Changes in Provision of Psychotherapy in the Early Weeks of the COVID-19 Lockdown in Austria


Abstract
:1. Introduction
2. Methods
2.1. Description of Study Participants
2.2. Working Tool
2.3. Investigation Strategy
2.4. Statistics
3. Results
3.1. Results for the Total Sample
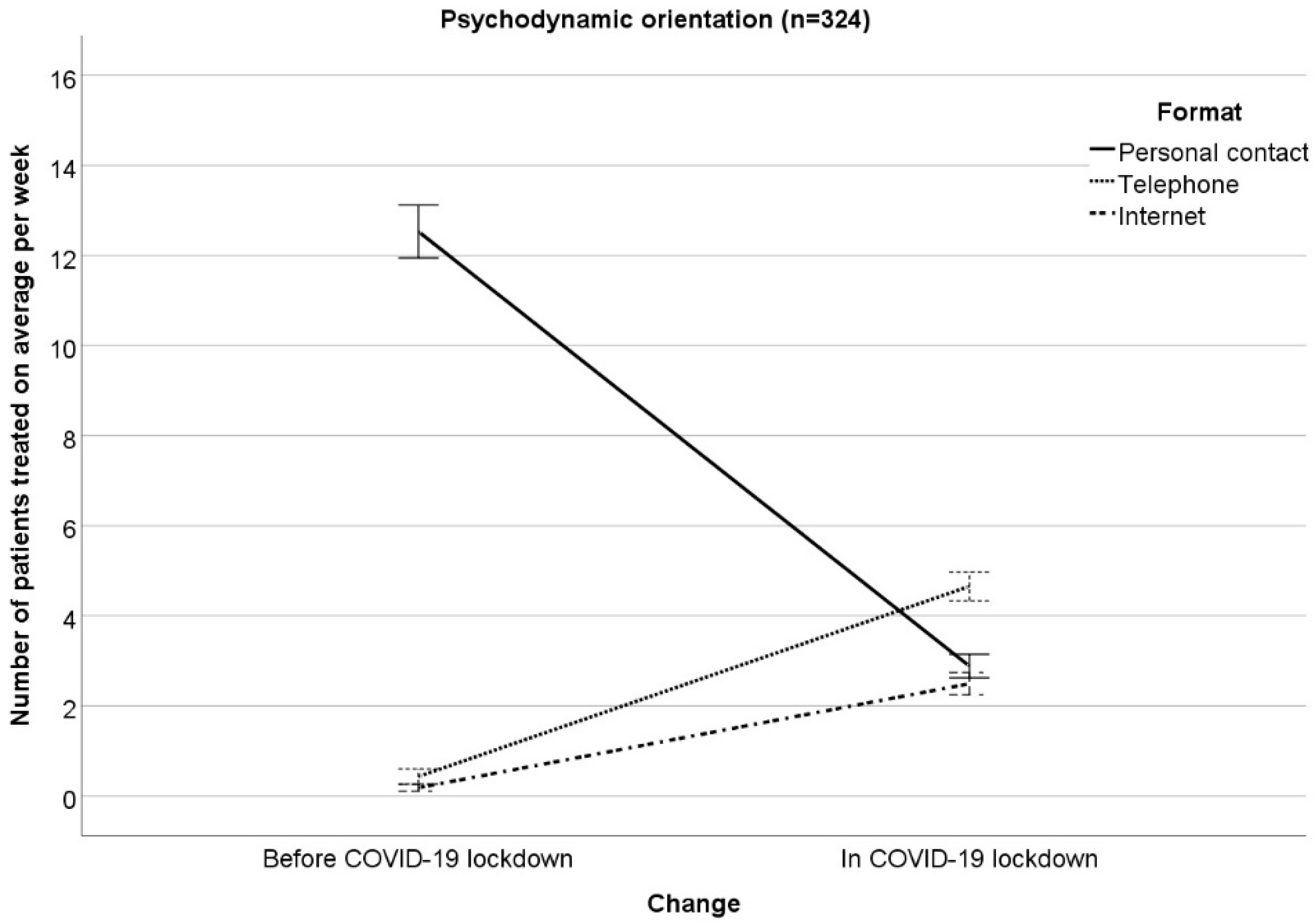
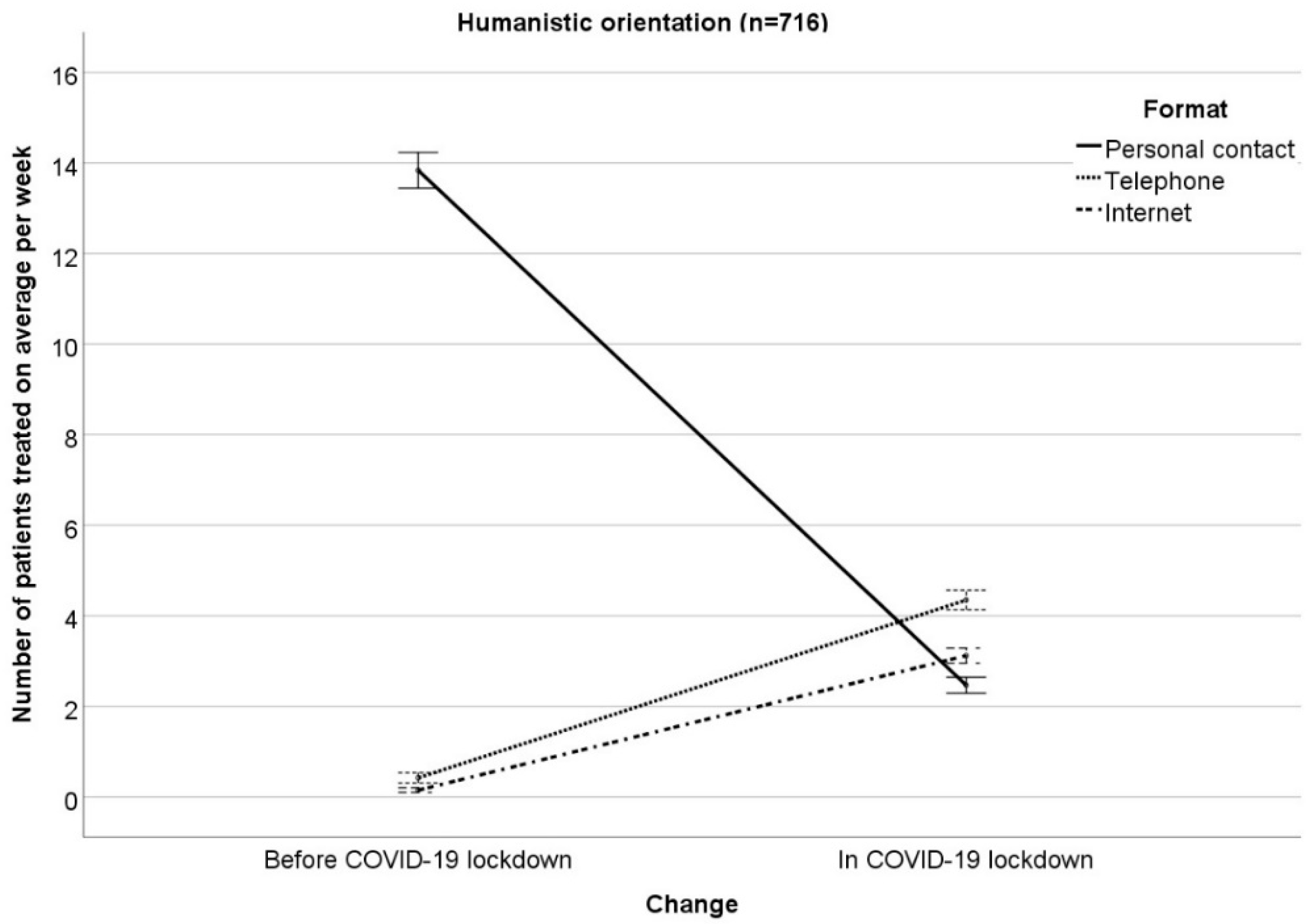
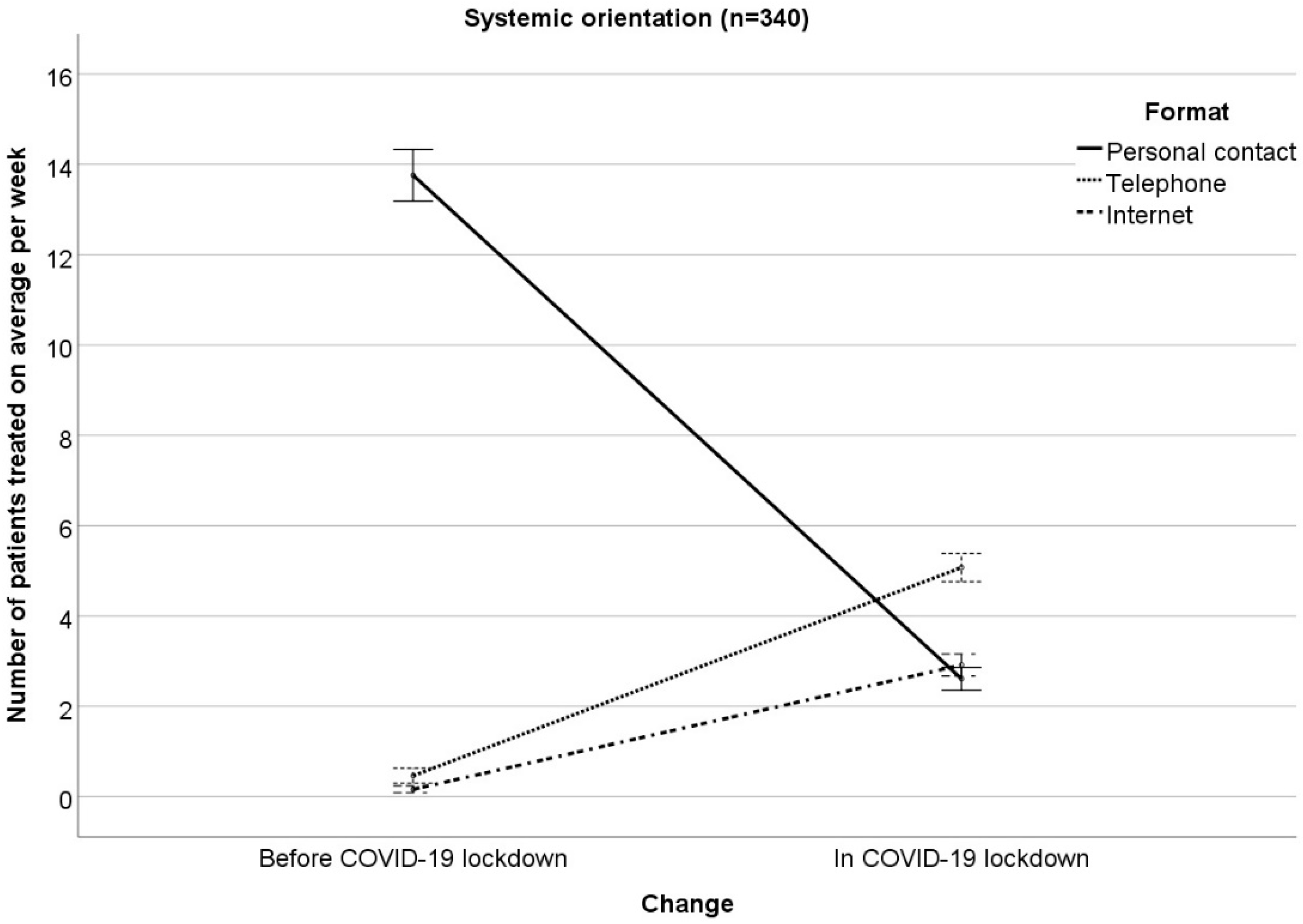
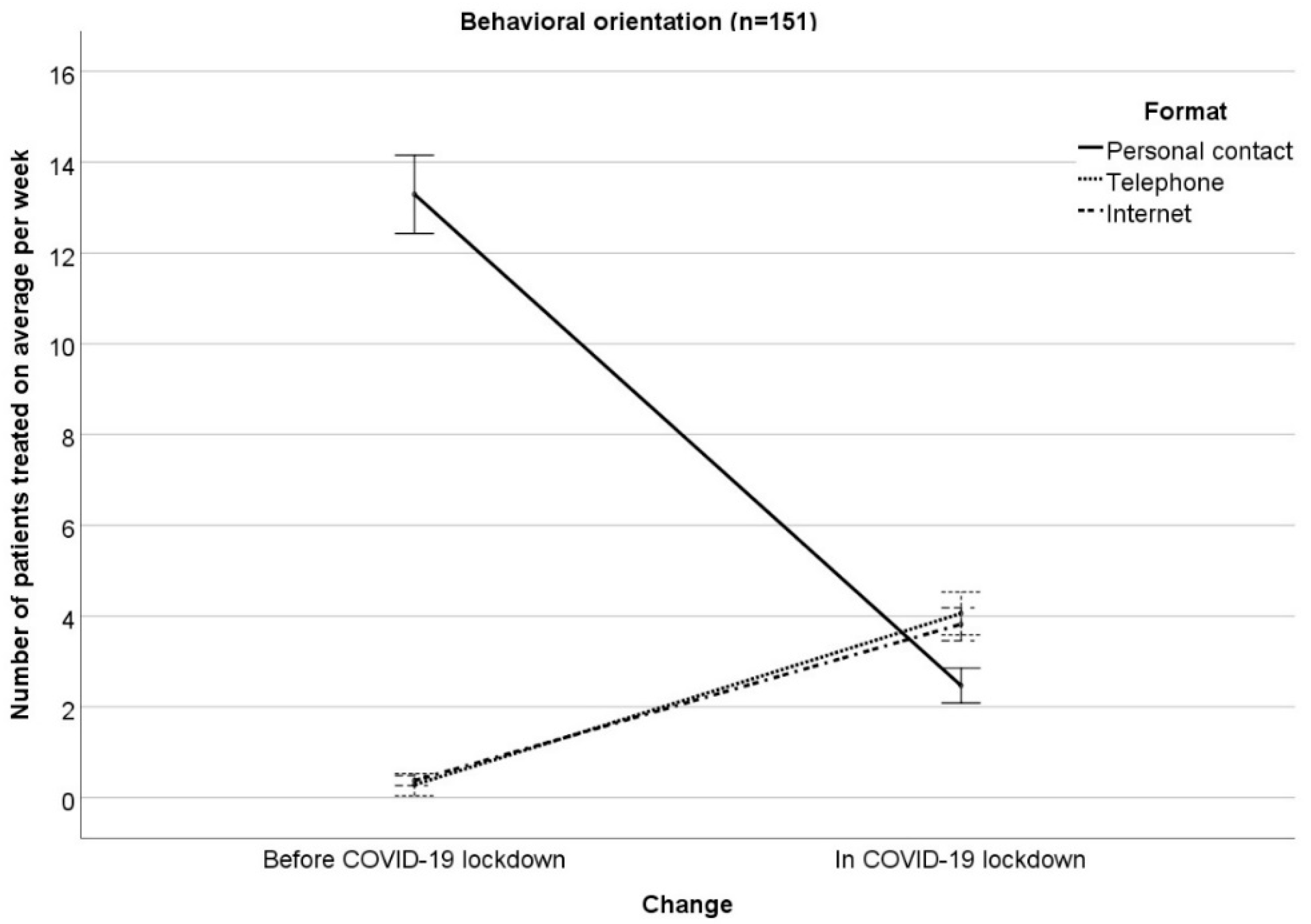
