Improving Working Conditions and Job Satisfaction in Healthcare: A Study Concept Design on a Participatory Organizational Level Intervention in Psychosocial Risks Management

 , ,
, , 
Abstract
:1. Introduction
1.1. The INAIL’s Methodology
1.2. Key Principles of an Participatory Organizational-Level Intervention
2. Material and Methods
2.1. Design and Setting
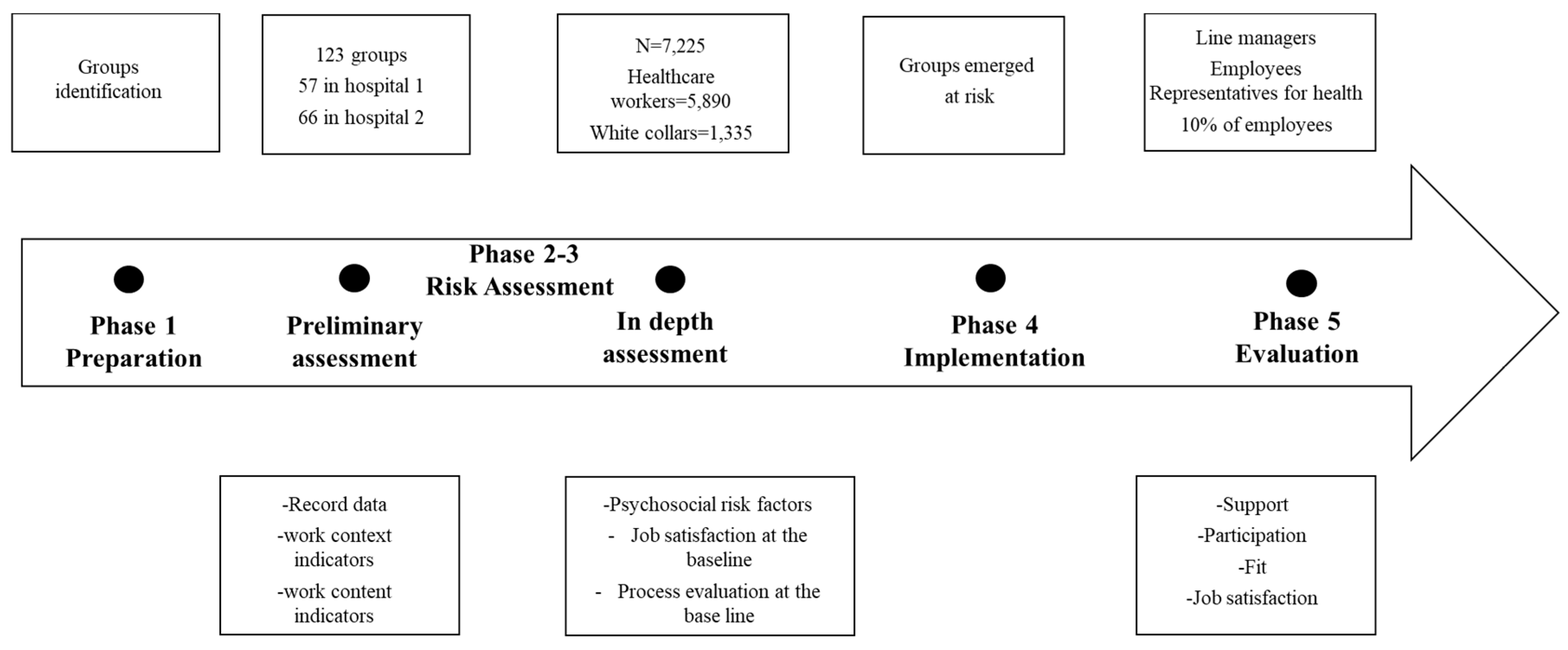
2.2. Study Population, Sample, and Procedures
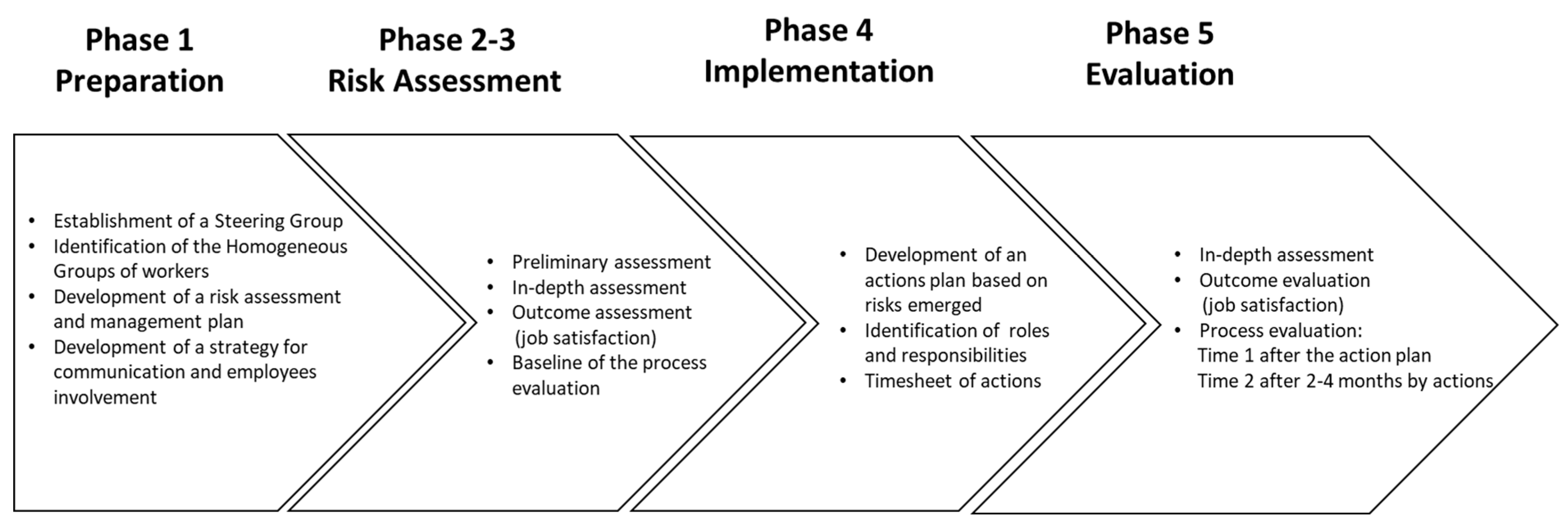
2.3. The Participatory Organizational-level Intervention
- Establishment of the Steering Group for the assessment and management of psychosocial risks. The employer, or in the case of hospitals, senior management, formally establishes a Steering group consisting of key stakeholders with a stake in worker health and working conditions, such as OSH professionals, human resource managers, and occupational psychologists. The key function of the Steering Group is to plan, monitor, and facilitate the process, to determine key milestones and to inform employees about intervention progress. A project champion should be identified who can coordinate the different activities and roles [43].
- Identification of the Homogeneous Groups of employees. Following Italian recommendation [30], organizations with more than 30 employees must set the assessment and management of work-related stress risks at the group level. As the hospitals involved in the present study have more than 3000 employed each, the Steering Committees in the respective hospitals identify Homogeneous Groups. Such groups consist of employees who share similar aspects of work organization, thus experiencing similar working conditions and work environment, who are within the same chain of command, and who receive communication through the same channels.
- Development of a POI plan with a formal timesheet of each action to be taken, roles, resources, and responsibilities.
- Development of a strategy of communication to inform employees about the POI, its phases and framework, surveys/questionnaires used in the assessment, figures involved, and timesheet. Communication should happen using the organization’s formal communication channels to disseminate information in the organization. Moreover, employee representatives for health are involved to improve informal communication, too [43].
