Effects of Different Ankle Supports on the Single-Leg Lateral Drop Landing Following Muscle Fatigue in Athletes with Functional Ankle Instability



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
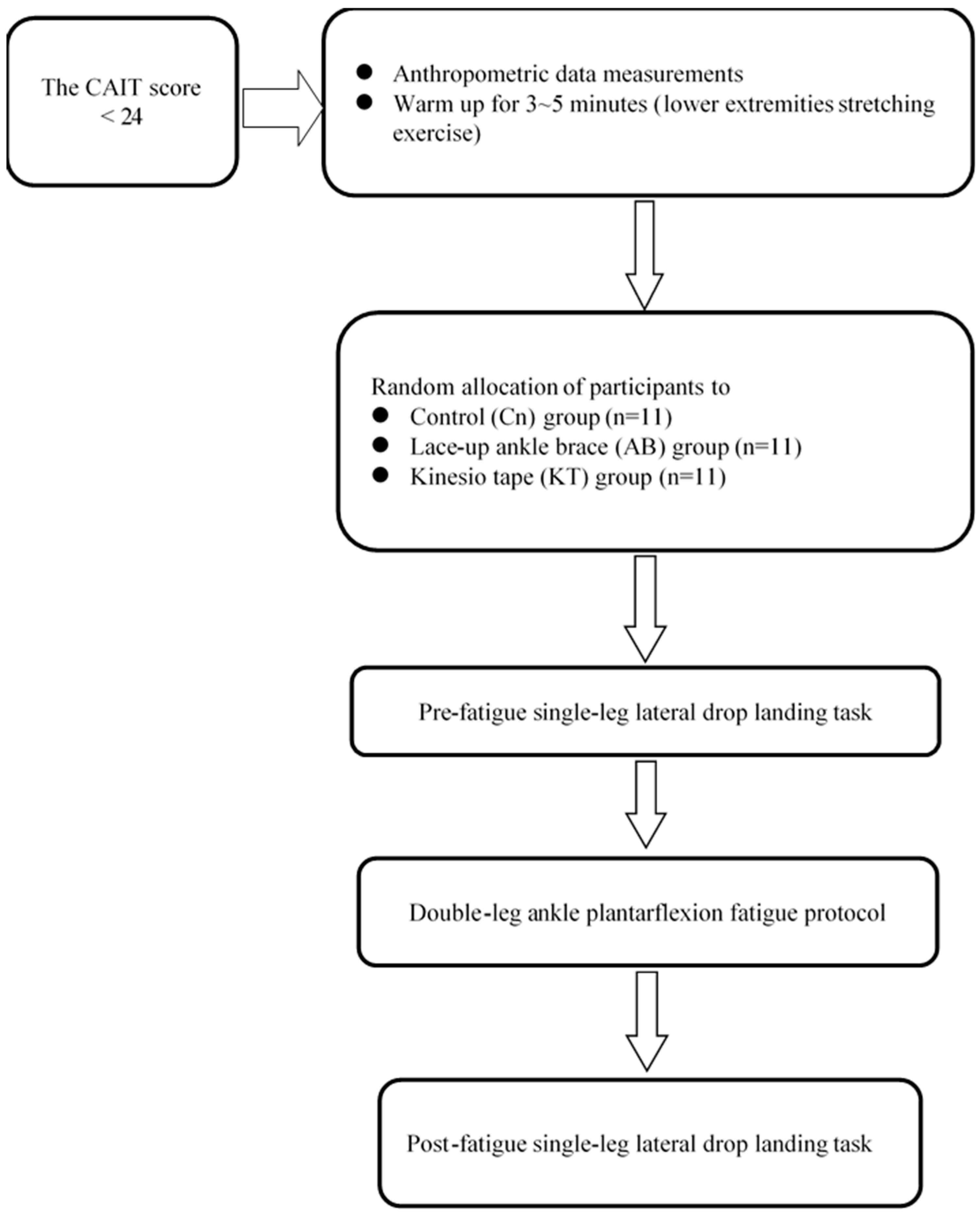
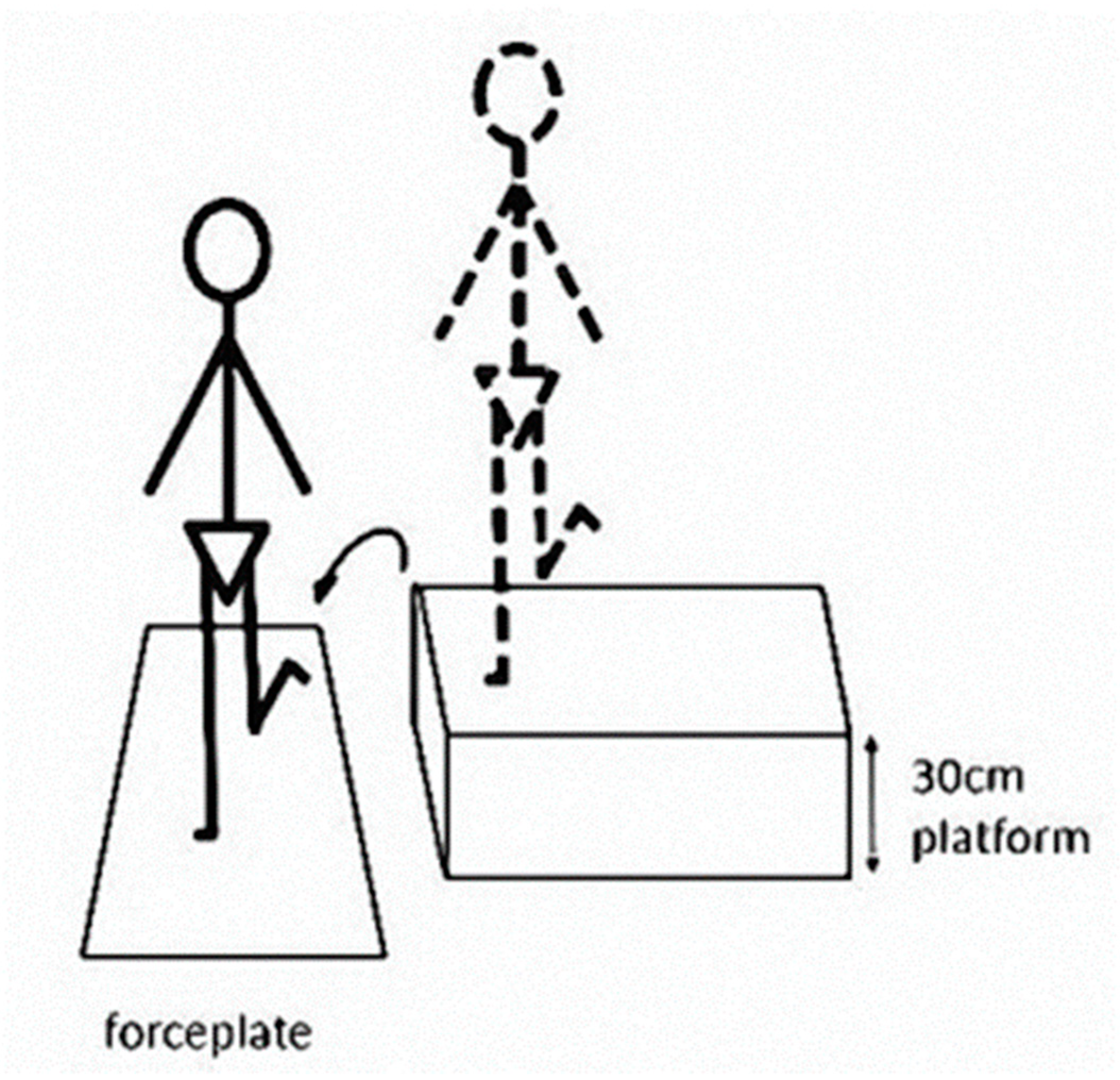
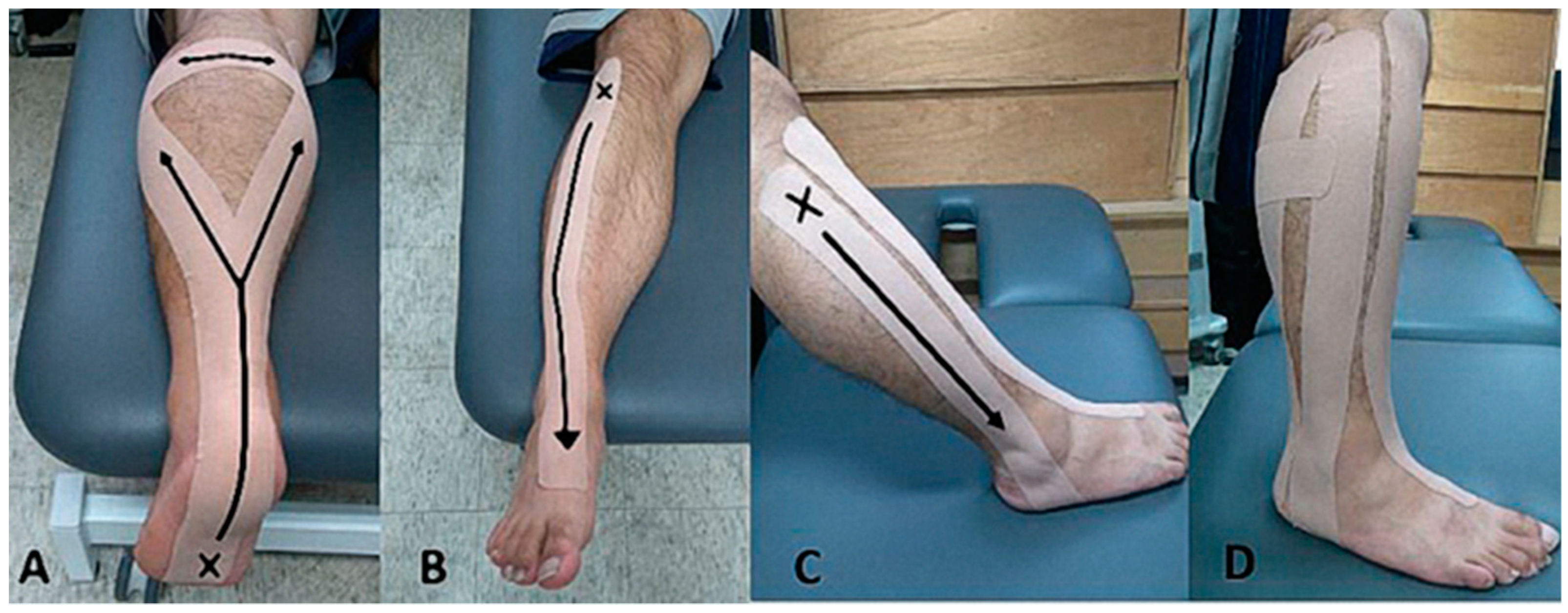
2.2. Experimental Procedure
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- McGowan, R.W.; Pierce, E.F.; Williams, M.; Eastman, N.W. Athletic injury and self diminution. J. Sports. Med. Phys. Fit. 1994, 34, 299–304. [Google Scholar]
- Usuelli, F.G.; Mason, L.; Grassi, M.; Maccario, C.; Ballal, M.; Molloy, A. Lateral ankle and hindfoot instability: A new clinical based classification. Foot Ankle Surg. 2014, 20, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.A. Instability of the foot after injuries to the lateral ligament of the ankle. J. Bone Jt. Surg. Br. 1965, 47, 669–677. [Google Scholar] [CrossRef] [Green Version]
- Refshauge, K.M.; Kilbreath, S.L.; Raymond, J. Deficits in detection of inversion and eversion movements among subjects with recurrent ankle sprains. J. Orthop. Sports Phys. Ther. 2003, 33, 166–173. [Google Scholar] [CrossRef]
- Fu, A.S.; Hui-Chan, C.W. Ankle joint proprioception and postural control in basketball players with bilateral ankle sprains. Am. J. Sports Med. 2005, 33, 1174–1182. [Google Scholar] [CrossRef]
- Wikstrom, E.A.; Tillman, M.D.; Chmielewski, T.L.; Cauraugh, J.H.; Borsa, P.A. Dynamic postural stability deficits in subjects with self-reported ankle instability. Med. Sci. Sports Exerc. 2007, 39, 397–402. [Google Scholar] [CrossRef]
- Buchanan, A.S.; Docherty, C.L.; Schrader, J. Functional performance testing in participants with functional ankle instability and in a healthy control group. J. Athl. Train. 2008, 43, 342–346. [Google Scholar] [CrossRef] [Green Version]
- Someeh, M.; Norasteh, A.A.; Daneshmandi, H.; Asadi, A. Influence of mulligan ankle taping on functional performance tests in healthy athletes and athletes with chronic ankle instability. Int. J. Athl. Ther. Train. 2015, 20, 39–45. [Google Scholar] [CrossRef]
- McGuine, T.A.; Greene, J.J.; Best, T.; Leverson, G. Balance as a predictor of ankle injuries in high school basketball players. Clin. J. Sport Med. 2000, 10, 239–244. [Google Scholar] [CrossRef]
