A Methodological Review of Mixed Methods Research in Palliative and End-of-Life Care (2014–2019)

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
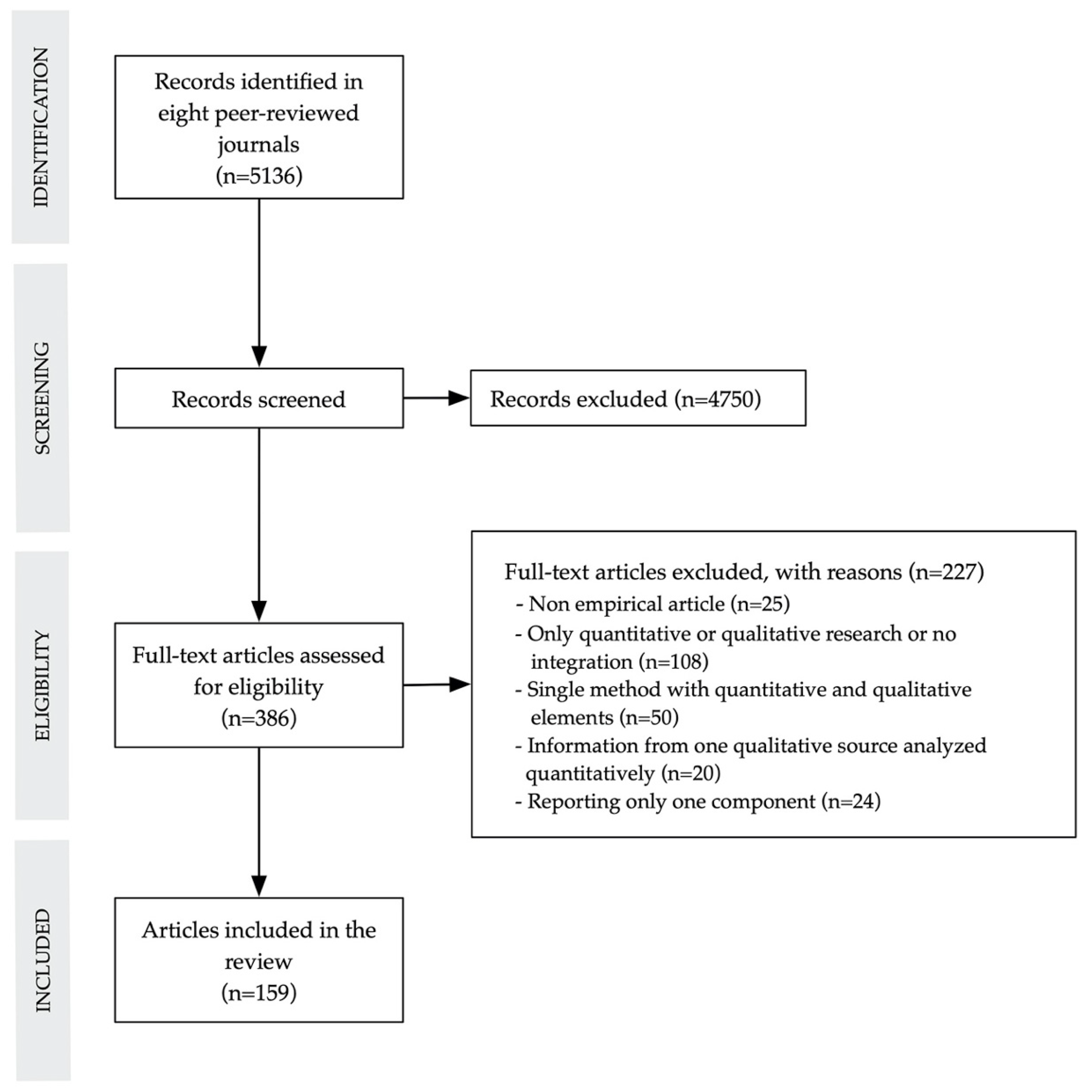
2.2. Study Selection
2.3. Screening and Eligibility Criteria
2.4. Data Extraction and Coding
3. Results
3.1. Characteristics of Articles Reporting Mixed Methods Studies
3.2. Reporting Quality and Mixed Methods Features
3.2.1. Justification for Using Mixed Methods Research
3.2.2. Mixed Methods Design
3.2.3. Quantitative and Qualitative Components
3.2.4. Integration
3.2.5. Limitations and Insights
3.3. Differences in Reporting Quality across Types of Mixed Methods Designs
4. Discussion
4.1. Main Findings
4.2. Implications for Future Research
4.3. Recommendations to Researchers
4.4. Recommendations to Editors
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Farquhar, M.C.; Ewing, G.; Booth, S. Using mixed methods to develop and evaluate complex interventions in palliative care research. Palliat. Med. 2011, 25, 748–757. [Google Scholar] [CrossRef]
- Walshe, C. Mixed method research in palliative care. In Textbook of Palliative Care; MacLeod, R., Block, V.D., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Fetters, M.D. The Mixed Methods Research Workbook: Activities for Designing, Implementing, and Publishing Projects; Sage: Thousand Oaks, CA, USA, 2020. [Google Scholar]
- Curry, L.; Nunez-Smith, M. Mixed Methods in Health Sciences Research; Sage: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Farquhar, M.C.; Preston, N.; Evans, C.J.; Grande, G.; Short, V.; Benalia, H.; Higginson, I.J.; Todd, C. Mixed methods research in the development and evaluation of complex interventions in palliative and end-of-life care: Report in the MORECare consensus exercise. J. Palliat. Med. 2013, 16, 1550–1560. [Google Scholar] [CrossRef] [Green Version]
- Flemming, K.; Adamson, J.; Atkin, K. Improving the effectiveness of interventions in palliative care: The potential role of qualitative research in enhancing evidence from randomized controlled trials. Palliat. Med. 2008, 22, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Seymour, J. Combined qualitative and quantitative research designs. Curr. Opin. Support. Palliat. Care 2012, 6, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Vedel, I.; El Sherif, R.; Pluye, P. Practical mixed methods strategies used to integrate qualitative and quantitative methods in community-based primary health care research. Fam. Pract. 2019, 36, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Pluye, P. A conceptual framework for critical appraisal in systematic mixed studies reviews. J. Mix. Methods Res. 2018, 13, 446–460. [Google Scholar] [CrossRef]
- Wisdom, J.P.; Cavaleri, M.A.; Onwuegbuzie, A.J.; Green, C.A. Methodological reporting in qualitative, quantitative, and mixed methods health services research articles. Health Serv. Res. 2012, 47, 721–745. [Google Scholar] [CrossRef]
- Bishop, F.L.; Holmes, M.M. Mixed methods in CAM research: A systematic review of studies published in 2012. Evid. Based Complement. Alternat. Med. 2013. [Google Scholar] [CrossRef] [Green Version]
- Granikov, V.; Hong, Q.N.; Crist, E.; Pluye, P. Mixed methods research in library and information science: A methodological review. Libr. Inf. Sci. Res. 2020, 42. [Google Scholar] [CrossRef]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef]
- Schreier, M. Qualitative Content Analysis in Practice; Sage: London, UK, 2012. [Google Scholar]
