Regional Temperature-Sensitive Diseases and Attributable Fractions in China


Abstract
:1. Introduction
2. Materials and Methods
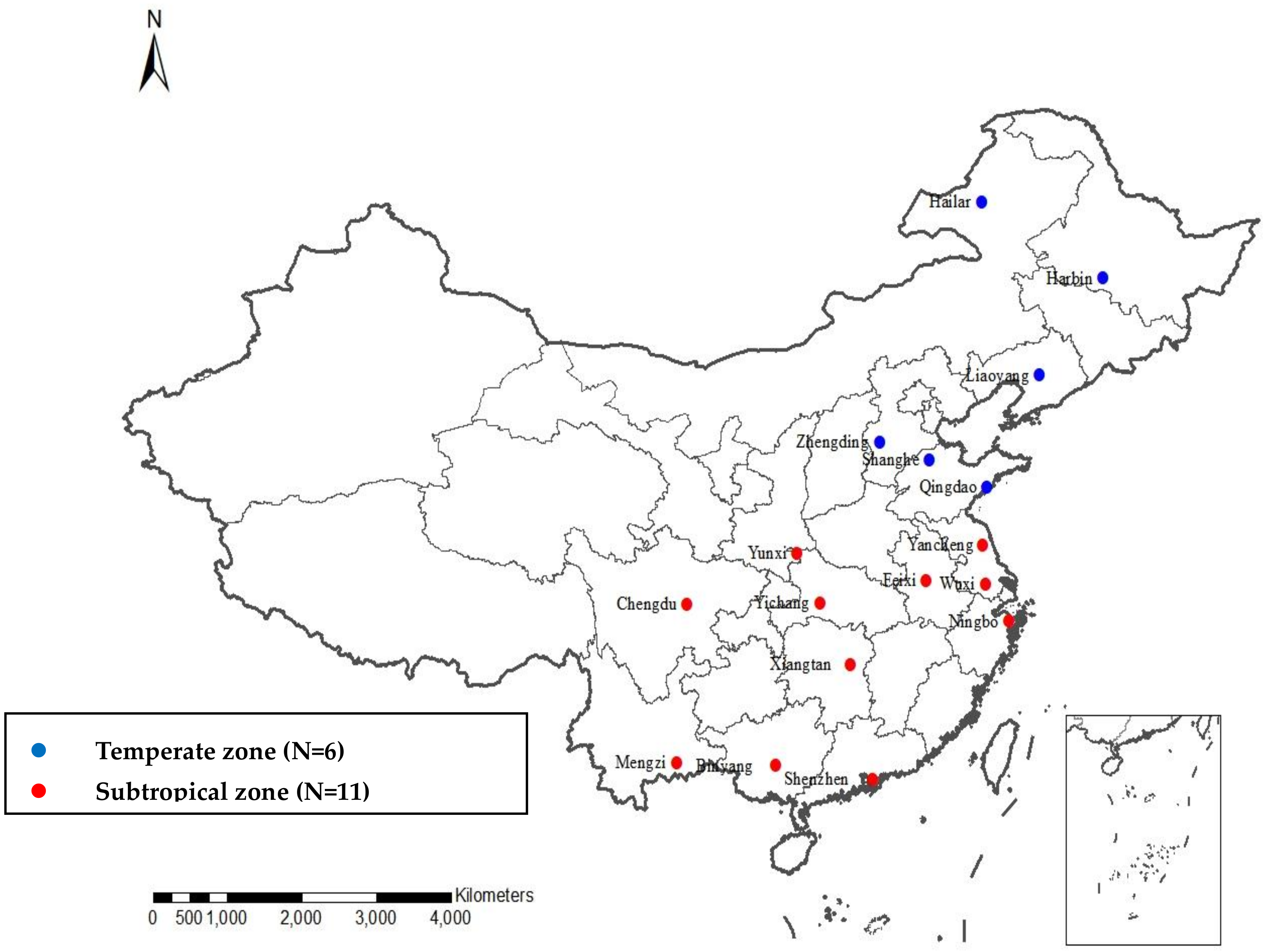
2.1. Study Regions
2.2. Mortality Data
2.3. Meteorological and Air Pollution Data
2.4. Statistical Analysis
2.4.1. Two-Stage Analysis
2.4.2. Estimation of Attributable Fractions
2.4.3. Assessing Regional Differences
2.5. Sensitivity Analysis
2.6. Ethics Approval and Consent to Participate
3. Results
3.1. Descriptive Statistics
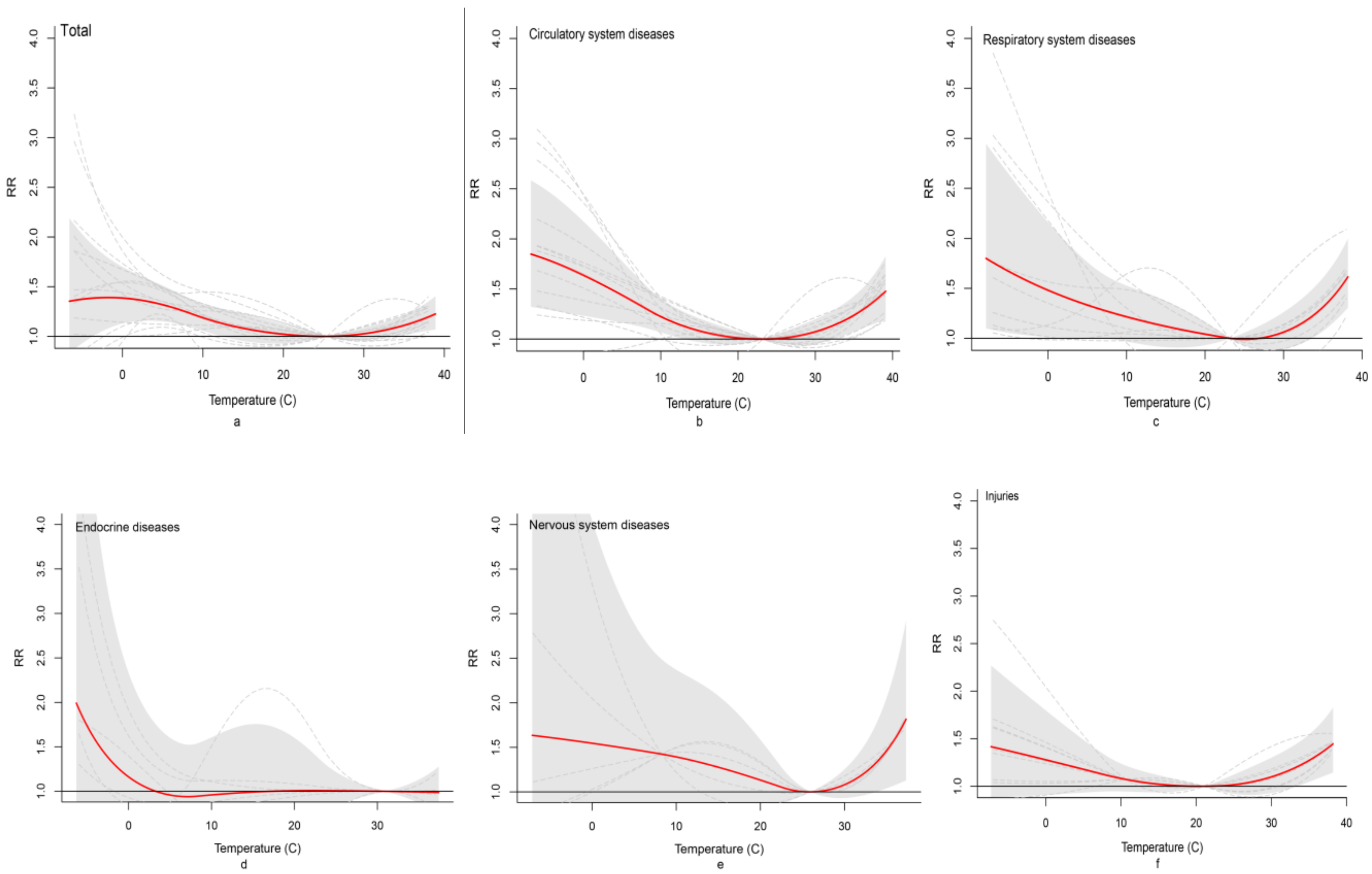
3.2. Association between Extreme Temperature and Cause-Specific Mortality
3.3. Attributable Fractions of Non-Optimum Temperatures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Diffenbaugh, N.S.; Scherer, M. Observational and model evidence of global emergence of permanent, unprecedented heat in the 20th and 21st centuries. Clim. Chang. 2011, 107, 615–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, N.; Mhawish, A.; Ghosh, S.; Banerjee, T.; Mall, R.K. Attributing mortality from temperature extremes: A time series analysis in Varanasi, India. Sci. Total Environ. 2019, 665, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Huang, C.; Barnett, A.G.; Wang, X.; Tong, S. Effects of extreme temperatures on years of life lost for cardiovascular deaths: A time series study in Brisbane, Australia. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 609–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Li, L.; Wang, J.; Huang, J.; Lu, S. Cardiovascular mortality associated with low and high temperatures: Determinants of inter-region vulnerability in China. Int. J. Environ. Res. Public Health 2015, 12, 5918–5933. [Google Scholar] [CrossRef]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Xiang, J.; Hansen, A.; Liu, Q.; Liu, X.; Tong, M.X.; Sun, Y.; Cameron, S.; Hanson-Easey, S.; Han, G.S.; Williams, C.; et al. Association between dengue fever incidence and meteorological factors in Guangzhou, China, 2005–2014. Environ. Res. 2017, 153, 17–26. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Chu, C.; Nguyen, H.L.T.; Nguyen, H.T.; Do, C.M.; Rutherford, S.; Phung, D. Temporal and spatial analysis of hand, foot, and mouth disease in relation to climate factors: A study in the Mekong Delta region, Vietnam. Sci. Total Environ. 2017, 581–582, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Dang, T.N.; Honda, Y.; Van Do, D.; Pham, A.L.T.; Chu, C.; Huang, C.; Phung, D. Effects of Extreme Temperatures on Mortality and Hospitalization in Ho Chi Minh City, Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 432. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, M.; Santana, P.; Rocha, A. Effects of extreme temperatures on cerebrovascular mortality in Lisbon: A distributed lag non-linear model. Int. J. Biometeorol. 2019, 63, 549–559. [Google Scholar] [CrossRef]