- Ross, S.; Guskiewicz, K. Examination of static and dynamic postural stability in individuals with functionally stable and unstable ankles. Clin. J. Sport Med. 2004, 14, 332–338. [Google Scholar] [CrossRef]
- De Noronha, M.; Refshauge, K.M.; Crosbie, J.; Kilbreath, S.L. Relationship between functional ankle instability and postural control. J. Orthop. Sports Phys. Ther. 2008, 38, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.J.; Arnold, B.L.; Ross, S.E. Altered kinematics and time to stabilization during drop-jump landings in individuals with or without functional ankle instability. J. Athl. Train. 2016, 51, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Rahnama, N.; Reilly, T.; Lees, A. Injury risk associated with playing actions during competitive soccer. Br. J. Sports Med. 2002, 36, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, P.A.; Hertel, J. Effect of hip and ankle muscle fatigue on unipedal postural control. J. Electromyogr. Kinesiol. 2004, 14, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Huston, J.L.; Sandrey, M.A.; Lively, M.W.; Kotsko, K. The effects of calf muscle fatigue on sagittal-plane joint-position sense in the ankle. J. Sport Rehabil. 2005, 14, 168–184. [Google Scholar] [CrossRef]
- Yalfani, A.; Gandomi, F.; Abbasi, H. The effect of fatigue on the ankle and knee proprioception and dynamic control of posture. Inter. J. Sports Sci. Fit. 2013, 3, 221–229. [Google Scholar]
- Santamaria, L.J.; Webster, K.E. The effect of fatigue on lower-limb biomechanics during single-limb landings: A systematic review. J. Orthop. Sports Phys. Ther. 2010, 40, 464–473. [Google Scholar] [CrossRef] [Green Version]
- Caulfield, B.; Garrett, M. Changes in ground reaction force during jump landing in subjects with functional instability of the ankle joint. Clin. Biomech. 2004, 19, 617–621. [Google Scholar] [CrossRef]
- Verhagen, E.A.; Bay, K. Optimising ankle sprain prevention: A critical review and practical appraisal of the literature. Br. J. Sports Med. 2010, 44, 1082–1088. [Google Scholar] [CrossRef]
- Niu, W.X.; Feng, T.N.; Wang, L.J.; Jiang, C.H.; Zhang, M. Effects of Prophylactic Ankle Supports on Vertical Ground Reaction Force during Landing: A Meta-analysis. J. Sports Sci. Med. 2016, 15, 1–10. [Google Scholar]
