Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review



Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Literature Screening
2.4. Data Collection
2.5. Quality Assessment
2.6. Statistical Analysis and Data Synthesis
3. Results
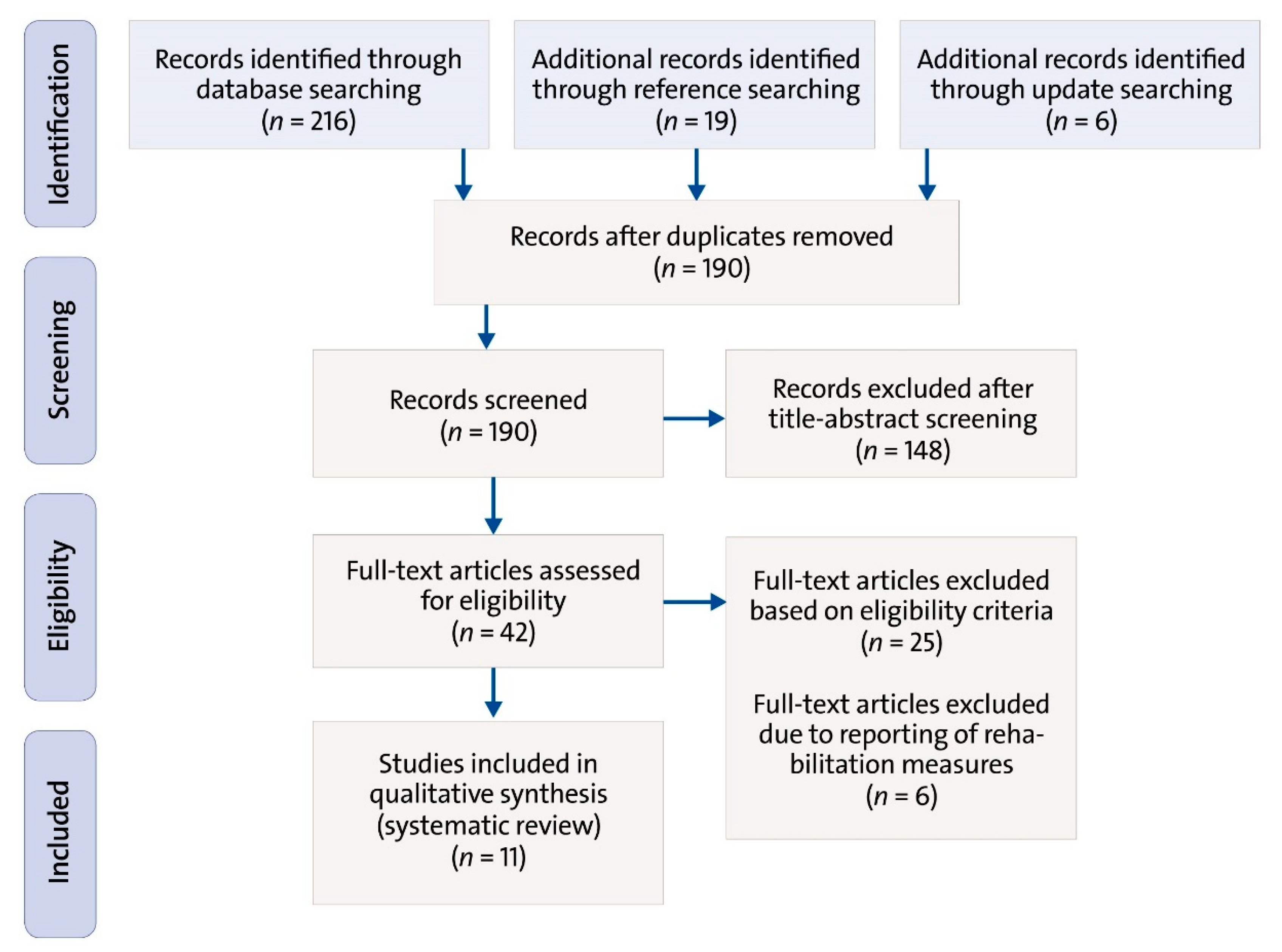
3.1. Study Selection
3.2. Study Characteristics
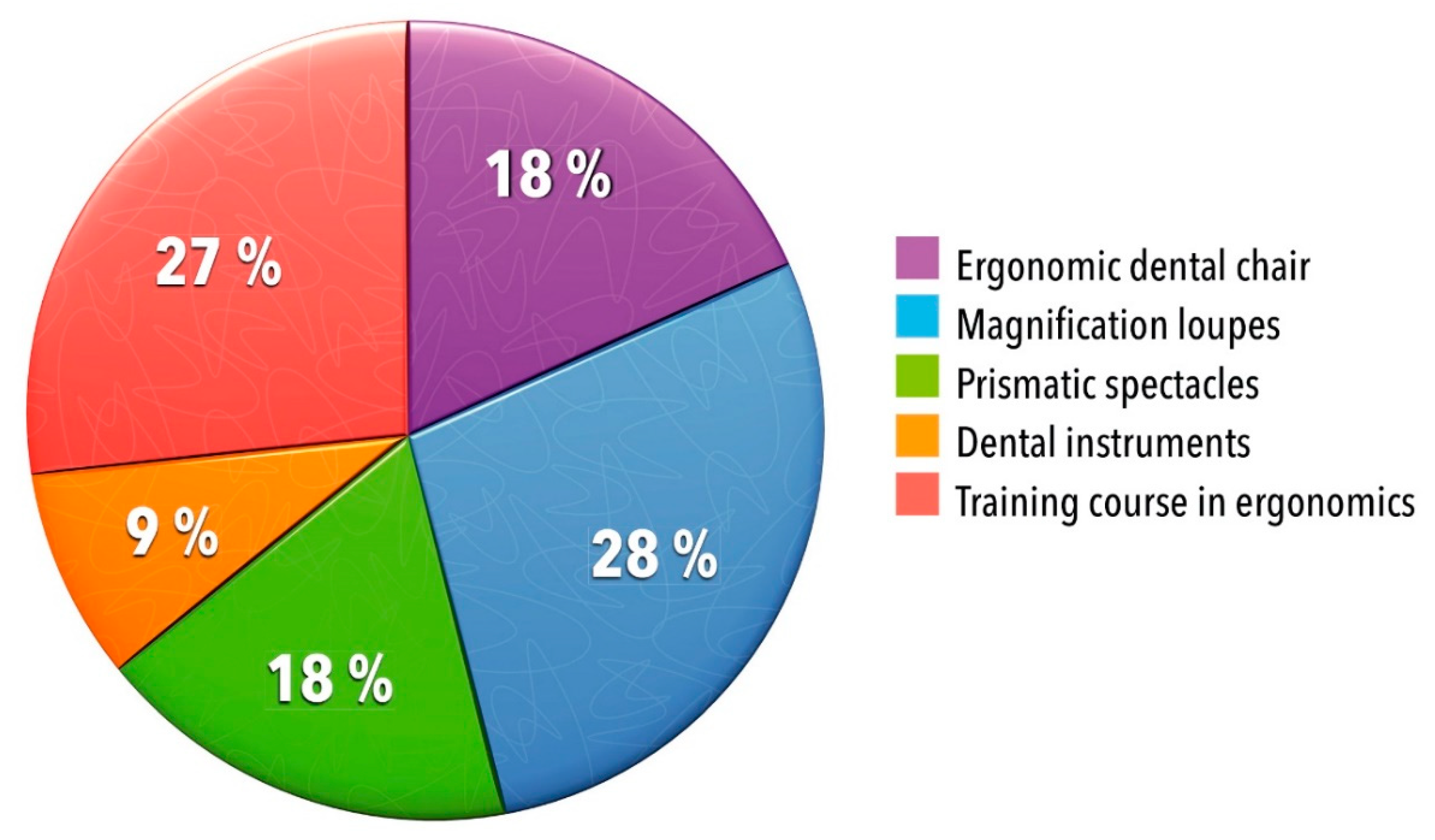
3.3. Ergonomic Interventions
3.3.1. Ergonomic Dental Chair
3.3.2. Magnification Loupes
3.3.3. Prismatic Spectacles
3.3.4. Dental Instruments
3.3.5. Training Course in Ergonomics
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Lietz, J.; Kozak, A.; Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS ONE 2018, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljanakh, M.; Shaikh, S.; Siddiqui, A.A.; Al-Mansour, M.; Hassan, S.S. Prevalence of musculoskeletal disorders among dentists in the Hail Region of Saudi Arabia. Ann. Saudi Med. 2015, 35, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Aminian, O.; Banafsheh Alemohammad, Z.; Sadeghniiat-Haghighi, K. Musculoskeletal disorders in female dentists and pharmacists: A cross-sectional study. Acta Med. Iran 2012, 50, 635–640. [Google Scholar] [PubMed]
- Nermin, Y. Musculoskeletal disorders (Msds) and dental practice. Part 1. General information-terminology, aetiology, work-relatedness, magnitude of the problem, and prevention. Int. Dent. J. 2006, 56, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Aminian, O.; Alemohammad, Z.B.; Hosseini, M.H. Neck and upper extremity symptoms among male dentists and pharmacists. Work 2015, 51, 863–868. [Google Scholar] [CrossRef]
- Blanc, D.; Farre, P.; Hamel, O. Variability of musculoskeletal strain on dentists: An electromyographic and goniometric study. Int. J. Occup. Saf. Ergon. 2014, 20, 295–307. [Google Scholar] [CrossRef]
- Ayers, K.M.S.; Thomson, W.M.; Newton, J.T.; Morgaine, K.C.; Rich, A.M. Self-reported occupational health of general dental practitioners. Occup. Med. 2009, 59, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Plessas, A.; Bernardes Delgado, M. The role of ergonomic saddle seats and magnification loupes in the prevention of musculoskeletal disorders: A systematic review. Int. J. Dent. Hyg. 2018, 4, 430–440. [Google Scholar] [CrossRef]
- Mulimani, P.; Hoe, V.C.; Hayes, M.J.; Idiculla, J.J.; Abas, A.B.; Karanth, L. Ergonomic interventions for preventing musculoskeletal disorders in dental care practitioners. Cochrane Database Syst. Rev. 2018, 10. [Google Scholar] [CrossRef]
- Roll, S.C.; Tung, K.D.; Chang, H.; Sehremelis, T.A.; Fukumura, Y.E.; Randolph, S.; Forrest, J.L. Prevention and rehabilitation of musculoskeletal disorders in oral health care professionals: A systematic review. J. Am. Dent. Assoc. 2019, 6, 489–502. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordhausen, T.; Hirt, J. Manual zur Literaturrecherche in Fachdatenbanken. Ref Hunter, Version 3.0; Martin-Luther-Universität Halle-Wittenberg: Deutschland, Germany; Fachhochschule: St. Gallen, Switzerland, 2019; pp. 16–17. [Google Scholar]
- Koni, A.; Kufersin, M.; Ronchese, F.; Travan, M.; Cadenaro, M.; Larese Filon, F. Approach to prevention of musculoskeletal symptoms in dental students: An interventional study. Med. Lav. 2018, 109, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Dehghan, N.; Aghilinejad, M.; Nassiri-Kashani, M.H.; Amiri, Z.; Talebi, A. The effect of a multifaceted ergonomic intervention program on reducing musculoskeletal disorders in dentists. Med. J. Islam. Repub. Iran 2016, 30, 472. [Google Scholar]
- Dable, R.A.; Wasnik, P.B.; Yeshwante, B.J.; Musani, S.I.; Patil, A.K.; Nagmode, S.N. Postural assessment of students evaluating the need of ergonomic seat and magnification in dentistry. J. Indian Prosthodont. Soc. 2014, 14, 51–58. [Google Scholar] [CrossRef]
- Farrokhnia, T.; Rezai, M.; Vaziri, M.-H.; Vaziri, F. Investigating the Effect of Educational Intervention on Musculoskeletal Disorders in Dentists. World Fam. Med. 2018, 16, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Hallaj, S.; Razi, S.S.M. Design and Evaluation of an Arm Support for Prevention of MSDs in Dentists. In Advances in Ergonomics in Design; Rebelo, F., Soares, M., Eds.; Springer: Cham, Switzerland, 2016; pp. 265–275. ISBN 978-3-319-41983-1. [Google Scholar]
- Hayes, M.J.; Osmotherly, P.G.; Taylor, J.A.; Smith, D.R.; Ho, A. The effect of wearing loupes on upper extremity musculoskeletal disorders among dental hygienists. Int. J. Dent. Hyg. 2014, 12, 174–179. [Google Scholar] [CrossRef]
- Hayes, M.J.; Osmotherly, P.G.; Taylor, J.A.; Smith, D.R.; Ho, A. The effect of loupes on neck pain and disability among dental hygienists. Work 2016, 53, 755–762. [Google Scholar] [CrossRef] [Green Version]
- Lindegard, A.; Gustafsson, M.; Hansson, G.-A. Effects of prismatic glasses including optometric correction on head and neck kinematics, perceived exertion and comfort during dental work in the oral cavity–A randomised controlled intervention. Appl. Ergon. 2012, 43, 246–253. [Google Scholar] [CrossRef]
- Lindegard, A.; Nordander, C.; Jacobsson, H.; Arvidsson, I. Opting to wear prismatic spectacles was associated with reduced neck pain in dental personnel: A longitudinal cohort study. BMC Musculoskelet. Disord. 2016, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maillet, J.P.; Millar, A.M.; Burke, J.M.; Maillet, M.A.; Maillet, W.A.; Neish, N.R. Effect of magnification loupes on dental hygiene student posture. J. Dent. Educ. 2008, 72, 33–44. [Google Scholar] [PubMed]
- Rempel, D.; Lee, D.L.; Dawson, K.; Loomer, P. The effects of periodontal curette handle weight and diameter on arm pain: A four-month randomized controlled trial. J. Am. Dent. Assoc. 2012, 143, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Labbafinejad, Y.; Ghasemi, M.S.; Bagherzadeh, A.; Aazami, H.; Eslami-Farsani, M.; Dehghan, N. Saddle seat reduces musculoskeletal discomfort in microsurgery surgeons. Int. J. Occup. Saf. Ergon. 2019, 25, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Aghilinejad, M.; Azar, N.S.; Ghasemi, M.S.; Dehghan, N.; Mokamelkhah, E.K. An ergonomic intervention to reduce musculoskeletal discomfort among semiconductor assembly workers. Work 2016, 54, 445–450. [Google Scholar] [CrossRef]
- Ludwig, E.A.; McCombs, G.B.; Tolle, S.L.; Russell, D.M. The Effect of Magnification loupes on dental hygienists’ posture while exploring. J. Am. Dent. Hyg. Assoc. 2017, 91, 46–52. [Google Scholar]
- Kuang, H.; Chen, G.; Wen, Q.; Li, S.; Chen, L.; Liang, F. Improving surgeons’ comfort with prismatic glasses during cleft palate surgery: Preliminary findings. J. Oral Maxillofac. Surg. 2017, 75. [Google Scholar] [CrossRef]
- Harari, D.; Casarotto, R.A. Effectiveness of a multifaceted intervention to manage musculoskeletal disorders in workers of a medium-sized company. Int. J. Occup. Saf. Ergon. 2019, 1–11. [Google Scholar] [CrossRef]
- Sanaeinasab, H.; Saffari, M.; Valipour, F.; Alipour, H.R.; Sepandi, M.; Al Zaben, F.; Koenig, H.G. The effectiveness of a model-based health education intervention to improve ergonomic posture in office computer workers: A randomized controlled trial. Int. Arch. Occup. Environ. Health 2018, 91, 951–962. [Google Scholar] [CrossRef]
- Ancuta, C.; Iordache, C.; Fatu, A.M.; Aluculesei, C.; Forna, N. Ergonomics and prevention of musculoskeletal—Work related pathology in dentistry: A pilot study. Rom. J. Oral Rehab. 2016, 8, 73–79. [Google Scholar]
- Chismark, A.M.; Hung, A.W. Complementary health approaches to reduce musculoskeletal pain. J. Calif. Dent. Hyg. Assoc. 2015, 33, 19–38. [Google Scholar]
- Gupta, D.; Bhaskar, D.J.; Gupta, R.K.; Jain, A.; Yadav, P.; Dalai, D.R.; Singh, R.; Singh, N.; Chaudhary, V.; Singh, A.; et al. Is complementary and alternative medicine effective in job satisfaction among dentists with musculoskeletal disorders? A cross sectional study. Med. Pr. 2014, 65, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Monson, A.L.; Chismark, A.M.; Cooper, B.R.; Krenik-Matejcek, T.M. Effects of yoga on musculoskeletal pain. J. Dent. Hyg. 2017, 91, 15–21. [Google Scholar] [PubMed]
- Peros, K.; Vodanovic, M.; Mestrovic, S.; Rosin-Grget, K.; Valic, M. Physical fitness course in the dental curriculum and prevention of low back pain. J. Dent. Educ. 2011, 75, 761–767. [Google Scholar] [PubMed]
- Koneru, S.; Tanikonda, R. Role of yoga and physical activity in work-related musculoskeletal disorders among dentists. J. Int. Soc. Prev. Community Dent. 2015, 5, 199–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talpos-Niculescu, C.; Lungeanu, D.; Anghel, M.; Ioan Stratul, S.; Bucur, A. The role of physical exercise in preventing musculoskeletal disorders caused by the dental profession. Timis. Med. J. 2010, 8, 293–298. [Google Scholar]
- Beaton, D.E.; Katz, J.N.; Fossel, A.H.; Wright, J.G.; Tarasuk, V.; Bombardier, C. Measuring the whole or the parts? Validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. J. Hand Ther. 2001, 14, 128–146. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PICOS | Study Inclusion Criteria |
|---|---|
| Population (P) | Dental professionals: e.g., dentists, orthodontists, dental assistants/hygienists/technicians/surgeons/students, dental laboratory assistants |
| Intervention (I) | Ergonomic interventions that lasted for at least two days |
| Control group (C) | All suitable control groups, including subjects representing both the intervention and control group (here, own controls) |
| Outcome (O) | Related to MSDs (prevalence or symptoms) or to working posture |
| Study design (S) | Intervention or evaluation studies, randomized controlled trials (RCTs), observational studies (e.g., cohort studies), once the effect of the intervention had been clearly analyzed |
| Additional Criteria | |
| Language | English |
| Publication status | Published and accessible articles with related abstracts, ideally from peer-reviewed journals |
| Publication date | January 2008 to May 2018 (update April 2019) |
| Reference | Study Design | Country | Setting | Population | Sample Size IG/CG | Related Outcome | Intervention | Study Quality Score |
|---|---|---|---|---|---|---|---|---|
| Dable 2014 [17] | Evaluation (between-subject experimental design) | India, Asia | Dental school/university | Dental students | 90 see above | Working posture | Ergonomic dental chairs, magnification loupes, lecture in ergonomics | 15 (Moderate) |
| Dehghan 2016 [16] | Intervention (3 survey periods) | Iran, Asia | Dental hospital/clinic | Dentists | 102 50/52 | Prevalence of MSDs | Training course in ergonomics | 21 (Moderate) |
| Farrokhnia 2018 [18] | Intervention (pre-post intervention design) | Iran, Asia | Dental hospital/clinic | Dentists | 84 see above | Symptoms of MSDs | Training course | 16 (Moderate) |
| Hallaj 2016 [19] | Evaluation (pre-post intervention design) | India, Asia | Dental hospital/clinic | Dentists | 29 see above | Working posture | Ergonomic dental chair with arm support | 11 (Moderate) |
| Hayes 2014 [20] | Intervention (pre-post intervention design) | Australia, Oceania | Dental school/university | Dental hygienists, dental hygiene students | 29 12/17 | Symptoms of MSDs | Magnification loupes | 18 (Moderate) |
| Hayes 2016a [21] | Intervention (pre-post intervention design) | Australia, Oceania | Dental school/university | Dental hygienists, dental hygiene students | 29 12/17 | Symptoms of MSDs | Magnification loupes | 23 (High) |
| Koni 2018 [14] | Intervention (pre-post intervention design) | Italy, Europe | Dental school/university | Dental students | 55 see above | Symptoms of MSDs | Training course in ergonomics | 22 (High) |
| Lindegård 2012 [22] | RCT (pre-post intervention design) | Sweden, Europe | Dental hospital/clinic | Dentists, dental hygienists | 45 25/20 | Working posture | Prismatic spectacles, lecture in ergonomics | 23 (High) |
| Lindegård 2016 [23] | Cohort (longitudinal pre-post intervention design) | Sweden, Europe | Dental hospital/clinic | Dentists, dental hygienists, orthodontic assistants | 564 371/193 | Symptoms of MSDs | Prismatic spectacles | 17 (Moderate) |
| Maillet 2008 [24] | Intervention (3 survey periods) | Canada, North America | Dental school/university | Dental hygiene students | 35 see above | Working posture | Magnification loupes | 20 (Moderate) |
| Rempel 2012 [25] | RCT (pre-post intervention design) | United States, North America | Dental practice | Dentists, dental hygienists | 110 54/56 | Symptoms of MSDs | Dental instruments | 30 (High) |
| Reference | Type of Prevention | Description of Intervention | Effect of Intervention | Analyzed Body Regions |
|---|---|---|---|---|
| Ergonomic Dental Chair | ||||
| Dable 2014 [17] | Setting prevention | Intervention: Ergonomic dental chairs; magnification loupes; lecture in ergonomics. Facts: 3 different dental chairs were analyzed (30 dental students in each group)—(a) saddle stool, (b) conventional chair with back rest, (c) conventional chair without back rest. All investigations on working posture were carried out without and with magnification loupes. All students were lectured on ergonomic posture. After 3 months of training, the assessment procedure started; it lasted for 3 days. Survey instruments: Rapid Upper Limb Assessment (RULA) & videotapes Control: Study participants were their own controls (allocated dental chair without vs. with magnification loupes) Length: 3 months Follow up: In 3 days MSD status of participants: Is not stated, but there is a hint that some participants had mild MSDs before the intervention |
|
|
| Hallaj 2016 [19] | Setting prevention | Intervention: Ergonomic dental chair with arm support Facts: A new designed arm support device was tested Survey instruments: Rapid Upper Limb Assessment (RULA) and photographs, feedback questionnaire with self-developed questions Control: Study participants were their own controls Length: 1 week Follow up: Time is not stated MSDs status of participants: Is not stated |
|
|
| Magnification Loupes | ||||
| Hayes 2014 [20] | Setting prevention | Intervention: Magnification loupes Facts: Galilean flip-up style loupes with 2.5 x magnification were used. The convergence and working angles of the magnification loupes were adjustable. Survey instruments: Disabilities of the Arm, Shoulder and Hand (DASH) Questionnaire, physical assessments based on validated protocols Control: Dental hygiene students not wearing magnification loupes Length: 6 months Follow up: After 6 monthsMSDs status of participants: All study subjects experienced MSDs before the intervention, subjects with chronic MSD conditions were not included in the study |
|
|
| Hayes 2016a [21] | Setting prevention | Intervention: Magnification loupes Facts: Galilean flip-up style loupes with 2.5 × magnification were used. The convergence and working angles of the magnification loupes were adjustable. Survey instruments: Neck Pain and Disability Scale (NPDS), physical assessments based on validated protocols Control: Dental hygiene students not wearing magnification loupes Length: 6 months Follow up: After 6 months MSDs status of participants: All study subjects experienced MSDs before the intervention, subjects with chronic MSDs conditions (persistent pain for at least 3 months) or with pre-existing MSDs unrelated to occupational factors were not included in the study |
|
|
| Maillet 2008 [24] | Setting prevention | Intervention: Magnification loupes Facts: The magnification loupes were Hires flip-ups, complete with head straps and side shields. The frames were all standard titanium frames, slate in color. Orascoptic also provided three rigid headbands to allow for prescription eyeglass wearers. The headbands and standard frames had interchangeable working lengths to allow for portability within the group. The magnification for all was 2.5 ×. The study consisted of two parts: preliminary study and formal study that were implemented in 2005. Group 1 wore the loupes for the first session and worked without them for the second session, while Group 2 worked without loupes for the first session and with loupes for the second. Survey instruments: Posture Assessment Instrument (PAI), Posture Assessment Criteria (PAC), post-study-survey with self-developed questions and videotapes Control: Study participants were their own controls (2 sessions each with and without magnification loupes) Length: 7 months Follow up: After 7 monthsMSDs status of participants: Is not stated |
|
|
| Prismatic Spectacles | ||||
| Lindegård 2012 [22] | Setting prevention | Intervention: Prismatic spectacles; lecture in ergonomics Facts: The prismatic glasses include optometric correction. The ergonomic education (lecture in ergonomics) includes a comprehensive 1.5 h information session about dental ergonomics including working postures, working technique and visual ergonomics. All study participants underwent the education. The assessments lasted 4 months. Survey instruments: Borg’s RPE Scale (modified), inclinometers and questionnaires Control: Dentists and dental hygienists not wearing prismatic spectacles Length: 12 months Follow up: CG: 7 and 8 weeks after the education, IG: 9 to 11 weeks and 12 months after the intervention MSD status of participants: Is not stated |
|
|
| Lindegård 2016 [23] | Setting prevention | Intervention: Prismatic spectacles Facts: All participants in the intervention group were given an eye test for adjusting the prismatic glasses individually. Survey instruments: Nordic Musculoskeletal Questionnaire (NMQ), Work Ability Index (WAI), questionnaire with self-developed questions for the follow up assessment, physical assessments based on Health Surveillance in Adverse Ergonomics Conditions (HECO) protocols Control: Remaining dental personnel not receiving prismatic spectacles Length: 12 months Follow up: After 12 months MSE status of participants: All study subjects experienced MSDs before the intervention (at baseline); the intervention group reported a higher prevalence of MSDs and clinical diagnoses at baseline than the control group |
|
|
| Dental Instruments | ||||
| Rempel 2012 [25] | Setting prevention | Intervention: Dental instruments Facts: Instrument 1 weighed 14g and had an 11mm diameter handle, Instrument 2 weighed 34g and had an 8mm diameter handle. Instrument 1 was made from black plastic, and Instrument 2, from steel plated with black coating. Randomization took place at the level of the dental office. Survey instruments: Online questionnaires at baseline, weekly during the intervention and at follow up Control: 2 intervention groups with own controls (use of light/wide vs. heavy/narrow instrument) Length: 5 months Follow up: After 5 months MSDs status of participants: Study subjects experienced MSDs before the intervention; subjects who received any treatment of MSDs before the intervention were not included in the study |
|
|
| Training Course in Ergonomics | ||||
| Dehghan 2016 [16] | Behavioral prevention | Intervention: Training course in ergonomics Facts: The intervention includes 4 sections: 1. knowledge and training about ergonomics (training sessions), 2. workstation modification (instructions how to modify working postures), 3. training and surveying ergonomics at the workstation (working conditions were evaluated, discussed and modified), 4. regular exercise program (stretching movements were explained by a physiotherapist). Survey instrument: Nordic Musculoskeletal Questionnaire (NMQ) Control: Dentists not receiving the ergonomic intervention program Length: 2 months Follow ups: After 3 and 6 months MSD status of participants: Is not stated |
|
|
| Farrokhnia 2018 [18] | Behavioral prevention | Intervention: Training course Facts: The educational intervention included a brief face-to-face teaching and distributing pamphlets Survey instruments: Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) and questionnaire with self-developed questions Control: Study participants were their own controls Length: More than two days (probably a few weeks) Follow up: After 2 months MSDs status of participants: Most of the study subjects (87%) experienced MSDs before the intervention; some study subjects (13%) were free of MSDs at this time |
|
|
| Koni 2018 [14] | Behavioral prevention | Intervention: Training course in ergonomics Facts: The intervention comprised several training sessions, each of 60 minutes in length. The program was organized by the University of Trieste, School of Dentistry and Physiotherapy degree course. The course taught the participants in basic knowledge on working postures and MSDs and in prevention strategies against symptoms of MSDs. Survey instruments: Verbal Numerical Scale (VNS), photographs and questionnaires Control: Study participants were their own controls Length: More than two days (probably a few weeks) Follow up: After 3 months MSDs status of participants: Is not stated, but there is a hint that all study participants had some form of MSDs before the intervention |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lietz, J.; Ulusoy, N.; Nienhaus, A. Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 3482. https://doi.org/10.3390/ijerph17103482
Lietz J, Ulusoy N, Nienhaus A. Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2020; 17(10):3482. https://doi.org/10.3390/ijerph17103482
Chicago/Turabian StyleLietz, Janna, Nazan Ulusoy, and Albert Nienhaus. 2020. "Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review" International Journal of Environmental Research and Public Health 17, no. 10: 3482. https://doi.org/10.3390/ijerph17103482
APA StyleLietz, J., Ulusoy, N., & Nienhaus, A. (2020). Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review. International Journal of Environmental Research and Public Health, 17(10), 3482. https://doi.org/10.3390/ijerph17103482