Neighborhood Ties Reduced Depressive Symptoms in Older Disaster Survivors: Iwanuma Study, a Natural Experiment

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
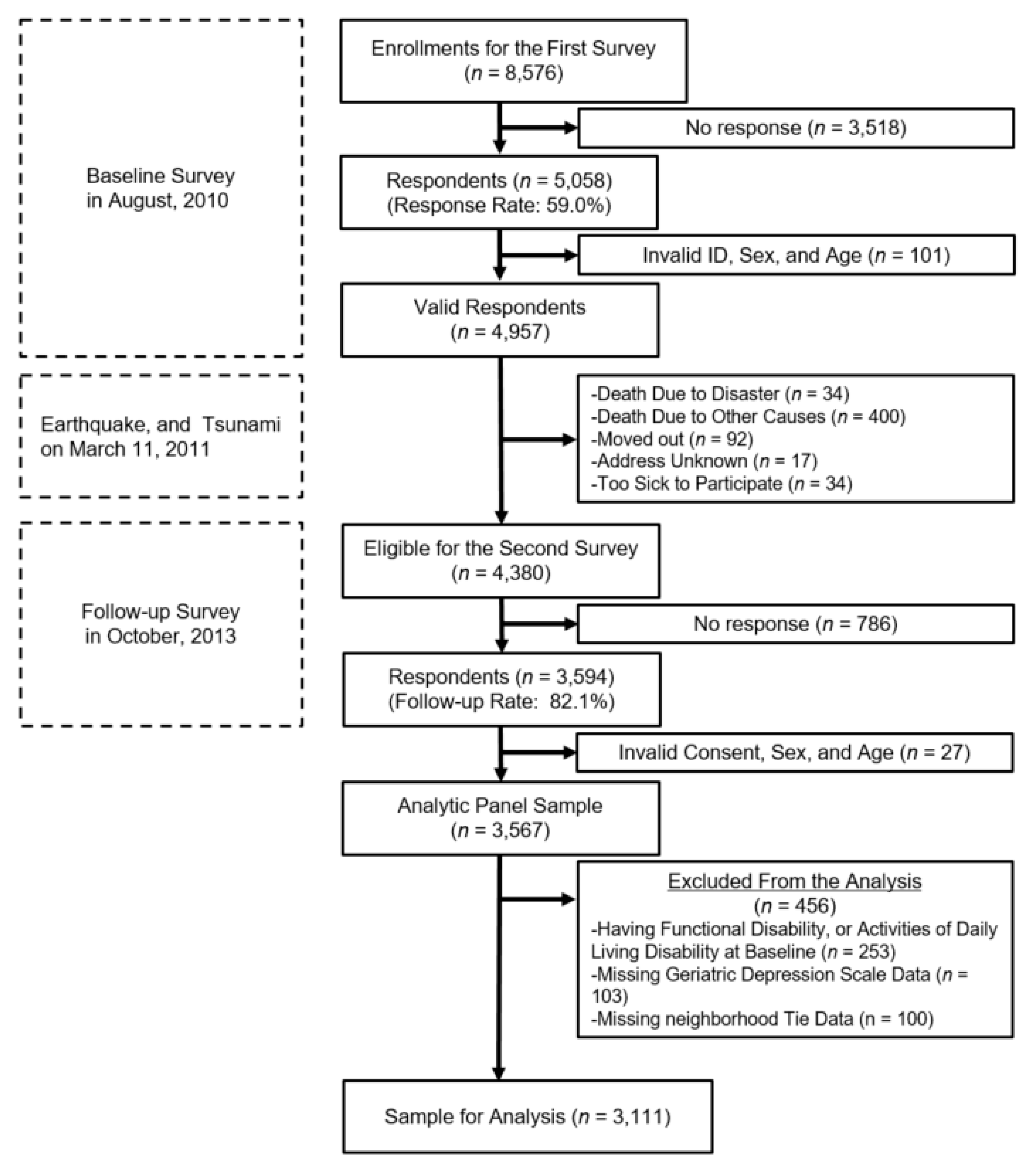
2.1. Study Design and Participants
2.2. Outcome Variable: Geriatric Depression Scale
2.3. Predictor Variable: Change in the Social Ties with Neighbors before and after the Disaster
3. Covariates: Sociodemographic Characteristics and Disaster Damage
3.1. Statistical Analysis
3.2. Ethical Considerations
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | VIF | 1/VIF | |
|---|---|---|---|
| Change in neighborhood tie (2010→2013) | No tie➡No tie | ||
| No tie➡Tie | 1.04 | 0.96 | |
| Tie➡No tie | 1.09 | 0.92 | |
| Tie➡Tie | 1.09 | 0.92 | |
| Sex | Female | 1.63 | 0.61 |
| Age | Age | 1.16 | 0.86 |
| Change in receiving medical treatment (2010→2013) | Treat➡Treat | ||
| Treat➡Non | 1.03 | 0.97 | |
| Non➡Treat | 1.06 | 0.94 | |
| Non➡Non | 1.06 | 0.94 | |
| Change in living status | Alone➡Alone | ||
| (2010→2013) | Alone➡Not alone | 1.10 | 0.91 |
| Not alone➡Alone | 1.36 | 0.74 | |
| Not alone➡Not alone | 1.48 | 0.68 | |
| Change in sports club participation (2010→2013) | No change | ||
| Increase | 1.07 | 0.93 | |
| Decrease | 1.06 | 0.94 | |
| Change in smoking behavior (2010→2013) | Smoke➡Smoke | ||
| Smoke➡Non | 1.44 | 0.69 | |