- Bicici, S.; Karatas, N.; Baltaci, G. Effect of athletic taping and kinesiotaping on measurements of functional performance in basketball players with chronic inversion ankle sprains. Int. J. Sports Phys. Ther. 2012, 7, 154–166. [Google Scholar]
- Kuni, B.; Mussler, J.; Kalkum, E. Effect of kinesiotaping, non-elastic taping and bracing on segmental foot kinematics during drop landing in healthy subjects and subjects with chronic ankle instability. Physiotherapy 2016, 102, 287–293. [Google Scholar] [CrossRef]
- Wang, Y.; Gu, Y.; Chen, J.; Luo, W.; He, W.; Han, Z.; Tian, J. Kinesio taping is superior to other taping methods in ankle functional performance improvement: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1472–1481. [Google Scholar] [CrossRef]
- Gök, H.; Örücü Atar, M.; Ateş, C.; Sonel Tur, B. Does kinesiotaping affect standing balance in healthy individuals? A pilot, double-blind, randomized-controlled study. Turk. J. Phys. Med. Rehabil. 2019, 65, 327–334. [Google Scholar] [CrossRef]
- Williams, S.; Whatman, C.; Hume, P.A.; Sheerin, K. Kinesiotaping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness. Sports Med. 2012, 42, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Barrenechea, I.A.; Garrido-Beroíza, M.A.; Achiardi, O.; Serón, P.; Marzuca-Nassr, G.N.A. systematic review of the functional effectiveness of kinesiotaping in individuals with ankle instability. Medwave 2019, 19, e7635. [Google Scholar]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland ankle instability tool: A report of validity and reliability testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.L.; Fourchet, F.; Fong, D.; Hertel, J.; Hiller, C.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J. Orthop. Sports Phys. Ther. 2013, 43, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delahunt, E.; Coughlan, G.F.; Caulfield, B.; Nightingale, E.J.; Lin, C.W.; Hiller, C.E. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med. Sci. Sports Exerc. 2010, 42, 2106–2121. [Google Scholar] [CrossRef] [PubMed]
- Rodacki, A.F.; Fowler, N.E.; Bennet, S. Multi-segment coordination: Fatigue effects. Med. Sci. Sports Exerc. 2001, 33, 1157–1167. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic applications of the Kinesio Taping Method; Kinesio Taping Association: Albuquerque, NM, USA, 2003. [Google Scholar]
