Initial Therapy, Regimen Change, and Persistence in a Spanish Cohort of Newly Treated Type 2 Diabetes Patients: A Retrospective, Observational Study Using Real-World Data

 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
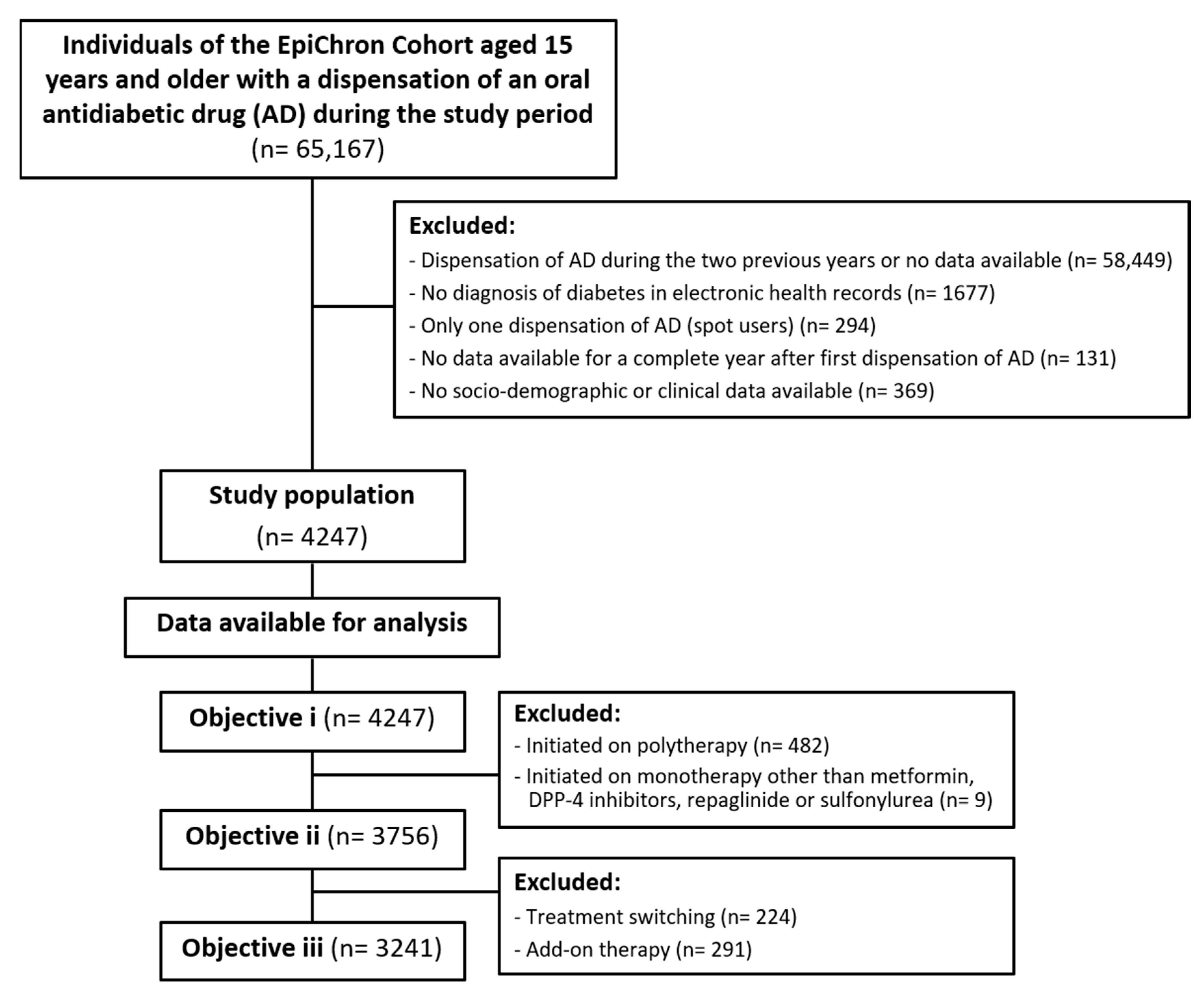
2.1. Study Design and Population
2.2. Study Variables and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Population and Antidiabetic Therapy
3.2. Changes in Therapy Regimen
3.3. Medication Persistence
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014; p. 176. [Google Scholar]
- Magliano, D.J.; Islam, R.M.; Barr, E.L.M.; Gregg, E.W.; Pavkov, M.E.; Harding, J.L.; Tabesh, M.; Koye, D.N.; Shaw, J.E. Trends in incidence of total or type 2 diabetes: Systematic review. BMJ 2019, 366, l5003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.; Lu, Y.; Hajifathalian, K.; Bentham, J.; Di Cesare, M.; Danaei, G.; Bixby, H.; Cowan, M.; Ali, M.; Taddei, C.; et al. Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4•4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef] [Green Version]
- Kolb, H.; Martin, S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- International Diabetes Federation Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017; Available online: http://www.diabetesatlas.org (accessed on 2 February 2020).
