Association of Work Patterns and Periodontitis Prevalence in Korean Adults Aged 50 Years or Older: A Nationwide Representative Study


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
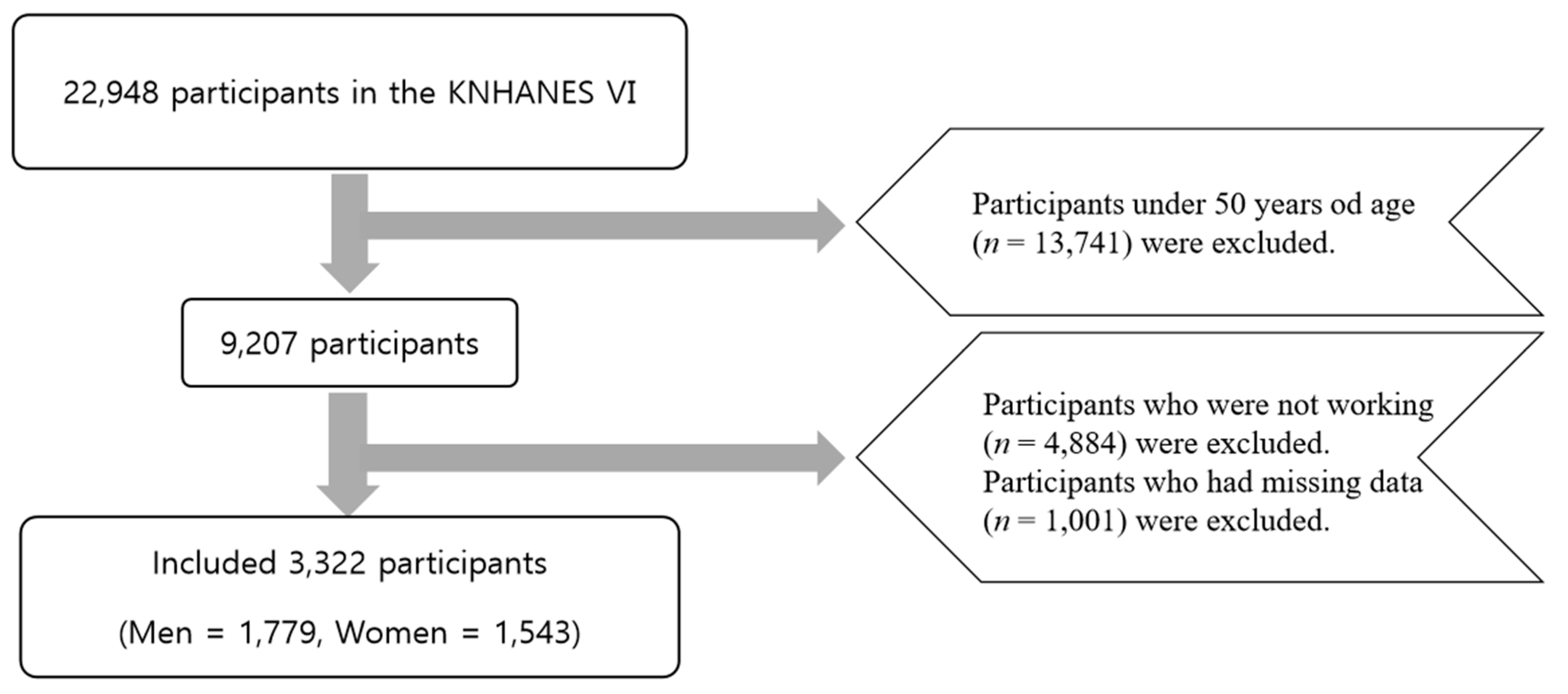
2.1. Study Population
2.2. General Characteristics of the Study Participants
2.3. Work Pattern
2.4. Oral Examination
2.5. Periodontal Status
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population at Baseline
3.2. Health Behaviors and Lifestyle-Related Disorders
3.3. Dental Health Care Behaviors
3.4. Association between Work Pattern and Periodontitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Locker, D.; Clarke, M.; Payne, B. Self-perceived oral health status, psychological well-being, and life satisfaction in an older adult population. J. Dent. Res. 2000, 79, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Lee, Y.H. Association between Sleep Duration, Dental Caries, and Periodontitis in Korean Adults: The Korea National Health and Nutrition Examination Survey, 2013–2014. J. Dent. Hyg. Sci. 2017, 17, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions–Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef]
- Burt, B. Position paper: Epidemiology of periodontal diseases. J. Periodontol. 2005, 76, 1406–1419. [Google Scholar]
- Hong, M.-H. Risk factors for the prevalence of periodontal diseases among adult workers. J. Korea Acad.-Ind. Coop. Soc. 2014, 15, 3706–3713. [Google Scholar]
- Petersen, P.E.; Ogawa, H. Strengthening the prevention of periodontal disease: The WHO approach. J. Periodontol. 2005, 76, 2187–2193. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Oral Health: Periodontal Diseases. Available online: https://www.cdc.gov/oralhealth/conditions/periodontal-disease.html (accessed on 2 June 2020).