| Non➡Smoke | 1.07 | 0.93 | |
| Non➡Non | 1.61 | 0.62 | |
| Change in drinking behavior (2010→2013) | Drink➡Drink | ||
| Drink➡Non | 1.18 | 0.84 | |
| Non➡Drink | 1.06 | 0.95 | |
| Non➡Non | 1.73 | 0.58 | |
| Change in self-rated economic situation(2010→2013) | Economic difficulty➡Economic difficulty | ||
| Economic difficulty➡No economic difficulty | 2.51 | 0.40 | |
| No economic difficulty➡Economic difficulty | 1.86 | 0.54 | |
| No economic difficulty➡No economic difficulty | 3.15 | 0.32 | |
| Change in walking/day behavior (2010→2013) | Walk < 30➡Walk < 30 | ||
| Walk < 30➡Walk => 30 | 1.54 | 0.65 | |
| Walk => 30➡Walk < 30 | 1.44 | 0.69 | |
| Walk => 30➡Walk => 30 | 1.90 | 0.53 | |
| Lost family members/relatives | Lost | ||
| No lost | 1.06 | 0.94 | |
| Lost friends | Lost | ||
| No lost | 1.05 | 0.95 | |
| Relocation after the disaster | No replacement | ||
| Group relocation to prefabricated housing | 1.04 | 0.96 | |
| Individual relocation to prefabricated housing | 1.01 | 0.99 | |
| Existing private accommodation | 1.06 | 0.94 | |
| Newly established housing | 1.04 | 0.97 | |
| Mean VIF | 1.35 |
References
- The Human Cost of Weather Related Disasters 1995–2015; The United Nations Office for Disaster Risk Reduction (UNISDR) & Centre for Research on the Epidemiology of Disasters (CRED): Geneva, Switzerland, 2015.