- Bobb, J.F.; Obermeyer, Z.; Wang, Y.; Dominici, F. Cause-specific risk of hospital admission related to extreme heat in older adults. JAMA 2014, 312, 2659–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.; Yin, P.; Wang, L.; Liu, C.; Niu, Y.; Wang, W.; Jiang, Y.; Liu, Y.; Liu, J.; Qi, J.; et al. Association between ambient temperature and mortality risk and burden: Time series study in 272 main Chinese cities. BMJ 2018, 363, k4306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascal, M.; Wagner, V.; Corso, M.; Laaidi, K.; Ung, A.; Beaudeau, P. Heat and cold related-mortality in 18 French cities. Environ. Int. 2018, 121, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Ohashi, N.; Doi, K.; Matsubara, T.; Kitsuta, Y.; Nakajima, S.; Yahagi, N. Impact of seasonal temperature environment on the neurologic prognosis of out-of-hospital cardiac arrest: A nationwide, population-based cohort study. J. Crit. Care 2014, 29, 840–847. [Google Scholar] [CrossRef]
- Ponjoan, A.; Blanch, J.; Alves-Cabratosa, L.; Marti-Lluch, R.; Comas-Cufi, M.; Parramon, D.; del Mar Garcia-Gil, M.; Ramos, R.; Petersen, I. Effects of extreme temperatures on cardiovascular emergency hospitalizations in a Mediterranean region: A self-controlled case series study. Environ. Health 2017, 16, 32. [Google Scholar] [CrossRef] [Green Version]
- Binazzi, A.; Bonafede, M.; Levi, M.; Bugani, M.; Messeri, A.; Morabito, M.; Marinaccio, A.; Baldasseroni, A. Evaluation of the impact of heat stress on the occurrence of occupational injuries: Meta-analysis of observational studies. Am. J. Ind. Med. 2019, 62, 233–243. [Google Scholar] [CrossRef]
- Varghese, B.M.; Barnett, A.G.; Hansen, A.L.; Bi, P.; Heyworth, J.S.; Sim, M.R.; Hanson-Easey, S.; Nitschke, M.; Rowett, S.; Pisaniello, D.L. Geographical variation in risk of work-related injuries and illnesses associated with ambient temperatures: A multi-city case-crossover study in Australia, 2005–2016. Sci Total Environ. 2019, 687, 898–906. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhang, Y.; Zhang, W.; Li, S.; Chen, G.; Wu, Y.; Qiu, C.; Ying, K.; Tang, H.; Huang, J.A.; et al. Ambient temperature and emergency department visits: Time-series analysis in 12 Chinese cities. Environ. Pollut. 2017, 224, 310–316. [Google Scholar] [CrossRef]