- Henoch, I.; Carlander, I.; Holm, M.; James, I.; Sarenmalm, E.K.; Hagelin, C.L.; Lind, S.; Sandgren, A.; Öhlén, J. Palliative Care Research—A systematic review of foci, designs and methods of research conducted in Sweden between 2007 and 2012. Scand. J. Caring Sci. 2016, 30, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Van den Hurk, D.G.; Schellekens, M.P.; Molema, J.; Speckens, A.E.; van der Drift, M.A. Mindfulness-based stress reduction for lung cancer patients and their partners: Results of a mixed methods pilot study. Palliat. Med. 2015, 29, 652–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Scoy, L.J.; Watson-Martin, E.; Bohr, T.A.; Levi, B.H.; Green, M.J. End-of-life conversation game increases confidence for having end-of-life conversations for chaplains-in-training. Am. J. Hosp. Palliat. Care 2018, 35, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Ankuda, C.K.; Kersting, K.; Guetterman, T.C.; Haefner, J.; Fonger, E.; Paletta, M.; Hopp, F. What matters most? A mixed methods study of critical aspects of a home-based palliative program. Am. J. Hosp. Palliat. Care 2018, 35, 236–243. [Google Scholar] [CrossRef]
- Plano Clark, V.L.; Ivankova, N.V. Mixed Methods Research: A Guide to the Field; Sage: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs—Principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [Green Version]
- Reese, D.J.; Beckwith, S.K. Organizational barriers to cultural competence in hospice. Am. J. Hosp. Palliat. Care 2015, 32, 685–694. [Google Scholar] [CrossRef]
- Kane, P.M.; Daveson, B.A.; Ryan, K.; Ellis-Smith, C.I.; Mahon, N.G.; McAdam, B.; McQuilllan, R.; Tracey, C.; Howley, C.; O’Gara, G.; et al. Feasibility and acceptability of a patient-reported outcome intervention in chronic heart failure. BMJ Support. Palliat. Care 2017, 7, 470–479. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.; Krueger, P.; Webster, F.; Downar, J.; Herx, L.; Jeney, C.; Oneschuk, D.; Schroder, C.; Sirianni, G.; Seccareccia, D.; et al. Development and validation of a set of palliative medicine entrustable professional activities: Findings from a mixed methods study. J. Palliat. Med. 2015, 18, 682–690. [Google Scholar] [CrossRef]
- Taylor, P.; Johnson, M.; Dowding, D.W. Clinical decision-making at the end of life: A mixed-methods study. BMJ Support. Palliat. Care 2018. [Google Scholar] [CrossRef]
- Fryer, C.S.; Seaman, E.L.; Clark, R.S.; Plano Clark, V. Mixed methods research in tobacco control with youth and young adults: A methodological review of current strategies. PLoS ONE 2017, 12, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Hill, H.C.; Paley, J.; Forbat, L. Observations of professional-patient relationships: A mixed-methods study exploring whether familiarity is a condition for nurses’ provision of psychosocial support. Palliat. Med. 2014, 28, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Boss, R.D.; Hutton, N.; Griffin, P.L.; Wieczorek, B.H.; Donohue, P.K. Novel legislation for pediatric advance directives: Surveys and focus groups capture parent and clinician perspectives. Palliat. Med. 2015, 29, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Pype, P.; Mertens, F.; Wens, J.; Stes, A.; Van Den, E.; Deveugele, M. Preparing palliative home care nurses to act as facilitators for physicians’ learning: Evaluation of a training programme. Palliat. Med. 2015, 29, 458–463. [Google Scholar] [CrossRef]