3.2. Results for the Four Therapeutic Orientations
- Months before COVID-19 lockdown: the number of patients treated on average per week was higher in personal contact vs. telephone (p < 0.001) and vs. Internet (p < 0.001). Furthermore, the number of patients treated on average per week was comparable for telephone and Internet (p = 0.151).
- In COVID-19 lockdown: the number of patients treated on average per week was lower in personal contact vs. telephone (p < 0.001) and vs. Internet (p < 0.026). Moreover, the number of patients treated on average per week was higher for telephone vs. Internet (p < 0.001).
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Christof, C.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 2020, CD013574. [Google Scholar] [CrossRef]
- Bundesgesetzblatt für die Republik Österreich. 98. Verordnung: Verordnung gemäß § 2 Z 1 des COVID-19-Maßnahmengesetzes. 2020. Available online: https://www.ris.bka.gv.at/Dokumente/BgblAuth/BGBLA_2020_II_98/BGBLA_2020_II_98.html (accessed on 25 May 2020).
- Bundesgesetzblatt für die Republik Österreich. 107. Verordnung: Änderung der Verordnung gemäß § 2 Z 1 des COVID-19-Maßnahmengesetzes. 2020. Available online: https://www.ris.bka.gv.at/Dokumente/BgblAuth/BGBLA_2020_II_107/BGBLA_2020_II_107.html (accessed on 25 May 2020).
