Effects of Vibration Rolling with and without Dynamic Muscle Contraction on Ankle Range of Motion, Proprioception, Muscle Strength and Agility in Young Adults: A Crossover Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
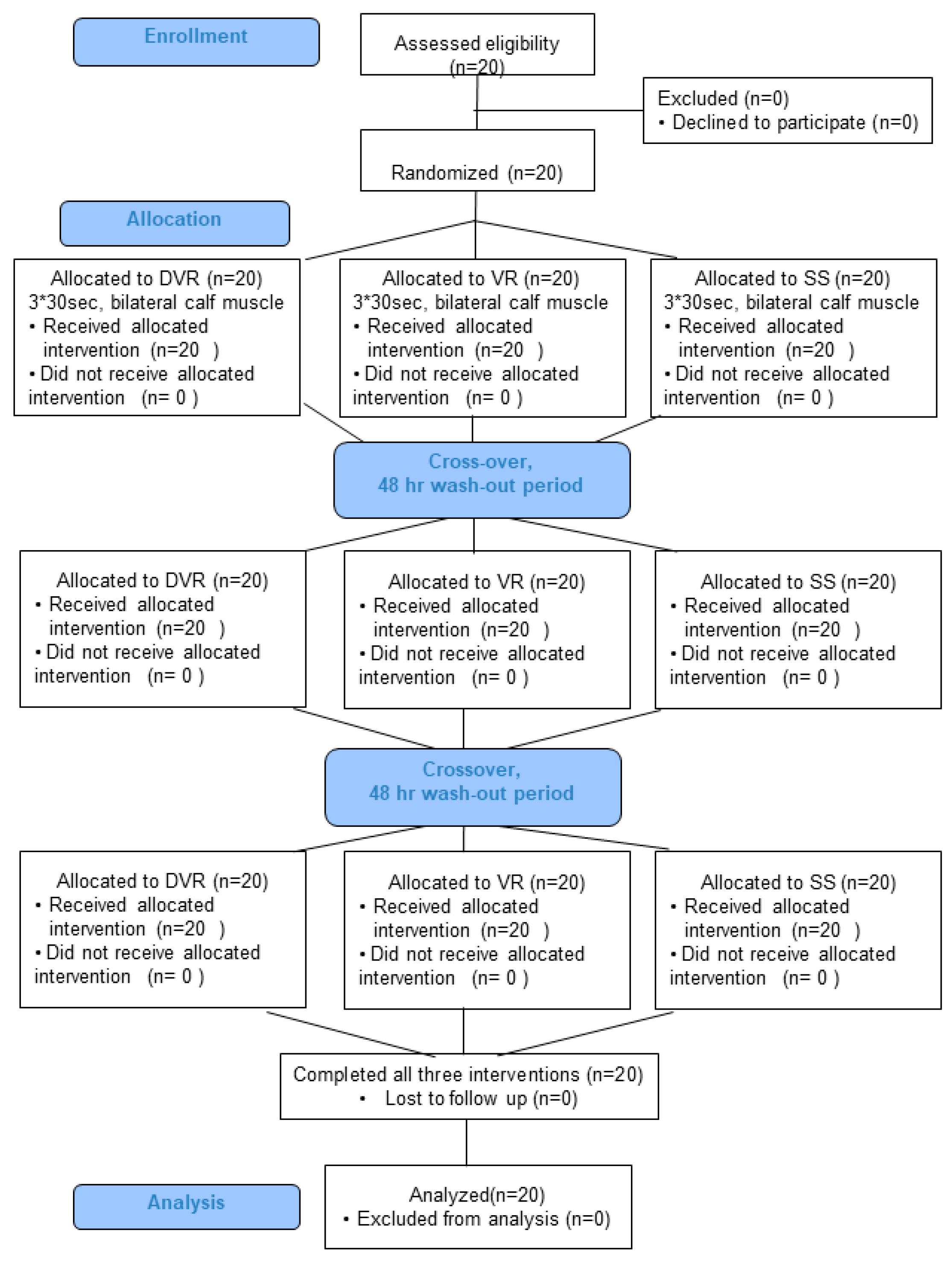
2.2. Study Procedures
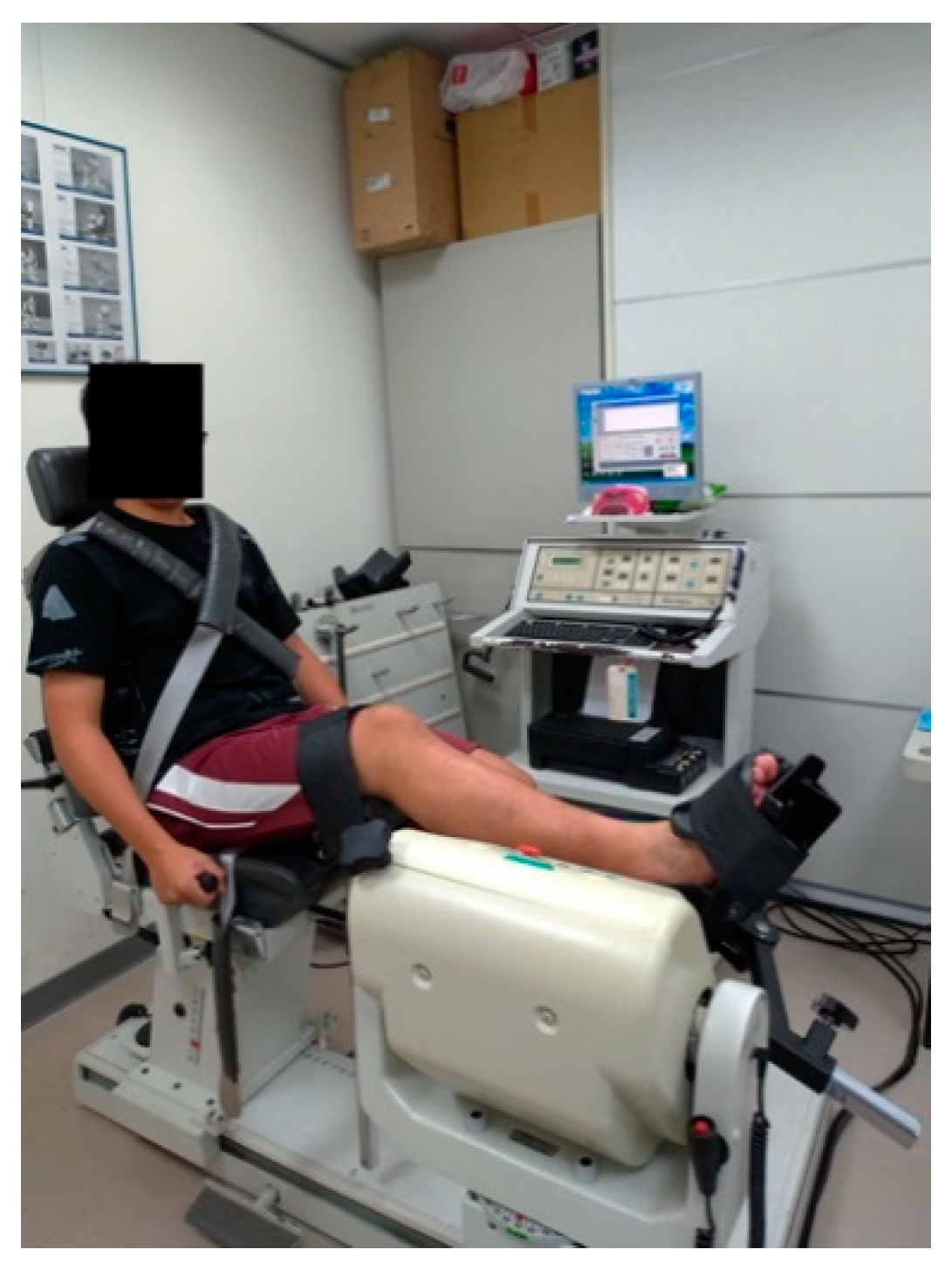
2.3. Outcome Measures
2.3.1. Primary Outcomes
2.3.2. Secondary Outcomes
2.4. Exercise Protocols
2.4.1. DVR Exercise
2.4.2. VR Exercise
2.4.3. Static Stretching
2.5. Statistical Analyses
3. Results
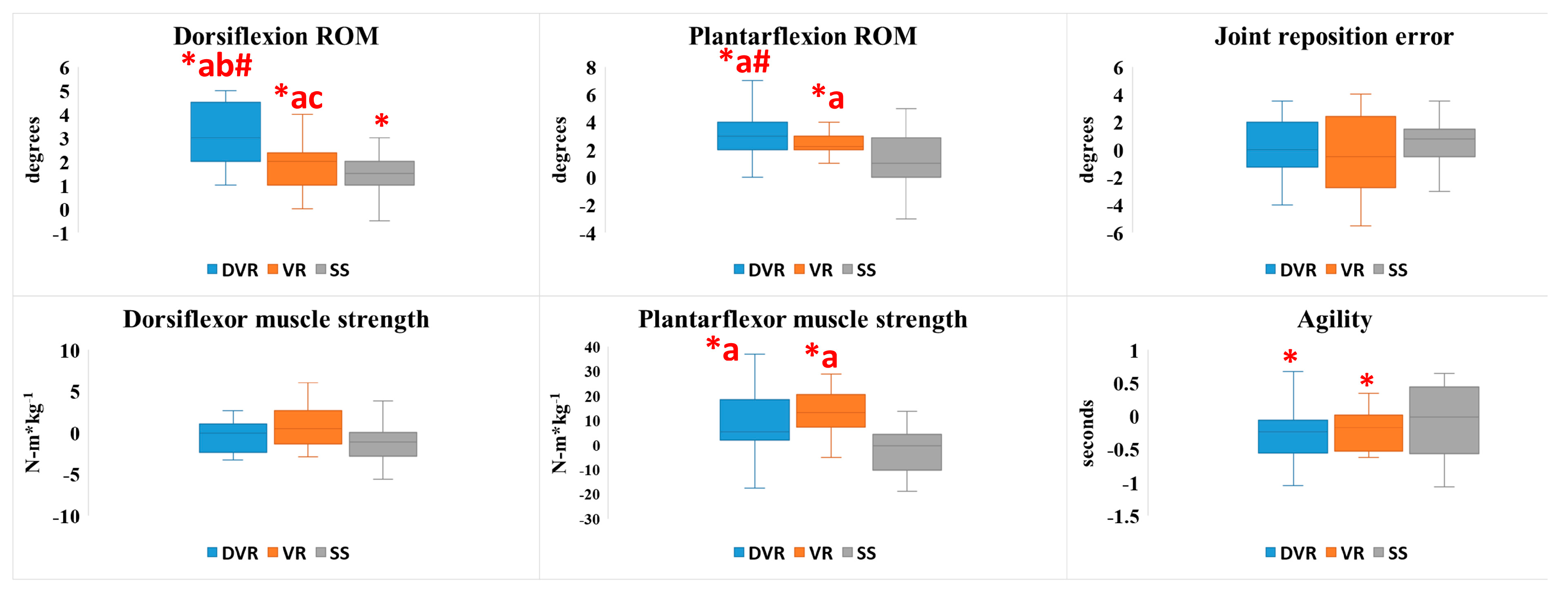
3.1. Ankle ROM Outcomes
3.2. Joint Proprioception Outcomes
3.3. Muscle Strength Outcomes
3.4. Agility Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hootman, J.M.; Dick, R.; Agel, J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J. Athl. Train. 2007, 42, 311–319. [Google Scholar]
- Owoeye, O.B.A.; Palacios-Derflingher, L.M.; Emery, C.A. Prevention of Ankle Sprain Injuries in Youth Soccer and Basketball: Effectiveness of a Neuromuscular Training Program and Examining Risk Factors. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2018, 28, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Thacker, S.B.; Gilchrist, J.; Stroup, D.F.; Kimsey, C.D., Jr. The impact of stretching on sports injury risk: A systematic review of the literature. Med. Sci. Sports Exerc. 2004, 36, 371–378. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.P.; Cosgrave, C.H. To stretch or not to stretch: The role of stretching in injury prevention and performance. Scand. J. Med. Sci. Sports 2010, 20, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Gil, H.M.; Neiva, P.H.; Sousa, C.A.; Marques, C.M.; Marinho, A.D. Current Approaches on Warming up for Sports Performance: A Critical Review. Strength Cond. J. 2019, 41, 70–79. [Google Scholar] [CrossRef]
- Behm, D.G.; Chaouachi, A. A review of the acute effects of static and dynamic stretching on performance. Eur. J. Appl. Physiol. 2011, 111, 2633–2651. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kolber, M.J.; Cain, M. Comparison of Video-Guided, Live Instructed, and Self-Guided Foam Roll Interventions on Knee Joint Range of Motion and Pressure Pain Threshold: A Randomized Controlled Trial. Int. J. Sports Phys. Ther. 2017, 12, 242–249. [Google Scholar]