- Identifying corrective/improvement action priorities based on the assessment results. The Steering Group examines and discusses the results of the assessment in order to establish the priority areas in which to intervene, especially in the event of multiple critical aspects requiring different actions.
- Verifying the need for any in-depth analysis or additional information. At this stage, participation is crucial. The involvement of the workers from the group, through focus group and workshops, can be helpful to better interpret the results of the assessment phases and to gather suggestions for effective and appropriate solutions. Focus groups can be conducted to inform the work of the Steering group in identifying corrective actions, particularly in those groups where it is not immediate to link actions to the risk areas emerged.
- Establishing improvement actions with regard to the priorities identified. The Steering Group establishes the actions to be implemented by evaluating their relevance and feasibility. At this stage, involvement of line managers with operational meeting is suggested. Line managers have a decision-making power over work processes and procedures requiring changes. They have also a role in promoting and communicating changes to employee. They can support and facilitate the implementation of the improvement actions defined by the Steering Group.
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schulte, P.A.; Delclos, G.; Felknor, S.A.; Chosewood, L.C. Toward an expanded focus for Occupational Safety and Health: A Commentary. Int. J. Environ. Res. Public Health 2019, 16, 4946. [Google Scholar] [CrossRef] [Green Version]
- Leka, S.; Jain, A. Health Impact of Psychosocial Hazards at Work: An Overview; World Health Organization: Geneva, Switzerland, 2010; ISBN 978-92-4-150027-2. [Google Scholar]
- EU-OSHA (European Agency for Safety and Health at Work). Second European Survey of Enterprises on New and Emerging Risks (ESENER-2). Overview Report: Managing Safety and Health at Work; Publications Office of the European Union: Luxembourg, 2016; ISBN 978-92-9240-897-8. [Google Scholar]
- European Council. Council Directive of 12 June 1989 on the introduction of measures to encourage improvements in the safety and health of workers at work (89/391/EEC). OJ L 1989, 183, 1–8. [Google Scholar]
- European Social Partners. Framework agreement on work-related stress. In European Social Partners–ETUC; UNICE(BUSINESSEUROPE), UEAPME and CEEP: Brussels, Belgium, 2004. [Google Scholar]
- Di Tecco, C.; Jain, A.; Valenti, A.; Iavicoli, S.; Leka, S. An evaluation of the impact of a policy-level intervention to address psychosocial risks on organisational action in Italy. Saf. Sci. 2017, 100, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Leka, S.; Jain, A.; Iavicoli, S.; Di Tecco, C. An evaluation of the policy context on psychosocial risks and mental health in the workplace in the European Union: Achievements, challenges and the future. BioMed Res. Int. 2015, 2015, 213089:1–213089:18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeJoy, D.M.; Wilson, M.G.; Vandenberg, R.J.; McGrath-Higgins, A.L.; Griffin-Blake, C.S. Assessing the impact of healthy work organization intervention. J. Occup. Organ. Psychol. 2010, 83, 139–165. [Google Scholar] [CrossRef]
- Framke, E.; Sørensen, O.H.; Pedersen, J.; Rugulies, R. Effect of a participatory organizational-level occupational health intervention on job satisfaction, exhaustion and sleep disturbances: Results of a cluster randomized controlled trial. BMC Public Health 2016, 16, 1210. [Google Scholar] [CrossRef] [Green Version]