- Moulis, G.; Ibañez, B.; Palmaro, A.; Aizpuru, F.; Millan, E.; Lapeyre-Mestre, M.; Sailler, L.; Cambra, K. Cross-national health care database utilization between Spain and France: Results from the Epichronic study assessing the prevalence of type 2 diabetes mellitus. Clin. Epidemiol. 2018, 10, 863–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The [email protected] Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; p. 86. [Google Scholar]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.; McDonald, H.; Garg, A.; Montague, P. Interventions for helping patients to follow prescriptions for medications. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2002; p. CD000011. [Google Scholar]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2015; Available online: https://www.who.int/chp/knowledge/publications/adherence_report/en/ (accessed on 20 February 2020).
- Cramer, J.A.; Roy, A.; Burrell, A.; Fairchild, C.J.; Fuldeore, M.J.; Ollendorf, D.A.; Wong, P.K. Medication Compliance and Persistence: Terminology and Definitions. Value Health 2008, 11, 44–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manteuffel, M.; Williams, S.; Chen, W.; Verbrugge, R.R.; Pittman, D.G.; Steinkellner, A. Influence of Patient Sex and Gender on Medication Use, Adherence, and Prescribing Alignment with Guidelines. J. Women’s Health 2014, 23, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Marinho, F.S.; Moram, C.B.M.; Rodrigues, P.C.; Leite, N.C.; Salles, G.F.; Cardoso, C.R.L. Treatment Adherence and Its Associated Factors in Patients with Type 2 Diabetes: Results from the Rio de Janeiro Type 2 Diabetes Cohort Study. J. Diabetes Res. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- McGovern, A.; Tippu, Z.; Hinton, W.; Munro, N.; Whyte, M.; de Lusignan, S. Systematic review of adherence rates by medication class in type 2 diabetes: A study protocol. BMJ Open 2016, 6, e010469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horii, T.; Iwasawa, M.; Kabeya, Y.; Atuda, K. Polypharmacy and oral antidiabetic treatment for type 2 diabetes characterised by drug class and patient characteristics: A Japanese database analysis. Sci. Rep. 2019, 9, 12992. [Google Scholar] [CrossRef] [PubMed]
- Aga, F.; Dunbar, S.B.; Kebede, T.; Gary, R. The role of concordant and discordant comorbidities on performance of self-care behaviors in adults with type 2 diabetes: A systematic review. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 333–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, C.J.; Kodack, M. Patient adherence to medication requirements for therapy of type 2 diabetes. Int. J. Clin. Pract. 2011, 65, 314–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno Juste, A.; Menditto, E.; Orlando, V.; Monetti, V.M.; Gimeno Miguel, A.; González Rubio, F.; Aza–Pascual-Salcedo, M.M.; Cahir, C.; Prados Torres, A.; Riccardi, G. Treatment Patterns of Diabetes in Italy: A Population-Based Study. Front. Pharmacol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Aguadé, A.S.; Gastaldi-Ménager, C.; Karsenty, D.; Fontaine, P.; Fagot-Campagna, A. Type 2 diabetes: Changing patterns of use of antidiabetic drugs 8 years after starting treatment (snds). Eur. J. Public Health 2019, 29. [Google Scholar]
- Datta-Nemdharry, P.; Thomson, A.; Beynon, J.; Donegan, K. Patterns of anti-diabetic medication use in patients with type 2 diabetes mellitus in England and Wales. Pharmacoepidemiol. Drug Saf. 2017, 26, 127–135. [Google Scholar] [CrossRef]
- Impact of New Antidiabetic Drugs on the Treatment of Type 2 Diabetes and Patients Safety: A Pharmacoepidemiological Challenge. Available online: https://refbio.eu/en/projets/epichronic-ii/./ (accessed on 21 March 2020).