- Davison, E.A.; Anderson, C.T.; Ponist, B.H.; Werner, D.M.; Jacobs, M.E.; Thompson, A.J.; Cook, M.R. Inhibitory effect of the Kinesio Taping® method on the gastrocnemius muscle. Am. J. Sports Sci. Med. 2016, 4, 33–38. [Google Scholar]
- Gross, T.S.; Nelson, R.C. The shock attenuation role of the ankle during landing from a vertical jump. Med. Sci. Sports Exerc. 1988, 20, 506–514. [Google Scholar] [CrossRef]
- Zhang, S.N.; Bates, B.T.; Dufek, J.S. Contributions of lower extremity joints to energy dissipation during landings. Med. Sci. Sports Exerc. 2000, 32, 812–819. [Google Scholar] [CrossRef]
- McCaw, S.T.; Cerullo, J.F. Prophylactic ankle stabilizers affect ankle joint kinematics during drop landings. Med. Sci. Sports Exerc. 1999, 31, 702–707. [Google Scholar] [CrossRef]
- Riemann, B.L.; Schmitz, R.J.; Gale, M.; McCaw, S.T. Effect of ankle taping and bracing on vertical ground reaction forces during drop landings before and after treadmill jogging. J. Orthop. Sports Phys. Ther. 2002, 32, 628–635. [Google Scholar] [CrossRef] [Green Version]
- Sacco, Ide. C.; Takahasi, H.Y.; Suda, E.Y.; Battistella, L.R.; Kavamoto, C.A.; Lopes, J.A.; Vasconcelos, J.C. Ground reaction force in basketball cutting maneuvers with and without ankle bracing and taping. Sao Paulo Med. J. 2006, 124, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Cordova, M.L.; Takahashi, Y.; Kress, G.M.; Brucker, J.B.; Finch, A.E. Influence of external ankle support on lower extremity joint mechanics during drop landings. J. Sport Rehabil. 2018, 19, 136–148. [Google Scholar] [CrossRef]
- Salci, Y.; Kentel, B.B.; Heycan, C.; Akin, S.; Korkusuz, F. Comparison of landing maneuvers between male and female college volleyball players. Clin. Biomech. 2004, 19, 622–628. [Google Scholar] [CrossRef]
- Rowe, A.; Wright, S.; Nyland, J.; Caborn, D.N.; Kling, R. Effects of a 2-hour cheerleading practice on dynamic postural stability, knee laxity, and hamstring extensibility. J. Orthop. Sports Phys. Ther. 1999, 29, 455–462. [Google Scholar] [CrossRef]
- Wikstrom, E.; Powers, M.; Tillman, M. Dynamic stabilization time after isokinetic and functional fatigue. J. Athl. Train. 2004, 39, 247–253. [Google Scholar]
