Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK


Abstract
:1. Introduction
2. Materials and Methods
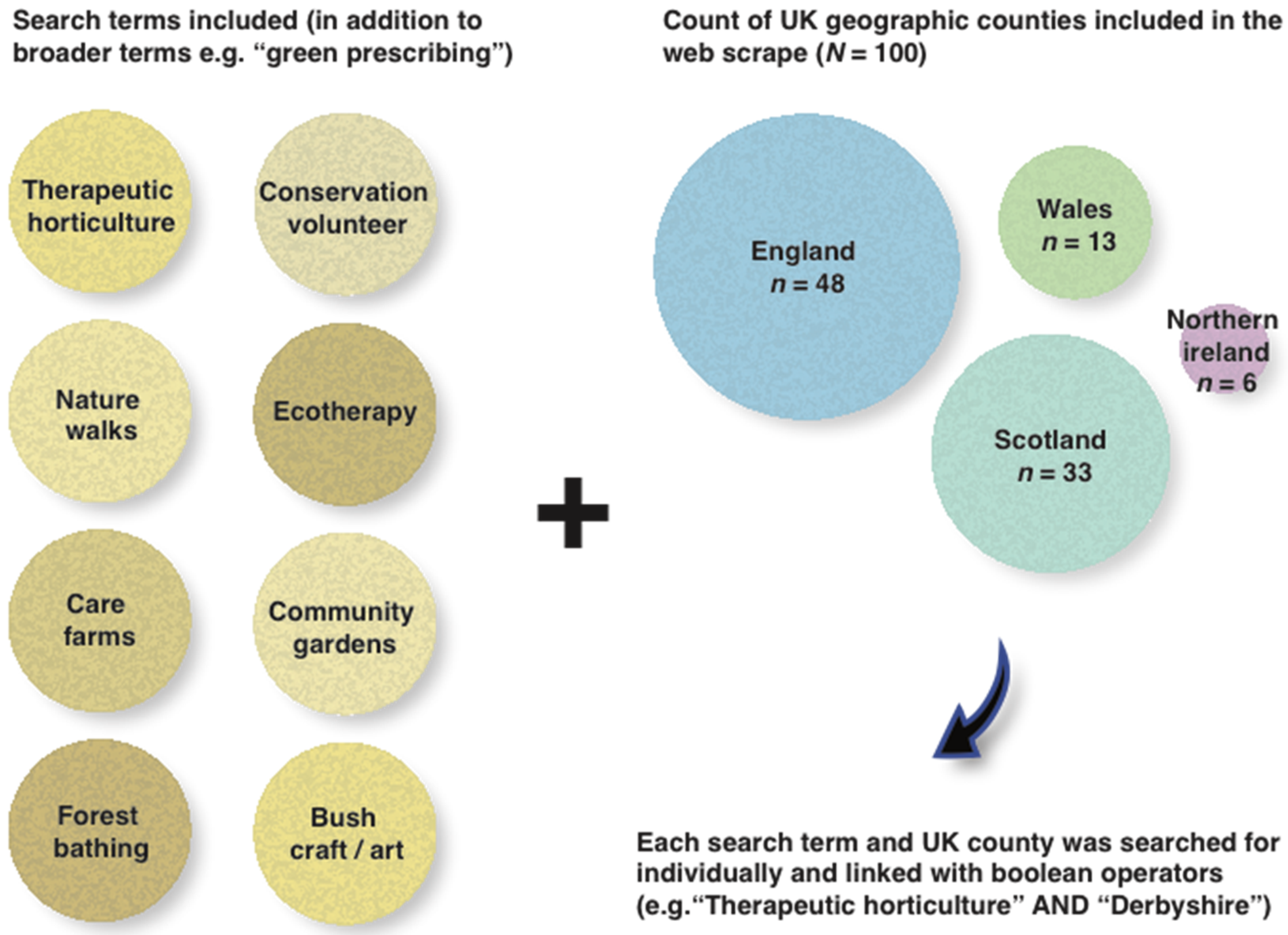
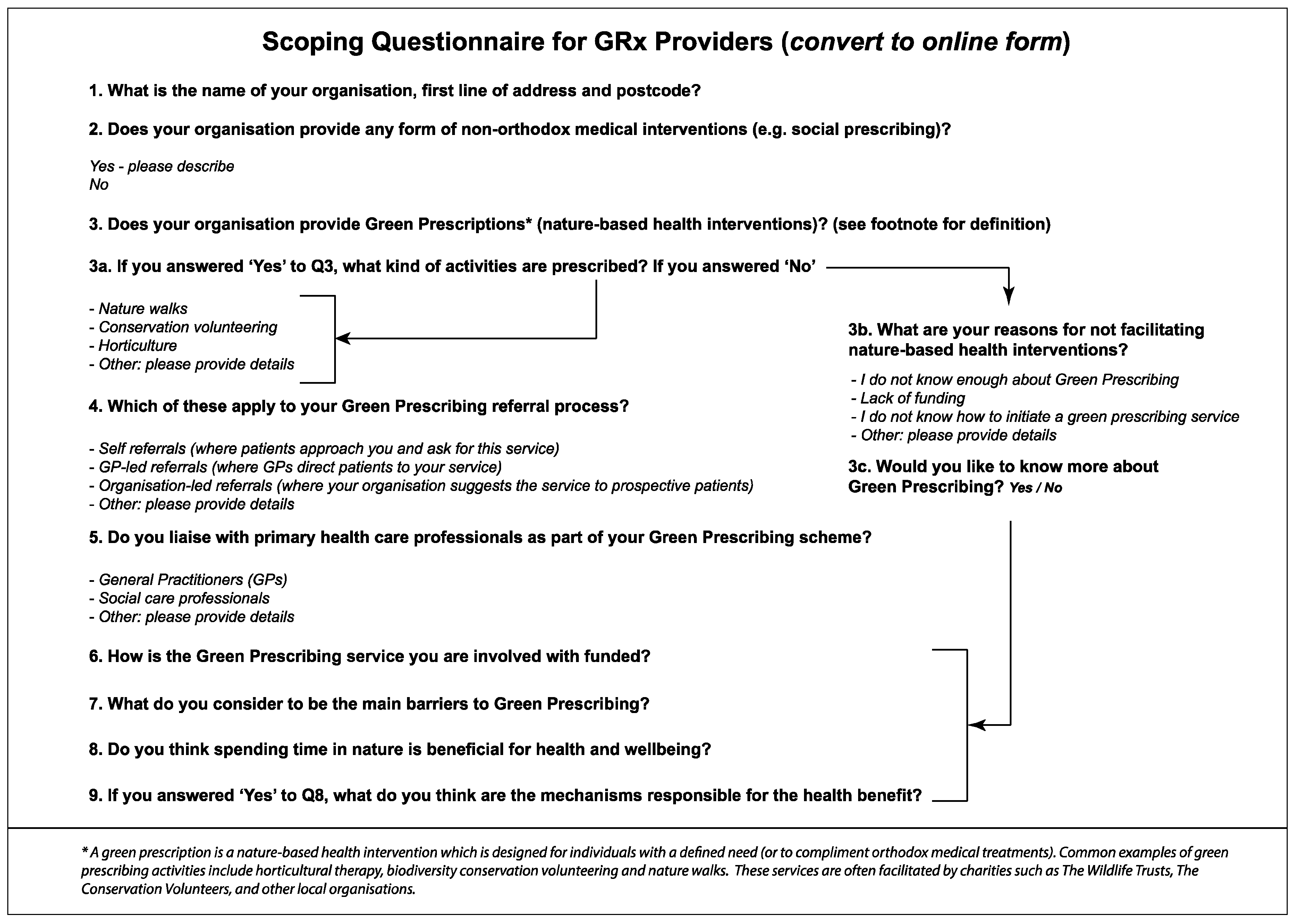
2.1. Online Questionnaire and the Web-Scrape Process
2.2. Coding of Open-Ended Responses
2.3. GIS Data
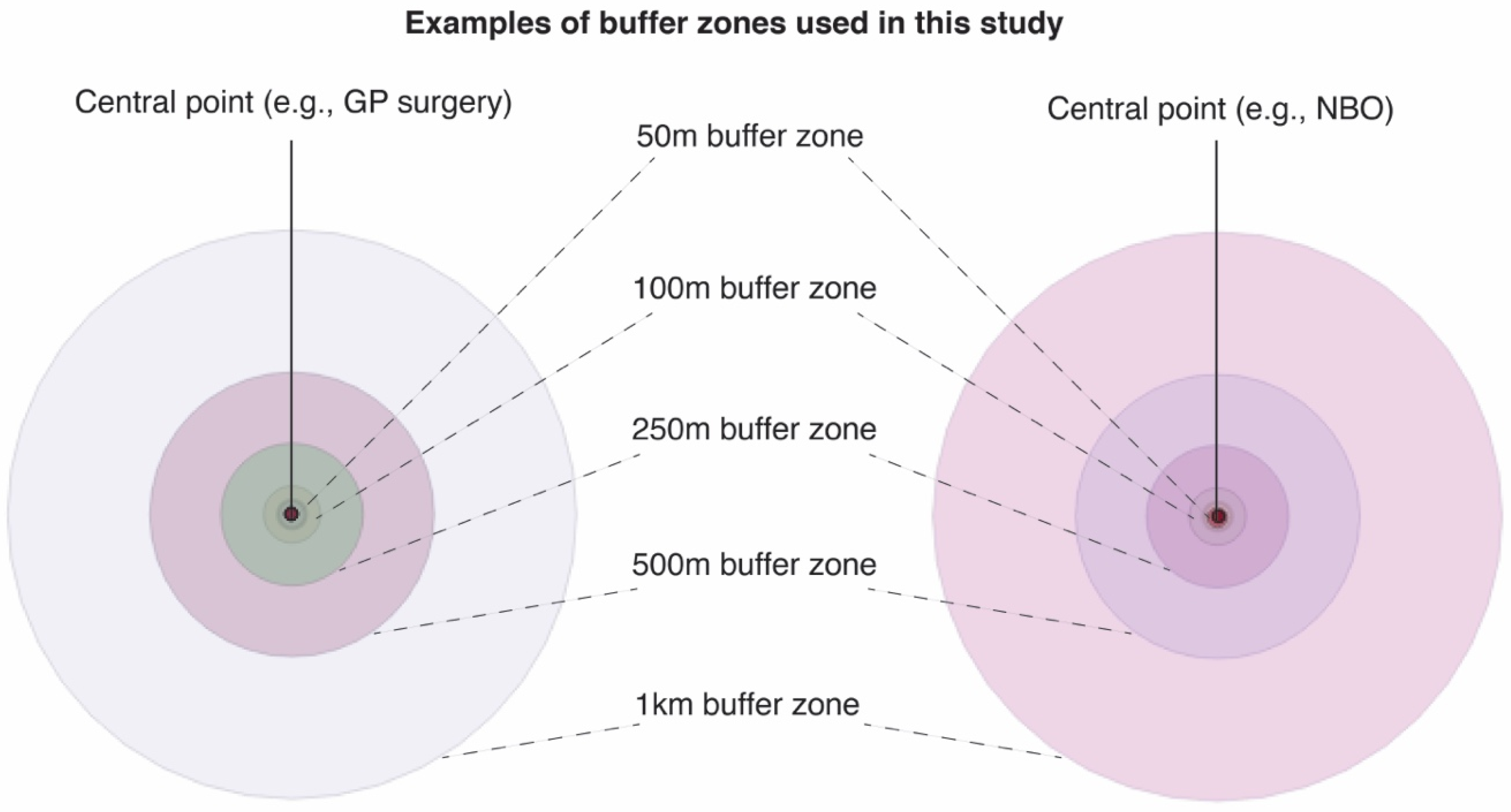
2.3.1. Buffer Analysis
2.3.2. Graduated Symbology
2.3.3. Landscape/Environmental Datasets
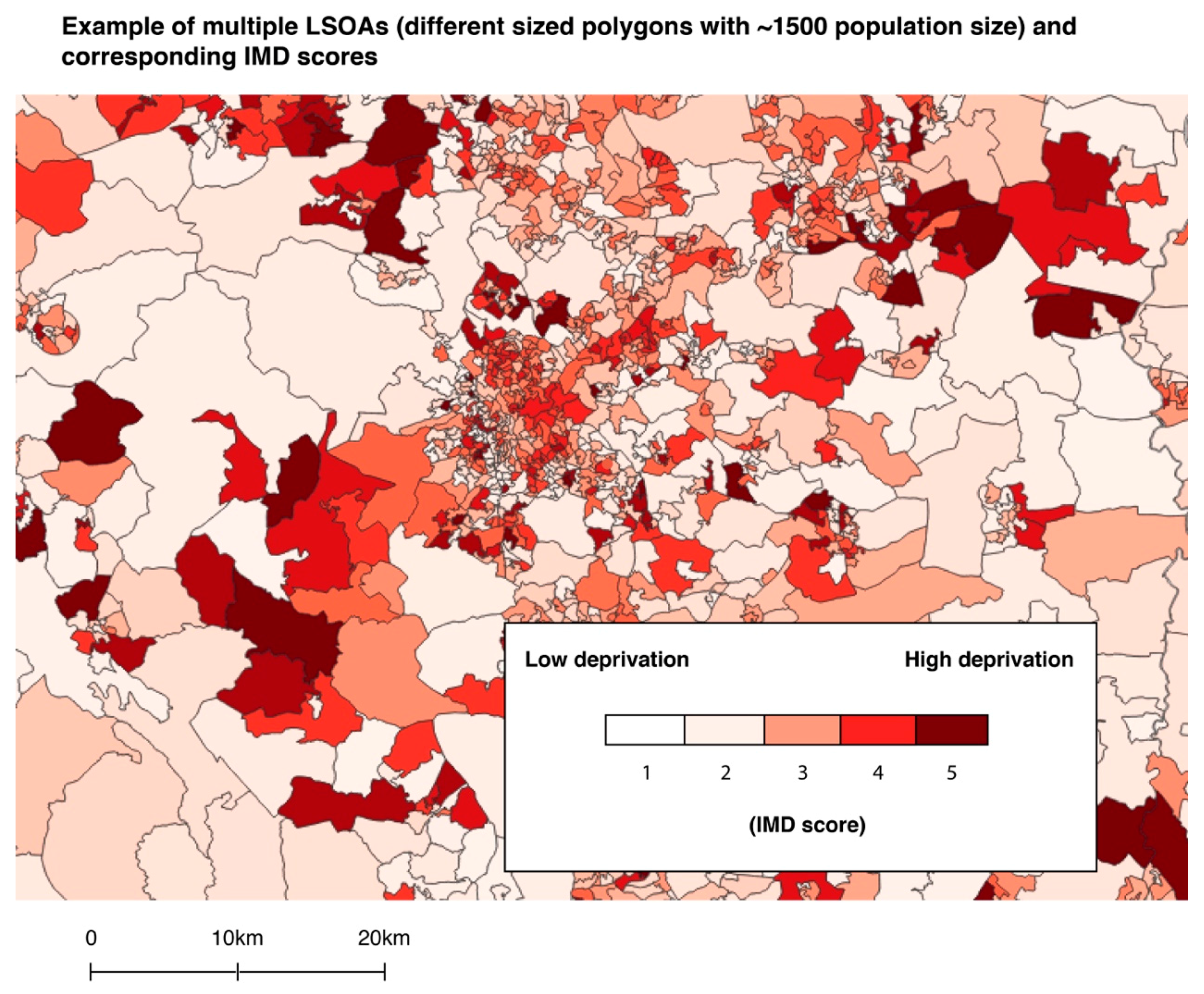
2.3.4. Deprivation Data
2.4. Spatial and Statistical Analyses
2.4.1. Landscape and Environmental Metrics
OS Open Greenspace
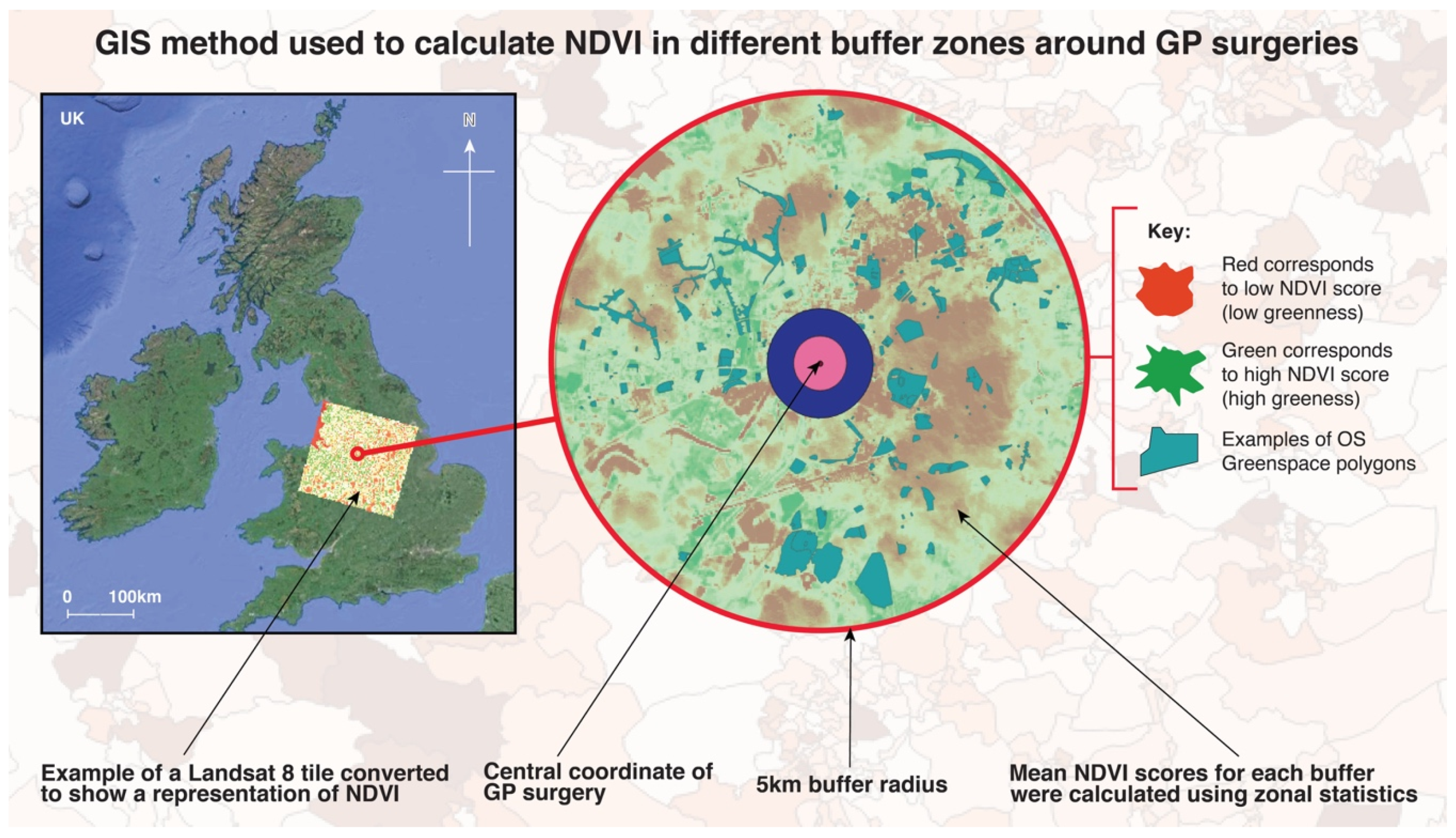
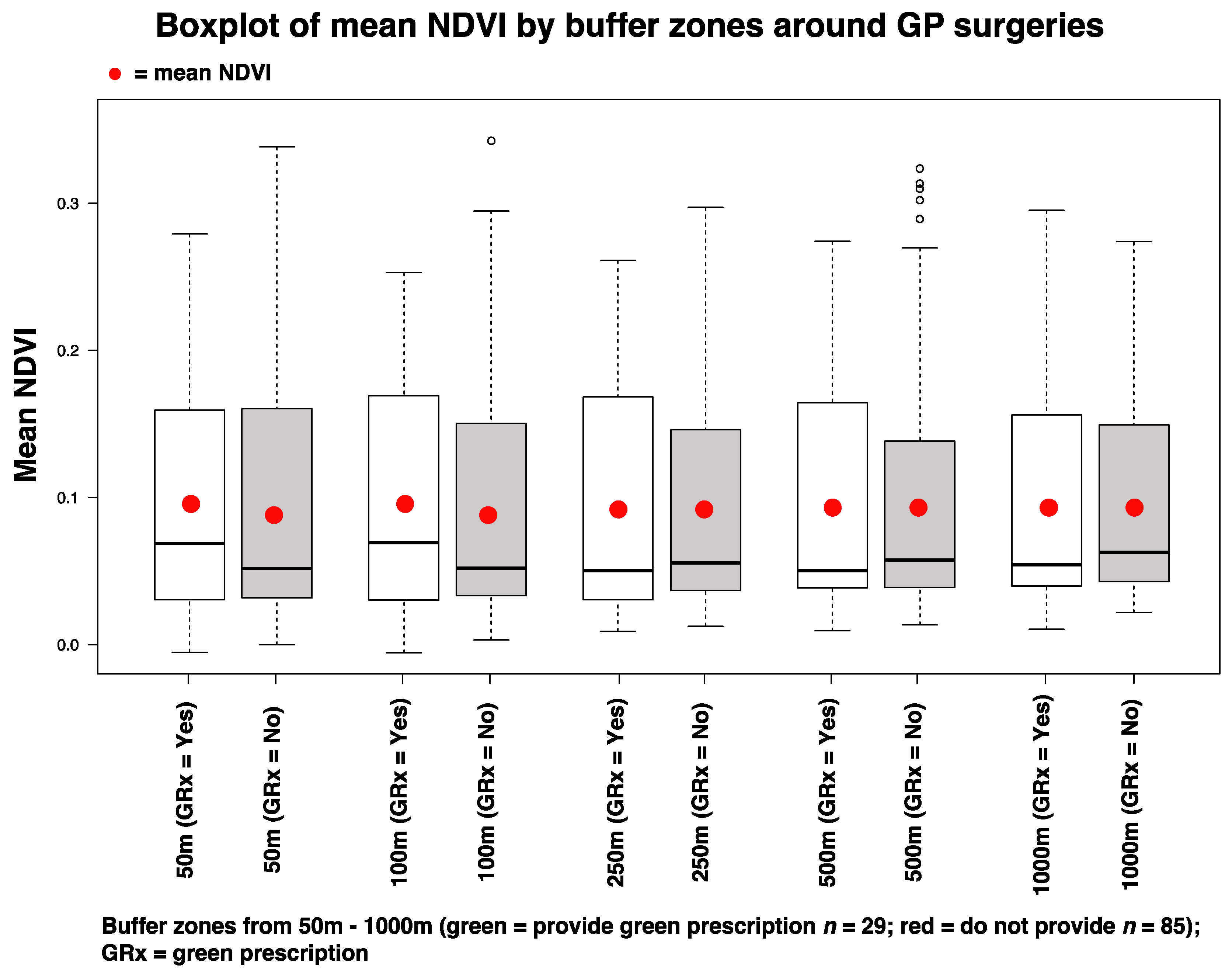
NDVI
2.4.2. Deprivation
2.4.3. Nature-Based Organisation Presence and GRx Provision
3. Results
3.1. Descriptive Statistics
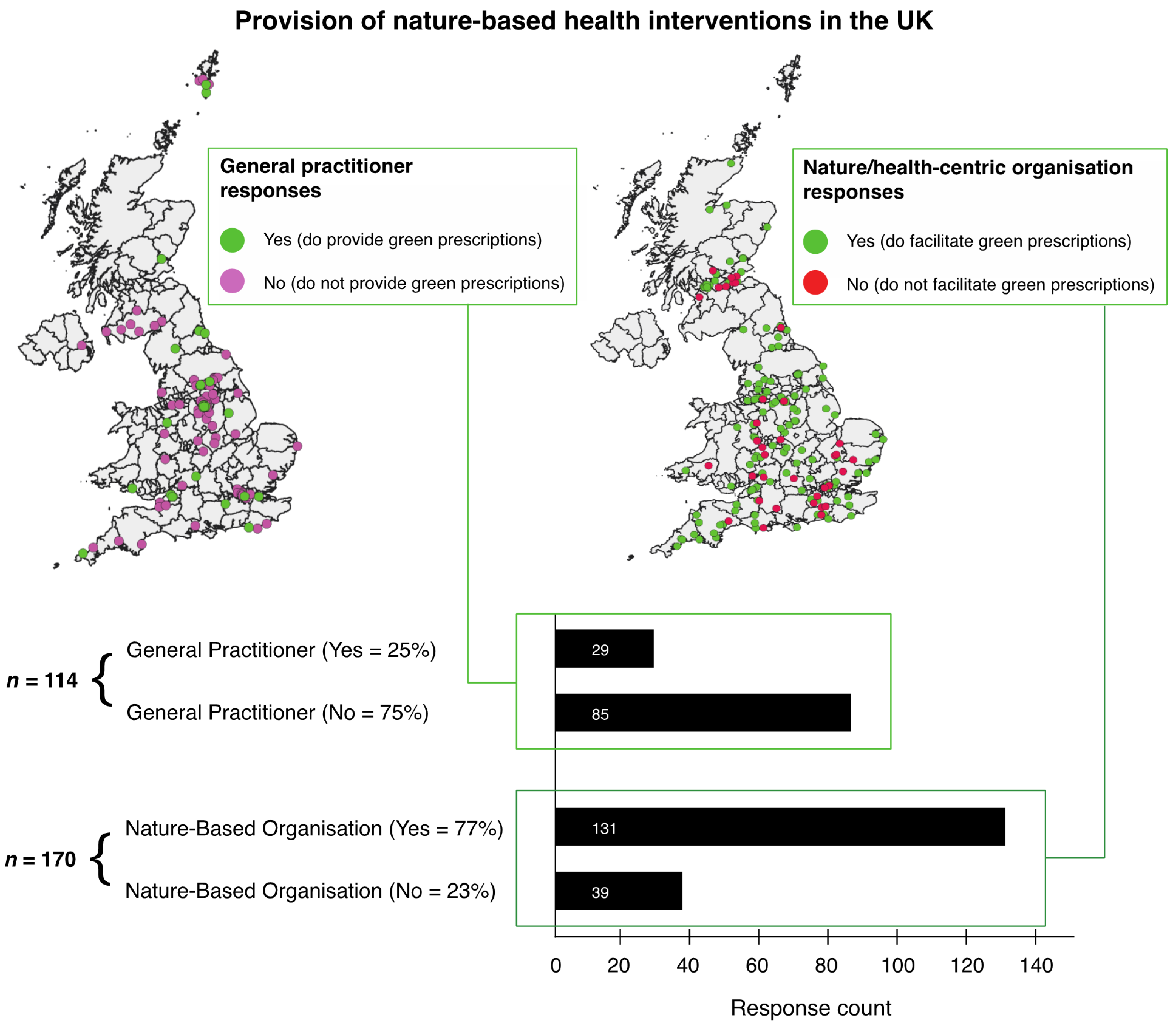
3.1.1. Results from the Questionnaire (Presence/Absence of Green Prescription Provision)
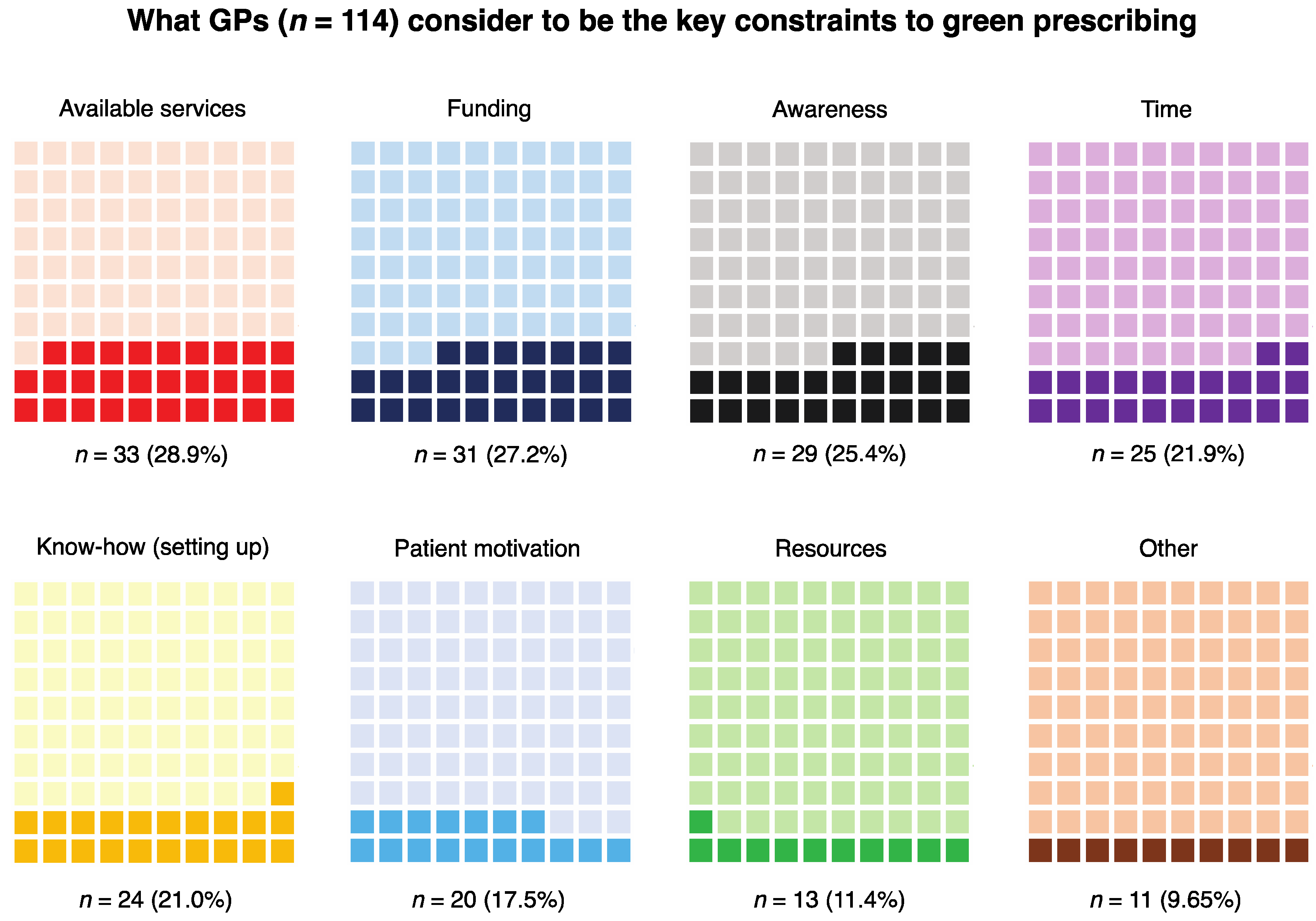
3.1.2. Results from the Coding of the Perceived Constraints Question (for GPs)
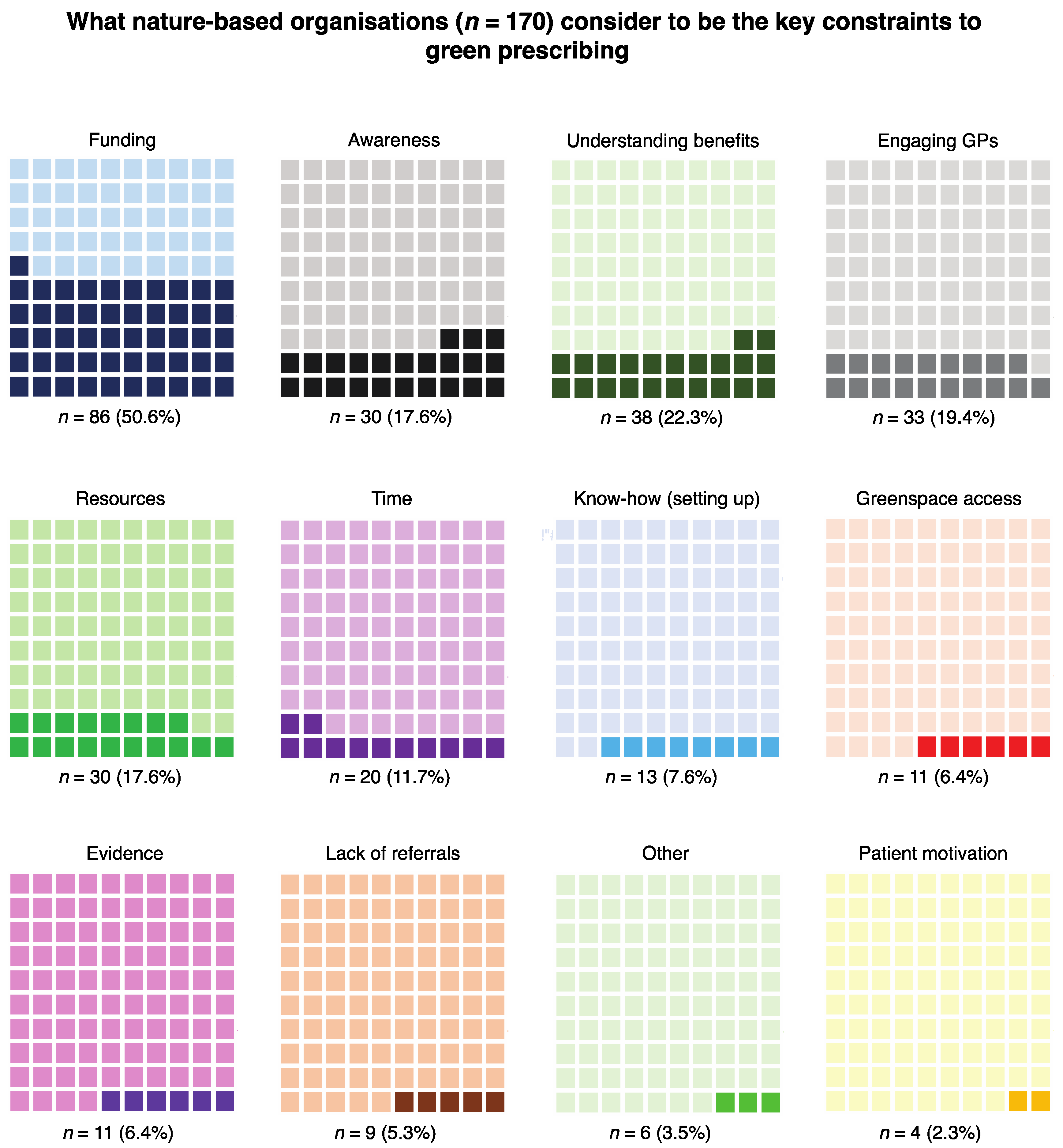
3.1.3. Results from the Coding of the Perceived Constraints Question (for Nature-Based Organisations)
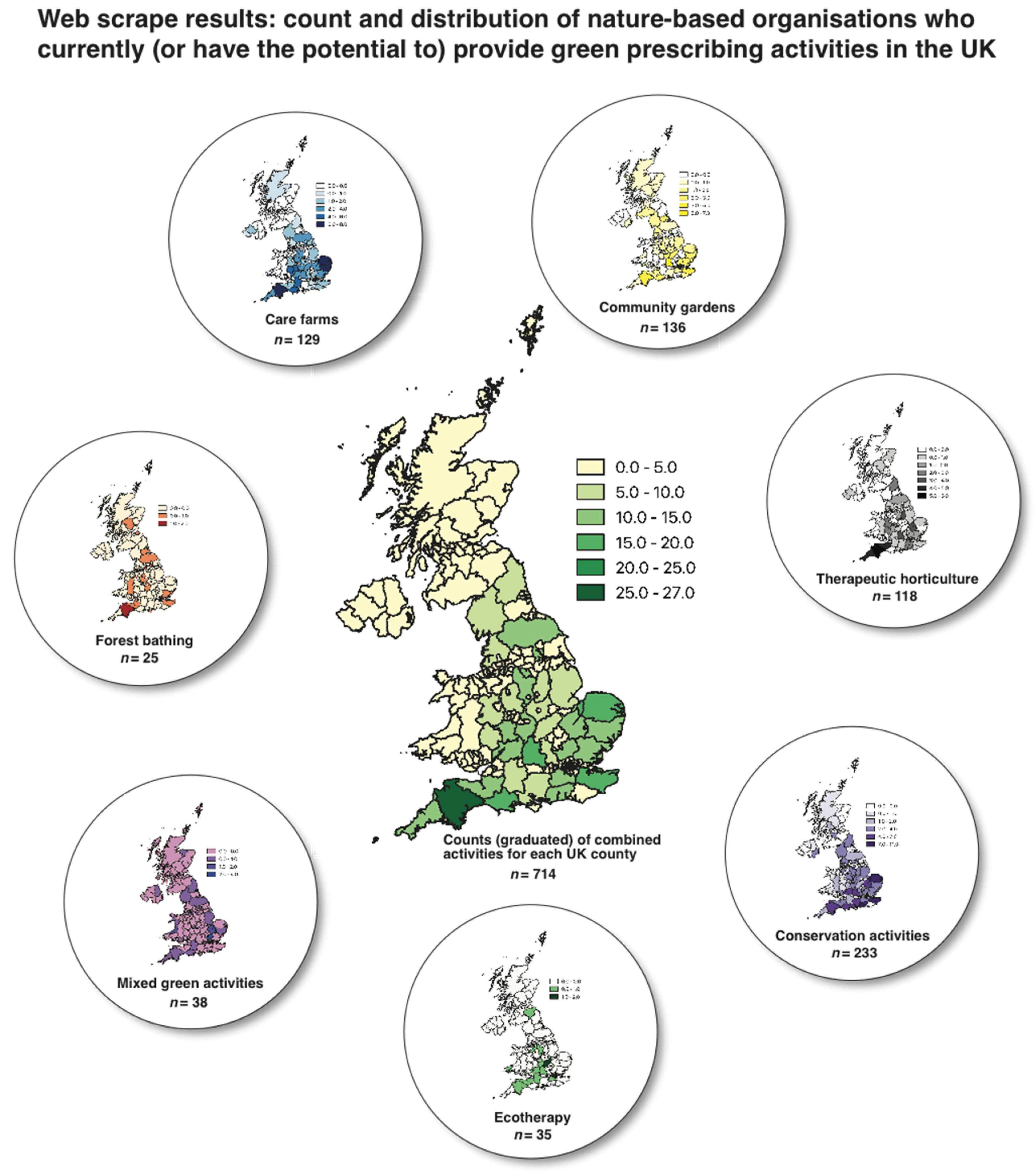
3.1.4. Results from the Web-Scrape Process (for Nature-Based Organisations)
3.2. Results from Spatial and Inferential Statistical Analyses
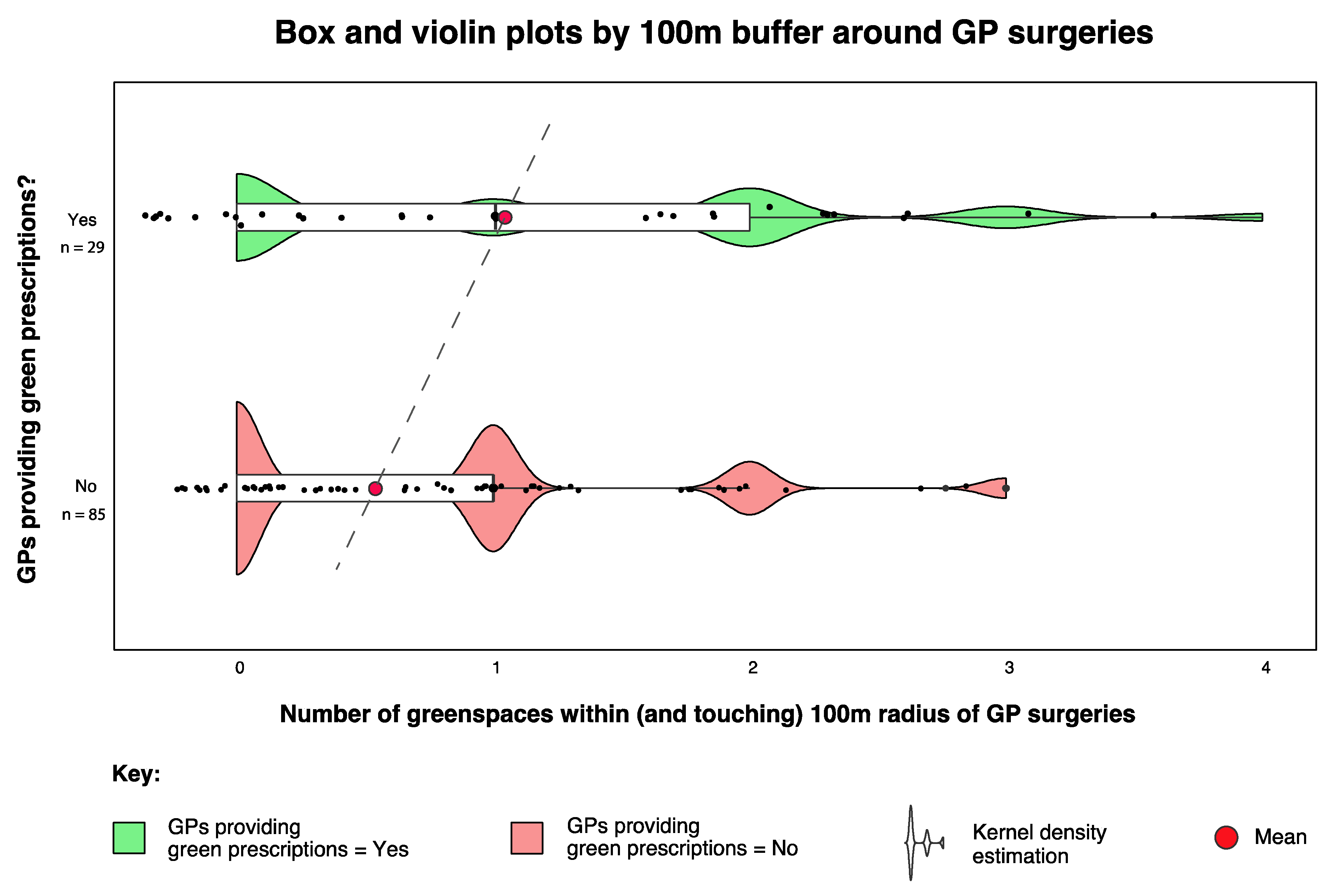
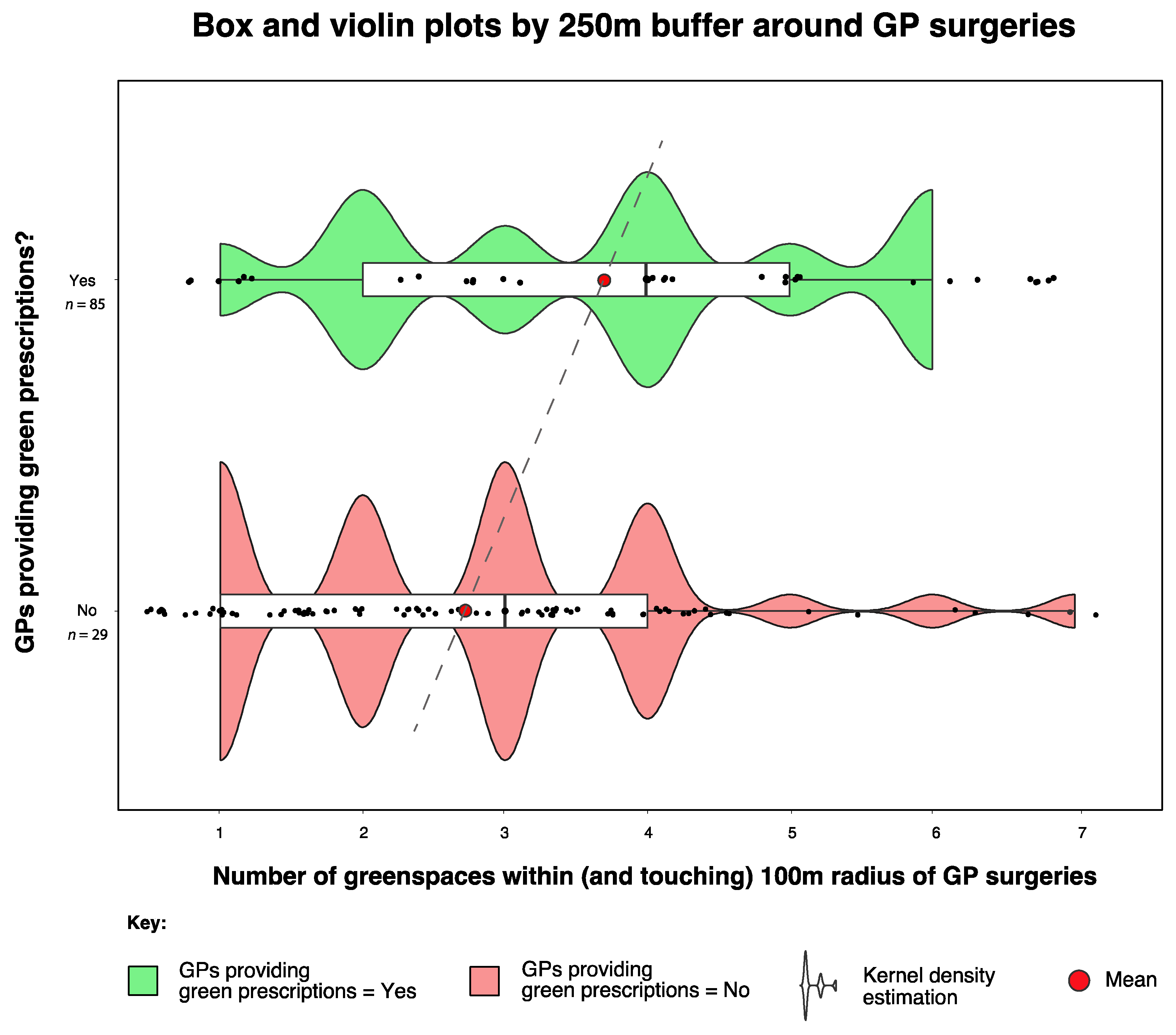
3.2.1. Landscape and Environmental Metrics
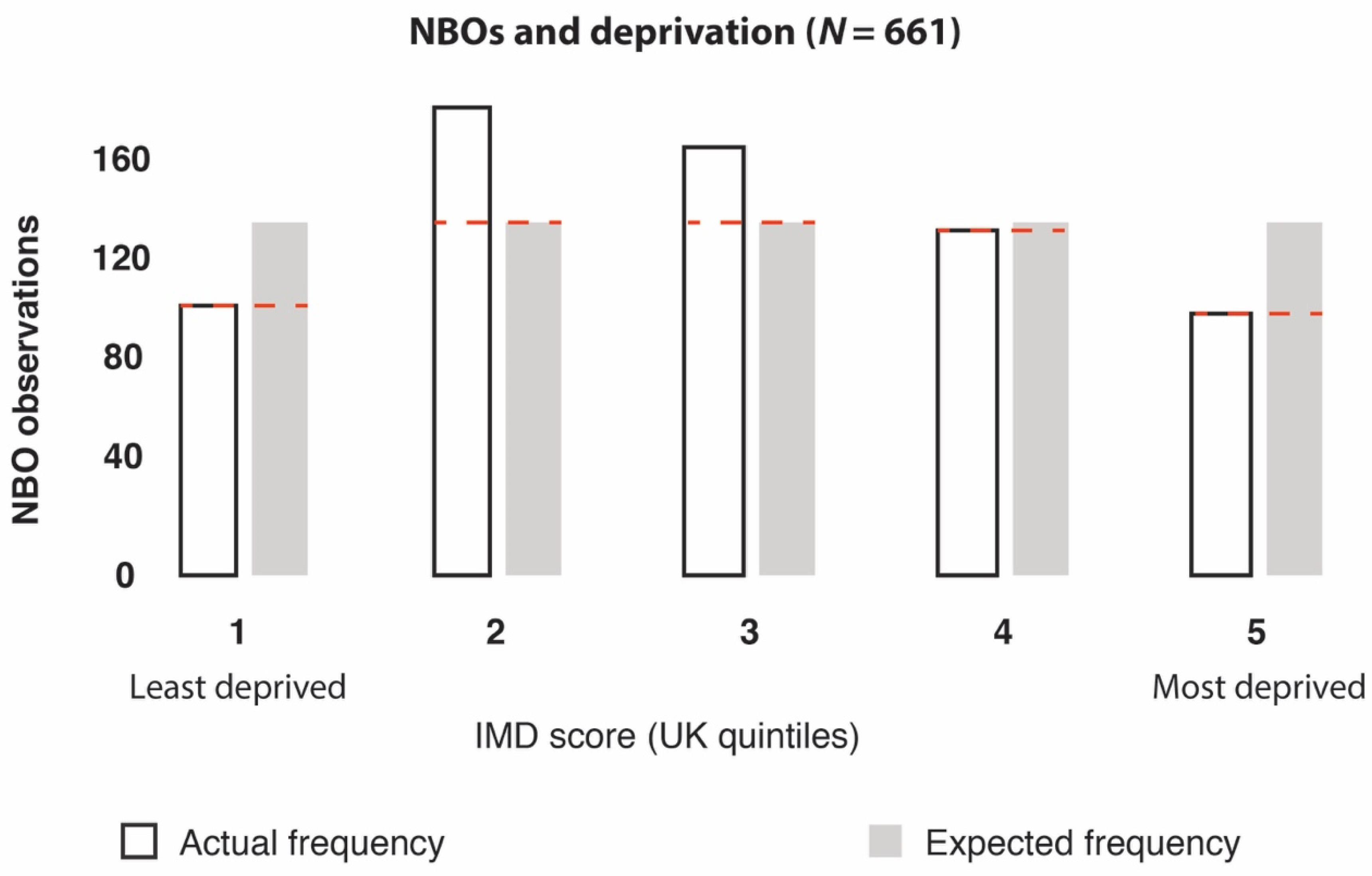
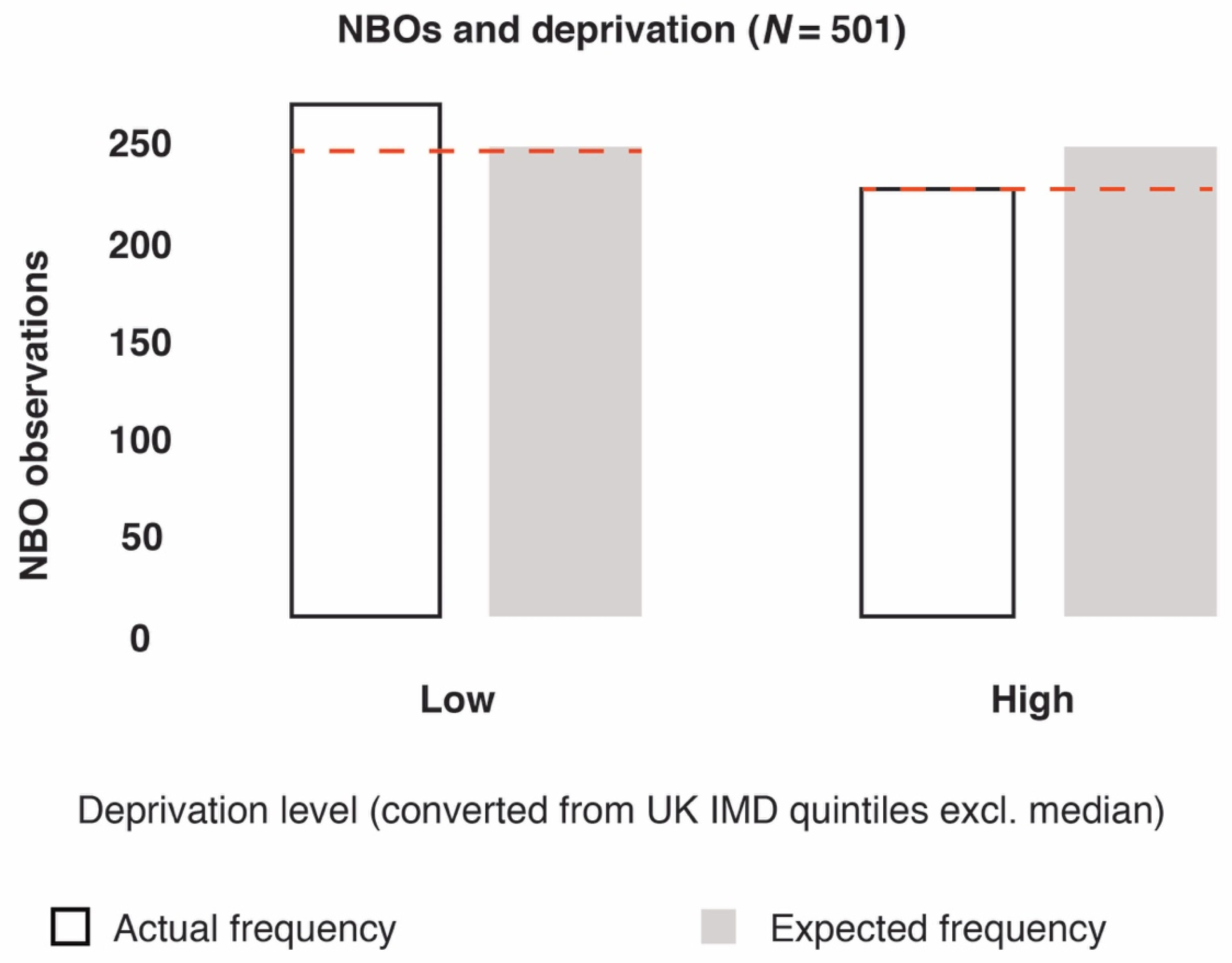
3.2.2. Deprivation Analyses
3.2.3. Geographical Presence of NBOs (Confirmed and Unconfirmed GRx Providers)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A


References