- MacDonald, G.Z.; Penney, M.D.; Mullaley, M.E.; Cuconato, A.L.; Drake, C.D.; Behm, D.G.; Button, D.C. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J. Strength Cond. Res. 2013, 27, 812–821. [Google Scholar] [CrossRef] [Green Version]
- Hendricks, S.; Hill, H.N.; Hollander, S.D.; Lombard, W.; Parker, R. Effects of foam rolling on performance and recovery: A systematic review of the literature to guide practitioners on the use of foam rolling. J. Bodyw. Mov. Ther. 2019. [Google Scholar] [CrossRef]
- Wiewelhove, T.; Doweling, A.; Schneider, C.; Hottenrott, L.; Meyer, T.; Kellmann, M.; Pfeiffer, M.; Ferrauti, A. A Meta-Analysis of the Effects of Foam Rolling on Performance and Recovery. Front. Physiol. 2019, 10, 376. [Google Scholar] [CrossRef] [Green Version]
- Jay, K.; Sundstrup, E.; Sondergaard, S.D.; Behm, D.; Brandt, M.; Saervoll, C.A.; Jakobsen, M.D.; Andersen, L.L. Specific and cross over effects of massage for muscle soreness: Randomized controlled trial. Int. J. Sports Phys. Ther. 2014, 9, 82–91. [Google Scholar] [PubMed]
- Cheatham, S.W.; Kolber, M.J. Does Roller Massage With a Foam Roll Change Pressure Pain Threshold of the Ipsilateral Lower Extremity Antagonist and Contralateral Muscle Groups? An Exploratory Study. J. Sport Rehabil. 2018, 27, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Chang, N.J.; Wu, W.L.; Guo, L.Y.; Chu, I.H. Acute Effects of Foam Rolling, Static Stretching, and Dynamic Stretching During Warm-Ups on Muscular Flexibility and Strength in Young Adults. J. Sport Rehabil. 2016, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Stull, K.R. Comparison of a foam rolling session with active joint motion and without joint motion: A randomized controlled trial. J. Bodyw. Mov. Ther. 2018, 22, 707–712. [Google Scholar] [CrossRef]
- Houston, M.N.; Hodson, V.E.; Adams, K.K.; Hoch, J.M. The effectiveness of whole-body-vibration training in improving hamstring flexibility in physically active adults. J. Sport Rehabil. 2015, 24, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Tseng, S.Y.; Hsu, P.S.; Lai, C.L.; Liao, W.C.; Lee, M.C.; Wang, C.H. Effect of Two Frequencies of Whole-Body Vibration Training on Balance and Flexibility of the Elderly: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2016, 95, 730–737. [Google Scholar] [CrossRef]
