Preconception Care in a Remote Aboriginal Community Context: What, When and by Whom?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type
2.2. Participants
2.3. Person, Place, Time
2.4. Data Analysis
2.5. Ethics
3. Results
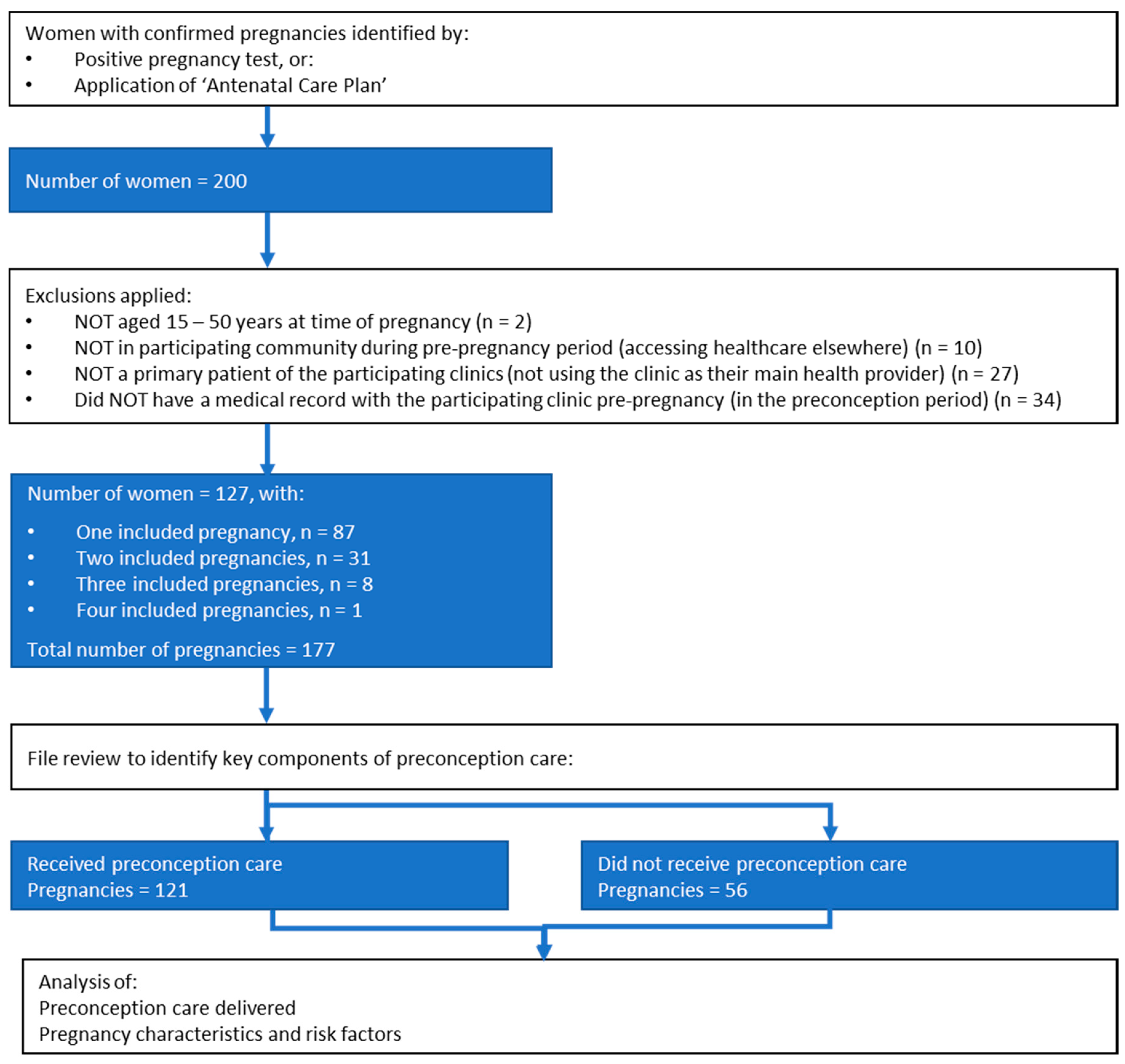
3.1. Participants and Pregnancy Characteristics
3.2. Pregnancy Risk Factors
3.3. Characteristics of Preconception Care Delivered
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Component | Royal Australian College of General Practitioners Recommendations [11] | Criteria Used to Count Care in Audit (Any of the Following): |
|---|---|---|
| Key components audited: | ||
| Folic acid supplementation | Most women: 0.5 mg/day supplementation, beginning ideally at least one month prior to conception and continuing for the first trimester. High-risk women: 5 mg/day supplementation. | Prescription of and/or dispensing of supply of folic acid (with or without iodine or iron); explanation of indication and support with adherence. |
| Nutrition and weight assessment | Nutritional assessment and appropriate intervention with an emphasis on optimising maternal body mass index (BMI) and micronutrient reserves. | Advice re. impact of weight and nutrition on conception and pregnancy; support to improve diet, weight and activity levels for healthy pregnancy. |
| Smoking cessation | Inform women who smoke that tobacco affects fetal growth and advise them to stop smoking. | Advice re. impact of use in pregnancy and support with cessation; prescription of nicotine replacement therapy, with reference to healthy pregnancy. |
| Alcohol and illicit drug use | Advise that not drinking is the safest option; illicit drugs may harm the fetus, advise them to avoid use. | Level of use documented; advice re. impact of use in pregnancy and support with cessation. |
| Chronic diseases | Optimise control of existing chronic diseases (e.g., diabetes, hypertension, epilepsy). Avoid teratogenic medications. | Management of chronic disease for healthy pregnancy. |
| Vaccinations | MMR; varicella (in those without a clear history of chickenpox or who are non-immune on testing); influenza; diphtheria; tetanus; acellular pertussis. | Collection of pathology to determine immune status; administration of relevant vaccine. |