- McEwan, K.; Richardson, M.; Sheffield, D.; Ferguson, F.J.; Brindley, P. A smartphone app for improving mental health through connecting with urban nature. Int. J Environ Res Public Health. 2019, 16, 3373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarris, J.; Manincor, D.; John, M.; Hargraves, F.; Tsonis, J. Harnessing the four elements for mental health. Front. Psychiatry 2019, 10, 256. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.S.; Suzuki, S. Blood pressure-Lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef] [PubMed]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9. [Google Scholar] [CrossRef] [Green Version]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening is beneficial for health: A meta-analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef]
- Clatworthy, J.; Hinds, J.M.; Camic, P. Gardening as a mental health intervention: A review. Ment. Health Rev. J. 2013, 18, 214–225. [Google Scholar] [CrossRef]
- Pasanen, T.P.; Johnson, K.A.; Lee, K.E.; Korpela, K.M. Can nature walks with psychological tasks improve mood, self-reported restoration, and sustained attention? Results from two experimental field studies. Front. Psychol. 2018, 9, 2057. [Google Scholar] [CrossRef]
- Wyles, K.J.; White, M.P.; Hattam, C.; Pahl, S.; King, H.; Austen, M. Are some natural environments more psychologically beneficial than others? The importance of type and quality on connectedness to nature and psychological restoration. Environ. Behav. 2019, 51, 111–143. [Google Scholar] [CrossRef]
- Largo-Wight, E.; Guardino, C.; Wludyka, P.S.; Hall, K.W.; Wight, J.T.; Merten, J.W. Nature contact at school: The impact of an outdoor classroom on children’s well-being. Int. J. Environ. Health Res. 2018, 28, 653–666. [Google Scholar] [CrossRef]
- Sbihi, H.; Boutin, R.C.; Cutler, C.; Suen, M.; Finlay, B.B.; Turvey, S.E. Thinking bigger: How early-life environmental exposures shape the gut microbiome and influence the development of asthma and allergic disease. Allergy 2019, 74, 2103–2115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deckers, J.; Lambrecht, B.N.; Hammad, H. How a farming environment protects from atopy. Curr. Opin. Immunol. 2019, 60, 163–169. [Google Scholar] [CrossRef]