- Kimbell, B.; Murray, S.A.; Byrne, H.; Baird, A.; Hayes, P.C.; MacGilchrist, A.; Finucane, A.; Brookes, Y.; O’Carroll, R.E.; Weir, C.J.; et al. Palliative care for people with advanced liver disease: A feasibility trial of a supportive care liver nurse specialist. Palliat. Med. 2018, 32, 919–929. [Google Scholar] [CrossRef] [Green Version]
- Philip, J.; Crawford, G.; Brand, C.; Gold, M.; Miller, B.; Hudson, P.; Smallwood, N.; Lau, R.; Sundararajan, V. A conceptual model: Redesigning how we provide palliative care for patients with chronic obstructive pulmonary disease. Palliat. Support. Care 2018, 16, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, P.B.; Ramalingam, N.; Carter, K.F.; Katz, K.; Harden, S. Nurse practitioners’ perspectives on the patient preferences about serious illness instrument. J. Hosp. Palliat. Nurs. 2016, 18, 332–341. [Google Scholar] [CrossRef]
- Younas, A.; Pedersen, M.; Tayaben, J. Review of mixed-methods research in nursing. Nurs. Res. 2019, 68, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.T.; Tam-Tham, H.; Dhaliwal, K.K.; Manns, B.J.; Hemmelgarn, B.R.; Sanmartin, C.; King-Shier, K. Use of mixed methods research in research on coronary artery disease, diabetes mellitus, and hypertension: A scoping review. Circ. Cardiovasc. Qual. Outcomes 2017, 10. [Google Scholar] [CrossRef]
- Brown, K.M.; Elliott, S.J.; Leatherdale, S.T.; Robertson-Wilson, J. Searching for rigour in the reporting of mixed methods population health research: A methodological review. Health Educ. Res. 2015, 30, 811–839. [Google Scholar] [CrossRef]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef]
- Tariq, S.; Woodman, J. Using mixed methods in health research. JRSM Short Rep. 2010, 4. [Google Scholar] [CrossRef] [PubMed]
- Leech, N.L.; Onwuegbuzie, A.J.; Combs, J.P. Writing publishable mixed research articles: Guidelines for emerging scholars in the health sciences and beyond. Int. J. Mult. Res. Approaches 2011, 5, 7–24. [Google Scholar] [CrossRef]
- Fàbregues, S.; Molina-Azorin, J.F. Addressing quality in mixed methods research: A review and recommendations for a future agenda. Qual. Quant. 2017, 51, 2847–2863. [Google Scholar] [CrossRef]
- Jors, K.; Tietgen, S.; Xander, C.; Momm, F.; Becker, G. Tidying rooms and tending hearts: An explorative, mixed-methods study of hospital cleaning staff’s experiences with seriously ill and dying patients. Palliat. Med. 2017, 31, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Zweers, D.; de Graaf, E.; Teunissen, S. Suitable support for anxious hospice patients: What do nurses ‘know’, ‘do’ and ‘need’? An explanatory mixed method study. BMJ Support. Palliat. Care 2017. [Google Scholar] [CrossRef]
- Knighting, K.; O’Brien, M.R.; Roe, B.; Gandy, R.; Lloyd-Williams, M.; Nolan, M.; Jack, B.A. Development of the Carers’ Alert Thermometer (CAT) to identify family carers struggling with caring for someone dying at home: A mixed method consensus study. BMC Palliat. Care 2015, 14. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Journals | Year | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Jan 2014 | 2015 | 2016 | 2017 | 2018 | April 2019 | Total | Mixed Methods Studies | % | |
| American Journal of Hospice & Palliative Medicine | 91 | 102 | 106 | 115 | 186 | 98 | 698 | 26 | 3.7 |
| BMC Palliative Care | 50 | 56 | 77 | 76 | 97 | 30 | 386 | 32 | 8.2 |
| BMJ Supportive & Palliative Care | 33 | 53 | 43 | 57 | 77 | 48 | 311 | 17 | 5.4 |