- Simpson, K.J.; Yom, J.P.; Fu, Y.C.; Arnett, S.W.; O’Rourke, S.; Brown, C.N. Does wearing a prophylactic ankle brace during drop landings affect lower extremity kinematics and ground reaction forces? J. Appl. Biomech. 2013, 29, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jafarnezhadgero, A.A.; Shahverdi, M.; Madadi Shad, M. The effectiveness of a novel Kinesio Taping technique on the ground reaction force components during bilateral drop landing in athletes with concurrent pronated foot and patella-femoral pain syndrome. J. Adv. Sport Technol. 2017, 1, 22–29. [Google Scholar]
- Ho, Y.H.; Lin, C.F.; Chang, C.H.; Wu, H.W. Effect of ankle kinesio taping on vertical jump with run-up and countermovement jump in athletes with ankle functional instability. J. Phys. Ther. Sci. 2015, 27, 2087–2090. [Google Scholar] [CrossRef] [Green Version]
- Bobbert, M.F.; Huijing, P.A.; van Ingen Schenau, G.J. Drop jumping. I. The influence of jumping technique on the biomechanics of jumping. Med. Sci. Sports Exerc. 1987, 19, 332–338. [Google Scholar] [CrossRef]
- Williams, K.R. Biomechanics of distance running. In Current Issues in Biomechanics; Grabiner, M., Ed.; Human Kinetics: Champaign, IL, USA, 1993; pp. 3–31. [Google Scholar]
- Pohl, M.B.; Mullineaux, D.R.; Milner, C.E.; Hamil, J.; Davis, I.S. Biomechanical predictors of retrospective tibial stress fractures in runners. J. Biomech. 2008, 41, 1160–1165. [Google Scholar] [CrossRef]
- Cleather, D.J.; Goodwin, J.E.; Bull, A.M. Hip and knee joint loading during vertical jumping and push jerking. Clin. Biomech. 2013, 28, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Minetti, A.E.; Ardigo, L.P.; Susta, D.; Cotelli, F. Using leg muscles as shock absorbers: Theoretical predictions and experimental results of drop landing performance. Erogonomics 1998, 41, 1771–1791. [Google Scholar] [CrossRef]
- Dai, B.; Garrett, W.E.; Gross, M.T.; Padua, D.A.; Queen, R.M.; Yu, B. The effects of 2 landing techniques on knee kinematics, kinetics, and performance during stop-jump and side-cutting tasks. Am. J. Sports Med. 2015, 43, 466–474. [Google Scholar] [CrossRef]
- Delahunt, E.; Monaghan, K.; Caulfield, B. Changes in lower limb kinematics, kinetics, and muscle activity in subjects with functional instability of the ankle joint during a single leg drop jump. J. Orthop. Res. 2006, 24, 1991–2000. [Google Scholar] [CrossRef]
