A Qualitative Analysis of an Aerobic Interval Training Programme for Obese Outpatients Carried Out in a Hospital Context


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Ethical Considerations
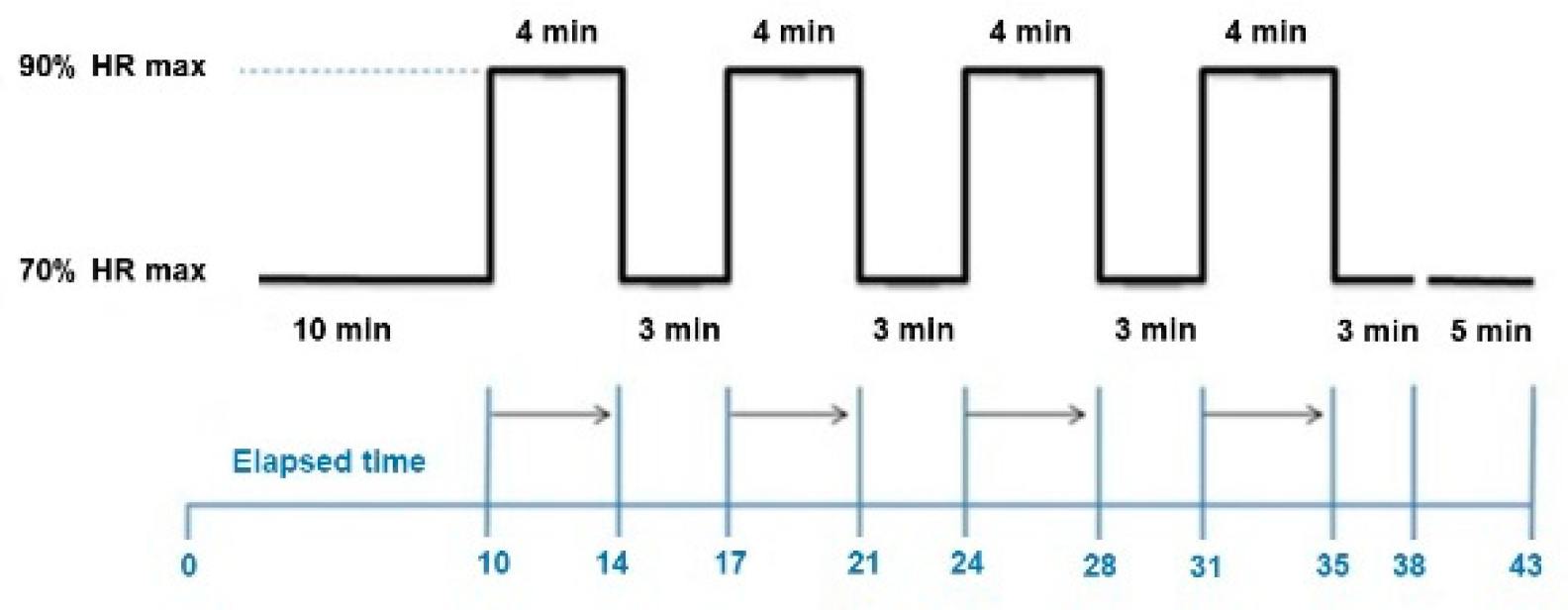
2.3. Training Protocol
2.4. Data Analysis
3. Results
3.1. Theme 1: General Aspects of the Physical Exercise Programme
3.2. Theme 2. Perspective on the Activity and the Environment
3.3. Perceived Benefits
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Rodríguez-Rodríguez, E.; López-Plaza, B.; López-Sobaler, A.M.; Ortega, R.M. Overweight and obesity among Spanish adults. Nutr. Hosp. 2011, 26, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Fisac, J.L.; Guallar-Castillón, P.; León-Muñoz, L.M.; Graciani, A.; Banegas, J.R.; Rodríguez-Artalejo, F. Prevalence of general and central obesity in the adult population of Spain, 2008–2010: The ENRICA study. Obes. Rev. 2012, 13, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Caspersen, C.J. Sedentary behaviour and cardiovascular disease: A review of prospective studies. Int. J. Epidemiol. 2012, 41, 1338–1353. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Forster, M.; Veerman, J.L.; Barendregt, J.J.; Vos, T. Cost-effectiveness of diet and exercise interventions to reduce overweight and obesity. Int. J. Obes. 2011, 35, 1071–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- LeFevre, M.L.; US Preventive Services Task Force. Behavioral counseling to promote a healthful diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2014, 161, 587–593. [Google Scholar] [CrossRef]
- Strath, S.J.; Kaminski, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gray, R.A.; Richardson, C.R.; Smith, D.T. Guide to the assessment of physical activity: Clinical and research applications. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M.; Lancet Sedentary Behaviour Working Group. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Prieto, J.A.; Del Valle, M.; Nistal, P.; Méndez, D.; Abelairas-Gómez, C.; Barcala-Furelos, R. Repercusión del ejercicio físico en la composición corporal y la capacidad aeróbica de adultos mayores con obesidad mediante tres modelos de intervención. Rev. Nutr. Hosp. 2015, 31, 1217–1224. [Google Scholar] [CrossRef]
- Laredo-Aguilera, J.A.; Cobo-Cuenca, A.I.; Santacruz-Salas, E.; Martins, M.M.; Rodríguez-Borrego, M.A.; López-Soto, P.J.; Carmona-Torres, J.M. Levels of Physical Activity, Obesity and Related Factors in Young Adults Aged 18-30 during 2009–2017. Int. J. Environ. Res. Public Health 2019, 16, 4033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rognmo, O.; Hetland, E.; Helgerud, J.; Hoff, J.; Slørdahl, S. High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Little, J.P.; Gillen, J.B.; Percival, M.E.; Safdar, A.; Tarnopolsky, M.A.; Punthakee, Z.; Jung, M.E.; Gibala, M.J. Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J. Appl. Physiol. 2011, 111, 1554–1560. [Google Scholar] [CrossRef] [Green Version]
- Tjønna, A.E.; Lee, S.J.; Rognmo, Ø.; Stølen, T.O.; Bye, A.; Haram, P.M.; Loennechen, J.P.; Al-Share, Q.Y.; Skogvoll, E.; Slørdahl, S.A.; et al. Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation 2008, 118, 346–354. [Google Scholar]
- Tong, T.K.; Zhang, H.; Shi, H.; Liu, Y.; Ai, J.; Nie, J.; Kong, Z. Comparing Time Efficiency of Sprint vs. High-Intensity Interval Training in Reducing Abdominal Visceral Fat in Obese Young Women: A Randomized, Controlled Trial. Front. Physiol. 2018. [Google Scholar] [CrossRef]