| Journal of Hospice & Palliative Nursing | 37 | 44 | 40 | 45 | 48 | 17 | 231 | 8 | 3.4 |
| Journal of Palliative Care | 13 | 22 | 0 | 15 | 39 | 11 | 100 | 3 | 3.0 |
| Journal of Palliative Medicine | 114 | 115 | 134 | 135 | 181 | 23 | 702 | 23 | 3.2 |
| Palliative & Supportive Care | 51 | 75 | 51 | 53 | 104 | 35 | 369 | 20 | 5.4 |
| Palliative Medicine | 64 | 73 | 63 | 65 | 123 | 40 | 428 | 30 | 7.0 |
| Total | 453 | 540 | 514 | 561 | 855 | 302 | 3225 | 159 | 4.9 |
| Characteristics | n (%) |
|---|---|
| Geographical area of the corresponding author | |
| Africa | 1 (0.6) |
| Asia | 7 (4.4) |
| Europe | 72 (45.3) |
| North America | 66 (41.5) |
| Oceania | 13 (8.2) |
| Study identification regarding mixed methods | |
| Self-identified as mixed methods | 108 (67.9) |
| Non-identified as mixed methods | 51 (32.1) |
| Cited key literature on mixed methods | 38 (23.9) |
| Study topic | |
| Care planning, place of care, transition, and documentation | 62 (39.0) |
| Caring, situations, and relationships | 7 (4.4) |
| Existential and ethical issues | 15 (9.4) |
| Experiences of illness, well-being, needs, and environment | 12 (7.5) |
| Organizational or professional development | 42 (26.4) |
| Symptom assessment and management | 10 (6.3) |
| Other topics | 11 (6.9) |
| Study purpose | |
| Assessment of palliative care needs | 4 (2.5) |
| Evaluation of an intervention in or program or service for palliative care | 69 (43.4) |
| Investigation of a research topic in palliative care | 51 (32.1) |
| Development and evaluation of an intervention in or program or service for palliative care | 6 (3.8) |
| Development and validation of a quantitative instrument for palliative care | 10 (6.3) |
| Development of a tool or model for palliative care | 19 (11.9) |
| GRAMMS Criteria | Yes 1 n (%) | Yes, but n (%) | No n (%) |
|---|---|---|---|
| 1. Describes the justification for using mixed methods research to the research question | 100 (62.9) | 48 (30.2) | 11 (6.9) |
| 2. Describes the mixed methods design in terms of the purpose, priority and sequence of methods | 8 (5.0) | 44 (27.7) | 107 (67.3) |
| 3. Describes each method in terms of sampling, data collection and analysis | 106 (66.7) | 51 (32.1) | 2 (1.3) |
| 4. Describes the integration of the quantitative and qualitative components 2 | 106 (66.7) | 17 (10.7) | 36 (22.6) |
| 5. Describes any limitation of one method associated with the presence of the other method | 6 (3.8) | 0 (0) | 153 (96.2) |
| 6. Describes any insights gained from mixing or integrating methods | 42 (26.4) | 5 (3.1) | 112 (70.4) |
| Mixed Methods Features 1 | n (%) |
|---|---|
| Justification for using mixed methods research criteria2(n = 148) | |
| Complementarity | 122 (82.4) |
| Development | 66 (44.6) |
| To inform data collection | 42 (28.4) |
| To inform sampling | 24 (16.2) |
| Triangulation | 20 (13.5) |
| Type of mixed methods design (n = 159) | |
| Convergent | 92 (57.9) |
| Exploratory sequential | 16 (10.1) |
| Explanatory sequential | 30 (18.9) |
| Multistage | 21 (13.2) |
| Integration at the methods level2(n = 123) | |
| Merging | 101 (82.1) |
| Building | 43 (35.0) |
| Connecting | 22 (17.9) |
| Integration at the reporting level2(n = 106) | |
| Narrative | 87 (82.1) |
| Joint display | 15 (14.2) |
| Data transformation | 4 (3.8) |
| Study Purpose | Type of Design | ||||
|---|---|---|---|---|---|
| Convergent n (%) | Exploratory Sequential n (%) | Explanatory Sequential n (%) | Multistage n (%) | Total n (%) | |