- Liddicoat, C.; Sydnor, H.; Cando-Dumancela, C.; Dresken, R.; Liu, J.; Gellie, N.J.; Mills, J.G.; Young, J.M.; Weyrich, L.S.; Hutchinson, M.R.; et al. Naturally-diverse airborne environmental microbial exposures modulate the gut microbiome and may provide anxiolytic benefits in mice. Sci. Total Environ. 2020, 701, 134684. [Google Scholar] [CrossRef] [PubMed]
- Bethelmy, L.C.; Corraliza, J.A. Transcendence and Sublime Experience in Nature: Awe and Inspiring Energy. Front. Psychol. 2019, 10, 509. [Google Scholar] [CrossRef] [PubMed]
- Barrable, A. The Case for Nature Connectedness as a Distinct Goal of Early Childhood Education. Int. J. Early Child. 2019, 6, 59–70. [Google Scholar]
- Jennings, V.; Bamkole, O. The Relationship between Social Cohesion and Urban Green Space: An Avenue for Health Promotion. Int. J. Environ. Res. Public Health 2019, 16, 452. [Google Scholar] [CrossRef] [Green Version]
- Fuller, R.A.; Irvine, K.N.; Devine-Wright, P.; Warren, P.H.; Gaston, K.J. Psychological benefits of greenspace increase with biodiversity. Biol. Lett. 2007, 3, 390–394. [Google Scholar] [CrossRef]
- Van Tubergen, A.; van der Linden, S. A brief history of spa therapy. Ann. Rheum. Dis. 2002, 61, 273. [Google Scholar] [CrossRef] [Green Version]
- Jackson, R. Waters and spas in the classical world. Med Hist. 1990, 34, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Vladeva, E.; Bacheva, D.; Todorov, I. SPAs and wellness–a new philosophy for harmony in life. Scr. Sci. Salut. Publicae 2016, 2, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Gianfaldoni, S.; Tchernev, G.; Wollina, U.; Roccia, M.G.; Fioranelli, M.; Gianfaldoni, R.; Lotti, T. History of the Baths and Thermal Medicine. Open Access Maced. J. Med Sci. 2017, 5, 566. [Google Scholar] [CrossRef] [Green Version]