- Bakhtiary, A.H.; Safavi-Farokhi, Z.; Aminian-Far, A. Influence of vibration on delayed onset of muscle soreness following eccentric exercise. Br. J. Sports Med. 2007, 41, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Imtiyaz, S.; Veqar, Z.; Shareef, M.Y. To Compare the Effect of Vibration Therapy and Massage in Prevention of Delayed Onset Muscle Soreness (DOMS). J. Clin. Diagn. Res. JCDR 2014, 8, 133–136. [Google Scholar] [CrossRef]
- Rehn, B.; Lidstrom, J.; Skoglund, J.; Lindstrom, B. Effects on leg muscular performance from whole-body vibration exercise: A systematic review. Scand. J. Med. Sci. Sports 2007, 17, 2–11. [Google Scholar] [CrossRef]
- Cardinale, M.; Lim, J. Electromyography activity of vastus lateralis muscle during whole-body vibrations of different frequencies. J. Strength Cond. Res. 2003, 17, 621–624. [Google Scholar]
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin. Physiol. 2001, 21, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Park, C.B. The immediate effects of foam roller with vibration on hamstring flexibility and jump performance in healthy adults. J. Exerc. Rehabil. 2019, 15, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Moraleda, B.; Gonzalez-Garcia, J.; Cuellar-Rayo, A.; Balsalobre-Fernandez, C.; Munoz-Garcia, D.; Morencos, E. Effects of Vibration and Non-Vibration Foam Rolling on Recovery after Exercise with Induced Muscle Damage. J. Sports Sci. Med. 2019, 18, 172–180. [Google Scholar] [PubMed]
- Cheatham, S.W.; Stull, K.R.; Kolber, M.J. Comparison of a Vibration Roller and a Nonvibration Roller Intervention on Knee Range of Motion and Pressure Pain Threshold: A Randomized Controlled Trial. J. Sport Rehabil. 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.L.; Chu, I.H.; Lyu, B.J.; Chang, W.D.; Chang, N.J. Comparison of vibration rolling, nonvibration rolling, and static stretching as a warm-up exercise on flexibility, joint proprioception, muscle strength, and balance in young adults. J. Sports Sci. 2018, 36, 2575–2582. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Gutierrez, M.T.; Guillen-Rogel, P.; Cochrane, D.J.; Marin, P.J. Cross transfer acute effects of foam rolling with vibration on ankle dorsiflexion range of motion. J. Musculoskelet. Neuronal Interact. 2018, 18, 262–267. [Google Scholar]
- Benito, A.M.d.; Valldecabres, R.; Ceca, D.; Richards, J.; Igual, J.B.; Pablos, A. Effect of vibration vs non-vibration foam rolling techniques on flexibility, dynamic balance and perceived joint stability after fatigue. PeerJ 2019, 7, e8000. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, D.J. The potential neural mechanisms of acute indirect vibration. J. Sports Sci. Med. 2011, 10, 19–30. [Google Scholar]
