Statistical Modelling of the Effects of Weather Factors on Malaria Occurrence in Abuja, Nigeria

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Management
2.3. Statistical Analysis
2.4. Ethical Clearance
3. Results
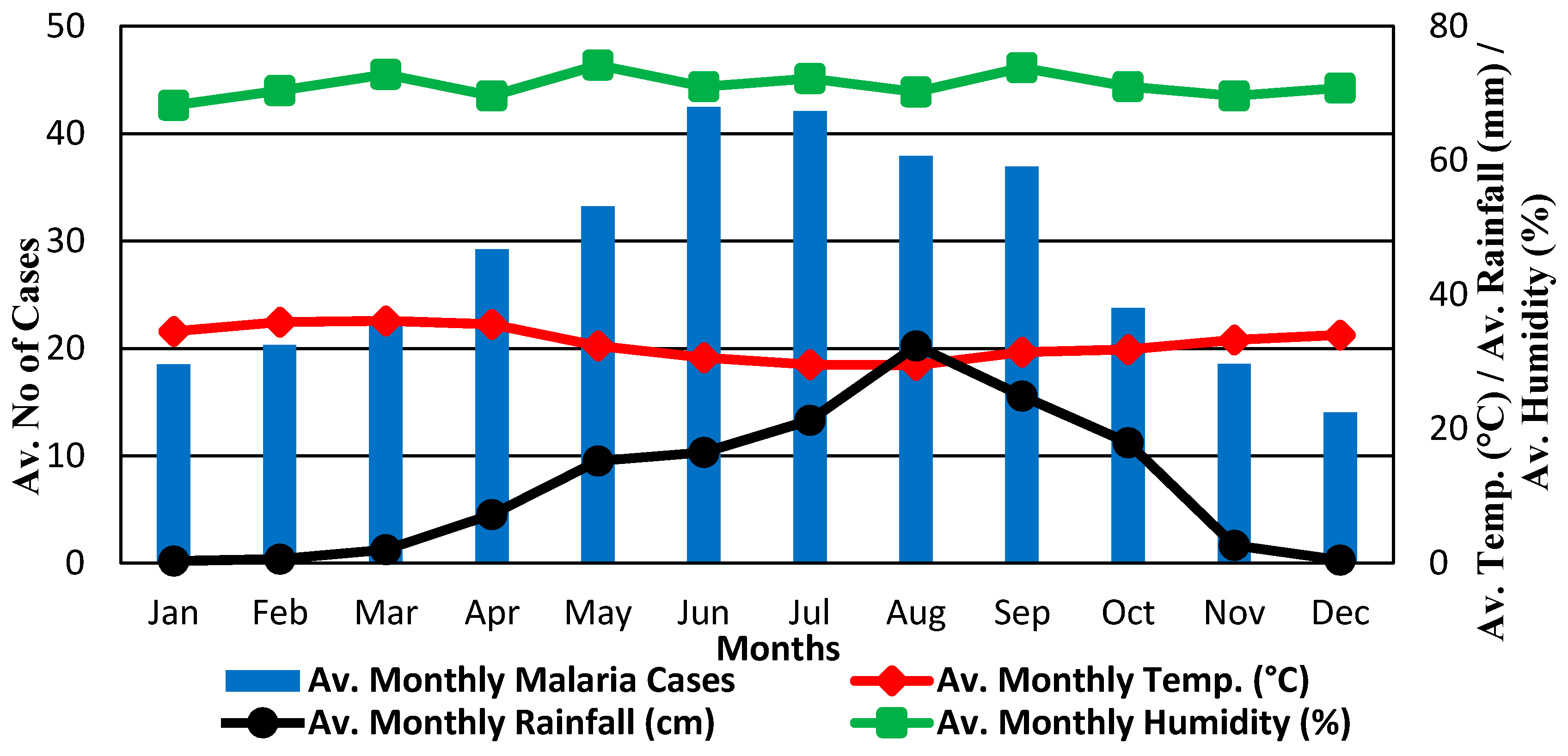
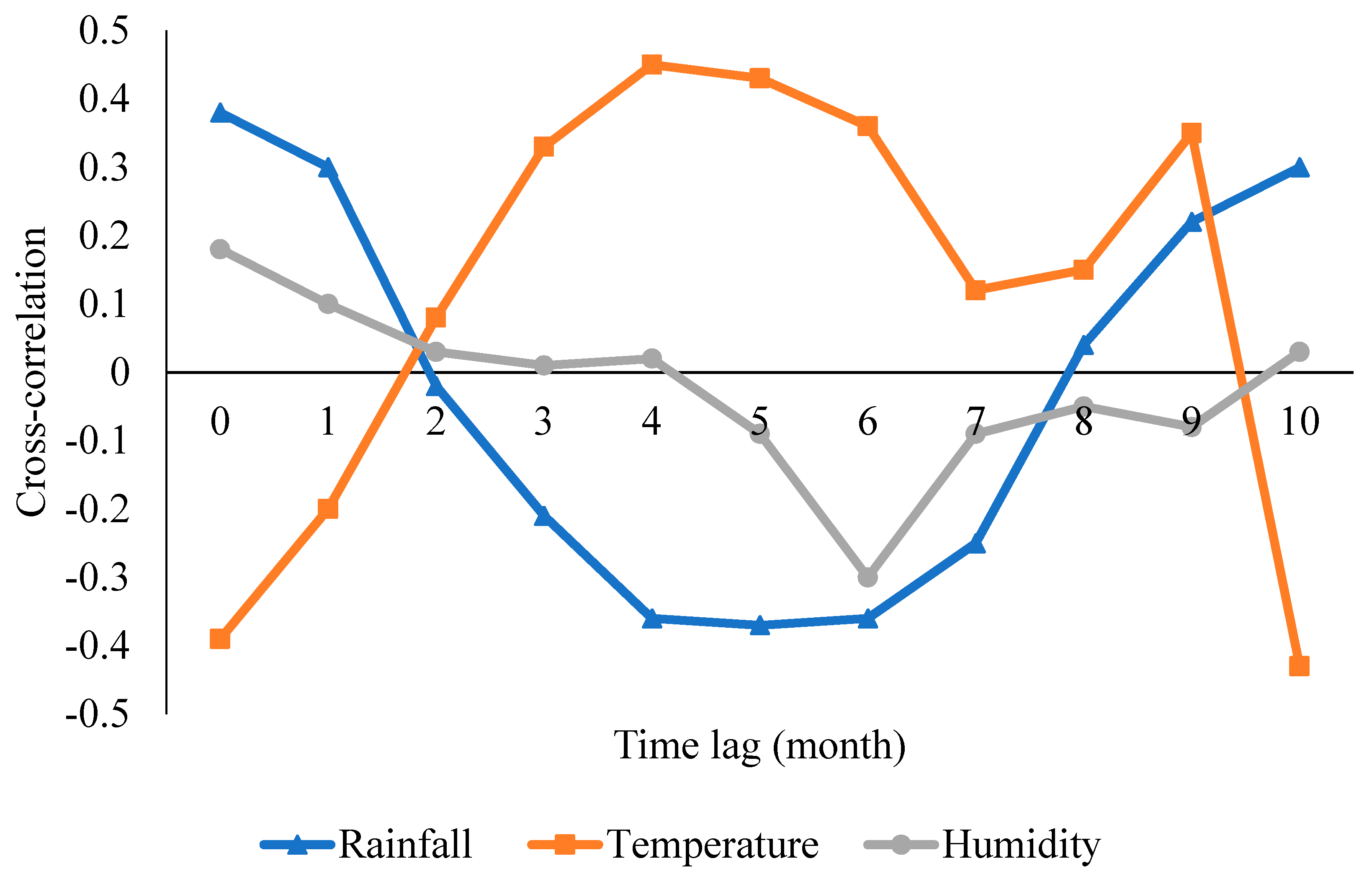
3.1. Descriptive Statistics
3.2. Model Outcomes and Information
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohammadkhani, M.; Khanjani, N.; Bakhtiari, B.; Sheikhzadeh, K. The relation between climatic factors and malaria incidence in Kerman, South East of Iran. Parasite Epidemiol. Control 2016, 1, 205–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LSMOH. Medium-Term Sector Strategy (MTSS) 2013–2015. Health Sector Zero Draft Report. Lagos. 2012. Available online: www.lagosstateministryofhealth.com-file (accessed on 8 March 2018).
- WHO. World Malaria Report. 2018. Available online: https//apps.who.int/iris/bitstream/handle/10665/175867/9789241565653-eng.pdf (accessed on 20 February 2020).