- Beaglehole, B.; Mulder, R.T.; Frampton, C.M.; Boden, J.M.; Newton-Howes, G.; Bell, C.J. Psychological distress and psychiatric disorder after natural disasters: Systematic review and meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2018, 213, 716–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnberg, F.K.; Gudmundsdottir, R.; Butwicka, A.; Fang, F.; Lichtenstein, P.; Hultman, C.M.; Valdimarsdottir, U.A. Psychiatric disorders and suicide attempts in Swedish survivors of the 2004 southeast Asia tsunami: A 5 year matched cohort study. Lancet Psychiatry 2015, 2, 817–824. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R. The impact of natural disasters on mental health. InPsych Bull. Aust. Psychol. Soc. 2009, 31, 8. [Google Scholar]
- Fergusson, D.M.; Horwood, L.J.; Boden, J.M.; Mulder, R.T. Impact of a major disaster on the mental health of a well-studied cohort. JAMA Psychiatry 2014, 71, 1025–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, R.D.; Galea, S. Science for the community: Assessing mental health after 9/11. J. Clin. Psychiatry 2004, 65 (Suppl. S1), 37–43. [Google Scholar]
- Ando, S.; Kuwabara, H.; Araki, T.; Kanehara, A.; Tanaka, S.; Morishima, R.; Kondo, S.; Kasai, K. Mental Health Problems in a Community After the Great East Japan Earthquake in 2011: A Systematic Review. Harv. Rev. Psychiatry 2017, 25, 15–28. [Google Scholar] [CrossRef]
- McGuire, A.P.; Gauthier, J.M.; Anderson, L.M.; Hollingsworth, D.W.; Tracy, M.; Galea, S.; Coffey, S.F. Social Support Moderates Effects of Natural Disaster Exposure on Depression and Posttraumatic Stress Disorder Symptoms: Effects for Displaced and Nondisplaced Residents. J. Trauma. Stress 2018, 31, 223–233. [Google Scholar] [CrossRef]
- Arnberg, F.K.; Hultman, C.M.; Michel, P.O.; Lundin, T. Social support moderates posttraumatic stress and general distress after disaster. J. Trauma. Stress 2012, 25, 721–727. [Google Scholar] [CrossRef]
- Watanabe, C.; Okumura, J.; Chiu, T.Y.; Wakai, S. Social support and depressive symptoms among displaced older adults following the 1999 Taiwan earthquake. J. Trauma. Stress 2004, 17, 63–67. [Google Scholar] [CrossRef]
- Lowe, S.R.; Chan, C.S.; Rhodes, J.E. Pre-hurricane perceived social support protects against psychological distress: A longitudinal analysis of low-income mothers. J. Consult. Clin. Psychol. 2010, 78, 551–560. [Google Scholar] [CrossRef] [Green Version]
- Masedu, F.; Mazza, M.; Di Giovanni, C.; Calvarese, A.; Tiberti, S.; Sconci, V.; Valenti, M. Facebook, quality of life, and mental health outcomes in post-disaster urban environments: The l’aquila earthquake experience. Front. Public Health 2014, 2, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, S.K.; Dunn, R.; Amlot, R.; Greenberg, N.; Rubin, G.J. Social and occupational factors associated with psychological distress and disorder among disaster responders: A systematic review. BMC Psychol. 2016, 4, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoits, P.A. Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, B.J.; Sou, K.; Chen, W.; Zhou, F.; Chang, K.; Latkin, C. An Evaluation of the Buffering Effects of Types and Sources of Support on Depressive Symptoms Among Natural Disaster-Exposed Chinese Adults. Psychiatry 2016, 79, 389–402. [Google Scholar] [CrossRef] [Green Version]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef]
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef]
- Parker, G.; Lie, D.; Siskind, D.J.; Martin-Khan, M.; Raphael, B.; Crompton, D.; Kisely, S. Mental health implications for older adults after natural disasters--a systematic review and meta-analysis. Int. Psychogeriatr. 2016, 28, 11–20. [Google Scholar] [CrossRef]
- Cherniack, E.P. The impact of natural disasters on the elderly. Am. J. Disaster Med. 2008, 3, 133–139. [Google Scholar] [CrossRef]
- Agency, N.P. Police Measures and Damage Situation of the 2011 Great East Japan Earthquake and Tsunami; The National Police Agency: Tokyo, Japan, 2019.