- Wheatley, B.; Wyzga, R. Mercury as a Global Pollutant: Human Health Issues; Wheatley, B., Wyzga, R., Eds.; Kluwer: Dordrecht, The Netherlands, 1997. [Google Scholar]
- Ganesharajah, C. Indigenous Health and Wellbeing: The Importance of Country; Native Title Research Unit, 2009. Australian Institute for Aboriginal and Torres Strait Islander Studies. Available online: https://aiatsis.gov.au/sites/default/files/products/report_research_outputs/ganesharajah-2009-indigenous-health-wellbeing-importance-country.pdf (accessed on 1 January 2020).
- Shanahan, D.F.; Astell–Burt, T.; Barber, E.A.; Brymer, E.; Cox, D.T.; Dean, J.; Depledge, M.; Fuller, R.A.; Hartig, T.; Irvine, K.N.; et al. Nature–Based Interventions for Improving Health and Wellbeing: The Purpose, the People and the Outcomes. Sports 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crnic, M.; Kondo, M.C. Nature Rx: Reemergence of Pediatric Nature-Based Therapeutic Programs From the Late 19th and Early 20th Centuries. AJPH 2019. [Google Scholar] [CrossRef] [PubMed]
- Margoliers, J. Refill as needed: To help ailing patients, Park Rx America prescribes a dose of nature. Landsc. Archit. 2018, 108, 212. [Google Scholar]
- Patel, A.; Schofield, G.M.; Kolt, G.S.; Keogh, J.W. General practitioners’ views and experiences of counselling for physical activity through the New Zealand Green Prescription program. BMC Fam. Pract. 2011, 12, 119. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.A.; Walter, L.G.; Arroll, B.; Tilyard, M.W.; Russell, D.G. The green prescription study: A randomized controlled trial of written exercise advice provided by general practitioners. Am. J. Public Health 1998, 88, 288–291. [Google Scholar] [CrossRef] [Green Version]
- Bragg, R.; Leck, C. Good Practice in Social Prescribing for Mental Health: The Role of Nature-Based Interventions; Natural England Commissioned Reports: York, UK, 2017. [Google Scholar]