- Li, Y.; Cheng, Y.; Cui, G.; Peng, C.; Xu, Y.; Wang, Y.; Liu, Y.; Liu, J.; Li, C.; Wu, Z.; et al. Association between high temperature and mortality in metropolitan areas of four cities in various climatic zones in China: A time-series study. Environ. Health 2014, 13, 65. [Google Scholar] [CrossRef] [Green Version]
- Williams, S.; Nitschke, M.; Weinstein, P.; Pisaniello, D.L.; Parton, K.A.; Bi, P. The impact of summer temperatures and heatwaves on mortality and morbidity in Perth, Australia 1994–2008. Environ. Int. 2012, 40, 33–38. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Multivariate meta-analysis for non-linear and other multi-parameter associations. Stat. Med. 2012, 31, 3821–3839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparrini, A.; Leone, M. Attributable risk from distributed lag models. BMC Med. Res. Methodol. 2014, 14, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenland, S. Interval estimation by simulation as an alternative to and extension of confidence. Int. J. Epidemiol. 2004, 33, 1389–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Yin, P.; Sun, J.; Wang, B.; Zhou, M.; Li, M.; Tong, S.; Meng, B.; Guo, Y.; Liu, Q. Heatwave and mortality in 31 major Chinese cities: Definition, vulnerability and implications. Sci. Total Environ. 2019, 649, 695–702. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Armstrong, B. Reducing and meta-analysing estimates from distributed lag non-linear models. BMC Med. Res. Methodol. 2013, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Kong, D.; Fu, J.; Zhang, Y.; Liu, Y.; Zhao, Y.; Lian, H.; Zhao, X.; Yang, J.; Fan, Z. Association between extreme temperature and acute myocardial infarction hospital admissions in Beijing, China: 2013–2016. PLoS ONE 2018, 13, e0204706. [Google Scholar] [CrossRef]
- Zhang, Y.Q.; Yu, C.H.; Bao, J.Z. Acute effect of daily mean temperature on ischemic heart disease mortality: A multivariable meta-analysis from 12 counties across Hubei Province, China. Zhonghua Yu Fang Yi Xue Za Zhi 2016, 50, 990–995. [Google Scholar]
- Green, D.; Bambrick, H.; Tait, P.; Goldie, J.; Schultz, R.; Webb, L.; Alexander, L.; Pitman, A. Differential Effects of Temperature Extremes on Hospital Admission Rates for Respiratory Disease between Indigenous and Non-Indigenous Australians in the Northern Territory. Int. J. Environ. Res. Public Health 2015, 12, 15352–15365. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhao, Y.; Li, S.; Zhang, Y.; Wang, Q.; Zhang, H.; Qiao, H.; Li, W.; Huxley, R.; Williams, G.; et al. Impact of ambient temperature on clinical visits for cardio-respiratory diseases in rural villages in northwest China. Sci. Total Environ. 2018, 612, 379–385. [Google Scholar] [CrossRef]