- Tomita, H. Perspectives on researches in disaster psychiatry. Seishin Shinkeigaku Zasshi Psychiatr. Neurol. Jpn. 2014, 116, 231–237. [Google Scholar]
- Rasid, H.; Shuncai, S.; Xiubo, Y.; Chen, Z. Structural vs non-structural flood-alleviation measures in the Yangtze Delta: A pilot survey of floodplain residents’ preferences. Disasters 1996, 20, 93–110. [Google Scholar] [CrossRef]
- Aldrich, D.P.; Kyota, E. Creating Community Resilience Through Elder-Led Physical and Social Infrastructure. Disaster Med. Public Health Prep. 2017, 11, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrera, M. Distinctions between social support concepts, measures, and models. Am. J. Community Psychol. 1986, 14, 413–445. [Google Scholar] [CrossRef]
- Lin, N.; Ye, X.; Ensel, W.M. Social support and depressed mood: A structural analysis. J. Health Soc. Behav. 1999, 344–359. [Google Scholar] [CrossRef]
- Kim, Y.C.; Kang, J. Communication, neighbourhood belonging and household hurricane preparedness. Disasters 2010, 34, 470–488. [Google Scholar] [CrossRef] [PubMed]
- Szreter, S.; Woolcock, M. Health by association? Social capital, social theory, and the political economy of public health. Int. J. Epidemiol. 2004, 33, 650–667. [Google Scholar] [CrossRef]
- Woolcock, M. The place of social capital in understanding social and economic outcomes. Can. J. Policy Res. 2001, 2, 11–17. [Google Scholar]
- Nakagawa, Y.; Shaw, R. Social capital: A missing link to disaster recovery. Int. J. Mass Emergencies Disasters 2004, 22, 5–34. [Google Scholar]
- Messer, L.C. Natural Experiment. Available online: https://www.britannica.com/science/natural-experiment (accessed on 25 April 2019).
- Hikichi, H.; Aida, J.; Tsuboya, T.; Kondo, K.; Kawachi, I. Can Community Social Cohesion Prevent Posttraumatic Stress Disorder in the Aftermath of a Disaster? A Natural Experiment From the 2011 Tohoku Earthquake and Tsunami. Am. J. Epidemiol. 2016, 183, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Tani, Y.; Sasaki, Y.; Haseda, M.; Kondo, K.; Kondo, N. Eating alone and depression in older men and women by cohabitation status: The JAGES longitudinal survey. Age Ageing 2015, 44, 1019–1026. [Google Scholar] [CrossRef] [Green Version]
- Koyama, S.; Aida, J.; Saito, M.; Kondo, N.; Sato, Y.; Matsuyama, Y.; Tani, Y.; Sasaki, Y.; Kondo, K.; Ojima, T.; et al. Community social capital and tooth loss in Japanese older people: A longitudinal cohort study. BMJ Open 2016, 6, e010768. [Google Scholar] [CrossRef] [Green Version]
- Tsuboya, T.; Aida, J.; Hikichi, H.; Subramanian, S.V.; Kondo, K.; Osaka, K.; Kawachi, I. Predictors of depressive symptoms following the Great East Japan earthquake: A prospective study. Soc. Sci. Med. 2016, 161, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiner, A.S.; Hayakawa, H.; Morimoto, T.; Kakuma, T. Screening for late life depression: Cut-off scores for the Geriatric Depression Scale and the Cornell Scale for Depression in Dementia among Japanese subjects. Int. J. Geriatr. Psychiatry 2003, 18, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, Y.; Aida, J.; Tsuji, T.; Miyaguni, Y.; Tani, Y.; Koyama, S.; Matsuyama, Y.; Sato, Y.; Tsuboya, T.; Nagamine, Y.; et al. Does the Type of Residential Housing Matter for Depressive Symptoms in the Aftermath of a Disaster? Insights from the Great East Japan Earthquake and Tsunami. Am. J. Epidemiol. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Wada, T.; Ishine, M.; Kita, T.; Fujisawa, M.; Matsubayashi, K. Depression screening of elderly community-dwelling Japanese. J. Am. Geriatr. Soc. 2003, 51, 1328–1329. [Google Scholar]