| Sexually transmissible infections (STI) * | Screening for STI and/or treatment for healthy pregnancy; advice re. regular testing, impact of STI in pregnancy, STI prevention. | |
| Additional components audited: | ||
| Psychosocial health | Discuss perinatal mental health conditions, psychological or psychiatric assessment and treatment, use of medication and the risk of exacerbation of mood disorders in pregnancy and postpartum. Mental health screening should include a psychosocial assessment. | Family and domestic violence OR mental health discussed, documented or assessed using formal tool; advice re. impact of use in pregnancy; brief intervention or referral to support agencies. |
| Cervical screening | Completion of cervical screening or pap smear. | |
| Advice regarding normal reproduction and conception | Advice re. timing of ovulation and positive pregnancy tests; fertile periods; signs and symptoms of early pregnancy. | |
References
- Preconception Care: Maximizing the Gains for Maternal and Child Health; World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.who.int/maternal_child_adolescent/documents/preconception_care_policy_brief.pdf?ua=1 (accessed on 23 January 2020).
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- van Elten, T.M.; van de Beek, C.; Geelen, A.; Gemke, R.J.; Groen, H.; Hoek, A.; Mol, B.W.; van Poppel, M.N.; Roseboom, T.J. Preconception Lifestyle and Cardiovascular Health in the Offspring of Overweight and Obese Women. Nutrients 2019, 11, 2446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oestreich, A.K.; Moley, K.H. Developmental and Transmittable Origins of Obesity-Associated Health Disorders. Trends Genet. 2017, 33, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Bueno, C.; Cavero-Redondo, I.; Lucas-De La Cruz, L.; Notario-Pacheco, B.; Martínez-Vizcaíno, V. Association between pre-pregnancy overweight and obesity and children’s neurocognitive development: A systematic review and meta-analysis of observational studies. Int. J. Epidemiol. 2017, 46, 1653–1666. [Google Scholar] [CrossRef] [PubMed]
- Government of Western Australia Department of Health. WA Aboriginal Health and Wellbeing Framework 2015–2030. 2015. Available online: https://ww2.health.wa.gov.au/~/media/Files/Corporate/general%20documents/Aboriginal%20health/PDF/12853_WA_Aboriginal_Health_and_Wellbeing_Framework.pdf (accessed on 23 January 2020).