- Miao, Y.; Shen, Y.-M.; Lu, C.; Zeng, J.; Deng, Q. Maternal exposure to ambient air temperature during pregnancy and early childhood pneumonia. J. Therm. Biol. 2017, 69, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lan, L.; Wang, Y.; Yang, C.; Tang, W.; Cui, G.; Luo, S.; Cheng, Y.; Liu, Y.; Liu, J.; et al. Extremely cold and hot temperatures increase the risk of diabetes mortality in metropolitan areas of two Chinese cities. Environ. Res. 2014, 134, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.H.; Luo, S.Q.; Lan, L.; Jin, M.G.; Yang, C.; He, J.Y.; Li, H.B.; Li, C.C.; Cheng, Y.B.; Jin, Y.L. Influence of extreme weather on years of life lost due to diabetes death in Chongqing and Harbin, China. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 303–308. [Google Scholar] [PubMed]
- Waernbaum, I.; Dahlquist, G. Low mean temperature rather than few sunshine hours are associated with an increased incidence of type 1 diabetes in children. Eur. J. Epidemiol. 2016, 31, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.M.; Ackland, T.R.; Dawson, B. The combined effect of heat and carbon monoxide on the performance of motorsport athletes. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2001, 128, 709–718. [Google Scholar] [CrossRef]
- Daanen, H.A.M.; Van De Vliert, E.; Huang, X. Driving performance in cold, warm, and thermoneutral environments. Appl. Ergon. 2003, 34, 597–602. [Google Scholar] [CrossRef]
- Wyon, D.P.; Wyon, I.; Norin, F. Effects of moderate heat stress on driver vigilance in a moving vehicle. Ergonomics 1996, 39, 61–75. [Google Scholar] [CrossRef]
- Liu, A.; Soneja, S.I.; Jiang, C.; Huang, C.; Kerns, T.; Beck, K.; Mitchell, C.; Sapkota, A. Frequency of extreme weather events and increased risk of motor vehicle collision in Maryland. Sci. Total Environ. 2017, 580, 550–555. [Google Scholar] [CrossRef]
- Schifano, P.; Asta, F.; Marinaccio, A.; Bonafede, M.; Davoli, M.; Michelozzi, P. Do exposure to outdoor temperatures, NO2 and PM10 affect the work-related injuries risk? A case-crossover study in three Italian cities, 2001–2010. BMJ Open 2019, 9, e023119. [Google Scholar] [CrossRef] [Green Version]