- Brennan, D.; Spencer, A.; Roberts-Thomson, K. Quality of life and disability weights associated with periodontal disease. J. Dent. Res. 2007, 86, 713–717. [Google Scholar] [CrossRef]
- Choi, M.-I.; Mun, S.-J. Relationship between socioeconomic characteristics and prevalence of periodontal disease in Korean adults: The 6 th Korean National Health and Nutrition (2015). J. Korean Soc. Dent. Hyg. 2017, 17, 1109–1119. [Google Scholar]
- Chen, M.S.; Stone, D.B. Toothbrushing, flossing, and dental visits in relation to socioeconomic characteristics of white American families. Community Dent. Oral Epidemiol. 1983, 11, 325–332. [Google Scholar] [CrossRef]
- Lee, J.-S.; Kang, H.-K. A Study on Factors to Periodontal Diseases in Patients with Metabolic Syndrome in Health Examination Examinees. J. Korea Converg. Soc. 2018, 9, 259–268. [Google Scholar]
- Kang, H.-J. Convergence relationship between Health Behaviors, urinalysis and Periodontitis. J. Korea Converg. Soc. 2018, 9, 117–124. [Google Scholar]
- Jung, J.-O.; Chun, J.-Y.; Lee, K.-H. The relationship between smoking and periodontal diseases in Korean adults: Based on the data from the Korea National Health and Nutrition Examination Survey 2010. J. Korean Soc. Dent. Hyg. 2013, 13, 481–489. [Google Scholar] [CrossRef]
- Preshaw, P.; Alba, A.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.-K.; Park, J.-R. The relationship of obesity and periodontal disease by age. J. Korean Soc. Dent. Hyg. 2013, 13, 1015–1021. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.-J.; Kim, E.-K.; An, S.-Y.; Im, S.-U.; Song, K.-B.; Choi, Y.-H. Relationship between periodontal status and chronic obstructive pulmonary disease. J. Korean Acad. Oral Health 2013, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Won, Y.-S.; Choi, C.-H.; OH, H. Risk factors of periodontal disease in Korean adults. J. Korean Acad. Oral Health 2014, 38, 176–183. [Google Scholar] [CrossRef]
- Wang, J.H.; Lee, G.; Song, J.T.; Kwon, J.; Choi, H.; Jung-Choi, K.; Lim, S. The association between shift work and bone mineral density: Analysis of 2008–2009 Korean National Health and Nutrition Examination Survey. Korean J. Occup. Environ. Med. 2012, 24, 274–286. [Google Scholar] [CrossRef]
- LaDou, J.; Harrison, R. Current Occupational & Environmental Medicine; McGraw-Hill New York: New York, NY, USA, 2007. [Google Scholar]
- Park, J.S.; Paek, D.; Lee, K.B.; Rhee, K.Y.; Yi, K.H. Shiftwork and Sickness Absence in Korean Manufacturing Industries. J. Prev. Med. Public Health 1994, 27, 475–486. [Google Scholar]
- Costa, G. The impact of shift and night work on health. Appl. Ergon. 1996, 27, 9–16. [Google Scholar] [CrossRef]