- Keytsman, C.; Hansen, D.; Wens, I.; Eijnde, B.O. Impact of high-intensity concurrent training on cardiovascular risk factors in persons with multiple sclerosis—Pilot study. Disabil. Rehabil. 2019, 41, 430–435. [Google Scholar] [CrossRef]
- Ferrandia, P.J.; Ficoa, B.G.; Whitehursta, M.; Zourdosa, M.C.; Baoa, F.; Dodgea, K.M.; Rodrigueza, A.L.; Penaa, G.; Huanga, C.-J. Acute high-intensity interval exercise induces comparable levels of circulating cell-free DNA and Interleukin-6 in obese and normal-weight individuals. Life Sci. 2018, 202, 161–166. [Google Scholar] [CrossRef]
- Sun, S.; Zhang, H.; Kong, Z.; Shi, Q.; Tong, T.K.; Nie, J. Twelve weeks of low volume sprint interval training improves cardio-metabolic health outcomes in overweight females. J. Sports Sci. 2019, 37, 1257–1264. [Google Scholar] [CrossRef]
- Schjerve, I.E.; Tyldum, G.A.; Tjønna, A.E.; Stølen, T.; Loennechen, J.P.; Hansen, H.E.M.; Haram, P.M.; Heinrich, G.; Bye, A.; Najjar, S.M.; et al. Both aerobic endurance and strength training programmes improve cardiovascular health in obese adults. Clin. Sci. 2008, 115, 283–293. [Google Scholar] [CrossRef] [Green Version]
- Munk, P.; Staal, E.; Butt, N.; Isaksen, K.; Larsen, A. High-intensity interval training may reduce in-stent restenosis following percutaneous coronary intervention with stent implantation A randomized controlled trial evaluating the relationship to endothelial function and inflammation. Am. Heart J. 2009, 158, 734–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stensvold, D.; Tjønna, A.E.; Skaug, E.-A.; Aspenes, S.; Stølen, T.; Wisløff, U.; Slørdahl, S.A. Strength training versus aerobic interval training to modify risk factors of metabolic syndrome. J. Appl. Physiol. 2010, 108, 804–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moholdt, T.; Aamot, I.; Slørdahl, S.; Gjerde, L.; Myklebust, G.; Walderhaug, L.; Brattbakk, L.; Hole, T.; Graven, T.; Stølen, T.O.; et al. Aerobic interval training increases peak oxygen uptake more than usual care exercise training in myocardial infarction patients: A randomized controlled study. Clin. Rehabil. 2012, 26, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Weston, K.; Wisløff, U.; Coombes, J. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef]
- Marton, F. Phenomenography. Describing Conceptions of the World around Us. Instr. Sci. 1981, 10, 177–200. [Google Scholar] [CrossRef]
- Marton, F.; Booth, S. Learning and Awareness; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1997. [Google Scholar]
- Sjöström, B.; Dahlgren, L.O. Applying phenomenography in nursing research. Nursing theory and concept development or analysis. J. Adv. Nurs. 2002, 40, 339–345. [Google Scholar] [CrossRef]
- Brown, I.; Gould, J. Qualitative studies of obesity: A review of methodology. Health 2013, 5, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Smith, C.A.; Costello, M.F.; MacMillan, F.; Moran, L.; Ee, C. Barriers and facilitators to weight management in overweight and obese women living in Australia with PCOS: A qualitative study. BMC Endocr. Disord. 2019, 19, 106. [Google Scholar] [CrossRef]
- Wiklund, M.; Olsén, M.F.; Willén, C. Physical activity as viewed by adults with severe obesity, awaiting gastric bypass surgery. Physiother. Res. Int. 2011, 16, 179–186. [Google Scholar] [CrossRef]
- Reljic DLampe, D.; Wolf, F.; Zopf, Y.; Herrmann, H.J.; Fischer, J. Prevalence and predictors of dropout from high-intensity interval training in sedentary individuals: A meta-analysis. Scand. J. Med. Sci. Sports 2019, 29, 1288–1304. [Google Scholar] [CrossRef]
- Wewege, M.; Van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef]
- Viana, R.B.; Naves, J.P.A.; Coswig, V.S.; de Lira, C.A.B.; Steele, J.; Fisher, J.P.; Gentil, P. Is interval training the magic bullet for fat loss? A systematic review and meta-analysis comparing moderate-intensity continuous training with high-intensity interval training (HIIT). Br. J. Sports Med. 2019, 53, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, D.; Soltani, H.; Copeland, R. The weight-loss experience: A qualitative exploration. BMC Public Health 2016, 16, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trost, S.; Owen, N.; Bauman, A.; Sallis, J.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Jerome, G.; McAuley, E. Enrollment and participation in a pilot walking programme: The role of self-efficacy. J. Health Psychol. 2013, 18, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Vuori, I.; Lavie, C.; Blair, S. Physical activity promotion in the health care system. Mayo Clin. Proc. 2013, 88, 1446–1461. [Google Scholar] [CrossRef] [Green Version]
- Nigg, C.; Borrelli, B.; Maddock, J.; Dishman, R. A Theory of Physical Activity Maintenance. Appl. Psychol. Int. Rev. 2008, 57, 544–560. [Google Scholar] [CrossRef]
- DiMarco, I.D.; Klein, D.A.; Clark, V.L.; Wilson, G.T. The use of motivational interviewing techniques to enhance the efficacy of guided self-help behavioral weight loss treatment. Eat Behav. 2009, 10, 134–136. [Google Scholar] [CrossRef] [Green Version]
- Payeras, J. Coaching y Liderazgo: Para Directivos Interesados en Incrementar sus Resultados; Ediciones Díaz de Santos: Madrid, Spain, 2004. [Google Scholar]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice Hall International: London, UK, 1980. [Google Scholar]


{kind=link}
| Participant Nº | Age | Sex (F/M) | Diagnosis a | Other therapies (Diet/Exercise) b |
|---|---|---|---|---|
| 1 | 72 | F | Obesity and hypertension a | Not following hospital hypocaloric diet |
| 2 | 53 | M | Obesity | Following hospital hypocaloric diet |
| 3 | 67 | F | Obesity | Following hospital hypocaloric diet |
| 4 | 35 | F | Obesity | Following hospital hypocaloric diet |
| 5 | 45 | M | Obesity | Following hospital hypocaloric diet and swimming 2 times/week |
| 6 | 75 | M | Obesity | Following hospital hypocaloric diet |
| 7 | 39 | F | Obesity and hypertension | Following hospital hypocaloric diet |
| 8 | 46 | F | Obesity | Not following hospital hypocaloric diet |
| 9 | 40 | F | Obesity | Not following hospital hypocaloric diet |
| 10 | 40 | M | Obesity and hypertension | Not following hospital hypocaloric diet |
| 11 | 34 | M | Obesity and hypertension | Following hospital hypocaloric diet |
| 12 | 69 | M | Obesity and hypertension | Following hospital hypocaloric diet |
| 13 | 52 | F | Obesity and hypertension | Not following hospital hypocaloric diet |
| 14 | 61 | F | Obesity | Following hospital hypocaloric diet |
| 15 | 43 | F | Obesity and hypertension | Following hospital hypocaloric diet |
| 16 | 74 | F | Obesity and type 2 diabetes | Following hospital hypocaloric diet |
| 17 | 65 | M | Obesity | Not following hospital hypocaloric diet and cycling 2 times/week |
| 18 | 54 | F | Obesity | Following hospital hypocaloric diet |
| 19 | 41 | F | Obesity | Following hospital hypocaloric diet |
| 20 | 59 | F | Obesity and hypertension | Following hospital hypocaloric diet |
| 21 | 45 | F | Obesity | Not following hospital hypocaloric diet |
| 22 | 57 | M | Obesity | Following hospital hypocaloric diet |
| 23 | 48 | F | Obesity | Following hospital hypocaloric diet |
| 24 | 53 | F | Obesity | Following hospital hypocaloric diet |
| Theme | Subtheme | Quotes a |
|---|---|---|
| General aspects of the programme | 1. Opinions of the programme | ‘...I liked it, I feel more encouraged and I am better physically’ (20) |
| 2. How patient received information on the programme | ‘My doctor recommended it’ (15) ‘Because my daughter participated in a programme like this and I saw the improvement, also to motivate and encourage myself’ (13) | |
| 3. Reasons for starting the programme | ‘To get slimmer’ (2) ‘Because I felt bad physically and emotionally’ (4) | |
| 4.Expectations | ‘It was time to do something’ (9) ‘I thought it would be very good for me’ (15) ‘Fear to be able to do it” (17) | |
| Opinion of the activity and the instructor | 5. Instructor | ‘The people themselves, especially the instructor, who has motivated us with his enthusiasm as we only had to compete against ourselves’ (13) |
| 6. Activity and environment | ‘Fantastic, very at ease’ (2) ‘I live a long way from the facility.’ (15) ‘Better equipment for the bikes’ (10) ‘Being sure that the programme was suitable’ (22) | |
| Perceived benefits | 7. Overall benefits | ‘Stronger, better psychologically’ (16) ‘I feel better, more agile. Before I thought that I couldn’t do it’ (8) ‘I have learned a lot in a short time, I am grateful, I must continue so that I don’t put on weight’ (17) ‘Surprised by my participation and constancy, improved mood, etc.’ (20) |
| 8. Future recommendations | ‘Excellent, the programme should continue’ (3) ‘Recommendable for more people’ (11) ‘It is fantastic and very complete’ (23) ‘It should be repeated’ (6) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabanillas-Cruz, E.; López-Rodriguez, C.; Romero-Blanco, C.; Aznar, S. A Qualitative Analysis of an Aerobic Interval Training Programme for Obese Outpatients Carried Out in a Hospital Context. Int. J. Environ. Res. Public Health 2020, 17, 312. https://doi.org/10.3390/ijerph17010312
Cabanillas-Cruz E, López-Rodriguez C, Romero-Blanco C, Aznar S. A Qualitative Analysis of an Aerobic Interval Training Programme for Obese Outpatients Carried Out in a Hospital Context. International Journal of Environmental Research and Public Health. 2020; 17(1):312. https://doi.org/10.3390/ijerph17010312
Chicago/Turabian StyleCabanillas-Cruz, Esther, Christian López-Rodriguez, Cristina Romero-Blanco, and Susana Aznar. 2020. "A Qualitative Analysis of an Aerobic Interval Training Programme for Obese Outpatients Carried Out in a Hospital Context" International Journal of Environmental Research and Public Health 17, no. 1: 312. https://doi.org/10.3390/ijerph17010312
APA StyleCabanillas-Cruz, E., López-Rodriguez, C., Romero-Blanco, C., & Aznar, S. (2020). A Qualitative Analysis of an Aerobic Interval Training Programme for Obese Outpatients Carried Out in a Hospital Context. International Journal of Environmental Research and Public Health, 17(1), 312. https://doi.org/10.3390/ijerph17010312