- Bundesgesetzblatt für die Republik Österreich. 108. Verordnung: Änderung der Verordnung gemäß § 2 Z 1 des COVID-19-Maßnahmengesetzes. 2020. Available online: https://www.ris.bka.gv.at/Dokumente/BgblAuth/BGBLA_2020_II_108/BGBLA_2020_II_108.html (accessed on 25 May 2020).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Pillai, D.R.; Lu, M.; Doolan, C.; Leal, J.; Kim, J.; Hollis, A. Impact of isolation precautions on quality of life: A meta-analysis. J. Hosp. Infect. 2020, 105, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The impact of COVID-19 epidemic declaration on psychological consequences: A study on active weibo users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [Green Version]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Hapke, U.; Cohrdes, C.; Nübel, J. Depressive symptoms in a European comparison–Results from the European Health Interview Survey (EHIS) 2. J. Health Monit. 2019, 4, 57–65. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, physical activity, and relationship status on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020. (under review). [Google Scholar]
- Thombs, B.D.; Bonardi, O.; Rice, D.B.; Boruff, J.T.; Azar, M.; He, C.; Markham, S.; Sun, Y.; Wu, Y.; Krishnan, A.; et al. Curating evidence on mental health during COVID-19: A living systematic review. J. Psychosom. Res. 2020, 110113. [Google Scholar] [CrossRef]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Pfefferbaum, B.; North, C.S. Mental health and the Covid-19 pandemic. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Executive Summary. Policy Brief: COVID-19 and the Need for Action on Mental Health. 2020. Available online: https://www.un.org/sites/un2.un.org/files/un_policy_brief-covid_and_mental_health_final.pdf (accessed on 25 May 2020).
- Wright, J.H.; Caudill, R. Remote treatment delivery in response to the COVID-19 pandemic. Psychother. Psychosom. 2020, 89, 1. [Google Scholar] [CrossRef] [PubMed]
- Whaibeh, E.; Mahmoud, H.; Naal, H. Telemental health in the context of a pandemic: The COVID-19 experience. Curr. Treat. Opt. Psychiatry 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The role of telehealth in reducing the mental health burden from COVID-19. Telemed. J. E Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. REDCap Consortium. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Heidegger, K.-E. The Situation of Psychotherapy in Austria. 2017. Available online: https://www.europsyche.org/app/uploads/2019/05/Situation-Psychotherapy-in-Austria−2017−10−20.pdf (accessed on 25 May 2020).
- Bundesministerium für Gesundheit und Frauen. Internetrichtlinie für Psychotherapeutinnen und Psychotherapeuten. Psychother. Forum. 2005, 13, S43–S51. [Google Scholar]
- Schuster, R.; Pokorny, R.; Berger, T.; Topooco, N.; Laireiter, A.R. The advantages and disadvantages of online and blended therapy: Survey study amongst licensed psychotherapists in Austria. J. Med. Internet Res. 2018, 20, e11007. [Google Scholar] [CrossRef]
- Connolly, S.L.; Miller, C.J.; Lindsay, J.A.; Bauer, M.S. A systematic review of providers’ attitudes toward telemental health via videoconferencing. Clin. Psychol. 2020, e12311. [Google Scholar] [CrossRef]
- Schröder, J.; Berger, T.; Meyer, B.; Lutz, W.; Hautzinger, M.; Späth, C.; Eichenberg, C.; Klein, J.P.; Moritz, S. Attitudes towards Internet interventions among psychotherapists and individuals with mild to moderate depression symptoms. Cognit. Ther. Res. 2017, 41, 745–756. [Google Scholar] [CrossRef]
- Apolinário-Hagen, J.; Harrer, M.; Kählke, F.; Fritsche, L.; Salewski, C.; Ebert, D.D. Public attitudes toward guided Internet-based therapies: Web-based survey study. JMIR Ment. Health 2018, 5, e10735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backhaus, A.; Agha, Z.; Maglione, M.L.; Repp, A.; Ross, B.; Zuest, D.; Rice-Thorp, N.M.; Lohr, J.; Thorp, S.R. Videoconferencing psychotherapy: A systematic review. Psychol. Serv. 2012, 9, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.L.; Shannon, G.W.; Bashshur, N.; Yellowlees, P.M. The empirical evidence for telemedicine interventions in mental disorders. Telemed. J. E Health 2016, 22, 87–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins-Guarnieri, M.A.; Pruitt, L.D.; Luxton, D.D.; Johnson, K. Patient perceptions of telemental health: Systematic review of direct comparisons to in-person psychotherapeutic treatments. Telemed. J. E Health 2015, 21, 652–660. [Google Scholar] [CrossRef]