- Labaude, S.; Moret, Y.; Cezilly, F.; Reuland, C.; Rigaud, T. Variation in the immune state of Gammarus pulex (Crustacea, Amphipoda) according to temperature: Are extreme temperatures a stress? Dev. Comp. Immunol. 2017, 76, 25–33. [Google Scholar] [CrossRef]
- Kox, M.; Stoffels, M.; Smeekens, S.P.; van Alfen, N.; Gomes, M.; Eijsvogels, T.M.H.; Hopman, M.T.; van der Hoeven, J.G.; Netea, M.G.; Pickkers, P. The influence of concentration/meditation on autonomic nervous system activity and the innate immune response: A case study. Psychosom. Med. 2012, 74, 489–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, W.; Zeng, W.; Zhou, M.; Wang, L.; Rutherford, S.; Lin, H.; Liu, T.; Zhang, Y.; Xiao, J.; Zhan, Y.; et al. The short-term effect of heat waves on mortality and its modi fi ers in China: An analysis from 66 communities. Environ. Int. 2015, 75, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, S.; Zhang, Y.; Armstrong, B.; Jaakkola, J.J.K.; Tong, S.; Pan, X. Extremely cold and hot temperatures increase the risk of ischaemic heart disease mortality: Epidemiological evidence from China. Heart 2013, 99, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yin, P.; Zhou, M.; Ou, C.; Guo, Y.; Gasparrini, A.; Liu, Y.; Yue, Y.; Gu, S.; Sang, S.; et al. Cardiovascular mortality risk attributable to ambient temperature in China. Heart 2015, 101, 1966–1972. [Google Scholar] [CrossRef]
- Ma, W.; Xu, X.; Peng, L.; Kan, H. Impact of extreme temperature on hospital admission in Shanghai, China. Sci. Total Environ. 2011, 409, 3634–3637. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Site | Study Period | Population | Maximum Temperature (°C) | Mean Relative Humidity (%) | Mean Barometric Pressure (hpa) | Mean PM2.5 (μg/m3) | Mean O3 (μg/m3) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (city/county) | (million) | Mean ± SD | Min | Max | MMT | 97.5th | 2.5th | Mean ± SD | Min | Max | Mean ± SD | Min | Max | Mean ± SD | Min | Max | Mean ± SD | Min | Max | |
| Harbin | 2014–2016 | 31.7 | 10 ± 15.2 | –21.6 | 36.2 | 26 | 32 | –16 | 65 ± 15 | 15 | 97 | 9994 ± 95 | 9732 | 10,252 | 64.8 ± 61 | 8 | 653 | 63.6 ± 42.7 | 10 | 179 |
| Liaoyang | 2014–2015 | 1.89 | 16.1 ± 12.7 | –17.1 | 37.1 | 29.5 | 33 | –7 | 56 ± 16 | 13 | 98 | 10,123 ± 96 | 9840 | 10,359 | 33 ± 28 | 3 | 423 | 82.3 ± 32.1 | 17 | 291 |
| Hailar | 2014–2017 | 0.29 | 5.8 ± 17.9 | –34.1 | 41.7 | 24 | 32 | –24 | 62 ± 15 | 15 | 94 | 9371 ± 76 | 9127 | 9618 | 29.1 ± 17 | 5 | 164 | 74.4 ± 72.4 | 13 | 160 |