- Cerullo, J.F.; Riemann, B.L.; Lephart, S.M. The combined effects of ankle and spat taping on vertical ground reaction force during drop landings. J. Athl. Train. 2000, 35, S33. [Google Scholar]
- Feuerbach, J.W.; Grabiner, M.D.; Koh, T.J.; Weiker, G.G. Effect of an ankle orthosis and ankle ligament anesthesia on ankle joint proprioception. Am. J. Sports Med. 1994, 22, 223–229. [Google Scholar] [CrossRef]
- Raymond, J.; Nicholson, L.L.; Hller, C.E.; Refshauge, K.M. The effect of ankle taping or bracing on proprioception in functional ankle instability: A systematic review and meta-analysis. J. Sci. Med. Sport 2012, 15, 386–392. [Google Scholar] [CrossRef]
- Cordova, M.L.; Ingersoll, C.D.; Palmieri, R.M. Efficacy of prophylactic ankle support: An experimental perspective. J. Athl. Train. 2002, 37, 446–457. [Google Scholar]
- Eils, E.; Demming, C.; Kollmeier, G.; Thorwesten, L.; Völker, K.; Rosenbaum, D. Comprehensive testing of 10 different ankle braces: Evaluation of passive and rapidly induced stability in subjects with chronic ankle instability. Clin. Biomech. 2002, 17, 526–535. [Google Scholar] [CrossRef]
- Cordova, M.L.; Ingersoll, C.D.; LeBlanc, M.J. Influence of ankle support on joint range of motion before and after exercise: A meta-analysis. J. Orthop. Sports Phys. Ther. 2000, 30, 170–182. [Google Scholar] [CrossRef] [Green Version]
- Shaw, M.Y.; Gribble, P.A.; Frye, J.L. Ankle bracing and fatigue on time to stabilization among collegiate volleyball athletes. J. Athl. Train. 2008, 43, 164–171. [Google Scholar] [CrossRef]
- Hadadi, M.; Mazaheri, M.; Mousavi, M.E.; Maroufi, N.; Bahrami-Zadeh, M.; Fardi-Pour, S. Effects of soft and semi-rigid ankle orthoses on postural sway in people with and without functional ankle instability. J. Sci. Med. Sport 2011, 14, 370–375. [Google Scholar] [CrossRef]
- Nakajima, M.A.; Baldridge, C. The effect of kinesio tape in vertical jump and dynamic postural control. Int. J. Sports Phys. Ther. 2013, 8, 393–406. [Google Scholar]
- Briem, K.; Eythorsdottir, H.; Magnusdottir, R.G.; Palmarsson, R.; Runarsdottir, T.; Sveinsson, T. Effects of kinesio tape compared with nonelastic sports tape and the untaped ankle during a sudden inversion perturbation in male athletes. J. Orthop. Sports Phys. Ther. 2011, 41, 328–335. [Google Scholar] [CrossRef] [Green Version]