- Faragher, E.B.; Cass, M.; Cooper, C.L. The relationship between job satisfaction and health: A meta-analysis. Occup. Environ. Med. 2005, 62, 105–112. [Google Scholar] [CrossRef]
- Nielsen, K.; Randall, R. The importance of employee participation and perception of changes in procedures in a teamworking intervention. Work Stress 2012, 26, 91–111. [Google Scholar] [CrossRef] [Green Version]
- ILO (International Labour Organization). Workplace Stress: A Collective Challenge; International Labour Organization Publications: Geneva, Switzerland, 2016; ISBN 978-92-2-130641-2. [Google Scholar]
- Eurofound and EU-OSHA. Psychosocial Risks in Europe: Prevalence and Strategies for Prevention; Publications Office of the European Union: Luxembourg, 2014; ISBN 978-92-897-1218-7. [Google Scholar]
- Kivimäki, M.; Kawachi, I. Work stress as a risk factor for cardiovascular disease. Curr. Cardiol. Rep. 2015, 17, 74:1–74:9. [Google Scholar] [CrossRef] [Green Version]
- Kraatz, S.; Lang, J.; Kraus, T.; Münster, E.; Ochsmann, E. The incremental effect of psychosocial workplace factors on the development of neck and shoulder disorders: A systematic review of longitudinal studies. Int. Arch. Occup. Environ. Health 2013, 86, 375–395. [Google Scholar] [CrossRef]
- Madsen, I.E.; Nyberg, S.T.; Hanson, L.M.; Ferrie, J.E.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Job strain as a risk factor for clinical depression: Systematic review and meta-analysis with additional individual participant data. Psychol. Med. 2017, 47, 1342–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EU-OSHA (European Agency for Safety and Health at Work). Third European Survey of Enterprises on New and Emerging Risks (ESENER-3). First Findings; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar]
- Eurofound. Sixth European Working Conditions Survey–Overview Report (2017 Update); Publications Office of the European Union: Luxembourg, 2017; ISBN 978-92-897-1596-6. [Google Scholar]
- Krämer, T.; Schneider, A.; Spieß, E.; Angerer, P.; Weigl, M. Associations between job demands, work-related strain and perceived quality of care: A longitudinal study among hospital physicians. Int. J. Qual. Health Care 2016, 28, 824–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donchin, Y.; Seagull, F.J. The hostile environment of the intensive care unit. Curr. Opin. Crit. Care 2002, 8, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Firth-Cozens, J.; Greenhalgh, J. Doctors’ perceptions of the links between stress and lowered clinical care. Soc. Sci. Med. 1997, 44, 1017–1022. [Google Scholar] [CrossRef]
- INAIL. Indagine Nazionale Sulla Salute e Sicurezza dei Lavoratori-Lavoratori e Datori di Lavoro; Tipolitografia INAIL: Milan, Italy, 2014; ISBN 978-88-7484-394-7. [Google Scholar]
- LaMontagne, A.D.; Keegel, T.; Louie, A.M.; Ostry, A.; Landsbergis, P.A. A systematic review of the job-stress intervention evaluation literature, 1990-2005. Int. J. Occup. Environ. Health 2007, 13, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.; Miraglia, M. What works for whom in which circumstances? On the need to move beyond the ‘what works?’ question in organizational intervention research. Hum. Relat. 2017, 70, 40–62. [Google Scholar] [CrossRef] [Green Version]
- Di Tecco, C.; Ronchetti, M.; Ghelli, M.; Russo, S.; Persechino, B.; Iavicoli, S. Do italian companies manage work-related stress effectively? A process evaluation in implementing the Inail methodology. BioMed Res. Int. 2015, 2015, 197156:1–197156:10. [Google Scholar] [CrossRef] [Green Version]
