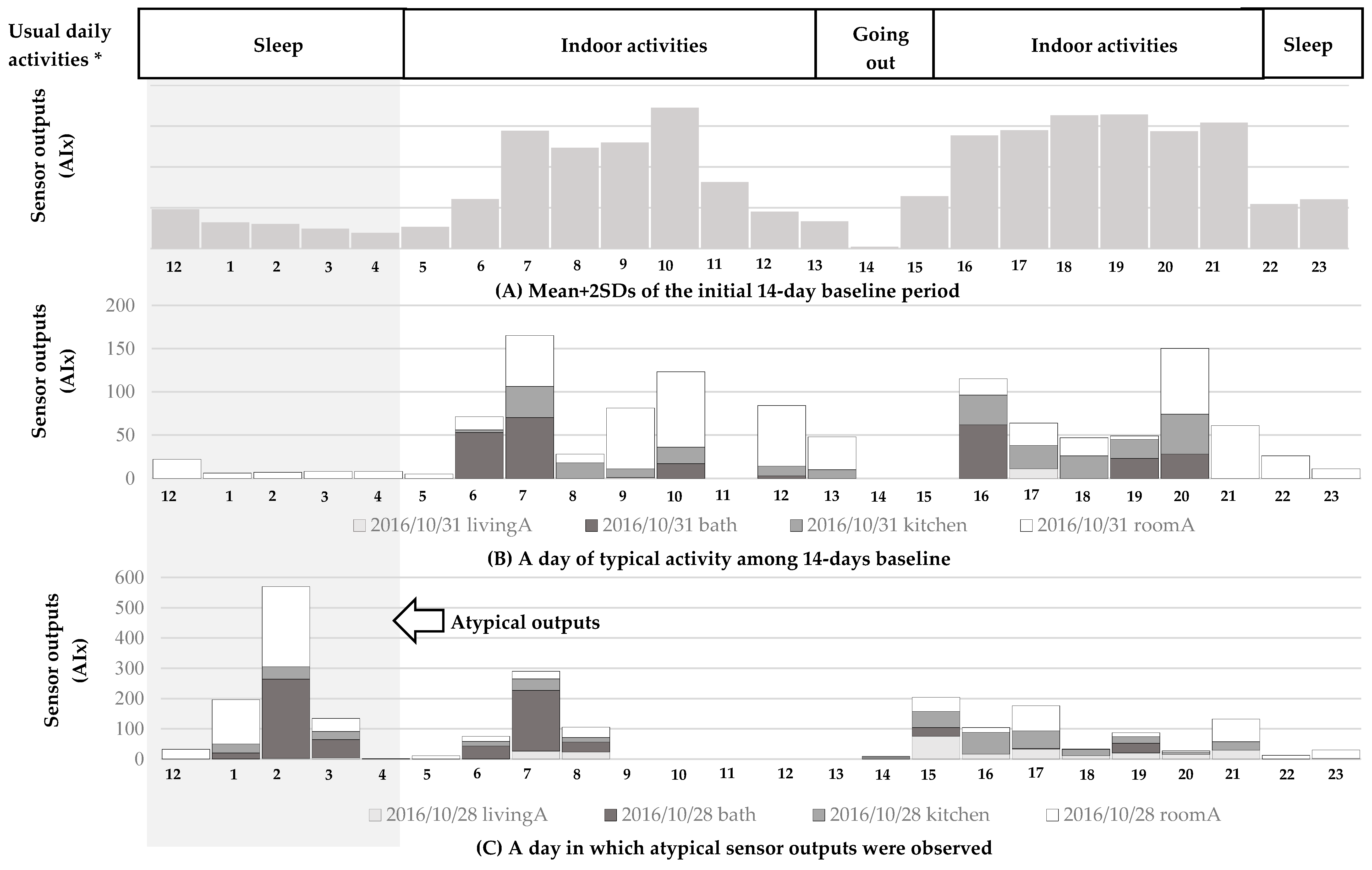
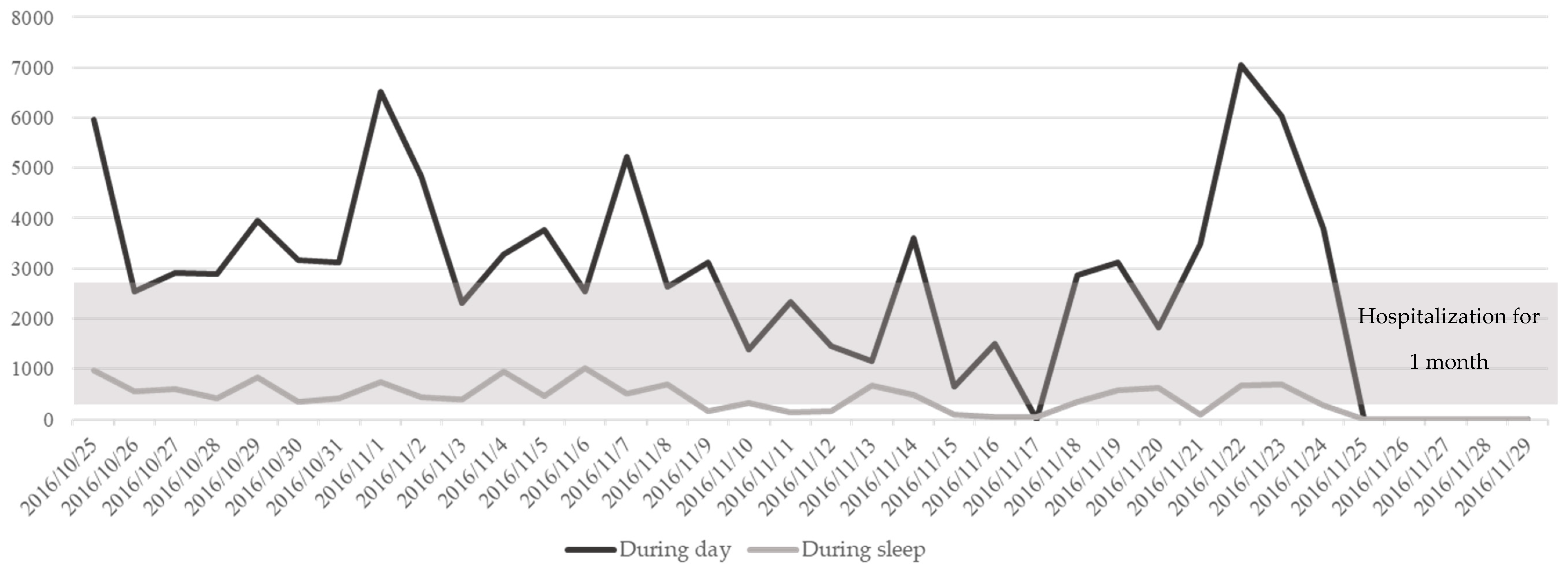
3.2. Determination of Atypical Patterns
3.3. Adaptability of the System to Participants: Satisfaction and Perceived Usefulness
3.4. Adaptability of the System Use from Visiting Nurses: Expectations of Usefulness
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ministry of the Interior and Safety. Resident Population in Five-Year Age Groups (2011~). 2017. Available online: http://kosis.kr/eng/statisticslist/statisticslist_01list.jsp?vwcd=mt_etitle&parentid=a#subcont (accessed on 19 September 2018).
- Statistics Korea. Population and Housing Census. 2017. Available online: http://kostat.go.kr/portal/eng/pressReleases/8/7/index.board?bmode=read&bSeq=&aSeq=370993&pageNo=1&rowNum=10&navCount=10&currPg=&sTarget=title&sTxt= (accessed on 12 December 2018).
- Do, Y.K.; Malhotra, C. The effect of coresidence with an adult child on depressive symptoms among older widowed women in South Korea: An instrumental variables estimation. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 384–391. [Google Scholar] [CrossRef]
- Fortin, M.; Hudon, C.; Haggerty, J.; van den Akker, M.; Almirall, J. Prevalence estimates of multimorbidity: A comparative study of two sources. BMC Health Serv. Res. 2010, 10, 111. [Google Scholar] [CrossRef]
- Ng, T.P.; Jin, A.; Feng, L.; Nyunt, M.S.Z.; Chow, K.Y.; Feng, L.; Fong, N.P. Mortality of older persons living alone: Singapore Longitudinal Ageing Studies. BMC Geriatr. 2015, 15, 126. [Google Scholar] [CrossRef]
- Mitzner, T.L.; Beer, J.M.; McBride, S.E.; Rogers, W.A.; Fisk, A.D. Older adults’ needs for home health care and the potential for human factors interventions. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting; Sage: Los Angeles, CA, USA, 2009; Volume 53, pp. 718–722. [Google Scholar]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The meaning of “Aging in Place” to older people. Gerontologist 2011, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Hood, L.; Friend, S.H. Predictive, personalized, preventive, participatory (P4) cancer medicine. Nat. Rev. Clin. Oncol. 2011, 8, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Charness, N.; Demiris, G.; Krupinski, E.A. Designing Telehealth for an Aging Population: A Human Factors Perspective; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Sun, W.; Doran, D. Using remote activity monitoring and guideline system for home care clients to support geriatric nursing care in the community. J. Nurs. Health Care 2014, 1, 123–129. [Google Scholar] [CrossRef]
- Schmitter-Edgecombe, M.; Parsey, C.; Lamb, R. Development and psychometric properties of the Instrumental Activities of Daily Living: Compensation Scale. Arch. Clin. Neuropsychol. 2014, 29, 776–792. [Google Scholar] [CrossRef]
- Scanaill, C.N.; Ahearne, B.; Lyons, G.M. Long-term telemonitoring of mobility trends of elderly people using SMS messaging. IEEE Trans. Inform. Technol. Biomed. 2006, 10, 412–413. [Google Scholar] [CrossRef]
- Bae, H.; Kim, J. Estimating need for home visiting nurse from public health centers. Perspect. Nurs. Sci. 2015, 12, 23–32. [Google Scholar] [CrossRef]
- National Law Information Center. Regional Public Health Act. Available online: http://www.law.go.kr/eng/engLsSc.do?menuId=2&query=REGIONAL%20PUBLIC%20HEALTH%20ACT#liBgcolor0 (accessed on 16 August 2018).
- Dean-Baar, S.; Murray, M.E.; Acord, L.; Henriques, J. Wisconsin Registered Nurse Survey 2010: Report. Wisconsin Center for Nursing. Available online: http://www.wisconsincenterfornursing.org/2010_wi_survey_analysis_report.html (accessed on 15 August 2018).
- Young, S.; Acord, L.; Schuler, S.; Hansen, J.M. Addressing the community/public health nursing shortage through a multifaceted regional approach. Publ. Health Nurs. 2014, 31, 566–573. [Google Scholar] [CrossRef]
- Park, Y.S.; Park, K.Y.; Kim, M.S.; Lee, S.Y.; Seo, J. Analysis of activities of daily living for silver generations with an IoT-based telecare system. J. Adv. Navig. Technol. 2015, 19, 6. [Google Scholar] [CrossRef]
- Suzuki, R.; Otake, S.; Izutsu, T.; Yoshida, M.; Iwaya, T. Monitoring daily living activities of elderly people in a nursing home using an infrared motion-detection system. Telemed. J. E Health 2006, 12, 146–155. [Google Scholar] [CrossRef]
- De Wit, N.J.; Schuurmans, M.J. Future care for older people in general practice: Paradigm shifts are needed. Br. J. Gen. Pract. 2017, 67, 500–501. [Google Scholar] [CrossRef]
- Charness, N.; Best, R.; Evans, J. Supportive home health care technology for older adults: Attitudes and implementation. Gerontechnology 2016, 15, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farina, N.; Lowry, R.G. Older adults’ satisfaction of wearing consumer-level activity monitors. J. Rehabil. Assist. Technol. Eng. 2017, 4, 1–6. [Google Scholar] [CrossRef]
- Preusse, K.C.; Mitzner, T.L.; Fausset, C.B.; Rogers, W.A. Older adults’ acceptance of activity trackers. J. Appl. Gerontol. 2017, 36, 127–155. [Google Scholar] [CrossRef]
- Schlomann, A. A case study on older adults’ long-term use of an activity tracker. Gerontechnology 2017, 16, 115–124. [Google Scholar] [CrossRef]
- Seifert, A.; Schlomann, A.; Rietz, C.; Schelling, H.R. The use of mobile devices for physical activity tracking in older adults’ everyday life. Digit. Health 2017, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bashshur, R.L.; Shannon, G.W.; Krupinski, E.A.; Grigsby, J.; Kvedar, J.C.; Weinstein, R.S.; Tracy, J. National telemedicine initiatives: Essential to healthcare reform. Telemed. J. E Health 2009, 15, 600–610. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2010, 3, E20. [Google Scholar] [CrossRef]
- Kuutti, J.; Blomqvist, K.H.; Sepponen, R.E. Evaluating of visitor counting technologies and their energy saving potential through demand-controlled ventilation. Energies 2014, 7, 1685–1705. [Google Scholar] [CrossRef]
- Bauer, D.; Brändle, N.; Seer, S.; Ray, M.; Kitazawa, K. Measurement of pedestrian movements: A comparative study on various existing systems. In Pedestrian Behavior; Timmermans, H., Ed.; Emerald Group Publishing Limited: Bingley, UK, 2009; pp. 325–344. [Google Scholar]
- Medical Advisory Secretariat. Social isolation in community-dwelling seniors: An evidence-based analysis. ONT Health Technol. Assess. Ser. 2008, 8, 1–49. [Google Scholar]
- Robertson, K. Mindful use of health information technology. Virtual Mentor 2011, 13, 193–196. [Google Scholar]
- Ossig, C.; Antonini, A.; Buhmann, C.; Classen, J.; Csoti, I.; Falkenburger, B.; Storch, A. Wearable sensor-based objective assessment of motor symptoms in Parkinson’s disease. J. Neural Transm. 2016, 123, 57–64. [Google Scholar] [CrossRef]
- Pan, D.; Dhall, R.; Lieberman, A.; Petitti, D.B. A mobile cloud-based Parkinson’s disease assessment system for home-based monitoring. JMIR mHealth uHealth 2015, 3, e29. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson’s disease: A pilot randomized controlled trial. Parkinsonism. Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and Parkinson’s disease: Toward clinical and at home use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef]
- Godinho, C.; Domingos, J.; Cunha, G.; Santos, A.T.; Fernandes, R.M.; Abreu, D.; Ferreira, J.J. A systematic review of the characteristics and validity of monitoring technologies to assess Parkinson’s disease. J. Neuroeng. Rehabil. 2016, 13, 24. [Google Scholar] [CrossRef]
- Ferreira, J.J.; Godinho, C.; Santos, A.T.; Domingos, J.; Abreu, D.; Lobo, R.; Maetzler, W. Quantitative home-based assessment of Parkinson’s symptoms: The SENSE-PARK feasibility and usability study. BMC Neurol. 2015, 15, 89. [Google Scholar] [CrossRef]
- Mactier, K.; Lord, S.; Godfrey, A.; Burn, D.; Rochester, L. The relationship between real world ambulatory activity and falls in incident Parkinson’s disease: Influence of classification scheme. Parkinsonism Relat. Disord. 2015, 21, 236–242. [Google Scholar] [CrossRef]
- Rantanen, T. Promoting mobility in older people. J. Prev. Med. Publ. Health 2013, 46, S50–S54. [Google Scholar] [CrossRef]
- Cavanaugh, J.T.; Ellis, T.D.; Earhart, G.M.; Ford, M.P.; Foreman, K.B.; Dibble, L.E. Toward understanding ambulatory activity decline in Parkinson disease. Phys. Ther. 2015, 95, 1142–1150. [Google Scholar] [CrossRef]
- Raknim, P.; Lan, K.C. Gait monitoring for early neurological disorder detection using sensors in a smartphone: Validation and a case study of Parkinsonism. Telemed. J. E Health 2016, 22, 75–81. [Google Scholar] [CrossRef]
- Stack, E.; King, R.; Janko, B.; Burnett, M.; Hammersley, N.; Agarwal, V.; Ashburn, A. Could in-home sensors surpass human observation of people with Parkinson’s at high risk of falling? An ethnographic study. BioMed Res. Int. 2016, 2016, 3703745. [Google Scholar] [CrossRef]
- Suzuki, R.; Ogawa, M.; Otake, S.; Izutsu, T.; Tobimatsu, Y.; Izumi, S.; Iwaya, T. Analysis of activities of daily living in elderly people living alone: Single-subject feasibility study. Telemed. J. E Health 2004, 10, 260–276. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- While, A.; Dewsbury, G. Nursing and information and communication technology (ICT): A discussion of trends and future directions. Int. J. Nurs. Stud. 2011, 48, 1302–1310. [Google Scholar] [CrossRef]
- Saba, V.; McCormick, K. Essentials of Nursing Informatics, 4th ed.; McGraw Hill: New York, NY, USA, 2006. [Google Scholar]
- Holden, R.J.; Karsh, B. The technology acceptance model: Its past and its future in health care. J. Biomed. Inform. 2010, 43, 159–172. [Google Scholar] [CrossRef]
- Kuo, K.M.; Liu, C.F.; Ma, C.C. An investigation of the effect of nurses’ technology readiness on the acceptance of mobile electronic medical record systems. BMC Med. Inform. Decis. Mak. 2013, 13, 88. [Google Scholar] [CrossRef]
- Daly, J.M.; Buckwalter, K.; Maas, M. Written and computerized care plans. Organizational processes and effect on patient outcomes. J. Gerontol Nurs. 2002, 28, 14–23. [Google Scholar] [CrossRef]
- Ammenwerth, E.; Mansmann, U.; Iller, C.; Eichstädter, R. Factors affecting and affected by user acceptance of computer-based nursing documentation: Results of a two-year study. J. Am. Med. Inform. Assoc. 2003, 10, 69–84. [Google Scholar] [CrossRef]
- Nemeth, C.; O’Connor, M.; Cook, R.; Wears, R.; Perry, S. Crafting information technology solutions, not experiments, for the emergency department. Acad. Emerg. Med. 2014, 11, 1114–1117. [Google Scholar] [CrossRef]
- Falck, R.S.; Landry, G.J.; Brazendale, K.; Liu-Ambrose, T. Measuring physical activity in older adults using motionwatch 8 actigraphy: How many days are needed? J. Aging Phys. Act. 2017, 25, 51–57. [Google Scholar] [CrossRef]
- Kharicha, K.; Iliffe, S.; Harari, D.; Swift, C.; Gillmann, G.; Stuck, A.E. Health risk appraisal in older people 1: Are older people living alone an “at-risk” group? Br. J. Gen. Pract. 2007, 57, 271–276. [Google Scholar]
- Kanning, M.; Schlicht, W. A bio-psycho-social model of successful aging as shown through the variable “physical activity”. Eur. Rev. Aging Phys. Act. 2008, 5, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Reed, K. Telemedicine: Benefits to advanced practice nursing and the communities they serve. J. Am. Acad. Nurse Pract. 2005, 17, 176–180. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | A | B | C | D | E | F | G | H |
|---|---|---|---|---|---|---|---|---|
| Sex/Age, years | F/87 | F/69 | F/93 | M/89 | F/81 | F/79 | F/74 | F/71 |
| Comorbidities | Hypertension Cancer Arthritis | Cancer Asthma | - | - | Diabetes Cancer | Hypertension Diabetes Heart disease | Hypertension | Hypertension Diabetes Cerebrovascular disease Cancer |
| Housing | Studio apartment | Studio apartment | Apartment | Studio apartment | Apartment | Studio apartment | Studio apartment | Apartment |
| Number of rooms * | 2 | 2 | 4 | 2 | 4 | 2 | 2 | 3 |
| Location of sensors | Bedroom Bathroom | Bedroom Bathroom | Bedroom Bathroom Living room Kitchen | Bedroom Bathroom | Bedroom Bathroom Living room Kitchen | Bedroom Bathroom | Bedroom Bathroom | Bedroom Bathroom Livingroom (Kitchen) |
| Bedroom is separate? | No | No | Yes | No | Yes | No | No | Yes |
| Sleep on the bed? | No | No | Yes | No | Yes | No | No | No |
| Chair or couch in the living room? | No | No | No | No | Yes | No | No | No |
| Table and chairs in the kitchen or dining room? | Yes | No | No | No | Yes | No | No | Yes |
| Washstand is installed in the bathroom? | No | Yes | No | No | Yes | No | No | No |
| Bedtime | 21:00 | 23:00 | 21:00 | 18:00 | 22:00 | 21:00 | 23:00 | 22:00 |
| Waking time | 07:00 | 05:00 | 05:00 | 05:00 | 06:30 | 08:00 | 08:00 | 08:00 |
| Sleep duration | 7 h | 5 h | 7 h | 10 h | 8 h | 10 h | 8 h | 9 h |
| Quality of sleep | Fair | Good | Fair | Fair | Fair | Fair | Good | Fair |
| Awaken during sleep | Everyday, Not specified times | Not at all | Every day, Not specified times | Every day, 1–2 times/night | Every day, every 2 h | Every day, 1–5 times/night | Sometimes, 1 time/night | Almost every day, 1–3 times |
| Take a nap | Not at all | Not at all | Everyday | Not at all | Sometimes | Not at all | Not at all | Not at all |
| Physical condition | Fair | Fair | Good | Good | Fair | Fair | Good | Fair |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, H.; Kim, H. A Pilot Study to Test the Feasibility of a Home Mobility Monitoring System in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 1512. https://doi.org/10.3390/ijerph16091512
Son H, Kim H. A Pilot Study to Test the Feasibility of a Home Mobility Monitoring System in Community-Dwelling Older Adults. International Journal of Environmental Research and Public Health. 2019; 16(9):1512. https://doi.org/10.3390/ijerph16091512
Chicago/Turabian StyleSon, Heesook, and Hyerang Kim. 2019. "A Pilot Study to Test the Feasibility of a Home Mobility Monitoring System in Community-Dwelling Older Adults" International Journal of Environmental Research and Public Health 16, no. 9: 1512. https://doi.org/10.3390/ijerph16091512
APA StyleSon, H., & Kim, H. (2019). A Pilot Study to Test the Feasibility of a Home Mobility Monitoring System in Community-Dwelling Older Adults. International Journal of Environmental Research and Public Health, 16(9), 1512. https://doi.org/10.3390/ijerph16091512