- Games, K.E.; Sefton, J.M.; Wilson, A.E. Whole-body vibration and blood flow and muscle oxygenation: A meta-analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Halperin, I.; Aboodarda, S.J.; Button, D.C.; Andersen, L.L.; Behm, D.G. Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int. J. Sports Phys. Ther. 2014, 9, 92–102. [Google Scholar]
- Kelly, S.; Beardsley, C. Specific and Cross-Over Effects of Foam Rolling on Ankle Dorsiflexion Range on Motion. Int. J. Sports Phys. Ther. 2016, 11, 544–551. [Google Scholar] [PubMed]
- Kim, D.H.; An, D.H.; Yoo, W.G. Validity and reliability of ankle dorsiflexion measures in children with cerebral palsy. J. Back Musculoskelet. Rehabil. 2018, 31, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Willems, T.; Witvrouw, E.; Verstuyft, J.; Vaes, P.; De Clercq, D. Proprioception and Muscle Strength in Subjects With a History of Ankle Sprains and Chronic Instability. J. Athl. Train. 2002, 37, 487–493. [Google Scholar] [PubMed]
- Halim-Kertanegara, S.; Raymond, J.; Hiller, C.E.; Kilbreath, S.L.; Refshauge, K.M. The effect of ankle taping on functional performance in participants with functional ankle instability. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2017, 23, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Caffrey, E.; Docherty, C.L.; Schrader, J.; Klossner, J. The ability of 4 single-limb hopping tests to detect functional performance deficits in individuals with functional ankle instability. J. Orthop. Sports Phys. Ther. 2009, 39, 799–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Krause, F.; Wilke, J.; Niederer, D.; Vogt, L.; Banzer, W. Acute effects of foam rolling on passive tissue stiffness and fascial sliding: Study protocol for a randomized controlled trial. Trials 2017, 18, 114. [Google Scholar] [CrossRef] [Green Version]
- Stone, J.A. Myofascial release. Athl. Ther. Today 2000, 5, 34–35. [Google Scholar] [CrossRef]
- Hamm, K.; Alexander, C.M. Challenging presumptions: Is reciprocal inhibition truly reciprocal? A study of reciprocal inhibition between knee extensors and flexors in humans. Man. Ther. 2010, 15, 388–393. [Google Scholar] [CrossRef]