- Aggar, C.; Caruana, T.; Thomas, T.; Baker, J.R. Social prescribing as an intervention for people with work-related injuries and psychosocial difficulties in Australia. Adv. Health Behav. 2020, 3, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Gearey, M.; Robertson, L.; Anderson, J.; Barros, P.; Cracknell, D. Planning Cities with Nature. Re-Naturing the City for Health and Wellbeing: Green/Blue Urban Spaces as Sites of Renewal and Contestation; Springer: Cham, Switzerland, 2019; pp. 153–168. [Google Scholar]
- Van den Berg, A.E. From green space to green prescriptions: Challenges and opportunities for research and practice. Front. Psychol. 2017, 8, 268. [Google Scholar] [CrossRef] [Green Version]
- Bragg, R.; Atkins, G. A Review of Nature-Based Interventions for Mental Health Care; Natural England Commissioned Reports: York, UK, 2016. [Google Scholar]
- Elsey, H.; Murray, J.; Bragg, R. Green fingers and clear minds: Prescribing ‘care farming’ for mental illness. Br. J. Gen. Pract. 2016, 66, 99–100. [Google Scholar] [CrossRef] [Green Version]
- Husk, K.; Lovell, R.; Garside, R. Prescribing gardening and conservation activities for health and wellbeing in older people. Maturitas 2018, 110, A1–A2. [Google Scholar] [CrossRef]
- Hart, J. Prescribing nature therapy for improved mental health. Altern. Complement. Ther. 2016, 22, 161–163. [Google Scholar] [CrossRef]
- Bloomfield, D. What makes nature-based interventions for mental health successful? BJPsych Int. 2017, 14, 82–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, J.M.; Breed, M.F. Green prescriptions and their co-benefits: Integrative strategies for public and environmental health. Challenges 2019, 10, 9. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A. How to… Write and analyse a questionnaire. J. Orthod. 2003, 30, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Brace, I. Questionnaire Design: How to Plan, Structure and Write Survey Material for Effective Market Research; Kogan Page Publishers: London, UK, 2018. [Google Scholar]
- Patten, M.L. Questionnaire Research: A Practical Guide; Routledge: Abingdon, UK, 2016. [Google Scholar]
- Rowley, J. Designing and using research questionnaires. Manag. Res. Rev. 2014, 37, 308–330. [Google Scholar] [CrossRef]
- Browning, M.; Lee, K. Within what distance does “greenness” best predict physical health? A systematic review of articles with GIS buffer analyses across the lifespan. Int. J. Environ. Res. Public Health 2017, 14, 675. [Google Scholar] [CrossRef] [Green Version]
- Houston, D. Implications of the modifiable areal unit problem for assessing built environment correlates of moderate and vigorous physical activity. Appl. Geogr. 2014, 50, 40–47. [Google Scholar] [CrossRef]
- Hochadel, M.; Heinrich, J.; Gehring, U.; Morgenstern, V.; Kuhlbusch, T.; Link, E.; Wichmann, H.E.; Krämer, U. Predicting long-term average concentrations of traffic-related air pollutants using GIS-based information. Atmos. Environ. 2006, 40, 542–553. [Google Scholar] [CrossRef]
- Mears, M.; Brindley, P.; Maheswaran, R.; Jorgensen, A. Understanding the socioeconomic equity of publicly accessible greenspace distribution: The example of Sheffield, UK. Geoforum 2019, 103, 126–137. [Google Scholar] [CrossRef]
- Dennis, M.; Barlow, D.; Cavan, G.; Cook, P.A.; Gilchrist, A.; Handley, J.; James, P.; Thompson, J.; Tzoulas, K.; Wheater, C.P.; et al. Mapping urban green infrastructure: A novel landscape-based approach to incorporating land use and land cover in the mapping of human-dominated systems. Land 2018, 7, 17. [Google Scholar] [CrossRef] [Green Version]
- Abel, G.A.; Barclay, M.E.; Payne, R.A. Adjusted indices of multiple deprivation to enable comparisons within and between constituent countries of the UK including an illustration using mortality rates. BMJ Open 2016, 6, e012750. [Google Scholar] [CrossRef] [PubMed]