- Nunes, G.S.; de Noronha, M.; Cunha, H.S.; Ruschel, C.; Borges, N.G. Effect of kinesio taping on jumping and balance in athletes: A crossover randomized controlled trial. J. Strength Cond. Res. 2013, 27, 3183–3189. [Google Scholar] [CrossRef] [Green Version]
- Cortesi, M.; Cattaneo, D.; Jonsdottir, J. Effect of kinesio taping on standing balance in subjects with multiple sclerosis: A pilot study. NeuroRehabilitation 2011, 28, 365–372. [Google Scholar] [CrossRef]
- Shields, C.A.; Needle, A.R.; Rose, W.C.; Swanik, C.B.; Kaminski, T.W. Effect of elastic taping on postural control deficits in subjects with healthy ankles, copers, and individuals with functional ankle instability. Foot Ankle Int. 2013, 34, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Semple, S.; Esterhuysen, C.; Grace, J. The effects of kinesio ankle taping on postural stability in semiprofessional rugby union players. J. Phys. Ther. Sci. 2012, 24, 1239–1242. [Google Scholar] [CrossRef] [Green Version]
- Simoneau, G.C.; Degner, R.M.; Kramper, C.A.; Kittleson, K.H. Changes in ankle joint proprioception resulting from strips of athletic tape applied over the skin. J. Athl. Train. 1997, 32, 141–147. [Google Scholar] [PubMed]
- Sesma, A.R.; Mattacola, C.G.; Uhl, T.L.; Nitz, A.J.; McKeon, P.O. Effect of foot orthotics on single and double limb dynamic balance tasks in patients with chronic ankle instability. Foot Ankle Spec. 2008, 1, 330–337. [Google Scholar] [CrossRef]
- Rowley, K.M.; Richards, J.G. Increasing plantarflexion angle during landing reduces vertical ground reaction forces, loading rates and the hip’s contribution to support moment within participants. J. Sports Sci. 2015, 33, 1922–1931. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control (n = 11) | Ankle Brace (n = 11) | Kinesiotape (n = 11) | p Value | |
|---|---|---|---|---|
| Gender | 8M3F | 8M3F | 9M2F | |
| Body height (cm) | 173.6 ± 7.2 | 172.6 ± 9.1 | 171.2 ± 6.5 | 0.760 |
| Body weight (kg) | 65.4 ± 6.8 | 70.1 ± 16.9 | 63.5 ± 7.7 | 0.393 |
| Age (yr) | 22.0 ± 2.8 | 22.5 ± 1.9 | 21.6 ± 3.0 | 0.724 |
| Duration of regular exercise (hr/week) | 10.0 ± 7.4 | 7.3 ± 2.9 | 9.0 ± 4.0 | 0.498 |
| CAIT score | 16.3 ± 5.9 | 16.7 ± 3.4 | 18.2 ± 4.9 | 0.632 |
| Post-fatigue RPE score | 18.0 ± 1.0 | 17.9 ± 0.8 | 17.8 ± 1.7 | 0.828 |
| Control | Ankle Brace | Kinesio Tape | K-W Test | |