- Persechino, B.; Valenti, A.; Ronchetti, M.; Rondinone, B.M.; Di Tecco, C.; Vitali, S.; Iavicoli, S. Work related stress risk assessment in Italy: A methodological proposal adapted to regulatory guidelines. Saf. Health Work 2013, 4, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Ronchetti, M.; Di Tecco, C.; Russo, S.; Castaldi, T.; Vitali, S.; Autieri, S.; Valenti, A.; Persechino, B.; Iavicoli, S. An integrated approach to the assessment of work-related stress risk: Comparison of findings from two tools in an Italian methodology. Saf. Sci. 2015, 80, 310–316. [Google Scholar] [CrossRef]
- Nielsen, K.; Abildgaard, J.S. Organizational interventions: A research-based framework for the evaluation of both process and effects. Work Stress 2013, 27, 278–297. [Google Scholar] [CrossRef]
- INAIL. Valutazione e Gestione del Rischio da Stress Lavoro-Correlato. Manuale ad uso Delle Aziende in Attuazione del D.Lgs. 81/08 e s.m.i.; Tipolitografia INAIL: Milan, Italy, 2011; ISBN 978-88-7484-197-4. [Google Scholar]
- INAIL. The Methodology for the Assessment and Management of Work-Related Stress Risk. Handbook for Companies, in Compliance with LEGISLATIVE. Decree 81/2008 and Subsequent Integrations and Modifications; Tipolitografia INAIL: Milan, Italy, 2018; ISBN 978-88-7484-119-6. [Google Scholar]
- Barbaranelli, C.; Ghezzi, V.; Di Tecco, C.; Ronchetti, M.; Fida, R.; Ghelli, M.; Persechino, B.; Iavicoli, S. Assessing objective and verifiable indicators associated with work-related stress: Validation of a structured checklist for the assessment and management of work-related stress. Front. Psychol. 2018, 9, 2424:1–2424:16. [Google Scholar] [CrossRef] [PubMed]
- Rondinone, B.M.; Persechino, B.; Castaldi, T.; Valenti, A.; Ferrante, P.; Ronchetti, M.; Iavicoli, S. Work-related stress risk assessment in Italy: The validation study of Health Safety and Executive Indicator Tool. G. Ital. Med. Lav. Ergon. 2012, 34, 392–399. [Google Scholar] [PubMed]
- Wood, S.; Ghezzi, V.; Barbaranelli, C.; Di Tecco, C.; Fida, R.; Farnese, M.L.; Ronchetti, M.; Iavicoli, S. Assessing the risk of stress in organizations: Getting the measure of organizational level stressors. Front. Psychol. 2019, 10, 2776:1–2776:18. [Google Scholar] [CrossRef] [PubMed]
- Cox, T. The recognition and measurement of stress: Conceptual and methodological issues. In Evaluation of Human Work. A practical ergonomics methodology, 1st ed.; Corlett, E.N., Wilson, J., Eds.; Taylor & Francis: London, UK, 1990; ISBN 978-0850664799. [Google Scholar]
- Cox, T.; Griffiths, A.; Rial-Gonzales, E. Research on Work-Related Stress. Report EU-OSHA; Office for Official Publications of the European Communities: Luxembourg, 2000; ISBN 92-828-9255-7. [Google Scholar]
- Nielsen, K.; Noblet, A. Introduction: Organizational interventions: Where we are, where we go from here? In Organizational Interventions for Health and well-being: A Handbook for Evidence-Based Practice; Nielsen, K., Noblet, A., Eds.; Routledge: Oxon, UK, 2018; pp. 1–23. ISBN 978-1-138-22141-3. [Google Scholar]
- Leka, S.; Cox, T. Psychosocial Risk Management at the Workplace Level. In Occupational Health Psychology; Leka, S., Houdmont, J., Eds.; Wiley Blackwell: Oxford, UK, 2010; pp. 124–156. ISBN 978-1-405-19115-9. [Google Scholar]
- Nielsen, K. How can we make organizational interventions work? Employees and line managers as actively crafting interventions. Hum. Relat. 2013, 66, 1029–1050. [Google Scholar] [CrossRef]
- Tafvelin, S.; von Thiele Schwarz, U.; Nielsen, K.; Hasson, H. Employees’ and line managers’ active involvement in participatory organizational interventions: Examining direct, reversed, and reciprocal effects on well-being. Stress Health 2018, 35, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, K. Leaders can make or break an intervention–but are they the villains of the play? In Leading to Occupational Health and Safety: How Leadership Behaviours Impact Organizational Safety and Well-Being; Kelloway, K., Nielsen, K., Dimoff, J., Eds.; Wiley Blackwell: Chichester, UK, 2017; pp. 197–210. ISBN 978-1-118-97370-7. [Google Scholar]
- Balducci, C.; Consiglio, C.; Avanzi, L.; De Longis, E.; Cepale, G. La valutazione del rischio stress lavoro-correlato nel settore socio-sanitario. In Proceedings of the “La Gestione Del Rischio Stress Lavoro-Correlato” National Conference, Rome, Italy, 14 July 2016. [Google Scholar]
- Di Tecco, C.; Ronchetti, M.; Ghelli, M.; Persechino, B.; Iavicoli, S. La gestione del rischio stress lavoro-correlato nelle aziende nell’ottica di processo e prevenzione: Approfondimenti sulla metodologia INAIL. G. Ital. di Psicol. 2019, 1–2, 107–112. [Google Scholar]
- Nielsen, K.; Stage, M.; Abildgaard, J.S.; Brauer, C.V. Participatory intervention from and organizational perspective: Employees as active agents in creating a healthy work environment. In Concepts of Salutogenic Organizations and Change: The Logics behind Organizational Health Intervention Research; Bauer, G., Jenny, G., Eds.; Springer Publications: Dordrecht, The Netherlands, 2013; pp. 327–350. ISBN 978-94-007-6470-5. [Google Scholar]
- INAIL. Piano di monitoraggio e d’intervento per l’ottimizzazione della valutazione e gestione dello stress lavoro-correlato. In Uno Sguardo ai Principali Risultati; Tipografia INAIL: Milano, Italy, 2016; ISBN 978-88-7484- 508-8. [Google Scholar]
- Dubinsky, A.J.; Howell, R.D.; Ingram, T.M.; Bellenger, D. Salesforce socialization. J. Mark. 1986, 50, 192–207. [Google Scholar] [CrossRef]
- Day, A.; Nielsen, K. What does our organization do to help our well-being? Creating healthy workplaces and workers. In An Introduction to Work and Organizational Psychology: An International Perspective, 3rd ed.; Chmiel, N., Fraccaroli, F., Sverke, M., Eds.; Wiley Blackwell: Chichester, UK, 2017; pp. 295–314. ISBN 978-1119168027. [Google Scholar]
- Nielsen, K.; Yarker, J.; Munir, F.; Bültmann, U. IGLOO: An integrated framework for sustainable return to work in workers with common mental disorders. Work Stress 2018, 32, 400–417. [Google Scholar] [CrossRef] [Green Version]
- Pawson, R.; Tilley, N. Realistic Evaluation; SAGE Publications: London, UK, 1997; ISBN 978-0761950097. [Google Scholar]
- Biron, C.; Gatrell, C.J.; Cooper, C.L. Autopsy of a failure. Evaluating process and contextual issues in an organizational-level work stress intervention. Int. J. Stress Manag. 2010, 17, 135–158. [Google Scholar] [CrossRef]
- Uchiyama, A.; Odagiri, Y.; Ohya, Y.; Takamiya, T.; Inoue, S.; Shimomitsu, T. Effect on mental health of a participatory intervention to improve psychosocial work environment: A cluster randomized controlled trial among nurses. J. Occup. Health 2013, 55, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Weiner, B.J. A theory of organizational readiness for change. Implement. Sci. 2009, 4, 67:1–67:9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Thiele Schwarz, U.; Nielsen, K.; Stenfors-Hayes, T.; Hasson, H. Using Kaizen to improve employee wellbeing: Results from two organizational intervention studies. Hum. Relat. 2017, 70, 966–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, G.; Peters, S.; Nielsen, K.; Nagler, E.; Karapanos, M.; Wallace, L.; Burke, L.; Dennerlein, J.T.; Wagner, G.R. Improving working conditions to promote worker safety, health, and wellbeing for low-wage workers: The Workplace Organizational Health study. Int. J. Environ. Res. Public Health 2019, 16, 1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray-Toft, P.; Anderson, J.G. Organizational stress in the hospital: Development of a model for diagnosis and prediction. Health Serv. Res. 1985, 19, 753–774. [Google Scholar] [PubMed]