- Burke, W.J.; Roccaforte, W.H.; Wengel, S.P. The short form of the Geriatric Depression Scale: A comparison with the 30-item form. J. Geriatr. Psychiatry Neurol. 1991, 4, 173–178. [Google Scholar] [CrossRef]
- Hikichi, H.; Sawada, Y.; Tsuboya, T.; Aida, J.; Kondo, K.; Koyama, S.; Kawachi, I. Residential relocation and change in social capital: A natural experiment from the 2011 Great East Japan Earthquake and Tsunami. Sci. Adv. 2017, 3, e1700426. [Google Scholar] [CrossRef] [Green Version]
- Kaniasty, K.; Norris, F.H. Longitudinal linkages between perceived social support and posttraumatic stress symptoms: Sequential roles of social causation and social selection. J. Trauma. Stress 2008, 21, 274–281. [Google Scholar] [CrossRef]
- Taylor, S.E.; Welch, W.T.; Kim, H.S.; Sherman, D.K. Cultural differences in the impact of social support on psychological and biological stress responses. Psychol. Sci. 2007, 18, 831–837. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Sherman, D.K. “Express yourself”: Culture and the effect of self-expression on choice. J. Personal. Soc. Psychol. 2007, 92, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Tsuji, T.; Sasaki, Y.; Matsuyama, Y.; Sato, Y.; Aida, J.; Kondo, K.; Kawachi, I. Reducing depressive symptoms after the Great East Japan Earthquake in older survivors through group exercise participation and regular walking: A prospective observational study. BMJ Open 2017, 7, e013706. [Google Scholar] [CrossRef] [PubMed]
- Murata, C.; Kondo, K.; Hirai, H.; Ichida, Y.; Ojima, T. Association between depression and socio-economic status among community-dwelling elderly in Japan: The Aichi Gerontological Evaluation Study (AGES). Health Place 2008, 14, 406–414. [Google Scholar] [CrossRef] [PubMed]


| n | % | |||
|---|---|---|---|---|
| GDS scores at 2010 | Mean ± SD | 2.4 | ± | 2.3 |
| GDS scores at 2013 | Mean ± SD | 2.4 | ± | 2.4 |
| Change of GDS scores (2010→2013) | Increase (get worse) | 1073 | 34.5 | |
| No change | 840 | 27.0 | ||
| Decrease | 1198 | 38.5 | ||
| GDS score at 2010 | GDS score <5 | 2563 | 82.4 | |
| GDS score 5–9 | 534 | 17.2 | ||
| GDS score ≥10 | 14 | 0.5 | ||
| GDS score at 2013 | GDS score <5 | 2572 | 82.7 | |
| GDS score 5–9 | 520 | 16.7 | ||
| GDS score ≥10 | 19 | 0.6 | ||
| Change in neighborhood tie (2010→2013) | No tie➡No tie | 2195 | 70.6 | |
| No tie➡Tie | 257 | 8.3 | ||
| Tie➡No tie | 336 | 10.8 | ||
| Tie➡Tie | 323 | 10.4 | ||
| Sex | Male | 1417 | 45.6 | |
| Female | 1694 | 54.5 | ||
| Age | Mean ± SD | 73 | ± | 5.9 |
| Educational level | <6 | 28 | 0.9 | |
| 6–9 | 999 | 32.1 | ||
| 10–12 | 1351 | 43.4 | ||
| =>13 | 659 | 21.2 | ||
| Missing | 74 | 2.4 | ||
| Change in receiving medical treatment (2010→2013) | Treat➡Treat | 2284 | 73.4 | |
| Treat➡Non | 98 | 3.2 | ||
| Non➡Treat | 392 | 12.6 | ||
| Non➡Non | 295 | 9.5 | ||
| Missing | 42 | 1.4 | ||