- Southon, G.E.; Jorgensen, A.; Dunnett, N.; Hoyle, H.; Evans, K.L. Perceived species-richness in urban green spaces: Cues, accuracy and well-being impacts. Landsc. Urban Plan. 2018, 172, 1–10. [Google Scholar] [CrossRef]
- De Keijzer, C.; Tonne, C.; Sabia, S.; Basagaña, X.; Valentín, A.; Singh-Manoux, A.; Antó, J.M.; Alonso, J.; Nieuwenhuijsen, M.J.; Sunyer, J.; et al. Green and blue spaces and physical functioning in older adults: Longitudinal analyses of the Whitehall II study. Environ. Int. 2019, 122, 346–356. [Google Scholar] [CrossRef]
- Coldwell, D.F.; Evans, K.L. Visits to urban green-space and the countryside associate with different components of mental well-being and are better predictors than perceived or actual local urbanisation intensity. Landsc. Urban Plan. 2018, 175, 114–122. [Google Scholar] [CrossRef]
- Brindley, P.; Cameron, R.W.; Ersoy, E.; Jorgensen, A.; Maheswaran, R. Is more always better? Exploring field survey and social media indicators of quality of urban greenspace, in relation to health. Urban For. Urban Green. 2019, 39, 45–54. [Google Scholar] [CrossRef]
- Mears, M.; Brindley, P.; Jorgensen, A.; Ersoy, E.; Maheswaran, R. Greenspace spatial characteristics and human health in an urban environment: An epidemiological study using landscape metrics in Sheffield, UK. Ecol. Indic. 2019, 106, 105464. [Google Scholar] [CrossRef]
- Houlden, V.; Weich, S.; Jarvis, S. A cross-sectional analysis of green space prevalence and mental wellbeing in England. BMC Public Health 2017, 17, 460. [Google Scholar] [CrossRef]
- Royal College of General Practitioners. GP Practices Supported to Recommend Active Lifestyles to Patients and Staff with Launch of New UK-Wide Active Practice Charter. 2019. Available online: https://www.rcgp.org.uk/about-us/news/2019/august/gp-practices-supported-to-recommend-active-lifestyles-to-patients-and-staff.aspx (accessed on 1 August 2019).