|---|---|---|---|---|
| Peak vGRF (%BW) | 0.043 * | |||
| Pre-fatigue | 3.20 ± 0.33 | 3.18 ± 0.35 | 3.38 ± 0.28 | |
| Post-fatigue | 3.19 ± 0.33 | 3.32 ± 0.40 | 3.34 ± 0.33 | |
| Difference | −0.01 | 0.14 *a,*b | −0.05 | |
| Loading rate (N/ms) | ||||
| Pre-fatigue | 16.60 ± 2.71 | 17.90 ± 4.71 | 16.92 ± 2.31 | |
| Post-fatigue | 17.19 ± 2.70 | 19.78 ± 4.54 | 18.13 ± 2.52 | 0.053 |
| Difference | 0.59 | 1.88 | 1.21 | |
| Loading time (ms) | ||||
| Pre-fatigue | 123.81 ± 4.97 | 122.91 ± 9.57 | 124.64 ± 8.55 | |
| Post-fatigue | 118.97 ± 5.17 | 114.36 ± 8.69 | 114.42 ± 7.33 | 0.139 |
| Difference | −4.84 | −8.55 | −10.21 |
| Control | Ankle Brace | Kinesio Tape | K-W Test | |
|---|---|---|---|---|
| Difference of COP range | ||||
| ML (%FW) | 0.67 | 0.77 | −0.15 *a,*b | 0.046 * |
| AP (%FL) Difference of COP velocity | 0.88 | 0.57 | −0.28 *c | 0.039 * |
| ML (%FW/sec) | 3.83 | 2.16 | 2.27 | 0.808 |
| AP (%FL/sec) | −0.55 | 3.70 | −4.50 *d,*e | 0.018 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-C.; Chen, S.-J.; Lee, W.-C.; Lin, C.-F. Effects of Different Ankle Supports on the Single-Leg Lateral Drop Landing Following Muscle Fatigue in Athletes with Functional Ankle Instability. Int. J. Environ. Res. Public Health 2020, 17, 3438. https://doi.org/10.3390/ijerph17103438
Lin C-C, Chen S-J, Lee W-C, Lin C-F. Effects of Different Ankle Supports on the Single-Leg Lateral Drop Landing Following Muscle Fatigue in Athletes with Functional Ankle Instability. International Journal of Environmental Research and Public Health. 2020; 17(10):3438. https://doi.org/10.3390/ijerph17103438
Chicago/Turabian StyleLin, Cheng-Chieh, Shing-Jye Chen, Wan-Chin Lee, and Cheng-Feng Lin. 2020. "Effects of Different Ankle Supports on the Single-Leg Lateral Drop Landing Following Muscle Fatigue in Athletes with Functional Ankle Instability" International Journal of Environmental Research and Public Health 17, no. 10: 3438. https://doi.org/10.3390/ijerph17103438
APA StyleLin, C. -C., Chen, S. -J., Lee, W. -C., & Lin, C. -F. (2020). Effects of Different Ankle Supports on the Single-Leg Lateral Drop Landing Following Muscle Fatigue in Athletes with Functional Ankle Instability. International Journal of Environmental Research and Public Health, 17(10), 3438. https://doi.org/10.3390/ijerph17103438