- Nielsen, K.; Nielsen, M.B.; Ogbonnaya, C.; Känsälä, M.; Saari, E.; Isaksson, K. Workplace resources to improve both employee well-being and performance: A systematic review and meta-analysis. Work Stress 2017, 31, 101–120. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Standard | Integrative * |
|---|---|
| Work-related Injuries | Mortality Ratio |
| Sick Leave Absences | Complaints from patients and relatives |
| Absences from Work | Patient aggressions |
| Left-over Vacation Days | Internal transfers managed by the company |
| Job Rotation | Prevalence of employees from other or0ganization |
| Turnover | Prevalence of contingent employees |
| Legal Actions/Disciplinary Sanctions | Appropriate procedures for shift work |
| Requests for Extraordinary | Work availability at night |
| Visits to the Occupational Physician | Tiling and training procedures for newcomers |
| Formal Records of Employees’ Complaints to the Company or to the Occupational Physician | Analysis of training needs |
| Work Environment and Work Equipment | Organizational changes |
| Task Planning | Procedures for managing conflicts |
| Work Load/Pattern of Work | Procedures for managing conflicts with patients/relatives |
| Working Hours | |
| Function and Organisational Culture | |
| Role Within the Organisation | |
| Career Path | |
| Decision-Making and Work Control | |
| Interpersonal Relationships at Work | |
| Home-Work Interface - Work/life Reconciliation |
| Standard | Integrative ** |
|---|---|
| Demands | Work-family conflict |
| Control | Emotional burden |
| Role | Team/equip integration |
| Support from colleagues | Emotional dissonance |
| Support from management | Harassment and violence |
| Relationships | Ergonomic risk |
| Change | Organizational fairness |
| Interaction with patients |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Tecco, C.; Nielsen, K.; Ghelli, M.; Ronchetti, M.; Marzocchi, I.; Persechino, B.; Iavicoli, S. Improving Working Conditions and Job Satisfaction in Healthcare: A Study Concept Design on a Participatory Organizational Level Intervention in Psychosocial Risks Management. Int. J. Environ. Res. Public Health 2020, 17, 3677. https://doi.org/10.3390/ijerph17103677
Di Tecco C, Nielsen K, Ghelli M, Ronchetti M, Marzocchi I, Persechino B, Iavicoli S. Improving Working Conditions and Job Satisfaction in Healthcare: A Study Concept Design on a Participatory Organizational Level Intervention in Psychosocial Risks Management. International Journal of Environmental Research and Public Health. 2020; 17(10):3677. https://doi.org/10.3390/ijerph17103677
Chicago/Turabian StyleDi Tecco, Cristina, Karina Nielsen, Monica Ghelli, Matteo Ronchetti, Ivan Marzocchi, Benedetta Persechino, and Sergio Iavicoli. 2020. "Improving Working Conditions and Job Satisfaction in Healthcare: A Study Concept Design on a Participatory Organizational Level Intervention in Psychosocial Risks Management" International Journal of Environmental Research and Public Health 17, no. 10: 3677. https://doi.org/10.3390/ijerph17103677
APA StyleDi Tecco, C., Nielsen, K., Ghelli, M., Ronchetti, M., Marzocchi, I., Persechino, B., & Iavicoli, S. (2020). Improving Working Conditions and Job Satisfaction in Healthcare: A Study Concept Design on a Participatory Organizational Level Intervention in Psychosocial Risks Management. International Journal of Environmental Research and Public Health, 17(10), 3677. https://doi.org/10.3390/ijerph17103677