- Prados-Torres, A.; Poblador-Plou, B.; Gimeno-Miguel, A.; Calderón-Larrañaga, A.; Poncel-Falcó, A.; Gimeno-Feliú, L.A.; González-Rubio, F.; Laguna-Berna, C.; Marta-Moreno, J.; Clerencia-Sierra, M.; et al. Cohort Profile: The Epidemiology of Chronic Diseases and Multimorbidity. The EpiChron Cohort Study. Int. J. Epidemiol. 2018, 47, 382f–384f. [Google Scholar]
- Orlando, V.; Guerriero, F.; Putignano, D.; Monetti, V.M.; Tari, D.U.; Farina, G.; Illario, M.; Iaccarino, G.; Menditto, E. Prescription patterns of antidiabetic treatment in the elderly. Results from Southern Italy. Curr. Diabetes Rev. 2016, 12, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Compés Dea, M.L.; Olivan Bellido, E.; Feja Solana, C.; Aguilar Palacio, I.; García-Carpintero Romero del Hombrebueno, G.; Adiego Sancho, B. Construction of a deprivation index by Basic Healthcare Area in Aragon using Population and Housing Census 2011. Rev. Esp. Salud Publica 2018, 92, 1–17. [Google Scholar]
- The Johns Hopkins University Johns Hopkins ACG® System. Available online: https://www.hopkinsacg.org/ (accessed on 14 March 2020).
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2011, 61, e12–e21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Chronic Respiratory Diseases. Allergic Rhinitis and Sinusitis; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Yeaw, J.; Benner, J.S.; Walt, J.G.; Sian, S.; Smith, D.B. Comparing adherence and persistence across 6 chronic medication classes. J. Manag. Care Pharm. 2009, 15, 728–740. [Google Scholar] [CrossRef] [PubMed]
- Giorgino, F.; Penfornis, A.; Pechtner, V.; Gentilella, R.; Corcos, A. Adherence to antihyperglycemic medications and glucagon-like peptide 1-receptor agonists in type 2 diabetes: Clinical consequences and strategies for improvement. Patient Prefer. Adherence 2018, 12, 707–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderten, H.; Dippel, F.W.; Kostev, K. Early discontinuation and related treatment costs after initiation of basal insulin in type 2 diabetes patients: A German primary care database analysis. J. Diabetes Sci. Technol. 2015, 9, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, J.; Divino, V.; Burudpakdee, C. Adherence and persistence in patients with type 2 diabetes mellitus newly initiating canagliflozin, dapagliflozin, DPP–4s, or GLP–1s in the United States. Curr. Med. Res. Opin. 2017, 33, 1317–1328. [Google Scholar] [CrossRef]
- Kardas, P.; Lewek, P.; Matyjaszczyk, M. Determinants of patient adherence: A review of systematic reviews. Front. Pharmacol. 2013, 4, 91. [Google Scholar] [CrossRef] [Green Version]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015, 38, 140–149. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 8. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes–2018. Diabetes Care 2018, 41, S73–S85. [Google Scholar] [CrossRef] [Green Version]
- Jaffiol, C. Current management of type 2 diabetes in France. Bull. Acad. Natl. Med. 2009, 193, 1645–1661. [Google Scholar]
- Morita, Y.; Murayama, H.; Odawara, M.; Bauer, M. Treatment patterns of drug-naive patients with type 2 diabetes mellitus: A retrospective cohort study using a Japanese hospital database. Diabetol. Metab. Syndr. 2019, 11, 90. [Google Scholar] [CrossRef] [Green Version]
- The National Institute for Health and Care Excellence. Type 2 Diabetes in Adults: Management NICE Guideline; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- FDA Drug Safety Communication: FDA Revises Warnings Regarding Use of the Diabetes Medicine Metformin in Certain Patients with Reduced Kidney Function. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-revises-warnings-regarding-use-diabetes-medicine-metformin-certain (accessed on 9 May 2020).