- Kimberley Aboriginal Health Planning Forum. Strategic Plan 2018–2028, Broome, Western Australia 2018. Available online: https://kahpf.org.au/s/kahpf_stratplan.pdf (accessed on 7 January 2020).
- Asresu, T.T.; Hailu, D.; Girmay, B.; Abrha, M.W.; Weldearegay, H.G. Mothers’ utilization and associated factors in preconception care in northern Ethiopia: A community based cross sectional study. BMC Pregnancy Childbirth 2019, 19, 347. [Google Scholar] [CrossRef] [Green Version]
- Ding, Y.; Li, X.-T.; Xie, F.; Yang, Y.-L. Survey on the Implementation of Preconception Care in Shanghai, China. Paediatr. Perinat. Epidemiol. 2015, 29, 492–500. [Google Scholar] [CrossRef]
- Wally, M.K.; Huber, L.R.B.; Issel, L.M.; Thompson, M.E. The Association Between Preconception Care Receipt and the Timeliness and Adequacy of Prenatal Care: An Examination of Multistate Data from Pregnancy Risk Assessment Monitoring System (PRAMS) 2009–2011. Matern. Child Health J. 2018, 22, 41–50. [Google Scholar] [CrossRef]
- The Royal Australian College of General Practitioners. Guidelines for Preventative Activities in General Practice, 9th ed.; RACGP: East Melbourne, Australia, 2018. [Google Scholar]
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Pre-Pregnancy Counselling 2017. Available online: https://ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical-Obstetrics/Pre-pregnancy-Counselling-(C-Obs-3a)-review-July-2017_1.pdf?ext=.pdf (accessed on 1 January 2020).
- Hall, J.A.; Benton, L.; Copas, A.; Stephenson, J. Pregnancy intention and pregnancy outcome: Systematic review and meta-Analysis. Matern. Child Health J. 2017, 21, 670–704. [Google Scholar] [CrossRef] [Green Version]
- McKenna, E.; Hure, A.; Perkins, A.; Gresham, E. Dietary supplement use during preconception: The Australian longitudinal study on women’s health. Nutrients 2017, 9, 1119. [Google Scholar] [CrossRef] [Green Version]
- Taft, A.J.; Shankar, M.; Black, K.I.; Mazza, D.; Hussainy, S.; Lucke, J.C. Unintended and unwanted pregnancy in Australia: A cross-sectional, national random telephone survey of prevalence and outcomes. Med. J. Aust. 2018, 209, 407–408. [Google Scholar] [CrossRef]
- Hibbert, E.; Chalasani, S.; Kozan, P.; Myszka, R.; Park, K.; Black, K. Preconception care and contraceptive use among women with diabetes. Aust. J. Gen. Pract. 2018, 47, 877–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diabetes Australia. NDSS Diabetes in Pregnancy National Development Program: Contraception, Pregnancy and Women’s Health Survey Summary Report; Diabetes Australia: Canberra, Australia, 2015; Available online: https://www.ndss.com.au/wp-content/uploads/resources/report-contraception-pregnancy-womens-health-survey-2015.pdf (accessed on 23 January 2020).
- Klein, J.; Boyle, J.A.; Kirkham, R.; Connors, C.; Whitbread, C.; Oats, J.; Barzi, F.; McIntyre, D.; Lee, I.; Luey, M.; et al. Preconception care for women with type 2 diabetes mellitus: A mixed-methods study of provider knowledge and practice. Diabetes Res. Clin. Pract. 2017, 129, 105–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework 2017 Report; AHMAC: Canberra, Australia, 2017. Available online: https://www.aihw.gov.au/reports-data/health-welfare-overview/indigenous-health-welfare/overview (accessed on 23 January 2020).