| Zhengding | 2014–2016 | 2.94 | 20.5 ± 11.1 | –9.1 | 43.4 | 18 | 37 | 1 | 54 ± 20 | 12 | 99 | 10,076 ± 99 | 9868 | 10,346 | 108 ± 89 | 0 | 653 | 102 ± 67 | 0 | 322 |
| Qingdao | 2014–2016 | 9.39 | 17.3 ± 9.3 | –7.7 | 36.9 | 29 | 32 | 1 | 69 ± 16 | 16 | 100 | 10,075 ± 90 | 9878 | 10,292 | 48 ± 34 | 4 | 298 | 102 ± 45 | 17 | 277 |
| Shanghe | 2014–2016 | 1.87 | 19.9 ± 10.6 | –10.6 | 40 | 17 | 35 | 1 | 68 ± 16 | 23 | 100 | 10,145 ± 99 | 9949 | 10,416 | 79 ± 52 | 8 | 342 | 122 ± 48 | 5 | 314 |
| Wuxi | 2014–2016 | 19.6 | 21.4 ± 9 | –3.8 | 40.6 | 25 | 36 | 6 | 75 ± 13 | 33 | 100 | 10,153 ± 92 | 9945 | 10,410 | 61 ± 26 | 11 | 223 | 103 ± 48 | 10 | 279 |
| Yancheng | 2014–2017 | 8.25 | 20.2 ± 9.1 | –6.2 | 39 | 28 | 35 | 4 | 76 ± 13 | 34 | 100 | 10,159 ± 92 | 9945 | 10,406 | 49 ± 35 | 5 | 226 | 83 ± 48 | 3 | 262 |
| Feixi | 2014–2017 | 4.00 | 21.5 ± 9.1 | –3.2 | 40.8 | 20.5 | 37 | 5 | 77 ± 12 | 32 | 99 | 10,133 ± 102 | 8586 | 10,424 | 51.8 ± 35.6 | 3 | 372 | 54 ± 43 | 12 | 251 |
| Yichang | 2014–2017 | 3.67 | 20.9 ± 8.8 | 0.4 | 38.3 | 30 | 36 | 5 | 76 ± 14 | 46 | 58 | 9852 ± 85 | 9692 | 10,126 | 71 ± 41 | 6 | 343 | 73 ± 42 | 10 | 198 |
| Yunxi | 2014–2016 | 1.59 | 21.7 ± 9.4 | –0.4 | 41.5 | 30 | 38 | 5 | 73 ± 14 | 14 | 99 | 9828 ± 95 | 9621 | 10,084 | 45 ± 33 | 0 | 554 | 83 ± 48 | 0 | 183 |
| Chengdu | 2013–2017 | 16.3 | 21.5 ± 7.8 | 2.8 | 36.7 | 30.5 | 35 | 8 | 80 ± 9 | 42 | 98 | 9506 ± 74 | 9325 | 9770 | 70 ± 49 | 9 | 423 | 89 ± 49 | 7 | 278 |
| Ningbo | 2014–2016 | 8.20 | 21.9 ± 8.6 | –2.3 | 39.2 | 30 | 36 | 6 | 80 ± 11 | 34 | 100 | 10,153 ± 88 | 9857 | 10,397 | 43 ± 26 | 7 | 202 | 94 ± 49 | 6 | 242 |
| Xiangtan | 2014–2016 | 2.85 | 23.4 ± 8.8 | 0.1 | 40 | 20 | 37 | 5 | 82 ± 12 | 38 | 100 | 10,071 ± 88 | 9911 | 10,368 | 51 ± 33 | 0 | 236 | 81 ± 48 | 0 | 279 |
| Mengzi | 2014–2017 | 1.62 | 25.1 ± 5.5 | 1.3 | 35.4 | 24 | 32 | 13 | 69 ± 12 | 26 | 100 | 8677 ± 40 | 8580 | 8813 | 19 ± 31 | 1 | 61 | 84 ± 40 | 12 | 175 |
| Shenzhen | 2016–2017 | 24.4 | 27.1 ± 5.6 | 6.5 | 36.9 | 25.5 | 34 | 14 | 75 ± 13 | 19 | 100 | 10,029 ± 64 | 9765 | 10,223 | 30 ± 17 | 6 | 110 | 82 ± 49 | 25 | 244 |
| Binyang | 2014–2016 | 3.26 | 25.9 ± 7.3 | 6.5 | 37.3 | 31.5 | 35 | 10 | 80 ± 11 | 36 | 100 | 9975 ± 74 | 9784 | 10,228 | 29 ± 19 | 4- | 117 | 89 ± 34 | 24 | 196 |
| Variables | Mean ± SD | Minimum | Maximum |
|---|---|---|---|
| Total | 63 ± 66 | 4 | 222 |
| Diseases of circulatory system | 21 ± 24 | 2 | 92 |
| Hypertension | 1.2 ± 1.6 | 0 | 6 |
| Ischemic heart disease | 8 ± 11 | 0 | 45 |
| Cerebrovascular disease | 11 ± 13 | 0 | 41 |