| Assessment of palliative care needs | 2 (2.2) | 0 (0) | 1 (3.3) | 1 (4.8) | 4 (2.5) |
| Evaluation of an intervention in or program or service for palliative care | 60 (65.2) | 0 (0) | 6 (20.0) | 3 (14.3) | 69 (43.4) |
| Investigation of a research topic in palliative care | 26 (28.3) | 4 (25) | 19 (63.3) | 2 (9.5) | 51 (32.1) |
| Development and evaluation of an intervention in or program or service for palliative care | 0 (0) | 0 (0) | 0 (0) | 6 (28.6) | 6 (3.8) |
| Development and validation of a quantitative instrument for palliative care | 1 (1.1) | 7 (43.8) | 0 (0) | 2 (9.5) | 10 (6.3) |
| Development of a tool or model for palliative care | 3 (3.3) | 5 (31.3) | 4 (13.3) | 7 (33.3) | 19 (11.9) |
| GRAMMS Criteria | Type of Design | ||||||
|---|---|---|---|---|---|---|---|
| Convergent n (%) | Exploratory Sequential n (%) | Explanatory Sequential n (%) | Multistage n (%) | Total n (%) | Fisher’s Value | p Value | |
| 1. Describes the justification for using mixed methods research to the research question | 34.586 | 0.001 | |||||
| Yes | 41 (44.6) | 16 (100) | 27 (90.0) | 16 (76.2) | 100 (62.9) | ||
| Yes, but | 42 (45.7) | 0 (0) | 2 (6.7) | 4 (19.0) | 48 (30.2) | ||
| No | 9 (9.8) | 0 (0) | 1 (3.3) | 1 (4.8) | 11 (6.9) | ||
| 2. Describes the mixed methods research design in terms of the purpose, priority and sequence of methods | 7.368 | 0.232 | |||||
| Yes | 8 (8.7) | 0 (0) | 0 (0) | 0 (0) | 8 (5.0) | ||
| Yes, but | 21 (22.8) | 6 (37.5) | 12 (40.0) | 5 (23.8) | 44 (27.7) | ||
| No | 63 (68.5) | 10 (62.5) | 18 (60.0) | 16 (76.2) | 107 (67.3) | ||
| 3. Describes each method in terms of sampling, data collection and analysis | 3.128 | 0.807 | |||||
| Yes | 64 (69.6) | 10 (62.5) | 20 (66.7) | 12 (57.1) | 106 (66.7) | ||
| Yes, but | 26 (28.3) | 6 (37.5) | 10 (33.3) | 9 (42.9) | 51 (32.1) | ||
| No | 2 (2.2) | 0 (0) | 0 (0) | 0 (0) | 2 (1.3) | ||
| 4. Describes the integration of the quantitative and qualitative components | 22.570 | 0.001 | |||||
| Yes | 58 (63.0) | 11 (68.8) | 20 (66.7) | 17 (81.0) | 106 (66.7) | ||
| Yes, but | 4 (4.3) | 5 (31.3) | 6 (20) | 2 (9.5) | 17 (10.7) | ||
| No | 30 (32.6) | 0 (0) | 4 (13.3) | 2 (9.5) | 36 (22.6) | ||
| 5. Describes any limitation of one method associated with the presence of the other method | 6.124 | 0.062 | |||||
| Yes | 2 (2.2) | 0 (0) | 4 (13.3) | 0 (0) | 6 (3.8) | ||
| Yes, but | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| No | 90 (97.8) | 16 (100) | 26 (86.7) | 21 (100) | 153 (96.2) | ||
| 6. Describes any insights gained from mixing or integrating methods | 6.051 | 0.347 | |||||
| Yes | 29 (31.5) | 2 (12.5) | 8 (26.7) | 3 (14.3) | 42 (26.4) | ||
| Yes, but | 3 (3.3) | 1 (6.3) | 0 (0) | 1 (4.8) | 5 (3.1) | ||
| No | 60 (65.2) | 13 (81.3) | 22 (73.3) | 17 (81.0) | 112 (70.4) | ||
| Authors | Objective | Justification for Using Mixed Methods | Mixed Methods Design | Data Sources | Integration | Insights Gained from Using Mixed Methods |
|---|---|---|---|---|---|---|
| Van Scoy et al. [17] | Evaluate an end-of-life conversation game | Complementarity [p. 595] 1 | Convergent [pp. 594–595] | Questionnaires on the confidence experienced by participants during the game, and interviews on participants’ views on the game [p. 595] | Merging, by comparing the quantitative and qualitative findings through a joint display table [pp. 595–598] | The convergence between the two types of findings strengthened the conclusions and facilitated a more comprehensive evaluation of the game [p. 599] |