- Thrift, A.P.; Callaway, L.K. The effect of obesity on pregnancy outcomes among Australian Indigenous and non-Indigenous women. Med. J. Aust. 2014, 201, 592–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, R.; Campbell, S.; Li, M.; McCulloch, B. The health and nutrition of young indigenous women in north Queensland-intergenerational implications of poor food quality, obesity, diabetes, tobacco smoking and alcohol use. Public Health Nutr. 2009, 12, 2143–2149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, S.K.; Lynch, J.; Esterman, A.; McDermott, R. Pre-pregnancy predictors of hypertension in pregnancy among Aboriginal and Torres Strait Islander women in north Queensland, Australia; a prospective cohort study. BMC Public Health 2013, 13, 138. [Google Scholar] [CrossRef] [Green Version]
- Campbell, S.K.; Lynch, J.; Esterman, A.; McDermott, R. Pre-pregnancy predictors of diabetes in pregnancy among Aboriginal and Torres Strait Islander women in North Queensland, Australia. Matern. Child Health J. 2012, 16, 1284–1292. [Google Scholar] [CrossRef]
- Arnold, L.; Hoy, W.; Wang, Z. Low birthweight increases risk for cardiovascular disease hospitalisations in a remote Indigenous Australian community—A prospective cohort study. Aust. N. Z. J. Public Health 2016, 40 (Suppl. 1), S102–S106. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, E.K.; Marley, J.V.; Friello, D.; Atkinson, D.N. Uptake of long-acting, reversible contraception in three remote Aboriginal communities: A population-based study. Med. J. Aust. 2016, 205, 21–25. [Google Scholar] [CrossRef]
- Griffiths, E.; Atkinson, D.; Friello, D.; Marley, J.V. Pregnancy intentions in a group of remote-dwelling Australian Aboriginal women: A qualitative exploration of formation, expression and implications for clinical practice. BMC Public Health 2019, 19, 568. [Google Scholar] [CrossRef]
- National Aboriginal Community Controlled Health Organisation (NACCHO). Aboriginal Health Definitions. 2018. Available online: https://www.naccho.org.au/about/aboriginal-health/definitions/ (accessed on 4 May 2020).
- Chronic Kidney Disease; Kimberley Aboriginal Medical Services (KAMS) and WA Country Health Service Kimberley: Broome, Australia, 2017; Available online: https://kahpf.org.au/clinical-protocols (accessed on 23 January 2020).
- Higgins, J.A.; Kramer, R.D.; Ryder, K.M. Provider bias in Long-Acting Reversible Contraception (LARC) promotion and pemoval: Perceptions of young adult women. Am. J. Public Health 2016, 106, 1932–1937. [Google Scholar] [CrossRef]
- Mazza, D.; Chapman, A. Improving the uptake of preconception care and periconceptional folate supplementation: What do women think? BMC Public Health 2010, 10, 786–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M.A.; Hunt, J.; Scrimgeour, D.J.; Davey, M.; Jones, V. Contribution of Aboriginal Community-Controlled Health Services to improving Aboriginal health: An evidence review. Aust. Health Rev. 2018, 42, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Panaretto, K.S.; Lee, H.M.; Mitchell, M.R.; Larkins, S.L.; Manessis, V.; Buettner, P.G.; Watson, D. Impact of a collaborative shared antenatal care program for urban Indigenous women: A prospective cohort study. Med. J. Aust. 2005, 182, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Australia’s Mothers and Babies 2016-in Brief; Perinatal statistics series no. 34. Cat. no. PER 97; AIHW: Canberra, Australia, 2018.
- Australian Institute of Health and Welfare. Tracking progress against the Implementation Plan goals for the Aboriginal and Torres Strait Islander Health Plan 2013–2023. Web Report Cat. No, IHW 201; 2019. Available online: https://www.aihw.gov.au/reports/indigenous-health-welfare/tracking-progress-against-ipg-2013-2023/contents/maternal-health-and-parenting-domain/goal-1-antenatal-care-first-trimester (accessed on 23 January 2020).
- Homer, C.S. Models of maternity care: Evidence for midwifery continuity of care. Med. J. Aust. 2016, 205, 370–374. [Google Scholar] [CrossRef]
- Reibel, T.; Morrison, L.; Griffin, D.; Chapman, L.; Woods, H. Young Aboriginal women’s voices on pregnancy care: Factors encouraging antenatal engagement. Women Birth 2015, 28, 47–53. [Google Scholar] [CrossRef]
- Sørensen, K.; Van Den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.A. Health literacy and adherence to medical treatment in chronic and acute illness: A meta-analysis. Patient Educ. Couns. 2016, 99, 1079–1086. [Google Scholar] [CrossRef] [Green Version]
- Lang, A.Y.; Bartlett, R.; Robinson, T.; Boyle, J.A. Perspectives on preconception health among migrant women in Australia: A qualitative study. Women Birth 2019. [Google Scholar] [CrossRef]
- Fekene, D.B.; Woldeyes, B.S.; Erena, M.M.; Demisse, G.A. Knowledge, uptake of preconception care and associated factors among reproductive age group women in West Shewa zone, Ethiopia, 2018. BMC Womens Health 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Li, D.; Huang, L.; Yang, W.; Qi, C.; Shang, L.; Xin, J.; Zeng, L.; Zhang, M.; Song, H.; Chung, M.C. Knowledge, attitude and practice level of women at the periconceptional period: A cross-sectional study in Shaanxi China. BMC Pregnancy Childbirth 2019, 19, 326. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.P.; Hopman, M.E.; Murugesu, L.; Rosman, A.N.; Smith, S.K. Preconception counselling for low health literate women: An exploration of determinants in the Netherlands. Reprod. Health. 2018, 15, 192. [Google Scholar] [CrossRef] [PubMed]
- Skogsdal, Y.; Fadl, H.; Cao, Y.; Karlsson, J.; Tyden, T. An intervention in contraceptive counseling increased the knowledge about fertility and awareness of preconception health-a randomized controlled trial. Ups. J. Med. Sci. 2019, 124, 203–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murugesu, L.; Hopman, M.E.; Van Voorst, S.F.; Rosman, A.N.; Fransen, M.P. Systematic Development of Materials for Inviting Low Health-Literate Individuals to Participate in Preconception Counseling. Int. J. Environ. Res. Public Health 2019, 16, 4223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazza, D.; Chapman, A.; Michie, S. Barriers to the implementation of preconception care guidelines as perceived by general practitioners: A qualitative study. BMC Health Serv. Res. 2013, 13, 36. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Indigenous Health Checks and Follow-Ups. Web Report Cat. No IHW 209; 2019. Available online: https://www.aihw.gov.au/reports/indigenous-australians/indigenous-health-checks-follow-ups/contents/overview (accessed on 23 January 2020).
- Dorney, E.; Black, K. Preconception care. Aust. J. Gen. Pract. 2018, 47, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Larkins, S.; Page, P.; Panaretto, K.; Mitchell, M.; Alberts, V.; McGinty, S.; Veitch, C. The transformative potential of young motherhood for disadvantaged Aboriginal and Torres Strait Islander women in Townsville, Australia. Med. J. Aust. 2011, 194, 551–555. [Google Scholar] [CrossRef]
- Stevens, L.M. Planning parenthood: Health care providers’ perspectives on pregnancy intention, readiness, and family planning. Soc. Sci. Med. 2015, 139, 44–52. [Google Scholar] [CrossRef]
- Warwick, S.; Atkinson, D.; Kitaura, T.; Lelievre, M.; Marley, J.V. Young Aboriginal people’s perspective on access to health care in remote Australia: Hearing their voices. Prog. Community Health Partnersh 2019, 13, 127. [Google Scholar] [CrossRef]
- Godfrey, E.M.; Chin, N.P.; Fielding, S.L.; Fiscella, K.; Dozier, A. Contraceptive method and use by women aged 35 and over: A qualitative study of perspectives. BMC Womens Health 2011, 11, 5. [Google Scholar] [CrossRef] [Green Version]
- Kizirian, N.V.; Black, K.I.; Musgrave, L.; Hespe, C.; Gordon, A. Understanding and provision of preconception care by general practitioners. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 799–804. [Google Scholar] [CrossRef]
- Kimberley Aboriginal Medical Services (KAMS) and WA Country Health Service Kimberley. Preconception Care, 24/06/2019. Available online: https://kahpf.org.au/clinical-protocols (accessed on 23 January 2020).