- Langarizadeh, M.; Tabatabaei, M.S.; Tavakol, K.; Naghipour, M.; Rostami, A.; Moghbeli, F. Telemental health care, an effective alternative to conventional mental care: A systematic review. Acta Inform. Med. 2017, 25, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.; Schwenk, S.; Schneck, C.D.; Griffin, R.J.; Mishkind, M.C. Technology-based mental health treatment and the impact on the therapeutic alliance. Curr. Psychiatry Rep. 2019, 21, 76. [Google Scholar] [CrossRef]
- Apolinário-Hagen, J.; Fritsche, L.; Bierhals, C.; Salewski, C. Improving attitudes toward e-mental health services in the general population via psychoeducational information material: A randomized controlled trial. Internet Interv. 2018, 12, 141–149. [Google Scholar] [CrossRef]
- Topooco, N.; Riper, H.; Araya, R.; Berking, M.; Brunn, M.; Chevreul, K.; Cieslak, R.; Ebert, D.D.; Etchmendy, E.; Herrero, R.; et al. E-COMPARED consortium. Attitudes towards digital treatment for depression: A European stakeholder survey. Internet Interv. 2017, 8, 1–9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Format | Orientation | Before COVID-19 M (SD) | In COVID-19 M (SD) | Statistics |
|---|---|---|---|---|
| Personal contact | Psychodynamic n = 324 | 12.53 (9.86) | 2.88 (4.86) | ME “change” F(1;1527) = 129.91; p < 0.001 IE “change x orientation” F(3;1527) = 1.21; p = 0.304 ME “format” F(1.75;2665.10) = 829.27; p < 0.001 IE “format x orientation” F(5.24;2665.10) = 1.24; p = 0.286 IE “change x format” F(1.42;2166.98) = 1231.43; p < 0.001 IE “change x format x orientation” F(4.26; 2166.98) = 2.19; p = 0.063 ME “orientation” F(3; 1527) = 0.63; p = 0.595 |
| Humanistic n = 716 | 13.84 (10.94) | 2.47 (4.50) | ||
| Systemic n = 340 | 13.76 (10.75) | 2.61 (4.87) | ||
| Behavioral n = 151 | 13.29 (9.82) | 2.47 (5.05) | ||
| Telephone | Psychodynamic n = 324 | 0.43 (2.24) | 4.65 (5.06) | |
| Humanistic n = 716 | 0.42 (3.85) | 4.35 (6.21) | ||
| Systemic n = 340 | 0.46 (2.22) | 5.07 (5.88) | ||
| Behavioral n = 151 | 0.28 (0.80) | 4.06 (4.83) | ||
| Internet | Psychodynamic n = 324 | 0.18 (1.02) | 2.49 (3.84) | |
| Humanistic n = 716 | 0.15 (0.94) | 3.12 (4.57) | ||
| Systemic n = 340 | 0.16 (0.66) | 2.91 (4.19) | ||
| Behavioral n = 151 | 0.38 (3.35) | 3.82 (5.49) | ||
| Total | Psychodynamic n = 324 | 13.14 (10.51) | 10.03 (8.44) | |
| Humanistic n = 716 | 14.41 (11.87) | 9.94 (9.17) | ||
| Systemic n = 340 | 14.38 (11.36) | 10.60 (9.41) | ||
| Behavioral n = 151 | 13.95 (10.33) | 10.35 (8.95) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Probst, T.; Stippl, P.; Pieh, C. Changes in Provision of Psychotherapy in the Early Weeks of the COVID-19 Lockdown in Austria. Int. J. Environ. Res. Public Health 2020, 17, 3815. https://doi.org/10.3390/ijerph17113815
Probst T, Stippl P, Pieh C. Changes in Provision of Psychotherapy in the Early Weeks of the COVID-19 Lockdown in Austria. International Journal of Environmental Research and Public Health. 2020; 17(11):3815. https://doi.org/10.3390/ijerph17113815
Chicago/Turabian StyleProbst, Thomas, Peter Stippl, and Christoph Pieh. 2020. "Changes in Provision of Psychotherapy in the Early Weeks of the COVID-19 Lockdown in Austria" International Journal of Environmental Research and Public Health 17, no. 11: 3815. https://doi.org/10.3390/ijerph17113815
APA StyleProbst, T., Stippl, P., & Pieh, C. (2020). Changes in Provision of Psychotherapy in the Early Weeks of the COVID-19 Lockdown in Austria. International Journal of Environmental Research and Public Health, 17(11), 3815. https://doi.org/10.3390/ijerph17113815