| Jors et al. [40] | Investigate interactions between cleaning staff and patients | Development to inform data collection/Triangulation [p. 64] | Exploratory sequential [p. 64] | Interviews and focus groups with cleaning staff on patient interaction and coping with death, and questionnaire distributed to cleaning staff [pp. 64–65] | Building, by using the qualitative findings to generate a questionnaire. Merging, by comparing both findings through narrative [pp. 64–67] | The qualitative findings provided a more comprehensive basis for designing the questions included in the quantitative questionnaire [p. 71] |
| Zweers et al. [41] | Examine nurses’ knowledge, needs and practices when supporting anxious patients | Complementarity/Development to inform sampling [p. 2] | Explanatory sequential [p. 2] | Online survey with nurses caring for anxious patients on their knowledge, needs and practices, and focus groups with nurses who completed the survey [p. 2–3] | Connecting, by using the survey findings to inform the qualitative sampling. Merging, by comparing both findings through narrative [pp. 2–7] | The quantitative findings helped to define the qualitative sample. The qualitative findings provided deeper insight into the quantitative findings on anxiety management practices by nurses [p. 8] |
| Knighting et al. [42] | Develop an alert thermometer for carers and non-specialist staff | Complementarity/Development to inform data collection/Development to inform sampling [pp. 3–4] | Multistage [p. 3] | Interviews and focus groups with carers for item generation. Delphi survey with carers and health professionals for item selection [pp. 3–9] | Building and connecting, by using the qualitative findings to inform the Delphi content and sampling. Merging through narrative [pp. 3–9] | Mixed methods enabled researchers to sequentially develop and select the items of the alert thermometer. It also allowed incorporation of views and experiences of a wide range of participants [pp. 10–11] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fàbregues, S.; Hong, Q.N.; Escalante-Barrios, E.L.; Guetterman, T.C.; Meneses, J.; Fetters, M.D. A Methodological Review of Mixed Methods Research in Palliative and End-of-Life Care (2014–2019). Int. J. Environ. Res. Public Health 2020, 17, 3853. https://doi.org/10.3390/ijerph17113853
Fàbregues S, Hong QN, Escalante-Barrios EL, Guetterman TC, Meneses J, Fetters MD. A Methodological Review of Mixed Methods Research in Palliative and End-of-Life Care (2014–2019). International Journal of Environmental Research and Public Health. 2020; 17(11):3853. https://doi.org/10.3390/ijerph17113853
Chicago/Turabian StyleFàbregues, Sergi, Quan Nha Hong, Elsa Lucia Escalante-Barrios, Timothy C. Guetterman, Julio Meneses, and Michael D. Fetters. 2020. "A Methodological Review of Mixed Methods Research in Palliative and End-of-Life Care (2014–2019)" International Journal of Environmental Research and Public Health 17, no. 11: 3853. https://doi.org/10.3390/ijerph17113853
APA StyleFàbregues, S., Hong, Q. N., Escalante-Barrios, E. L., Guetterman, T. C., Meneses, J., & Fetters, M. D. (2020). A Methodological Review of Mixed Methods Research in Palliative and End-of-Life Care (2014–2019). International Journal of Environmental Research and Public Health, 17(11), 3853. https://doi.org/10.3390/ijerph17113853