| Change in living status (2010→2013) | Alone➡Alone | 239 | 7.7 | |
| Alone➡Not alone | 21 | 0.7 | ||
| Not alone➡Alone | 89 | 2.9 | ||
| Not alone➡Not alone | 2648 | 85.1 | ||
| Missing | 114 | 3.7 | ||
| Change in equivalized income (2010→2013) | No change | 568 | 18.3 | |
| Increase | 791 | 25.4 | ||
| Decrease | 969 | 31.2 | ||
| Missing | 783 | 25.2 | ||
| Change in sports club participation (2010→2013) | No change | 1828 | 58.8 | |
| Increase | 367 | 11.8 | ||
| Decrease | 389 | 12.5 | ||
| Missing | 527 | 16.9 | ||
| Change in smoking behavior (2010→2013) | Smoke➡Smoke | 232 | 7.5 | |
| Smoke➡Non | 105 | 3.4 | ||
| Non➡Smoke | 17 | 0.6 | ||
| Non➡Non | 2533 | 81.4 | ||
| Missing | 224 | 7.2 | ||
| Change in drinking behavior (2010→2013) | Drink➡Drink | 971 | 31.2 | |
| Drink➡Non | 216 | 6.9 | ||
| Non➡Drink | 66 | 2.1 | ||
| Non➡Non | 1797 | 57.8 | ||
| Missing | 61 | 2.0 | ||
| Change in employment status (2010→2013) | No work➡No work | 2151 | 69.1 | |
| No work➡Work | 78 | 2.5 | ||
| Work➡No work | 207 | 6.7 | ||
| Work➡Work | 311 | 10.0 | ||
| Missing | 364 | 11.7 | ||
| Change in self-rated economic situation (2010→2013) | Difficulty➡Difficulty | 193 | 6.2 | |
| Difficulty➡No difficulty | 314 | 10.1 | ||
| No difficulty➡Difficulty | 177 | 5.7 | ||
| No difficulty➡No difficulty | 2248 | 72.3 | ||
| Missing | 179 | 5.8 | ||
| Change in walking/day behavior (2010→2013) | Walk < 30 min➡Walk < 30 min | 605 | 19.5 | |
| Walk < 30 min➡Walk => 30 min | 448 | 14.4 | ||
| Walk => 30 min➡Walk < 30 min | 374 | 12.0 | ||
| Walk => 30 min➡Walk => 30 min | 1560 | 50.1 | ||
| Missing | 124 | 4.0 | ||
| Housing damage | Yes | 1793 | 57.6 | |
| No | 1247 | 40.1 | ||
| Missing | 71 | 2.3 | ||
| Lost family members/relatives | Yes | 830 | 26.7 | |
| No | 2281 | 73.3 | ||
| Lost friends | Yes | 488 | 15.7 | |
| No | 2623 | 84.3 | ||
| Relocation after the disaster | No relocation | 2872 | 92.3 | |
| Group relocation to prefabricated housing | 63 | 2.0 | ||
| Individual relocation to prefabricated housing | 7 | 0.2 | ||
| Existing private accommodation | 28 | 0.9 | ||
| Newly established housing | 48 | 1.5 | ||
| Missing | 93 | 3.0 |
| Variable | B | β | SE | 95% CI | p Value | ||
|---|---|---|---|---|---|---|---|
| Change in neighborhood tie | No tie➡No tie | ||||||
| (2010→2013) | No tie➡Tie | −0.05 | −0.39 | 0.17 | −0.72 | −0.06 | 0.02 |
| Tie➡No tie | 0.02 | 0.15 | 0.15 | −0.15 | 0.45 | 0.32 | |
| Tie➡Tie | 0.00 | 0.01 | 0.15 | −0.28 | 0.30 | 0.95 | |
| Sex | Male | ||||||
| Female | −0.03 | −0.12 | 0.12 | −0.35 | 0.11 | 0.32 | |
| Age | 0.02 | 0.01 | 0.01 | −0.01 | 0.02 | 0.46 | |
| Change in receiving medical treatment | Treat➡Treat | ||||||
| (2010→2013) | Treat➡Non | −0.02 | −0.18 | 0.23 | −0.63 | 0.28 | 0.45 |
| Non➡Treat | 0.02 | 0.14 | 0.13 | −0.11 | 0.39 | 0.27 | |
| Non➡Non | −0.01 | −0.04 | 0.13 | −0.29 | 0.22 | 0.79 | |
| Change in living status | Alone➡Alone | ||||||
| (2010→2013) | Alone➡Not alone | −0.02 | −0.58 | 0.65 | −1.86 | 0.70 | 0.38 |
| Not alone➡Alone | 0.01 | 0.12 | 0.33 | −0.52 | 0.76 | 0.72 | |
| Not alone➡Not alone | −0.04 | −0.24 | 0.17 | −0.57 | 0.10 | 0.17 | |
| Change in sports club participation | No change | ||||||
| (2010→2013) | Increase | −0.02 | −0.13 | 0.12 | −0.36 | 0.10 | 0.26 |
| Decrease | 0.02 | 0.11 | 0.12 | −0.12 | 0.35 | 0.34 | |
| Change in smoking behavior | Smoke➡Smoke | ||||||
| (2010→2013) | Smoke➡Non | 0.10 | 1.05 | 0.31 | 0.44 | 1.66 | 0.00 |
| Non➡Smoke | 0.04 | 1.35 | 0.80 | −0.23 | 2.92 | 0.09 | |
| Non➡Non | 0.02 | 0.13 | 0.17 | −0.20 | 0.46 | 0.44 | |
| Change in drinking behavior | Drink➡Drink | ||||||
| (2010→2013) | Drink➡Non | 0.05 | 0.36 | 0.18 | 0.01 | 0.71 | 0.04 |
| Non➡Drink | −0.03 | −0.36 | 0.29 | −0.92 | 0.20 | 0.21 | |
| Non➡Non | 0.02 | 0.09 | 0.11 | −0.14 | 0.31 | 0.45 | |
| Change in self-rated economic situation | Economic difficulty➡Economic difficulty | ||||||
| (2010→2013) | |||||||
| Economic difficulty➡No economic difficulty | −0.09 | −0.57 | 0.26 | −1.08 | −0.07 | 0.03 | |
| No economic difficulty➡Economic difficulty | 0.08 | 0.68 | 0.28 | 0.14 | 1.22 | 0.01 | |
| No economic difficulty➡No economic difficulty | 0.02 | 0.12 | 0.22 | −0.31 | 0.54 | 0.59 | |
| Change in walking/day behavior | Walk < 30 ➡Walk < 30 | ||||||
| (2010→2013) | Walk < 30 ➡Walk => 30 | −0.02 | −0.09 | 0.17 | −0.42 | 0.25 | 0.60 |
| Walk => 30➡Walk < 30 | 0.08 | 0.51 | 0.18 | 0.15 | 0.86 | 0.01 | |
| Walk => 30➡Walk => 30 | 0.02 | 0.07 | 0.12 | −0.17 | 0.31 | 0.58 | |
| Lost family members/relatives | Lost | ||||||
| No lost | −0.04 | −0.17 | 0.10 | −0.37 | 0.02 | 0.08 | |
| Lost friends | Lost | ||||||
| No lost | 0.03 | 0.18 | 0.12 | −0.07 | 0.42 | 0.16 | |
| Relocation after the disaster | No replacement | ||||||
| Group relocation to prefabricated housing | 0.04 | 0.72 | 0.41 | −0.08 | 1.52 | 0.08 | |
| Individual relocation to prefabricated housing | −0.02 | −0.58 | 0.71 | −1.97 | 0.81 | 0.41 | |
| Existing private accommodation | 0.03 | 0.67 | 0.48 | −0.27 | 1.61 | 0.16 | |
| Newly established housing | −0.01 | −0.14 | 0.34 | −0.80 | 0.52 | 0.67 | |
| R-squared = 0.053 | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, Y.; Tsuji, T.; Koyama, S.; Tani, Y.; Saito, T.; Kondo, K.; Kawachi, I.; Aida, J. Neighborhood Ties Reduced Depressive Symptoms in Older Disaster Survivors: Iwanuma Study, a Natural Experiment. Int. J. Environ. Res. Public Health 2020, 17, 337. https://doi.org/10.3390/ijerph17010337
Sasaki Y, Tsuji T, Koyama S, Tani Y, Saito T, Kondo K, Kawachi I, Aida J. Neighborhood Ties Reduced Depressive Symptoms in Older Disaster Survivors: Iwanuma Study, a Natural Experiment. International Journal of Environmental Research and Public Health. 2020; 17(1):337. https://doi.org/10.3390/ijerph17010337
Chicago/Turabian StyleSasaki, Yuri, Taishi Tsuji, Shihoko Koyama, Yukako Tani, Tami Saito, Katsunori Kondo, Ichiro Kawachi, and Jun Aida. 2020. "Neighborhood Ties Reduced Depressive Symptoms in Older Disaster Survivors: Iwanuma Study, a Natural Experiment" International Journal of Environmental Research and Public Health 17, no. 1: 337. https://doi.org/10.3390/ijerph17010337
APA StyleSasaki, Y., Tsuji, T., Koyama, S., Tani, Y., Saito, T., Kondo, K., Kawachi, I., & Aida, J. (2020). Neighborhood Ties Reduced Depressive Symptoms in Older Disaster Survivors: Iwanuma Study, a Natural Experiment. International Journal of Environmental Research and Public Health, 17(1), 337. https://doi.org/10.3390/ijerph17010337