- Knutsson, A. Health disorders of shift workers. Occup. Med. 2003, 53, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Skogstad, M.; Mamen, A.; Lunde, L.-K.; Ulvestad, B.; Matre, D.; Aass, H.C.D.; Øvstebø, R.; Nielsen, P.; Samuelsen, K.N.; Skare, Ø. Shift work including night work and long working hours in industrial plants increases the risk of atherosclerosis. Int. J. Environ. Res. Public Health 2019, 16, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.-C.; Chen, T.-P.; Wei, C.-Y.; Chang, Y.-C. Association between peptic ulcer disease and periodontitis: A nationwide population-based case-control study in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthelsen, M.; Pallesen, S.; Magerøy, N.; Tyssen, R.; Bjorvatn, B.; Moen, B.E.; Knardahl, S. Effects of psychological and social factors in shiftwork on symptoms of anxiety and depression in nurses: A 1-year follow-up. J. Occup. Environ. Med. 2015, 57, 1127–1137. [Google Scholar] [CrossRef]
- Lee, A.; Myung, S.-K.; Cho, J.J.; Jung, Y.-J.; Yoon, J.L.; Kim, M.Y. Night shift work and risk of depression: Meta-analysis of observational studies. J. Korean Med Sci. 2017, 32, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.K.; Lee, K.R.; Suh, H.S.; Ko, K.D. Association between shift work and suicidal ideation: Data from the Korea National Health and Nutrition Examination Survey (2008–2016) Kim KK, Lee KR, Suh HS, Ko KD, Hwang IC. Depress. Anxiety 2019, 8, 9. [Google Scholar]
- Liu, X.; Uchiyama, M.; Kim, K.; Okawa, M.; Shibui, K.; Kudo, Y.; Doi, Y.; Minowa, M.; Ogihara, R. Sleep loss and daytime sleepiness in the general adult population of Japan. Psychiatry Res. 2000, 93, 1–11. [Google Scholar] [CrossRef]
- Hong, S.H.; Kim, S.Y. Effects of sleep promoting program on sleep and immune response in elderly. J. Korean Acad. Adult Nurs. 2009, 21, 167. [Google Scholar]
- Kawachi, I.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Manson, J.E.; Speizer, F.E.; Hennekens, C.H. Prospective study of shift work and risk of coronary heart disease in women. Circulation 1995, 92, 3178–3182. [Google Scholar] [CrossRef]
- Åkerstedt, T.; Nordin, M.; Alfredsson, L.; Westerholm, P.; Kecklund, G. Sleep and sleepiness: Impact of entering or leaving shiftwork—A prospective study. Chronobiol. Int. 2010, 27, 987–996. [Google Scholar] [CrossRef]
- Hansen, J.; Stevens, R.G. Night shiftwork and breast cancer risk: Overall evidence. Occup. Environ. Med. 2011, 68, 236. [Google Scholar] [CrossRef]
- Moon, S.-H.; Lee, B.-J.; Kim, S.-J.; Kim, H.-C. Relationship between thyroid stimulating hormone and night shift work. Ann. Occup. Environ. Med. 2016, 28, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, M.-J.; Song, Y.-M.; Shin, J.-Y.; Choi, B.-Y.; Keum, J.-H.; Lee, E.-A. The association between shift work and health behavior: Findings from the Korean National Health and Nutrition Examination Survey. Korean J. Fam. Med. 2017, 38, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Total (n = 3320) | Work Pattern | Weighted | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Regular | Irregular | Regular | Irregular | ||||