- Use of Metformin to Treat Diabetes Now Expanded to Patients with Moderately Reduced Kidney Function; EMA/603690/2016; European Medicines Agency: London, UK, 2016; Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Referrals_docu (accessed on 6 April 2020).
- Huelgas, R.G.; Gómez-Huelgas, R.; Martínez-Castelao, A.; Artola, S.; Górriz, J.L.; Javier, J.; Bravo, M. Consensus Document on treatment of type 2 diabetes in patients with chronic kidney disease. Nefrología 2014, 34, 34–45. [Google Scholar]
- Grimes, R.T.; Bennett, K.; Tilson, L.; Usher, C.; Smith, S.M.; Henman, M.C. Initial therapy, persistence and regimen change in a cohort of newly treated type 2 diabetes patients. Br. J. Clin. Pharmacol. 2015, 79, 1000–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregoire, J.P.; Sirois, C.; Perez, N.; Demers, E.; Moisan, J. Persistence patterns with oral anti-hypergilycemic drug treatment in newly treated patients - A population-based study. Value Health 2010, 13, 810–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overbeek, J.A.; Heintjes, E.M.; Prieto-Alhambra, D.; Blin, P.; Lassalle, R.; Hall, G.C.; Lapi, F.; Bianchini, E.; Hammar, N.; Bezemer, I.D.; et al. Type 2 Diabetes Mellitus Treatment Patterns Across Europe: A Population-based Multi-database Study. Clin. Ther. 2017, 39, 759–770. [Google Scholar] [CrossRef]
- Noh, Y.; Lee, S.; Shin, S. Durability of initial antidiabetic monotherapy and subsequent treatment adjustment patterns among newly treated type 2 diabetes patients. Ther. Clin. Risk Manag. 2018, 14, 1563–1571. [Google Scholar] [CrossRef] [Green Version]
- Iglay, K.; Cartier, S.E.; Rosen, V.M.; Zarotsky, V.; Rajpathak, S.N.; Radican, L.; Tunceli, K. Meta-analysis of studies examining medication adherence, persistence, and discontinuation of oral antihyperglycemic agents in type 2 diabetes. Curr. Med. Res. Opin. 2015, 31, 1283–1296. [Google Scholar] [CrossRef]
- Guénette, L.; Moisan, J.; Breton, M.C.; Sirois, C.; Grégoire, J.P. Difficulty adhering to antidiabetic treatment: Factors associated with persistence and compliance. Diabetes Metab. 2013, 39, 250–257. [Google Scholar] [CrossRef]
- Nishimura, R.; Kato, H.; Kisanuki, K.; Oh, A.; Hiroi, S.; Onishi, Y.; Guelfucci, F.; Shimasaki, Y. Treatment patterns, persistence and adherence rates in patients with type 2 diabetes mellitus in Japan: A claims-based cohort study. BMJ Open 2019, 9, e025806. [Google Scholar] [CrossRef] [Green Version]
- Kadowaki, T.; Sarai, N.; Hirakawa, T.M.; Taki, K.; Iwasaki MBA, K.; Urushihara DrPH, H.; Co, I.; Lilly Japan, E.K. Persistence of oral antidiabetic treatment for type 2 diabetes characterized by drug class, patient characteristics, and severity of renal impairment: A Japanese database analysis. Diabetes Obes. Metab. 2018, 20, 2830–2839. [Google Scholar] [CrossRef]