| Cerebral infarction | 3 ± 5 | 0 | 17 |
| Intracerebral hemorrhage | 4 ± 5 | 0 | 18 |
| Stroke | 1 ± 1 | 0 | 3 |
| Sequelae of cerebrovascular disease | 2 ± 3 | 0 | 8 |
| Diseases of respiratory system | 8 ± 13 | 0 | 53 |
| Chronic lower respiratory disease | 6 ± 10 | 0 | 40 |
| Influenza and pneumonia | 2 ± 3 | 0 | 10 |
| Diseases of digestive system | 1 ± 2 | 0 | 7 |
| Diseases of genitourinary system | 1 ± 1 | 0 | 2 |
| Endocrine diseases | 2 ± 2 | 0 | 6 |
| Diabetes | 2 ± 2 | 0 | 6 |
| Diseases of nervous system | 1 ± 1 | 0 | 3 |
| Infectious diseases | 1 ± 1 | 0 | 3 |
| Injuries | 4 ± 4 | 0 | 13 |
| Region | Extreme Heat | Extreme Cold | ||||
|---|---|---|---|---|---|---|
| Overall | Subtropical Zone | Temperate Zone | Overall | Subtropical Zone | Temperate Zone | |
| Total | 1.13 (1.09, 1.18) | 1.18 (1.08, 1.25) | 1.06 (1.02, 1.15) | 1.30 (1.10, 1.54) | 1.34 (1.11, 1.62) | 1.14 (0.98, 1.32) |
| Circulatory system | 1.19 (1.12, 1.26) | 1.27 (1.13, 1.43) | 1.14 (1.03, 1.25) | 1.46 (1.16, 1.82) | 1.54 (1.20, 1.97) | 1.47 (0.85, 2.54) |
| Hypertension | 1.46 (1.26, 1.69) | — | — | 1.64 (0.91, 2.93) | — | — |
| Ischemic heart disease | 1.18 (1.07, 1.31) | 1.28 (1.07, 1.53) | 1.10 (1.00, 1.21) | 1.75 (1.26, 2.44) | 1.75 (1.32, 2.32) | 2.16 (0.82, 5.67) |
| Cerebrovascular disease | 1.19 (1.12, 1.26) | 1.23 (1.14, 1.33) | 1.08 (1.01, 1.16) | 1.39 (1.09, 1.76) | 1.71 (1.43, 2.03) | 0.78 (0.56, 1.08) |
| Cerebral infarction | 1.20 (1.08, 1.35) | — | — | 1.49 (0.99, 2.26) | — | — |
| Intracerebral hemorrhage | 1.08 (1.00, 1.16) | 1.12 (1.00, 1.25) | 0.96 (0.86, 1.07) | 1.49 (1.13, 1.96) | 1.32 (1.13, 1.99) | 1.45 (1.15, 1.90) |
| Stroke | 1.52 (1.12, 2.09) | — | — | 1.29 (0.57, 2.93) | — | — |
| Sequelae of cerebrovascular disease | 1.61 (1.41, 1.85) | — | — | 1.18 (0.75, 1.85) | — | — |
| Respiratory system | 1.25 (1.09, 1.30) | 1.30 (1.17, 1.45) | 1.18 (0.96, 1.45) | 1.34 (1.07, 1.42) | 1.33 (1.14, 1.48) | 0.90 (0.68, 1.43) |
| Influenza and pneumonia | 1.28 (1.15, 1.43) | 1.28 (1.14, 1.44) | 1.29 (1.04, 1.61) | 1.36 (0.76, 2.41) | 0.92 (0.70, 1.17) | 1.20 (0.74, 1.96) |
| Chronic obstructive pulmonary disease | 1.22 (1.12, 1.32) | 1.26 (1.09, 1.45) | 1.41 (1.07, 1.85) | 1.35 (1.10, 1.65) | 1.49 (1.30, 1.71) | 0.94 (0.76, 1.17) |
| Endocrine diseases | 1.13 (1.02, 1.25) | — | — | 0.94 (0.51, 1.73) | — | — |
| Diabetes | 1.13 (1.03, 1.25) | — | — | 0.95 (0.50, 1.81) | — | — |
| Digestive system | 1.22 (0.95, 1.56) | — | — | 1.23 (1.04, 1.45) | — | — |