| Sex | Male | 1779 (53.6%) | 1504 (53.3%) | 275 (55.2%) | 58.6% | 59.5% | 0.756 |
| Female | 1543 (46.4%) | 1320 (46.7%) | 223 (44.8%) | 41.4% | 40.5% | ||
| Age, years | 60.86 ± 7.32 | 60.99 ± 7.40 | 60.12 ± 6.84 | 59.40 ± 0.19 | 58.83 ± 0.34 | 0.133 | |
| Family income, percentile, % | 25th | 629 (18.9%) | 565 (20.0%) | 64 (12.9%) | 16.9% | 12.5% | 0.065 |
| 25–50th | 957 (28.8%) | 808 (28.6%) | 149 (29.9%) | 26.8% | 27.6% | ||
| 50–75th | 810 (24.4%) | 663 (23.5%) | 147 (29.5%) | 25.4% | 30.9% | ||
| 75–100th | 926 (27.9%) | 788 (27.9%) | 138 (27.7%) | 30.9% | 29.0% | ||
| Education level, % | Elementary school or less | 1196 (36.0%) | 1048 (37.1%) | 148 (29.7%) | 32.4% | 25.9% | <0.001 |
| Middle school graduate | 664 (20.0%) | 567 (20.1%) | 97 (19.5%) | 20.6% | 18.4% | ||
| High school graduate | 894 (26.9%) | 710 (25.1%) | 184 (36.9%) | 27.0% | 39.4% | ||
| College graduate or higher | 568 (17.1%) | 499 (17.7%) | 69 (13.9%) | 20.1% | 16.3% | ||
| Smoking status, % | Yes | 593 (17.9%) | 487 (17.2%) | 106 (21.3%) | 19.1% | 24.9% | 0.014 |
| Alcohol consumption, % | High risk | 461 (13.9%) | 402 (14.2%) | 59 (11.8%) | 17.0% | 14.2% | 0.248 |
| Obesity | BMI >25 | 1249 (37.6%) | 1066 (37.7%) | 183 (36.7%) | 38.0% | 36.6% | 0.867 |
| BMI | 24.26 ± 3.01 | 24.28 ± 3.02 | 24.13 ± 2.95 | 24.29 ± 0.07 | 24.13 ± 0.14 | 0.307 | |
| HTN | Yes | 1084 (32.6%) | 937 (33.2%) | 147 (29.5%) | 29.8% | 27.9% | 0.463 |
| DM | Yes | 382 (11.5%) | 318 (11.3%) | 64 (12.9%) | 10.6% | 13.5% | 0.114 |
| Dyslipidemia | Yes | 678 (20.4%) | 562 (19.9%) | 116 (23.3%) | 18.7% | 23.1% | 0.041 |
| Male Workers | p-Value | Female Workers | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Regular Shifts | Irregular Shifts | Regular Shifts | Irregular Shifts | ||||
| Diabetes mellitus | Yes | 12.4% | 15.3% | 0.273 | 8.0% | 10.8% | 0.264 |
| Hypertension | Yes | 8.8% | 30.0% | 0.73 | 31.4% | 24.9% | 0.087 |
| Dyslipidemia | Yes | 15.5% | 19.5% | 0.168 | 23.2% | 28.4% | 0.159 |
| Annual health examination | Yes | 73.5% | 77.9% | <0.001 | 75.9% | 76.4% | <0.001 |
| Smoking status, % | Yes | 30.6% | 37.3% | 0.071 | 2.8% | 6.8% | 0.013 |
| Alcohol consumption, % | No | 35.5% | 38.5% | 0.429 | 78.2% | 72.5% | 0.112 |
| Low risk | 39.5% | 40.9% | 16.0% | 22.7% | |||
| High risk | 25.0% | 20.5% | 5.7% | 4.8% | |||
| Sleep duration (h/day) | 6.71 ± 0.04 | 6.63 ± 0.09 | 0.358 | 6.49 ± 0.04 | 6.32 ± 0.09 | 0.09 | |
| Stress level | High | 2.9% | 2.7% | 0.977 | 4.6% | 5.0% | 0.641 |
| Moderate | 13.6% | 13.6% | 20.7% | 22.2% | |||
| Male Workers | p-Value | Female Workers | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Regular Shifts | Irregular Shifts | