Correlations between Mortality-to-Incidence Ratios and Health Care Disparities in Testicular Cancer

 ,
, 
 and
and 
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Incidence and Mortality in Testicular Cancer Are Higher in More-Developed Regions than in Less-Developed Regions
3.2. The Mortality-to-Incidence Ratios for Prostate and Testicular Cancer Are High in Less-Developed Regions
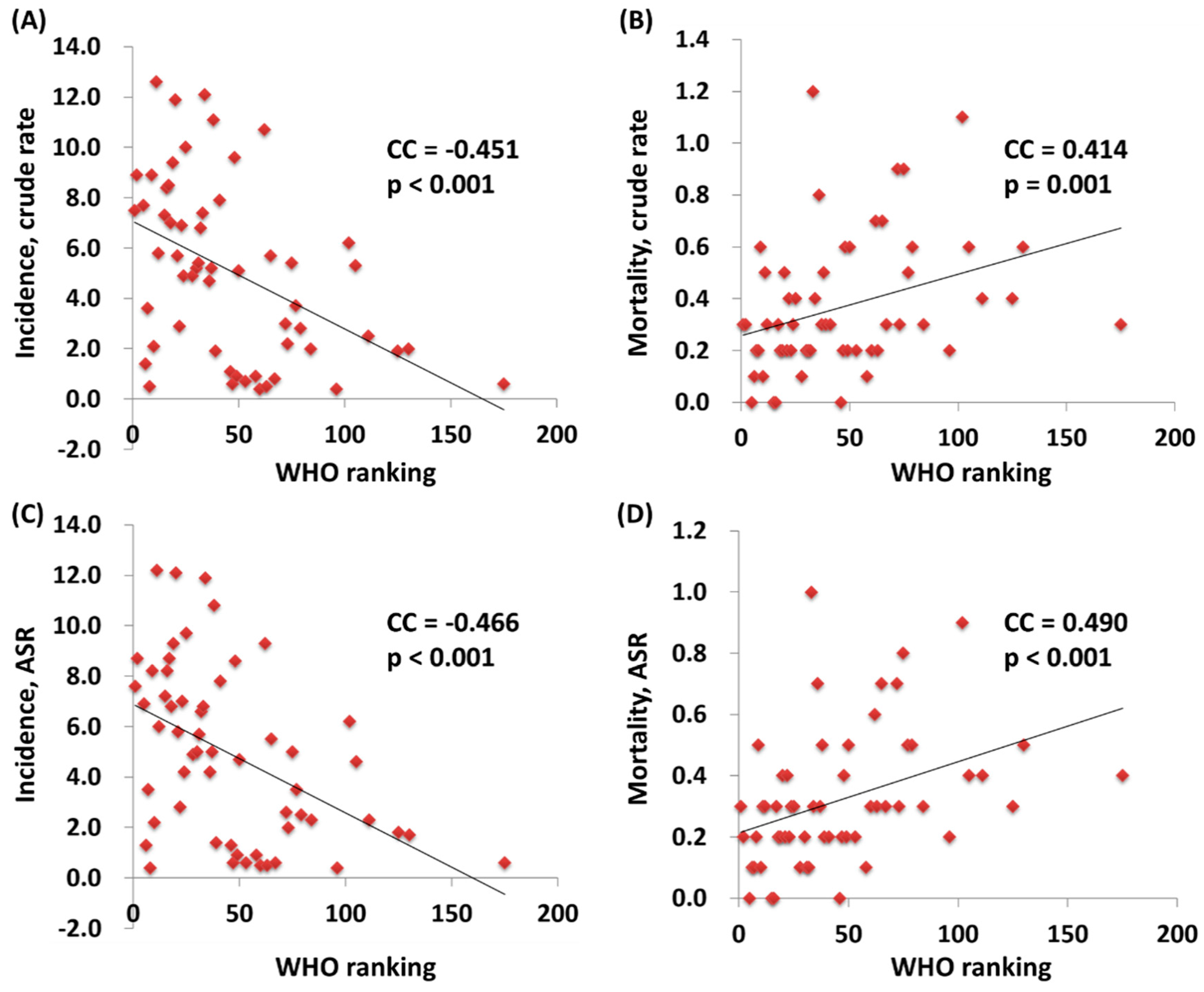
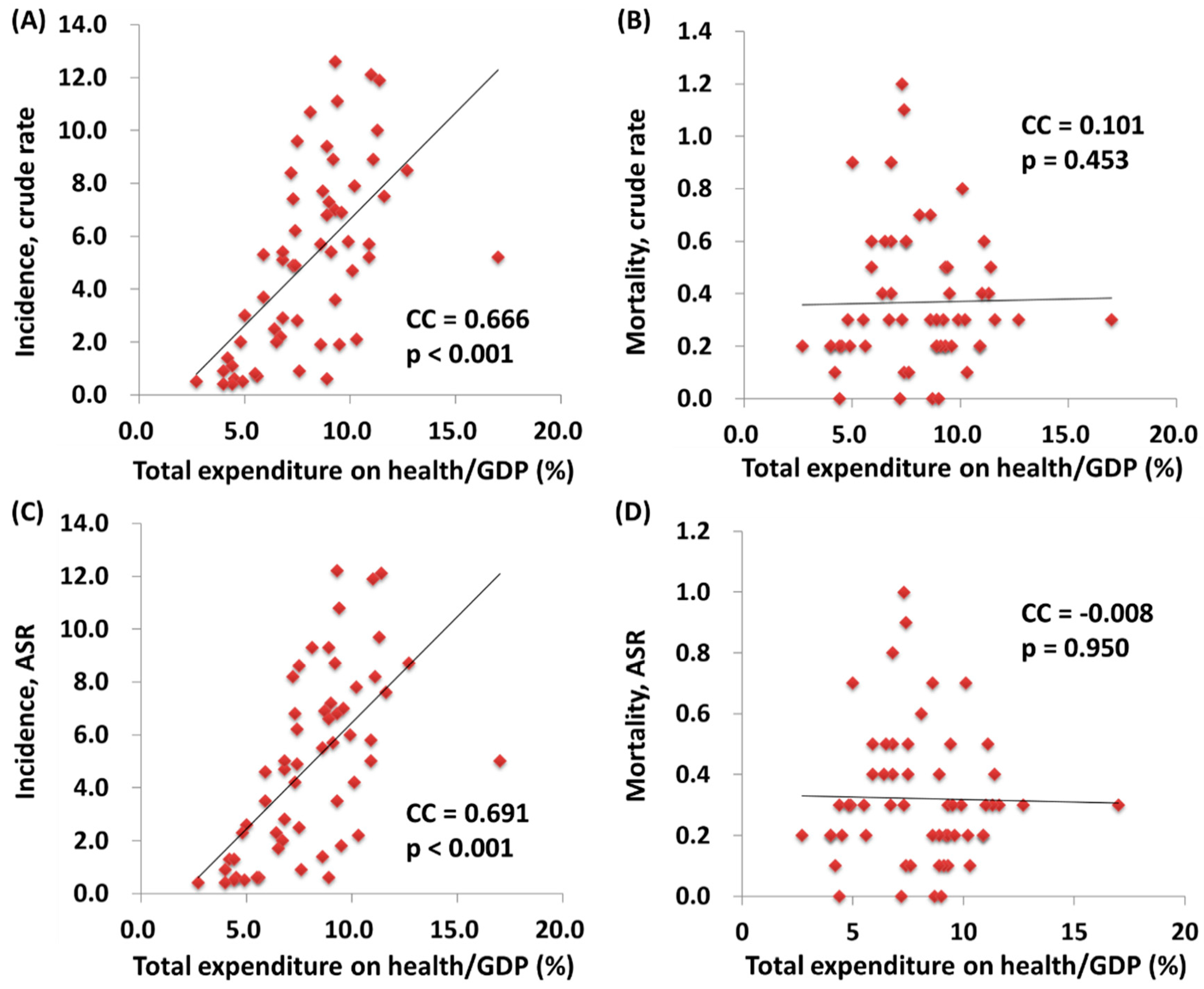
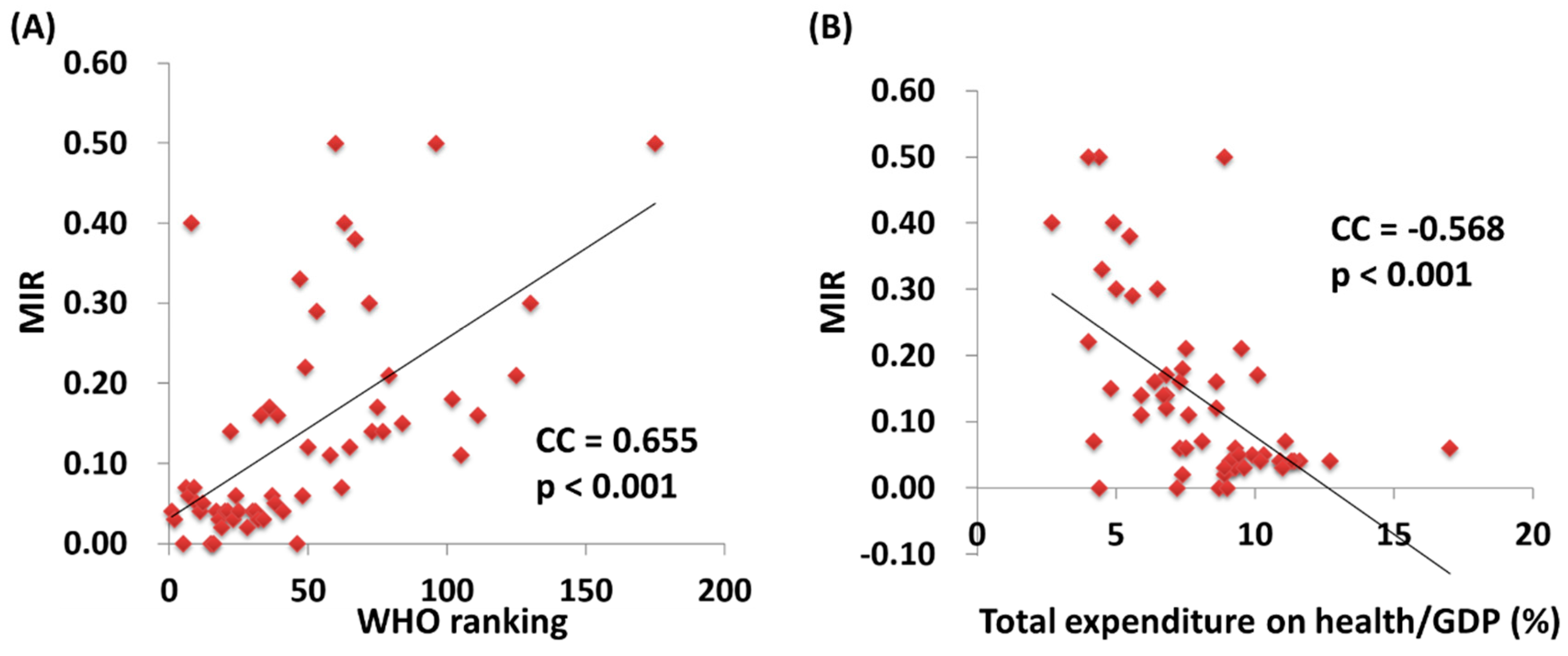
3.3. A Country’s World Health Organization Ranking and Total Expenditure on Health/Gdp Have a Significant Association with Its Mortality-to-Incidence Ratio for Testicular Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ASR | age-standardized rate |
| CC | correlation coefficient |
| e/GDP | total expenditures on health/gross domestic product |
| MIR | mortality-to-incidence ratio |
| WHO | World Health Organization |
References
- Znaor, A.; Lortet-Tieulent, J.; Jemal, A.; Bray, F. International variations and trends in testicular cancer incidence and mortality. Eur. Urol. 2014, 65, 1095–1106. [Google Scholar] [CrossRef] [PubMed]
- Shanmugalingam, T.; Soultati, A.; Chowdhury, S.; Rudman, S.; Van Hemelrijck, M. Global incidence and outcome of testicular cancer. Clin. Epidemiol. 2013, 5, 417–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledano, M.B.; Jarup, L.; Best, N.; Wakefield, J.; Elliott, P. Spatial variation and temporal trends of testicular cancer in Great Britain. Br. J. Cancer 2001, 84, 1482–1487. [Google Scholar] [CrossRef] [Green Version]
- Le Cornet, C.; Lortet-Tieulent, J.; Forman, D.; Beranger, R.; Flechon, A.; Fervers, B.; Schuz, J.; Bray, F. Testicular cancer incidence to rise by 25% by 2025 in Europe? Model-based predictions in 40 countries using population-based registry data. Eur. J. Cancer 2014, 50, 831–839. [Google Scholar] [CrossRef]
- Hanna, N.H.; Einhorn, L.H. Testicular cancer—Discoveries and updates. N. Engl. J. Med. 2014, 371, 2005–2016. [Google Scholar] [CrossRef] [Green Version]
- Trama, A.; Foschi, R.; Larranaga, N.; Sant, M.; Fuentes-Raspall, R.; Serraino, D.; Tavilla, A.; Van Eycken, L.; Nicolai, N. Survival of male genital cancers (prostate, testis and penis) in Europe 1999–2007: Results from the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2206–2216. [Google Scholar] [CrossRef]
- Richiardi, L.; Vizzini, L.; Pastore, G.; Segnan, N.; Gillio-Tos, A.; Fiano, V.; Grasso, C.; Ciuffreda, L.; Lista, P.; Pearce, N.; et al. Lifetime growth and risk of testicular cancer. Int. J. Cancer 2014, 135, 695–701. [Google Scholar] [CrossRef]
- Rosen, A.; Jayram, G.; Drazer, M.; Eggener, S.E. Global trends in testicular cancer incidence and mortality. Eur. Urol. 2011, 60, 374–379. [Google Scholar] [CrossRef]
- Fossa, S.D.; Cvancarova, M.; Chen, L.; Allan, A.L.; Oldenburg, J.; Peterson, D.R.; Travis, L.B. Adverse prognostic factors for testicular cancer-specific survival: A population-based study of 27,948 patients. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 963–970. [Google Scholar] [CrossRef]
- Sui, W.; Morrow, D.C.; Bermejo, C.E.; Hellenthal, N.J. Trends in Testicular Cancer Survival: A Large Population-based Analysis. Urology 2015, 85, 1394–1398. [Google Scholar] [CrossRef]
- Chalya, P.L.; Simbila, S.; Rambau, P.F. Ten-year experience with testicular cancer at a tertiary care hospital in a resource-limited setting: A single centre experience in Tanzania. World J. Surg. Oncol. 2014, 12, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebert, J.R.; Daguise, V.G.; Hurley, D.M.; Wilkerson, R.C.; Mosley, C.M.; Adams, S.A.; Puett, R.; Burch, J.B.; Steck, S.E.; Bolick-Aldrich, S.W. Mapping cancer mortality-to-incidence ratios to illustrate racial and sex disparities in a high-risk population. Cancer 2009, 115, 2539–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, L.C.; Neri, A.J.; Tai, E.; Glenn, J.D. Testicular cancer: A narrative review of the role of socioeconomic position from risk to survivorship. Urol. Oncol. 2012, 30, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tandon, A.; Murray, C.J.; Lauer, J.A.; Evans, D.B. Measuring Overall Health System Performance for 191 Countries; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Nur, U.; Rachet, B.; Parmar, M.K.; Sydes, M.R.; Cooper, N.; Stenning, S.; Read, G.; Oliver, T.; Mason, M.; Coleman, M.P. Socio-economic inequalities in testicular cancer survival within two clinical studies. Cancer Epidemiol. 2012, 36, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.L.; Wang, S.C.; Ho, C.J.; Kao, Y.L.; Hsieh, T.Y.; Chen, W.J.; Chen, C.J.; Wu, P.R.; Ko, J.L.; Lee, H.; et al. Prostate Cancer Mortality-To-Incidence Ratios Are Associated with Cancer Care Disparities in 35 Countries. Sci. Rep. 2017, 7, 40003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.C.; Sung, W.W.; Kao, Y.L.; Hsieh, T.Y.; Chen, W.J.; Chen, S.L.; Chang, H.R. The gender difference and mortality-to-incidence ratio relate to health care disparities in bladder cancer: National estimates from 33 countries. Sci. Rep. 2017, 7, 4360. [Google Scholar] [CrossRef] [Green Version]
- Sunkara, V.; Hebert, J.R. The colorectal cancer mortality-to-incidence ratio as an indicator of global cancer screening and care. Cancer 2015, 121, 1563–1569. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.C.; Tsai, M.C.; Peng, C.M.; Lee, H.L.; Chen, H.Y.; Yang, T.W.; Sung, W.W.; Lin, C.C. Favorable liver cancer mortality-to-incidence ratios of countries with high health expenditure. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1397–1401. [Google Scholar] [CrossRef]
- Tsai, M.C.; Wang, C.C.; Lee, H.L.; Peng, C.M.; Yang, T.W.; Chen, H.Y.; Sung, W.W.; Lin, C.C. Health disparities are associated with gastric cancer mortality-to-incidence ratios in 57 countries. World J. Gastroenterol. 2017, 23, 7881–7887. [Google Scholar] [CrossRef]
- Huang, C.Y.; Au, K.K.; Chen, S.L.; Wang, S.C.; Liao, C.Y.; Hsu, H.H.; Sung, W.W.; Wang, Y.C. Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity. Int. J. Environ. Res. Public Health 2018, 15, 2889. [Google Scholar] [CrossRef] [Green Version]
- Znaor, A.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Bray, F. International testicular cancer incidence trends: Generational transitions in 38 countries 1900–1990. Cancer Causes Control 2015, 26, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Roy, R.K.; Casson, K. Attitudes Toward Testicular Cancer and Self-Examination Among Northern Irish Males. Am. J. Men’s Health 2017, 11, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Tal, R.; Holland, R.; Belenky, A.; Konichezky, M.; Baniel, J. Incidental testicular tumors in infertile men. Fertil. Steril. 2004, 82, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.; Belot, A.; Rachet, B.; Coleman, M.P. The Mortality-to-Incidence Ratio Is Not a Valid Proxy for Cancer Survival. J. Glob. Oncol. 2019, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Region | Number | Crude Rate 1 | Age-Standardized Rate 1 | Mortality-to-Incidence Ratio 2 | |||
|---|---|---|---|---|---|---|---|
| Incidence | Mortality | Incidence | Mortality | Incidence | Mortality | ||
| World | 55,266 | 10,351 | 1.6 | 0.3 | 1.5 | 0.3 | 0.19 |
| Development | |||||||
| More-developed regions | 32,740 | 2209 | 5.4 | 0.4 | 5.2 | 0.3 | 0.07 |
| Less-developed regions | 22,526 | 8142 | 0.8 | 0.3 | 0.7 | 0.3 | 0.38 |
| WHO region categories | |||||||
| WHO Africa region | 1024 | 593 | 0.2 | 0.1 | 0.3 | 0.2 | 0.50 |
| WHO Americas region | 16,162 | 1988 | 3.4 | 0.4 | 3.2 | 0.4 | 0.12 |
| WHO East Mediterranean region | 2843 | 1438 | 0.9 | 0.5 | 0.9 | 0.5 | 0.56 |
| WHO Europe region | 23,560 | 2302 | 5.4 | 0.5 | 5 | 0.4 | 0.09 |
| WHO South-East Asia region | 5854 | 2766 | 0.6 | 0.3 | 0.6 | 0.3 | 0.50 |
| WHO Western Pacific region | 5819 | 1264 | 0.6 | 0.1 | 0.6 | 0.1 | 0.17 |
| Continent | |||||||
| Africa | 1529 | 864 | 0.3 | 0.2 | 0.4 | 0.3 | 0.67 |
| Latin America and Caribbean | 7197 | 1504 | 2.4 | 0.5 | 2.2 | 0.5 | 0.21 |
| Northern America | 8965 | 484 | 5.2 | 0.3 | 5 | 0.2 | 0.06 |
| Asia | 15,053 | 5849 | 0.7 | 0.3 | 0.7 | 0.3 | 0.43 |
| Europe | 21,548 | 1612 | 6 | 0.5 | 5.6 | 0.4 | 0.08 |
| Oceania | 974 | 38 | 5.2 | 0.2 | 5 | 0.2 | 0.04 |
| Country | Ranking | Total Expenditure on Health/GDP (%) | Life Expectancy | Number | Crude Rate 1 | Age-Standardized Rate 1 | Mortality-to-Incidence Ratio 2 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Incidence | Mortality | Incidence | Mortality | Incidence | Mortality | |||||
| France | 1 | 11.6 | 82 | 2332 | 98 | 7.5 | 0.3 | 7.6 | 0.3 | 0.04 |
| Italy | 2 | 9.2 | 83 | 2664 | 82 | 8.9 | 0.3 | 8.7 | 0.2 | 0.03 |
| Malta | 5 | 8.7 | 81 | 16 | 0 | 7.7 | 0.0 | 6.9 | 0.0 | 0.00 |
| Singapore | 6 | 4.2 | 83 | 37 | 3 | 1.4 | 0.1 | 1.3 | 0.1 | 0.07 |
| Spain | 7 | 9.3 | 83 | 823 | 42 | 3.6 | 0.2 | 3.5 | 0.1 | 0.06 |
| Oman | 8 | 2.7 | 76 | 8 | 3 | 0.5 | 0.2 | 0.4 | 0.2 | 0.40 |
| Austria | 9 | 11.1 | 81 | 368 | 25 | 8.9 | 0.6 | 8.2 | 0.5 | 0.07 |
| Japan | 10 | 10.3 | 84 | 1274 | 86 | 2.1 | 0.1 | 2.2 | 0.1 | 0.05 |
| Norway | 11 | 9.3 | 82 | 313 | 12 | 12.6 | 0.5 | 12.2 | 0.3 | 0.04 |
| Portugal | 12 | 9.9 | 81 | 302 | 18 | 5.8 | 0.3 | 6.0 | 0.3 | 0.05 |
| Iceland | 15 | 9.0 | 82 | 12 | 0 | 7.3 | 0.0 | 7.2 | 0.0 | 0.00 |
| Luxembourg | 16 | 7.2 | 82 | 22 | 0 | 8.4 | 0.0 | 8.2 | 0.0 | 0.00 |
| Netherlands | 17 | 12.7 | 81 | 709 | 26 | 8.5 | 0.3 | 8.7 | 0.3 | 0.04 |
| United Kingdom | 18 | 9.3 | 81 | 2163 | 64 | 7.0 | 0.2 | 6.8 | 0.2 | 0.03 |
| Ireland | 19 | 8.9 | 81 | 216 | 5 | 9.4 | 0.2 | 9.3 | 0.2 | 0.02 |
| Switzerland | 20 | 11.4 | 83 | 453 | 19 | 11.9 | 0.5 | 12.1 | 0.4 | 0.04 |
| Belgium | 21 | 10.9 | 80 | 300 | 13 | 5.7 | 0.2 | 5.8 | 0.2 | 0.04 |
| Colombia | 22 | 6.8 | 78 | 676 | 89 | 2.9 | 0.4 | 2.8 | 0.4 | 0.14 |
| Sweden | 23 | 9.6 | 82 | 329 | 9 | 6.9 | 0.2 | 7.0 | 0.2 | 0.03 |
| Cyprus | 24 | 7.3 | 82 | 28 | 2 | 4.9 | 0.3 | 4.2 | 0.3 | 0.06 |
| Germany | 25 | 11.3 | 81 | 4031 | 146 | 10.0 | 0.4 | 9.7 | 0.3 | 0.04 |
| Israel | 28 | 7.4 | 82 | 185 | 5 | 4.9 | 0.1 | 4.9 | 0.1 | 0.02 |
| Canada | 30 | 10.9 | 82 | 890 | 36 | 5.2 | 0.2 | 5.0 | 0.2 | 0.04 |
| Finland | 31 | 9.1 | 81 | 144 | 4 | 5.4 | 0.2 | 5.7 | 0.1 | 0.04 |
| Australia | 32 | 8.9 | 83 | 780 | 20 | 6.8 | 0.2 | 6.6 | 0.1 | 0.03 |
| Chile | 33 | 7.3 | 80 | 640 | 101 | 7.4 | 1.2 | 6.8 | 1.0 | 0.16 |
| Denmark | 34 | 11.0 | 80 | 336 | 11 | 12.1 | 0.4 | 11.9 | 0.3 | 0.03 |
| Costa Rica | 36 | 10.1 | 79 | 114 | 19 | 4.7 | 0.8 | 4.2 | 0.7 | 0.17 |
| United States of America | 37 | 17.0 | 79 | 8073 | 448 | 5.2 | 0.3 | 5.0 | 0.3 | 0.06 |
| Slovenia | 38 | 9.4 | 80 | 111 | 5 | 11.1 | 0.5 | 10.8 | 0.5 | 0.05 |
| Cuba | 39 | 8.6 | 78 | 106 | 17 | 1.9 | 0.3 | 1.4 | 0.2 | 0.16 |
| New Zealand | 41 | 10.2 | 82 | 173 | 7 | 7.9 | 0.3 | 7.8 | 0.2 | 0.04 |
| Bahrain | 46 | 4.4 | 77 | 9 | 0 | 1.1 | 0.0 | 1.3 | 0.0 | 0.00 |
| Thailand | 47 | 4.5 | 75 | 208 | 64 | 0.6 | 0.2 | 0.6 | 0.2 | 0.33 |
| Czech Republic | 48 | 7.5 | 78 | 496 | 30 | 9.6 | 0.6 | 8.6 | 0.4 | 0.06 |
| Malaysia | 49 | 4.0 | 74 | 135 | 34 | 0.9 | 0.2 | 0.9 | 0.2 | 0.22 |
| Poland | 50 | 6.8 | 77 | 939 | 116 | 5.1 | 0.6 | 4.7 | 0.5 | 0.12 |
| Jamaica | 53 | 5.6 | 74 | 9 | 3 | 0.7 | 0.2 | 0.6 | 0.2 | 0.29 |
| Korea, Republic of | 58 | 7.6 | 82 | 222 | 17 | 0.9 | 0.1 | 0.9 | 0.1 | 0.11 |
| Philippines | 60 | 4.4 | 69 | 204 | 94 | 0.4 | 0.2 | 0.5 | 0.3 | 0.50 |
| Slovakia | 62 | 8.1 | 76 | 284 | 18 | 10.7 | 0.7 | 9.3 | 0.6 | 0.07 |
| Egypt | 63 | 4.9 | 71 | 204 | 97 | 0.5 | 0.2 | 0.5 | 0.3 | 0.40 |
| Uruguay | 65 | 8.6 | 77 | 93 | 12 | 5.7 | 0.7 | 5.5 | 0.7 | 0.12 |
| Trinidad and Tobago | 67 | 5.5 | 71 | 5 | 2 | 0.8 | 0.3 | 0.6 | 0.3 | 0.38 |
| Belarus | 72 | 5.0 | 72 | 131 | 41 | 3.0 | 0.9 | 2.6 | 0.7 | 0.30 |
| Lithuania | 73 | 6.7 | 74 | 34 | 5 | 2.2 | 0.3 | 2.0 | 0.3 | 0.14 |
| Argentina | 75 | 6.8 | 76 | 1090 | 184 | 5.4 | 0.9 | 5.0 | 0.8 | 0.17 |
| Estonia | 77 | 5.9 | 77 | 23 | 3 | 3.7 | 0.5 | 3.5 | 0.5 | 0.14 |
| Ukraine | 79 | 7.5 | 71 | 570 | 133 | 2.8 | 0.6 | 2.5 | 0.5 | 0.21 |
| Mauritius | 84 | 4.8 | 74 | 13 | 2 | 2.0 | 0.3 | 2.3 | 0.3 | 0.15 |
| Fiji | 96 | 4.0 | 70 | 2 | 1 | 0.4 | 0.2 | 0.4 | 0.2 | 0.50 |
| Bulgaria | 102 | 7.4 | 75 | 220 | 41 | 6.2 | 1.1 | 6.2 | 0.9 | 0.18 |
| Latvia | 105 | 5.9 | 74 | 55 | 6 | 5.3 | 0.6 | 4.6 | 0.4 | 0.11 |
| Ecuador | 111 | 6.4 | 76 | 187 | 31 | 2.5 | 0.4 | 2.3 | 0.4 | 0.16 |
| Brazil | 125 | 9.5 | 75 | 1873 | 364 | 1.9 | 0.4 | 1.8 | 0.3 | 0.21 |
| Russian Federation | 130 | 6.5 | 69 | 1330 | 399 | 2.0 | 0.6 | 1.7 | 0.5 | 0.30 |
| South African Republic | 175 | 8.9 | 60 | 151 | 68 | 0.6 | 0.3 | 0.6 | 0.4 | 0.50 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.-J.; Huang, C.-Y.; Huang, Y.-H.; Wang, S.-C.; Hsieh, T.-Y.; Chen, S.-L.; Sung, W.-W.; Lee, T.-H. Correlations between Mortality-to-Incidence Ratios and Health Care Disparities in Testicular Cancer. Int. J. Environ. Res. Public Health 2020, 17, 130. https://doi.org/10.3390/ijerph17010130
Chen W-J, Huang C-Y, Huang Y-H, Wang S-C, Hsieh T-Y, Chen S-L, Sung W-W, Lee T-H. Correlations between Mortality-to-Incidence Ratios and Health Care Disparities in Testicular Cancer. International Journal of Environmental Research and Public Health. 2020; 17(1):130. https://doi.org/10.3390/ijerph17010130
Chicago/Turabian StyleChen, Wen-Jung, Cheng-Yu Huang, Yu-Hui Huang, Shao-Chuan Wang, Tzuo-Yi Hsieh, Sung-Lang Chen, Wen-Wei Sung, and Tsung-Hsien Lee. 2020. "Correlations between Mortality-to-Incidence Ratios and Health Care Disparities in Testicular Cancer" International Journal of Environmental Research and Public Health 17, no. 1: 130. https://doi.org/10.3390/ijerph17010130
APA StyleChen, W. -J., Huang, C. -Y., Huang, Y. -H., Wang, S. -C., Hsieh, T. -Y., Chen, S. -L., Sung, W. -W., & Lee, T. -H. (2020). Correlations between Mortality-to-Incidence Ratios and Health Care Disparities in Testicular Cancer. International Journal of Environmental Research and Public Health, 17(1), 130. https://doi.org/10.3390/ijerph17010130