- Graham, S.; Smith, L.W.; Fairley, C.K.; Hocking, J. Prevalence of chlamydia, gonorrhoea, syphilis and trichomonas in Aboriginal and Torres Strait Islander Australians: A systematic review and meta-analysis. Sex Health 2016, 13, 99–113. [Google Scholar] [CrossRef] [PubMed]

| n | Received PCC | Did Not Receive PCC | Logistic Regression | p | |
|---|---|---|---|---|---|
| n (%) | n (%) | OR (95% CI) | |||
| Age at first antenatal visit: | |||||
| 15–19 years | 35 | 22 (18) | 13 (23) | 0.66 (0.27–1.60) | 0.35 |
| 20–24 years | 68 | 49 (41) | 19 (34) | 1 λ | |
| 25–29 years | 33 | 24 (20) | 9 (16) | 1.03 (0.39–2.73) | 0.95 |
| 30–34 years | 23 | 17 (14) | 6 (11) | 1.10 (0.38–3.21) | 0.86 |
| 35 years and over | 18 | 9 (7) | 9 (16) | 0.39 (0.11–1.41) | 0.15 |
| Pregnancy outcome: | |||||
| Live birth | 141 | 95 (78) | 46 (82) | 1 λ | |
| Miscarriage | 28 | 19 (16) | 9 (16) | 1.02 (0.32–3.24) | 0.97 |
| Other * | 8 | 7 (6) | 1 (2) | 3.39 (0.40–28.98) | 0.27 |
| Gestation at first antenatal visit: | |||||
| Unknown # | 34 | 25 (20) | 9 (16) | 1.27 (0.39–4.09) | 0.69 |
| <6 weeks | 38 | 30 (25) | 8 (14) | 1.71 (0.66–4.44) | 0.27 |
| 6–12 weeks | 67 | 46 (38) | 21 (38) | 1 λ | |
| 12–24 weeks | 26 | 13 (11) | 13 (23) | 0.46 (0.18–1.17) | 0.10 |
| 24–36 weeks | 12 | 7 (6) | 5 (9) | 0.64 (0.19–2.18) | 0.48 |
| Parity prior: | |||||
| 0 | 56 | 39 (32) | 17 (30) | 1 λ | |
| 1 | 53 | 38 (32) | 15 (27) | 1.10 (0.49–2.48) | 0.81 |
| 2 | 30 | 21 (17) | 9 (16) | 1.02 (0.41–2.54) | 0.97 |
| 3 | 18 | 13 (11) | 5 (9) | 1.13 (0.35–3.64) | 0.83 |
| 4 and greater | 20 | 10 (8) | 10 (18) | 0.44 (0.13–1.48) | 0.18 |
| Diabetes status preconception (by HbA1c (mmol/mol) or care plan allocated): | |||||
| Unknown (no result) | 98 | 64 (53) | 34 (61) | n.a. | |
| Normal (<5.7%) | 41 | 30 (25) | 11 (19) | 1 λ | |
| Prediabetes (5.7–6.4%) | 13 | 11 (9) | 2 (4) | 2.02 (0.37–10.86) | 0.41 |
| Diabetes (≥6.5%) | 25 | 16 (13) | 9 (16) | 0.65 (0.21–2.00) | 0.45 |
| Albuminuria status preconception (by albumin: creatinine ratio (mg/mmol) or care plan allocated): | |||||
| Unknown (no result) | 76 | 53 (44) | 23 (41) | n.a. | |
| Normal (<3.0) | 58 | 38 (31) | 20 (36) | 1 λ | |
| Elevated (≥3.0) | 43 | 30 (25) | 13 (23) | 1.21 (0.52–2.81) | 0.65 |
| BMI preconception (kg/m2): | |||||
| Unknown (no result) | 97 | 61 (50) | 36 (65) | n.a. | |
| <18.5 | 20 | 13 (11) | 7 (12) | 0.44 (0.12–1.65) | 0.23 |
| 18.5–25 | 26 | 21 (17) | 5 (9) | 1 λ | |
| 25–30 | 18 | 13 (11) | 5 (9) | 0.62 (0.13–2.93) | 0.55 |
| >30 | 16 | 13 (11) | 3 (5) | 1.03 (0.21–5.14) | 0.97 |
| Smoking behaviour preconception: | |||||
| Unknown (no record) | 102 | 67 (55) | 35 (63) | n.a. | |
| Current smoker | 45 | 35 (29) | 10 (18) | 1 λ | |
| Ex-smoker | 10 | 6 (5) | 4 (7) | 0.43 (0.11–1.60) | 0.21 |