- Moreno Juste, A.; Gimeno Miguel, A.; Poblador Plou, B.; González Rubio, F.; Aza Pascual-Salcedo, M.M.; Menditto, E.; Prados Torres, A. Adherence to treatment of hypertension, hypercholesterolaemia and diabetes in an elderly population of a Spanish cohort. Med. Clin. (Barc). 2019, 153, 1–5. [Google Scholar] [CrossRef] [Green Version]
- O’Shea, M.P.; Teeling, M. Bennet An observational study examining the effect of comorbidity on the rates of persistence and adherence to newly initiated oral anti-hyperglycaemic agents. Pharmacoepidemiol. Drug Saf. 2013, 22, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- Menditto, E.; Cahir, C.; Aza-Pascual-Salcedo, M.; Bruzzese, D.; Poblador-Plou, B.; Malo-Fumanal, S.; Costa, E.; González-Rubio, F.; Orlando, V.; Gimeno-Miguel, A.; et al. Adherence to chronic medication in older populations: Application of a common protocol among three European cohorts. Patient Prefer. Adherence 2018, 12, 1975–1987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rozenfeld, Y.; Hunt, J.S.; Plauschinat, C.; Wong, K.S. Oral antidiabetic medication adherence and glycemic control in managed care. Am. J. Manag. Care 2008, 14, 71–75. [Google Scholar] [PubMed]
- Simard, P.; Presse, N.; Roy, L.; Dorais, M.; White-Guay, B.; Räkel, A.; Perreault, S. Persistence and adherence to oral antidiabetics: A population-based cohort study. Acta Diabetol. 2015, 52, 547–556. [Google Scholar] [CrossRef] [PubMed]
- DenBraver, N.R.; Lakerveld, J.; Rutters, F.; Schoonmade, L.J.; Brug, J.; Beulens, J.W.J. Built environmental characteristics and diabetes: A systematic review and meta-analysis. BMC Med. 2018, 16, 12. [Google Scholar]
- Jermendy, G.; Wittmann, I.; Nagy, L.; Kiss, Z.; Rokszin, G.; Abonyi-Tóth, Z.; Katona, L.; Paragh, G.; Karádi, I.; Merkely, B. Persistence of initial oral antidiabetic treatment in patients with type 2 diabetes mellitus. Med. Sci. Monit. 2012, 18, 72–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Monotherapy | Combination Therapy | Total | p-Value c | |||||
|---|---|---|---|---|---|---|---|---|---|
| Metformin | DPP-4i a | Repaglinide | Sulfonylureas | Other b | Fixed | Free | |||
| N (%) | 3420 (80.5%) | 221 (5.2%) | 65 (1.5%) | 50 (1.2%) | 9 (0.2%) | 354 (8.3%) | 128 (3.0%) | 4247 (100%) | |
| Age (years) | |||||||||
| Mean ± SD d | 64.2 ± 12.6 | 71.6 ± 13.3 | 72.9 ± 11.8 | 71.6 ± 14.3 | 77.6 ± 5.9 | 61.6 ± 12.5 | 64.2 ± 11.8 | 64.6 ± 12.8 | <0.001 |
| Age interval (n, %) | |||||||||
| 15–39 | 99 (85.3%) | 5 (4.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 10 (8.6%) | 2 (1.7%) | 116 (100%) | |
| 40–59 | 1135 (81.6%) | 35 (2.5%) | 14 (1.0%) | 12 (0.9%) | 0 (0.0%) | 152 (10.9%) | 43 (3.1%) | 1391 (100%) | |
| 60–79 | 1750 (82.3%) | 103 (4.8%) | 27 (1.3%) | 18 (0.9%) | 6 (0.3%) | 158 (7.4%) | 64 (3.0%) | 2126 (100%) | |
| ≥80 | 436 (71.0%) | 78 (12.7%) | 24 (3.9%) | 20 (3.3%) | 3 (0.5%) | 34 (5.5%) | 19 (3.1%) | 614 (100%) | |
| Gender (n, %) | 0.079 | ||||||||
| Women | 1468 (81.5%) | 101 (5.6%) | 33 (1.8%) | 20 (1.1%) | 5 (0.3%) | 128 (7.1%) | 47 (2.6%) | 1802 (100%) | |
| Men | 1952 (79.8%) | 120 (4.9%) | 32 (1.3%) | 30 (1.2%) | 4 (0.2%) | 226 (9.2%) | 81 (3.3%) | 2445 (100%) | |
| Residence area (n, %) | 0.008 | ||||||||
| Urban | 2027 (81.5%) | 140 (5.6%) | 31 (1.3%) | 34 (1.4%) | 4 (0.2%) | 190 (7.6%) | 62 (2.5%) | 2488 (100%) | |
| Rural | 1393 (79.2%) | 81 (4.6%) | 34 (1.9%) | 16 (0.9%) | 5 (0.3%) | 164 (9.3%) | 66 (3.8%) | 1759 (100%) | |
| Depriv. index e (n, %) | 0.295 | ||||||||
| Q1 | 798 (79.5%) | 56 (5.6%) | 16 (1.6%) | 15 (1.5%) | 2 (0.2%) | 83 (8.3%) | 34 (3.4%) | 1004 (100%) | |
| Q2 | 893 (83.1%) | 56 (5.2%) | 17 (1.6%) | 6 (0.6%) | 3 (0.3%) | 68 (6.3%) | 32 (3.0%) | 1075 (100%) | |
| Q3 | 692 (78.6%) | 48 (5.5%) | 18 (2.1%) | 11 (1.3%) | 1 (0.1%) | 81 (9.2%) | 29 (3.3%) | 880 (100%) | |
| Q4 | 1037 (80.5%) | 61 (4.7%) | 14 (1.1%) | 18 (1.4%) | 3 (0.2%) | 122 (9.5%) | 33 (2.6%) | 1288 (100%) | |
| Immigrant status (n, %) | 0.025 | ||||||||
| Native | 3266 (80.7%) | 214 (5.3%) | 63 (1.6%) | 48 (1.2%) | 9 (0.2%) | 331 (8.2%) | 115 (2.8%) | 4046 (100%) | |
| Immigrant | 154 (76.6%) | 7 (3.5%) | 2 (1.0%) | 2 (1.0%) | 0 (0.0%) | 23 (11.4%) | 13 (6.5%) | 201 (100%) | |
| Concomitant drugs | |||||||||
| Mean ± SD | 6.2 ± 4.2 | 8.2 ± 4.7 | 8.1 ± 5.4 | 5.9 ± 4.1 | 5.9 ± 3.1 | 5.1 ± 4.6 | 4.5 ± 4.6 | 6.2 ± 4.4 | <0.001 |
| 0–5 | 1661 (79.8%) | 65 (3.1%) | 25 (1.2%) | 29 (1.4%) | 4 (0.2%) | 218 (10.5%) | 80 (3.8%) | 2082 (100%) | |
| 6–9 | 1051 (83.8%) | 75 (6.0%) | 13 (1.0%) | 8 (0.6%) | 3 (0.2%) | 72 (5.7%) | 33 (2.6%) | 1255 (100%) | |
| ≥10 | 708 (77.8%) | 81 (8.9%) | 27 (3.0%) | 13 (1.4%) | 2 (0.2%) | 64 (7.0%) | 15 (1.7%) | 910 (100%) | |
| Comorbidities | |||||||||
| Mean ± SD | 3.9 ± 2.6 | 5.1 ± 3.1 | 5.1 ± 4.0 | 4.0 ± 2.5 | 3.4 ± 1.7 | 3.3 ± 3.0 | 3.0 ± 2.4 | 3.9 ± 2.7 | <0.001 |
| 0 | 199 (73.4%) | 6 (2.2%) | 4 (1.5%) | 3 (1.1%) | 0 (0.0%) | 45 (16.6%) | 14 (5.2%) | 271 (100%) | |
| 1–4 | 2046 (81.2%) | 98 (3.9%) | 33 (1.3%) | 29 (1.2%) | 7 (0.3%) | 218 (8.7%) | 88 (3.5%) | 2519 (100%) | |
| ≥5 | 1175 (80.7%) | 117 (8.0%) | 28 (1.9%) | 18 (1.2%) | 2 (0.1%) | 91 (6.3%) | 26 (1.8%) | 1457 (100%) | |
| Chronic renal failure | <0.001 | ||||||||
| No | 3297 (82.2%) | 166 (4.1%) | 44 (1.1%) | 39 (1.0%) | 8 (0.2%) | 335 (8.4%) | 120 (3.0%) | 4009 (100%) | |
| Yes | 123 (51.7%) | 55 (23.1%) | 21 (8.8%) | 11 (4.6%) | 1 (0.4%) | 19 (8.0%) | 8 (3.4%) | 238 (100%) | |
| Initial Therapy | Total | Type of Treatment Switching/Add-On Therapy (n, % b) | ||||||