- Rogerson, M.; Wood, C.; Pretty, J.; Schoenmakers, P.; Bloomfield, D.; Barton, J. Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing. Int. J. Environ. Res. Public Health 2020, 17, 1526. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of walking in a forest on young women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef] [Green Version]
- Garrett, J.K.; White, M.P.; Huang, J.; Ng, S.; Hui, Z.; Leung, C.; Tse, L.A.; Fung, F.; Elliott, L.R.; Depledge, M.H.; et al. Urban blue space and health and wellbeing in Hong Kong: Results from a survey of older adults. Health Place 2019, 55, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Hunter, M.R.; Gillespie, B.W.; Chen, S.Y.P. Urban nature experiences reduce stress in the context of daily life based on salivary biomarkers. Front. Psychol. 2019, 10, 722. [Google Scholar] [CrossRef] [PubMed]
- La Puma, J. Nature Therapy: An Essential Prescription for Health. Altern. Complement. Ther. 2019, 25, 68–71. [Google Scholar] [CrossRef] [Green Version]
- Husk, K.; Elston, J.; Gradinger, F.; Callaghan, L.; Asthana, S. Social prescribing: Where is the evidence? Br. J. Gen. Pract. 2019, 69, 6–7. [Google Scholar] [CrossRef] [Green Version]
- Nelson, D.H.; Prescott, S.L.; Logan, A.C.; Bland, J.S. Clinical Ecology—Transforming 21st-Century Medicine with Planetary Health in Mind. Challenges 2019, 10, 15. [Google Scholar] [CrossRef] [Green Version]
- Cook, P.A.; Howarth, M.; Wheater, C.P. Biodiversity and Health in the Face of Climate Change: Implications for Public Health. In Biodiversity and Health in the Face of Climate Change; Springer: Cham, Switzerland, 2019; pp. 251–281. [Google Scholar]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2019, 28, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Leavell, M.A.; Leiferman, J.A.; Gascon, M.; Braddick, F.; Gonzalez, J.C.; Litt, J.S. Nature-Based Social Prescribing in Urban Settings to Improve Social Connectedness and Mental Well-being: A Review. Curr. Environ. Health Rep. 2019, 6, 297–308. [Google Scholar] [CrossRef]
- Barbosa, O.; Tratalos, J.A.; Armsworth, P.R.; Davies, R.G.; Fuller, R.A.; Johnson, P.; Gaston, K.J. Who benefits from access to green space? A case study from Sheffield, UK. Landsc. Urban Plan. 2007, 83, 187–195. [Google Scholar] [CrossRef]
- Larson, L.R.; Jennings, V.; Cloutier, S.A. Public parks and wellbeing in urban areas of the United States. PLoS ONE 2016, 11, e0153211. [Google Scholar] [CrossRef]
- Wood, L.; Hooper, P.; Foster, S.; Bull, F. Public green spaces and positive mental health–investigating the relationship between access, quantity and types of parks and mental wellbeing. Health Place 2017, 48, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Flies, E.J.; Skelly, C.; Negi, S.S.; Prabhakaran, P.; Liu, Q.; Liu, K.; Goldizen, F.C.; Lease, C.; Weinstein, P. Biodiverse green spaces: A prescription for global urban health. Front. Ecol. Environ. 2017, 15, 510–516. [Google Scholar] [CrossRef]
- Barton, J.; Griffin, M.; Pretty, J. Exercise-, nature-and socially interactive-based initiatives improve mood and self-esteem in the clinical population. Perspect. Public Health 2012, 132, 89–96. [Google Scholar] [CrossRef]
- Buckley, R.C.; Westaway, D.; Brough, P. Social Mechanisms to get People Outdoors: Bimodal Distribution of interest in nature? Front. Public Health 2016, 4, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peacock, J.; Hine, R.; Pretty, J. The Mental Health Benefits of Green Exercise Activities and Green Care; MIND: Colchester, UK, 2007; pp. 1–18. [Google Scholar]
- Razani, N.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Flores, H.H.; Rutherford, G.W. Design and evaluation of a park prescription program for stress reduction and health promotion in low-income families: The Stay Healthy in Nature Everyday (SHINE) study protocol. Contemp. Clin. Trials 2016, 51, 8–14. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Van Dillen, S.M.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Akpinar, A. How is quality of urban green spaces associated with physical activity and health? Urban For. Urban Green. 2016, 16, 76–83. [Google Scholar] [CrossRef]
- Zhang, Y.; Van den Berg, A.; Van Dijk, T.; Weitkamp, G. Quality over quantity: Contribution of urban green space to neighborhood satisfaction. Int. J. Environ. Res. Public Health 2017, 14, 535. [Google Scholar] [CrossRef]
- Clifford, D. Voluntary sector organisations working at the neighbourhood level in England: Patterns by local area deprivation. Environ. Plan. A 2012, 44, 1148–1164. [Google Scholar] [CrossRef] [Green Version]
- Mohan, J.; Bennett, M.R. Community-level impacts of the third sector: Does the local distribution of voluntary organizations influence the likelihood of volunteering? Environ. Plan. A Econ. Space 2019, 51, 950–979. [Google Scholar] [CrossRef] [Green Version]
- Braubach, M.; Egorov, A.; Mudu, P.; Wolf, T.; Thompson, C.W.; Martuzzi, M. Effects of urban green space on environmental health, equity and resilience. In Nature-Based Solutions to Climate Change Adaptation in Urban Areas; Springer: Cham, Switzerland, 2017; pp. 187–205. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Greenspace | Number in 100 m of GRx = “Yes” (n = 29) | Number in 100 m of GRx = “No” (n = 85) |
|---|---|---|
| Playing field | 5 | 6 |
| Other sports facility | 5 | 3 |
| Play space | 3 | 6 |
| Cemetery | 1 | 1 |
| Allotment or community garden | 3 | 5 |
| Religious grounds | 7 | 8 |
| Public park or garden | 6 | 10 |
| Bowling green | 1 | 1 |
| Tennis court | 1 | 1 |
| Golf course | 0 | 1 |
| Public park * | 2 | 0 |
| Sports field * | 1 | 1 |
| Grassland/scrub * | 1 | 0 |
| Radius | Total Greenspaces | Mean | Median | Standard Deviation |
|---|---|---|---|---|
| 100 m GRx Yes | 34 | 1.17 | 1 | 1.12 |
| 100 m GRx No | 85 | 0.51 | 0 | 0.81 |
| 250 m GRx Yes | 85 | 3.69 | 4 | 1.66 |
| 250 m GRx No | 188 | 2.72 | 3 | 1.49 |
| 500 m GRx Yes | 239 | 8.24 | 8 | 3.80 |
| 500 m GRx No | 554 | 6.50 | 6 | 3.50 |
| 1000 m GRx Yes | 602 | 20.70 | 21 | 11 |
| 1000 m GRx No | 1669 | 19.60 | 19 | 9 |
| 5000 m GRx Yes | 8120 | 280.00 | 297 | 210 |
| 5000 m GRx No | 19,936 | 234.00 | 190 | 209 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, J.M.; Jorgensen, A.; Cameron, R.; Brindley, P. Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK. Int. J. Environ. Res. Public Health 2020, 17, 3460. https://doi.org/10.3390/ijerph17103460
Robinson JM, Jorgensen A, Cameron R, Brindley P. Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK. International Journal of Environmental Research and Public Health. 2020; 17(10):3460. https://doi.org/10.3390/ijerph17103460
Chicago/Turabian StyleRobinson, Jake M., Anna Jorgensen, Ross Cameron, and Paul Brindley. 2020. "Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK" International Journal of Environmental Research and Public Health 17, no. 10: 3460. https://doi.org/10.3390/ijerph17103460
APA StyleRobinson, J. M., Jorgensen, A., Cameron, R., & Brindley, P. (2020). Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK. International Journal of Environmental Research and Public Health, 17(10), 3460. https://doi.org/10.3390/ijerph17103460