| Never smoked | 20 | 13 (11) | 7 (12) | 0.53 (0.13–2.13) | 0.37 |
| TOTAL | 121 (100) | 56 (100) | |||
| Reason for Presentation, by Consultation (n = 579): | n (%) |
|---|---|
| Requesting pregnancy test | 163 (28) |
| Requesting cessation of contraception | 135 (23) |
| Unwell or other unrelated health concern | 114 (20) |
| Preconception care | 70 (12) |
| Sexual health | 30 (5) |
| Chronic disease management or scheduled health check | 29 (5) |
| Multiple reasons | 21 (4) |
| Requesting check-up | 17 (3) |
| Designation of staff member/s, by consultation (n = 579): | |
| Nurse or Aboriginal health worker only | 343 (59) |
| General practitioner * and nurse or Aboriginal health worker | 111 (19) |
| General practitioner * only | 98 (17) |
| Midwife | 22 (4) |
| Other | 5 (1) |
| Components of care delivered, by pregnancy (n = 121) **: | |
| Sexually transmissible infections | 86 (71) |
| Folic acid | 69 (57) |
| Smoking cessation and avoidance | 52 (43) |
| Nutrition and weight | 44 (36) |
| Alcohol and illicit substances | 31 (26) |
| Chronic disease management | 20 (17) |
| Vaccinations | 14 (12) |
| Year | Pregnancies, Total (n) | “Received PCC” Pregnancies (n (%)) | Of Those Receiving Care: Components of PCC Delivered, by Pregnancy (Median) | ||
|---|---|---|---|---|---|
| Number of Key Components ** | Number of Times *** | Number of Consultations | |||
| 2011 | 13 | 8 (53) | 2.5 | 3 | 2.5 |
| 2012 | 29 | 18 (58) | 1 | 1 | 3 |
| 2013 | 26 | 17 (52) | 3 | 3 | 3 |
| 2014 | 22 | 13 (57) | 2 | 3 | 2 |
| 2015 | 37 | 24 (60) | 3 | 4 | 4 |
| 2016 | 18 | 14 (74) | 3 | 4 | 3.5 |
| 2017 | 23 | 18 (70) | 3.5 | 5.5 | 5.5 |
| 2018 | 11 * | 9 (75) | 4 | 7 | 5 |
| Total | 177 | 121 (100) | |||
| p# | 0.105 | 0.044 | 0.003 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffiths, E.; Marley, J.V.; Atkinson, D. Preconception Care in a Remote Aboriginal Community Context: What, When and by Whom? Int. J. Environ. Res. Public Health 2020, 17, 3702. https://doi.org/10.3390/ijerph17103702
Griffiths E, Marley JV, Atkinson D. Preconception Care in a Remote Aboriginal Community Context: What, When and by Whom? International Journal of Environmental Research and Public Health. 2020; 17(10):3702. https://doi.org/10.3390/ijerph17103702
Chicago/Turabian StyleGriffiths, Emma, Julia V Marley, and David Atkinson. 2020. "Preconception Care in a Remote Aboriginal Community Context: What, When and by Whom?" International Journal of Environmental Research and Public Health 17, no. 10: 3702. https://doi.org/10.3390/ijerph17103702
APA StyleGriffiths, E., Marley, J. V., & Atkinson, D. (2020). Preconception Care in a Remote Aboriginal Community Context: What, When and by Whom? International Journal of Environmental Research and Public Health, 17(10), 3702. https://doi.org/10.3390/ijerph17103702