- Nyarko, S.H.; Cobblah, A. Sociodemographic determinants of Malaria among under-five children in Ghana. Malar. Res. Treat. 2014, 2014, 304361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, E.E.; Caminade, C.; Thomas, B.N. Climate change contribution to the emergence or re-emergence of parasitic diseases. Infect. Dis. Res. Treat. 2017, 10, 1178633617732296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinbobola, A.; Omotosho, J.B. Predicting malaria occurrence in Southwest and North-central Nigeria using meteorological parameters. Int. J. Biometeorol. 2013, 57, 721–728. [Google Scholar] [CrossRef]
- Alout, H.; Roche, B.; Dabire, R.K.; Cohuet, A. Consequences of insecticide resistance on malaria transmission. PLoS Pathog. 2017, 13, 3–7. [Google Scholar] [CrossRef]
- Artzy-Randrup, Y.; Alonso, D.; Pascual, M. Transmission intensity and drug resistance in malaria population dynamics: Implications for climate change. PLoS ONE 2010, 5, e13588. [Google Scholar] [CrossRef] [Green Version]
- Eunice, A.; Wanjoya, A.; Luboobi, L. Statistical modeling of malaria incidences in Apac District, Uganda. Open J. Stat. 2017, 7, 901–919. [Google Scholar] [CrossRef] [Green Version]
- Ebenezer, A.; Noutcha, A.E.M.; Okiwelu, S.N. Relationship of annual entomological inoculation rates to malaria transmission indices, Bayelsa State, Nigeria. J. Vector-Borne Dis. 2016, 53, 46–53. [Google Scholar]
- Omonijo, A.G.; Matzarakis, A.; Oguntoke, O.; Adeofun, C.O. Influence of weather and climate on malaria occurrence based on human-biometeorological methods in Ondo State, Nigeria. J. Environ. Sci. Eng. 2011, 5, 1215–1228. [Google Scholar]
- Ojua, T.A.; Ishor, D.G.; Ndom, P.J. African cultural practices and health implications for Nigeria rural development. Int. Rev. Manag. Bus. Res. 2013, 2, 176–183. [Google Scholar]
- Ewona, I.O.; Osang, J.E.; Udo, S. Trend Analyses of Rainfall Patterns in Nigeria Using Regression Parameters. Int. J. Technol. Enhanc. Emerg. Eng. Res. 2014, 2, 129–133. [Google Scholar]
- Lotfy, W.M. Climate change and epidemiology of human parasitosis in Egypt: A review. J. Adv. Res. 2014, 5, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pemola, D.N.; Jauhari, R.K. Climatic variables and malaria incidence in Dehradun, Uttaranchal, India. J. Vector-Borne Dis. 2006, 43, 21–28. [Google Scholar]
- Okonkwo, I.O.; Soleye, F.A.; Amusan, T.A.; Ogun, A.A.; Udeze, A.O.; Nkang, A.O.; Ejembi, J.; Faleye, T.O.O. Prevalence of malaria plasmodium in Abeokuta, Nigeria. Malays. J. Microbiol. 2009, 5, 113–118. [Google Scholar]
- WHO. Climate Change and Human Health, Global Environmental Change. 2016. Available online: www.who.int./globalchange/climate/summary/en/index5.html (accessed on 17 May 2017).
- Devi, N.P.; Jauhari, R.K. Meteorological variables and malaria cases based on 12 years data analysis in Dehradun (Uttarakhand) India. Eur. J. Exp. Biol. 2013, 3, 28–37. [Google Scholar]
- Dasgupta, S. Burden of climate change on malaria mortality. Int. J. Hyg. Environ. Health 2018, 221, 782–791. [Google Scholar] [CrossRef] [Green Version]
- Siraj, A.S.; Santos-Vega, M.; Bouma, M.J.; Yadeta, D.; Ruiz-Carrascal, D.; Pascual, M. Altitudinal changes in malaria. Science 2014, 1154, 1154–1159. [Google Scholar] [CrossRef]