|---|---|---|---|---|---|---|---|---|
| (n, % a) | Metformin | DPP-4i c | Repaglinide | Sulfonylureas | Other d | Polytherapy | Insulin | |
| Total (n = 3756) | ||||||||
| Switchers | 224 (6.0) | 9 (4.0) | 128 (57.1) | 25 (11.2) | 47 (20.8) | 1 (0.4) | 9 (4.0) | 5 (2.2) |
| Add-on | 291 (7.7) | 25 (8.6) | 204 (70.1) | 17 (5.8) | 16 (5.5) | 3 (1.0) | 6 (2.1) | 20 (6.9) |
| Metformin (n = 3420) | ||||||||
| Switchers | 200 (5.8) | - | 127 (63.5) | 21 (10.5) | 43 (21.5) | 1 (0.5) | 5 (2.5) | 3 (1.5) |
| Add-on | 256 (7.5) | - | 204 (79.7) | 12 (4.7) | 16 (6.3) | 2 (0.8) | 5 (2.0) | 17 (6.6) |
| DPP-4i (n = 221) | ||||||||
| Switchers | 16 (7.2) | 7 (43.8) | - | 4 (25.0) | 4 (25.0) | 0 (0.0) | 1 (6.3) | 0 (0.0) |
| Add-on | 29 (13.1) | 22 (75.9) | - | 5 (17.2) | 0 (0.0) | 1 (3.5) | 0 (0.0) | 1 (3.5) |
| Repaglinide (n = 65) | ||||||||
| Switchers | 5 (7.7) | 1 (20.0) | 1 (20.0) | - | 0 (0.0) | 0 (0.0) | 1 (20.0) | 2 (40.0) |
| Add-on | 6 (9.2) | 3 (50.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (16.7) | 2 (33.3) | |
| Sulfonylurea (n = 50) | ||||||||
| Switchers | 3 (6.0) | 1 (33.3) | 0 (0.0) | 0 (0.0) | - | 0 (0.0) | 2 (66.7) | 0 (0.0) |
| Add-on | 0 (0.0) | - | - | - | - | - | - | - |
| Initial Monotherapy Treatment | ||||||
|---|---|---|---|---|---|---|
| Metformin | DPP-4i a | Repaglinide | Sulfonylureas | Total | p-Value b | |
| Frequency (N, %) | 0.068 | |||||
| Persistence | 2038 (68.8%) | 135 (76.7%) | 33 (61.1%) | 30 (63.8%) | 2236 (69.0%) | |
| Discontinuation | 926 (31.2%) | 41 (23.3%) | 21 (38.9%) | 17 (36.2%) | 1005 (31.0%) | |
| Days to (median, IQR c) | ||||||
| Discontinuation | 108 (25–206) | 79 (57–195) | 133 (30–226) | 150 (62–231) | 108 (25–206) | 0.507 |
| Switching | 55 (21–140) | 98.5 (33–195) | 6 (3–15) | 25 (2–73) | 55 (21–145) | 0.054 |
| Add-on | 84 (39–199) | 159 (76–217) | 31.5 (20–38) | - | 85 (40–200) | 0.025 |
| Variables | Crude HR a (95% CI) | p-Value | Adjusted HR b (95% CI) | p-Value c |
|---|---|---|---|---|
| Age (years) | ||||
| 15–39 | Reference | Reference | ||
| 40–59 | 0.59 (0.43–0.81) | 0.001 | 0.63 (0.46–0.86) | 0.004 |
| 60–79 | 0.49 (0.36–0.67) | <0.001 | 0.53 (0.38–0.72) | <0.001 |
| ≥80 | 0.50 (0.36–0.71) | <0.001 | 0.55 (0.39–0.78) | 0.001 |
| Gender | ||||
| Men | Reference | Reference | ||
| Women | 1.10 (0.97–1.24) | 0.138 | 1.14 (1.00–1.29) | 0.053 |
| Area of living | ||||
| Urban | Reference | Reference | ||
| Rural | 0.77 (0.67–0.87) | <0.001 | 0.79 (0.69–0.90) | <0.001 |
| Deprivation index d | ||||
| Q1 | Reference | Reference | ||
| Q2 | 0.77 (0.65–0.91) | 0.003 | 0.79 (0.66–0.94) | 0.007 |
| Q3 | 0.78 (0.65–0.93) | 0.007 | 0.82 (0.68–0.98) | 0.031 |
| Q4 | 0.75 (0.64–0.89) | 0.001 | 0.77 (0.65–0.91) | 0.002 |
| Concomitant drugs | ||||