| Genitourinary system | 1.03 (0.55, 1.92) | — | — | 1.13 (0.35, 3.63) | — | — |
| Nervous system | 1.41 (1.10, 1.77) | 1.51 (1.04, 2.19) | 1.28 (0.88, 1.87) | 1.28 (0.64, 3.43) | 1.92 (0.87, 4.22) | 0.36 (0.06, 2.00) |
| Injuries | 1.45 (1.27, 1.65) | 1.34 (1.16, 1.56) | 1.27 (1.15, 1.36) | 1.17 (0.95, 1.44) | 1.21 (0.98, 1.51) | 1.49 (0.83, 2.65) |
| Infectious diseases | 0.43 (0.07, 2.58) | — | — | 1.00 (0.2, 4.96) | — | — |
| Cause of Death | AFall | High Temperature | Low Temperature | ||||
|---|---|---|---|---|---|---|---|
| Overall | Subtropical Zone | Temperature Zone | Overall | Subtropical Zone | Temperature Zone | ||
| Total | 11.03 | 1.62 (0.76, 2.43) | 1.96 (0.95. 2.91) | 0.99 (0.42, 1.56) | 9.40 (2.92, 15.83) | 9.06 (4.67, 13.53) | 10.0 (−1.8, 20.1) |
| Circulatory system | 15.7 | 3.9 (0.42, 7.09) | 2.5 (0.8, 4.1) | 6.2 (−0.13, 12.0) | 11.8 (2.4, 19.6) | 15.1 (4.1, 24.6) | 6.5 (−0.4, 11.5) |
| Respiratory system | 15.2 | 1.85 (0.68, 2.85) | 2.6 (1.3, 3.8) | 0.58 (−0.26, 1.26) | 13.3 (5.6, 23.6) | 24.2 (9.8, 36) | −4.3 (−15.8, 3.54) |
| Endocrine | 9.3 | 0.9 (−0.3, 1.9) | — | — | 8.4 (−15.6, 25.0) | — | — |
| Nervous system | 12.6 | 4.2 (1.0, 7.03) | 5.03 (1.8, 7.8) | 1.8 (−;1.6, 4.4) | 8.4 (−21.1, 32.4) | 16.0 (−5.1, 29.2) | −16.5 (−48.2, 56.7) |
| Injuries | 10.1 | 6.5 (2.5, 10.0) | 6.2 (2.2, 9.8) | 7.6 (3.5, 31.1) | 3.6 (−10.6, 14.1) | 3.8 (−7.1, 12.0) | 2.9 (−21.5, 20.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, X.; Cheng, Y.; Wang, Y.; Liu, Y.; Li, N.; Li, Y.; Yao, X. Regional Temperature-Sensitive Diseases and Attributable Fractions in China. Int. J. Environ. Res. Public Health 2020, 17, 184. https://doi.org/10.3390/ijerph17010184
Su X, Cheng Y, Wang Y, Liu Y, Li N, Li Y, Yao X. Regional Temperature-Sensitive Diseases and Attributable Fractions in China. International Journal of Environmental Research and Public Health. 2020; 17(1):184. https://doi.org/10.3390/ijerph17010184
Chicago/Turabian StyleSu, Xuemei, Yibin Cheng, Yu Wang, Yue Liu, Na Li, Yonghong Li, and Xiaoyuan Yao. 2020. "Regional Temperature-Sensitive Diseases and Attributable Fractions in China" International Journal of Environmental Research and Public Health 17, no. 1: 184. https://doi.org/10.3390/ijerph17010184
APA StyleSu, X., Cheng, Y., Wang, Y., Liu, Y., Li, N., Li, Y., & Yao, X. (2020). Regional Temperature-Sensitive Diseases and Attributable Fractions in China. International Journal of Environmental Research and Public Health, 17(1), 184. https://doi.org/10.3390/ijerph17010184