- Babajide, S.; Perry, B.; Huffer, F.W.; Onubogu, O.; Dutton, M.; Becker, A.; Saleh, R. Effect of meteorological variables on malaria incidence in Ogun State, Nigeria. Int. J. Public Health Epidemiol. 2015, 4, 205–215. [Google Scholar]
- Beck-Johnson, L.M.; Nelson, W.A.; Paaijmans, K.P.; Read, A.F.; Thomas, M.B.; Bjørnstad, O.N. The effect of temperature on Anopheles mosquito population dynamics and the potential for malaria transmission. PLoS ONE 2018, 8, e79276. [Google Scholar] [CrossRef]
- Mishra, G. Hospital-based study of malaria in Ratnagiri district, Maharashtra. J. Vector-Borne Dis. 2003, 40, 109–111. [Google Scholar]
- Goswami, P.; Murty, U.S.; Mutheneni, S.R.; Krishnan, S.T. Relative roles of weather variables and change in human population in malaria: Comparison over different states of India. PLoS ONE 2014, 9, e99867. [Google Scholar] [CrossRef] [PubMed]
- Evans, O.P.; Adenomon, M.O. Modeling the prevalence of malaria in Niger State: An application of Poisson regression and negative binomial regression models. Int. J. Phys. Sci. 2014, 2, 61–68. [Google Scholar]
- Gunda, R.; Chimbari, M.J.; Shamu, S.; Sartorius, B.; Mukaratirwa, S. Malaria incidence trends and their association with climatic variables in rural Gwanda, Zimbabwe, 2005–2015. Malar. J. 2017, 16, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouma, M.J.; Siraj, A.S.; Rodo, X.; Pascual, M. El Niño-based malaria epidemic warning for Oromia, Ethiopia, from August 2016 to July 2017. Trop. Med. Int. Health 2016, 21, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Nmadu, P.M.; Peter, E.; Alexander, P.; Koggie, A.Z.; Maikenti, J.I. The Prevalence of Malaria in Children between the Ages 2–15 Visiting Gwarinpa General Hospital Life-Camp, Abuja, Nigeria. J. Health Sci. 2015, 5, 47–51. [Google Scholar]
- Olaniran, O.J. Rainfall anomaly patterns in dry and wet years over Nigeria. Int. J. Climatol. 1991, 11, 177–204. [Google Scholar] [CrossRef]
- Nanvyat, N.; Mulambalah, C.; Barshep, Y.; Ajiji, D.; Dakul, D.; Tsingalia, H. Malaria transmission trends and its lagged association with climate factors in the highlands of Plateau State, Nigeria. Trop. Parasitol. 2018, 8, 18–23. [Google Scholar] [CrossRef]
- Digi-geske, I.; Olasehinde, I.; Fidinad, I.; Arogundade, D.; Darby, P. Epidemiological data of falciparum malaria in Ado/Ota, Southwest Ogun State, Nigeria. Data Brief 2018, 19, 1398–1402. [Google Scholar] [CrossRef]
- Okorie, P.N.; McKenzie, F.E.; Ademowo, O.G.; Bockarie, M.; Kelly-Hope, L. Nigeria Anopheles vector database: An overview of 100 years’ research. PLoS ONE 2011, 6, 6–7. [Google Scholar] [CrossRef] [Green Version]
- Badaru, Y.U.; Adejoke, A.O.; Abubakar, A.S.; Emigilati, M.A. Rainfall Variations as the Determinant of Malaria in the Federal Capital Territory Abuja, Nigeria. J. Environ. Earth Sci. 2014, 4, 149–159. [Google Scholar]
- NPC. National Population Commission’s Population Figures for the Nigeria States for 2006 Population and Housing Census; NPC: Abuja, Nigeria, 2006. [Google Scholar]
- FMoH. Federal Ministry of Health, National Malaria Control Programme, Abuja, Nigeria. Strategic Plan 2009–2013. Nigeria Strategic Plan 2009–2013: A Road Map for Malaria Control in Nigeria. Abuja, Nigeria. 2008. Available online: http://www.nationalplanningcycles.org/sites/default/files/country_docs/Nigeria/nigeria_draft_malaria_strategic_plan_2009-2013.pdf (accessed on 11 October 2017).
- Balogun, O. The Federal Capital Territory of Nigeria: A Geography of its Development; University of Ibadan Press: Ibadan, Nigeria, 2001. [Google Scholar]
- Sam Wobo, S.O.; Adekunle, N.O.; Adeleke, N.A.; Dedeke, G.A.; Oke, O.A.; Abimbola, W.A.; Surakat, O.A. Epidemiological factors in the prevalence of malaria parasites in Primary Health facilities Attendees, Ogun State, Nigeria. Malar. Chemother. Control Elimin. 2014, 3, 1–6. [Google Scholar]
- Gupta, R.C.; Ong, S.H. Analysis of long-tailed count data by Poisson mixtures. Commun. Stat. Theory Methods 2005, 34, 557–573. [Google Scholar] [CrossRef]
- Yusuf, O.B.; Ugalahi, L.O. On the performance of the Poisson, negative Binomial and generalized Poisson regression models in the prediction of antenatal care visits in Nigeria. Am. J. Math. Stat. 2015, 5, 128–136. [Google Scholar]
- Razavi, S.; Vogel, R. Prewhitening of hydroclimatic time series? Implications for inferred change and variability across time scales. J. Hydrol. 2018, 557, 109–115. [Google Scholar] [CrossRef]
- Sena, L.; Deressa, W.; Ali, A. Correlation of climate variability and malaria: A retrospective comparative study, Southwest Ethiopia. Ethiop. J. Health Sci. 2015, 25, 129–138. [Google Scholar] [CrossRef]
- Bouma, M.J.; Dye, C.; Van der kaay, H.J. Falciparum malaria and climate change in the northwest frontier province of Pakistan. Am. J. Trop. Med. Hyg. 1996, 55, 131–137. [Google Scholar] [CrossRef]
- Akpan, G.E.; Adepoju, K.A.; Oladosu, O.R.; Adelabu, S.A. Dominant malaria vector species in Nigeria: Modelling potential distribution of Anopheles gambiae sensu lato and its siblings with MaxEnt. PLoS ONE 2018, 13, e0204233. [Google Scholar] [CrossRef]
- Britton, E.; Hales, S.; Venugopal, K.; Baker, M.G. The impact of climate variability and change on cryptosporidiosis and giardiasis rates in New Zealand. J. Water Health 2010, 8, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Oluleye, A.; Akinbobola, A. Malaria and pneumonia occurrence in Lagos, Nigeria: Role of temperature and rainfall. Afr. J. Environ. Sci. Technol. 2010, 4, 506–516. [Google Scholar]
- Onyabe, D.Y.; Conn, J.E. The distribution of two major malaria vectors, Anopheles gambiae and Anopheles arabiensis, in Nigeria. Mem. Inst. Oswaldo Cruz 2001, 96, 1081–1084. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Model Predictor | Std Error | Wald Chi-Square | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|
| Intercept | 4.603 | 0.321 | 206.117 | 99.821 | 53.247,187.13 | <0.001 |
| Rainfall | 0.001 | 0.000 | 25.945 | 1.001 | 1.000,1.001 | <0.001 |
| Temperature | −0.060 | 0.007 | 63.243 | 0.942 | 0.928,0.956 | <0.001 |
| Humidity | 0.010 | 0.003 | 14.078 | 1.010 | 1.005,1.015 | <0.001 |
| Lag 1 | Lag 4 | Lag 5 | ||||
|---|---|---|---|---|---|---|
| Variables | IRR (0.95CI) | p-Value | IRR (0.95CI) | p-Value | IRR (0.95CI) | p-Value |
| Rainfall | 1.001 (1.001–1.001) | <0.001 * | 0.999 (0.999–1.000) | <0.001 * | 0.999 (0.999–0.999) | <0.001 * |
| Temperature | 0.988 (1.974–1.002) | 0.105 | 1.079 (1.064–1.095) | <0.001 * | 1.065 (1.050–1.080) | <0.001 * |
| Humidity | 1.005 (1.000–1.005) | 0.068 | 1.006 (1.001–1.011) | 0.016 * | 0.998 (0.993–1.004) | 0.556 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segun, O.E.; Shohaimi, S.; Nallapan, M.; Lamidi-Sarumoh, A.A.; Salari, N. Statistical Modelling of the Effects of Weather Factors on Malaria Occurrence in Abuja, Nigeria. Int. J. Environ. Res. Public Health 2020, 17, 3474. https://doi.org/10.3390/ijerph17103474
Segun OE, Shohaimi S, Nallapan M, Lamidi-Sarumoh AA, Salari N. Statistical Modelling of the Effects of Weather Factors on Malaria Occurrence in Abuja, Nigeria. International Journal of Environmental Research and Public Health. 2020; 17(10):3474. https://doi.org/10.3390/ijerph17103474
Chicago/Turabian StyleSegun, Oguntade Emmanuel, Shamarina Shohaimi, Meenakshii Nallapan, Alaba Ajibola Lamidi-Sarumoh, and Nader Salari. 2020. "Statistical Modelling of the Effects of Weather Factors on Malaria Occurrence in Abuja, Nigeria" International Journal of Environmental Research and Public Health 17, no. 10: 3474. https://doi.org/10.3390/ijerph17103474
APA StyleSegun, O. E., Shohaimi, S., Nallapan, M., Lamidi-Sarumoh, A. A., & Salari, N. (2020). Statistical Modelling of the Effects of Weather Factors on Malaria Occurrence in Abuja, Nigeria. International Journal of Environmental Research and Public Health, 17(10), 3474. https://doi.org/10.3390/ijerph17103474