| 0–5 | Reference | Reference | ||
| 6–9 | 0.79 (0.68–0.91) | 0.001 | 0.84 (0.72–0.99) | 0.034 |
| ≥10 | 0.92 (0.78–1.08) | 0.295 | 1.03 (0.85–1.25) | 0.783 |
| Comorbidities | ||||
| 0 | Reference | Reference | ||
| 1–4 | 0.91 (0.70–1.19) | 0.503 | 1.02 (0.78–1.34) | 0.870 |
| ≥5 | 0.79 (0.60–1.05) | 0.103 | 0.92 (0.68–1.26) | 0.611 |
| Chronic renal failure | ||||
| No | Reference | Reference | ||
| Yes | 0.97 (0.73–1.28) | 0.804 | 1.08 (0.80–1.46) | 0.599 |
| Initial therapy | ||||
| Metformin | Reference | Reference | ||
| DPP-4i e | 0.72 (0.52–0.98) | 0.036 | 0.73 (0.53–1.00) | 0.052 |
| Repaglinide | 1.29 (0.84–1.99) | 0.242 | 1.32 (0.85–2.07) | 0.216 |
| Sulfonylureas | 1.16 (0.72–1.88) | 0.539 | 1.10 (0.68–1.80) | 0.698 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Juste, A.; Poblador-Plou, B.; Aza-Pascual-Salcedo, M.; González-Rubio, F.; Malo, S.; Librero López, J.; Pico-Soler, V.; Giménez Labrador, E.; Mucherino, S.; Orlando, V.; et al. Initial Therapy, Regimen Change, and Persistence in a Spanish Cohort of Newly Treated Type 2 Diabetes Patients: A Retrospective, Observational Study Using Real-World Data. Int. J. Environ. Res. Public Health 2020, 17, 3742. https://doi.org/10.3390/ijerph17103742
Moreno-Juste A, Poblador-Plou B, Aza-Pascual-Salcedo M, González-Rubio F, Malo S, Librero López J, Pico-Soler V, Giménez Labrador E, Mucherino S, Orlando V, et al. Initial Therapy, Regimen Change, and Persistence in a Spanish Cohort of Newly Treated Type 2 Diabetes Patients: A Retrospective, Observational Study Using Real-World Data. International Journal of Environmental Research and Public Health. 2020; 17(10):3742. https://doi.org/10.3390/ijerph17103742
Chicago/Turabian StyleMoreno-Juste, Aida, Beatriz Poblador-Plou, Mercedes Aza-Pascual-Salcedo, Francisca González-Rubio, Sara Malo, Julián Librero López, Victoria Pico-Soler, Eva Giménez Labrador, Sara Mucherino, Valentina Orlando, and et al. 2020. "Initial Therapy, Regimen Change, and Persistence in a Spanish Cohort of Newly Treated Type 2 Diabetes Patients: A Retrospective, Observational Study Using Real-World Data" International Journal of Environmental Research and Public Health 17, no. 10: 3742. https://doi.org/10.3390/ijerph17103742
APA StyleMoreno-Juste, A., Poblador-Plou, B., Aza-Pascual-Salcedo, M., González-Rubio, F., Malo, S., Librero López, J., Pico-Soler, V., Giménez Labrador, E., Mucherino, S., Orlando, V., Menditto, E., Prados-Torres, A., & Gimeno-Miguel, A. (2020). Initial Therapy, Regimen Change, and Persistence in a Spanish Cohort of Newly Treated Type 2 Diabetes Patients: A Retrospective, Observational Study Using Real-World Data. International Journal of Environmental Research and Public Health, 17(10), 3742. https://doi.org/10.3390/ijerph17103742