- Herda, T.J.; Herda, N.D.; Costa, P.B.; Walter-Herda, A.A.; Valdez, A.M.; Cramer, J.T. The effects of dynamic stretching on the passive properties of the muscle-tendon unit. J. Sports Sci. 2013, 31, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, T. Changes in joint range of motion and muscle-tendon unit stiffness after varying amounts of dynamic stretching. J. Sports Sci. 2017, 35, 2157–2163. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Blazevich, A.J.; Kay, A.D.; McHugh, M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: A systematic review. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Et Metab. 2016, 41, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moezy, A.; Olyaei, G.; Hadian, M.; Razi, M.; Faghihzadeh, S. A comparative study of whole body vibration training and conventional training on knee proprioception and postural stability after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2008, 42, 373–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, W.Y.; Nosaka, K. Effect of vibration treatment on symptoms associated with eccentric exercise-induced muscle damage. Am. J. Phys. Med. Rehabil. 2011, 90, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Daenen, L.; Cras, P.; Struyf, F.; Roussel, N.; Oostendorp, R.A. Nociception affects motor output: A review on sensory-motor interaction with focus on clinical implications. Clin. J. Pain 2012, 28, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, C.; Freiwald, J.; Kuhnemann, M.; Hotfiel, T.; Huttel, M.; Hoppe, M.W. Foam Rolling of the Calf and Anterior Thigh: Biomechanical Loads and Acute Effects on Vertical Jump Height and Muscle Stiffness. Sports 2019, 7. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Intervention | Pre | Post | Effect Size | F (p Value) | |
|---|---|---|---|---|---|---|
| Ankle Range of Motion | Dorsiflexion (degrees) | DVR | 11.1 ± 4.16 | 14.18 ± 3.8 * | 0.78 | condition × time: 22.741 (<0.001) |
| VR | 11.63 ± 4.23 | 13.48 ± 4.45 * | 0.43 | time factor: 103.023 (<0.001) | ||
| SS | 11.23 ± 3.73 | 12.58 ± 3.85 * | 0.36 | |||
| Plantarflexion (degrees) | DVR | 51.75 ± 5.3 | 55.1 ± 5.45 * | 0.62 | condition × time: 13.125 (<0.001) | |
| VR | 51.03 ± 5.37 | 53.48 ± 5.6 * | 0.45 | time factor: 64.668 (<0.001) | ||
| SS | 52.4 ± 5.97 | 53.68 ± 6.18 * | 0.21 | |||
| Joint Proprioception | Joint reposition error (degrees) | DVR | 3.5 ± 1.94 | 3.5 ± 1.5 | 0 | condition × time: 0.096 (0.909) |
| VR | 3.75 ± 2.51 | 3.48 ± 1.79 | 0.12 | time factor: 0.073 (0.79) | ||
| SS | 3.73 ± 2.7 | 3.78 ± 2.44 | 0.02 | |||
| Muscle Max Strength | Dorsi flexors (N-m × kg−1) | DVR | 0.43 ± 0.11 | 0.44 ± 0.09 | 0.05 | condition × time:1.447 (0.248) |
| VR | 0.43 ± 0.09 | 0.44 ± 0.1 | 0.14 | time factor: 0.153 (0.7) | ||
| SS | 0.43 ± 0.1 | 0.41 ± 0.1 | 0.13 | |||
| Plantar flexors (N-m × kg−1) | DVR | 1.22 ± 0.39 | 1.32 ± 0.35 * | 0.27 | condition × time: 9.652(<0.001) | |
| VR | 1.15 ± 0.33 | 1.28 ± 0.35 * | 0.39 | time factor t: 23.18 (<0.001) | ||
| SS | 1.15 ± 0.39 | 1.13 ± 0.35 | 0.05 | |||
| Agility | Figure-of-8 Hop test (s) | DVR | 11.05 ± 2.24 | 10.76 ± 2.05 * | 0.14 | condition × time: 1.164(0.323) |
| VR | 11.1 ± 2.29 | 10.88 ± 2.36 * | 0.09 | time factor: 12.213 (0.002) | ||
| SS | 11.03 ± 2.06 | 10.96 ± 2.17 | 0.03 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyu, B.-J.; Lee, C.-L.; Chang, W.-D.; Chang, N.-J. Effects of Vibration Rolling with and without Dynamic Muscle Contraction on Ankle Range of Motion, Proprioception, Muscle Strength and Agility in Young Adults: A Crossover Study. Int. J. Environ. Res. Public Health 2020, 17, 354. https://doi.org/10.3390/ijerph17010354
Lyu B-J, Lee C-L, Chang W-D, Chang N-J. Effects of Vibration Rolling with and without Dynamic Muscle Contraction on Ankle Range of Motion, Proprioception, Muscle Strength and Agility in Young Adults: A Crossover Study. International Journal of Environmental Research and Public Health. 2020; 17(1):354. https://doi.org/10.3390/ijerph17010354
Chicago/Turabian StyleLyu, Bo-Jhang, Chia-Lun Lee, Wen-Dien Chang, and Nai-Jen Chang. 2020. "Effects of Vibration Rolling with and without Dynamic Muscle Contraction on Ankle Range of Motion, Proprioception, Muscle Strength and Agility in Young Adults: A Crossover Study" International Journal of Environmental Research and Public Health 17, no. 1: 354. https://doi.org/10.3390/ijerph17010354
APA StyleLyu, B. -J., Lee, C. -L., Chang, W. -D., & Chang, N. -J. (2020). Effects of Vibration Rolling with and without Dynamic Muscle Contraction on Ankle Range of Motion, Proprioception, Muscle Strength and Agility in Young Adults: A Crossover Study. International Journal of Environmental Research and Public Health, 17(1), 354. https://doi.org/10.3390/ijerph17010354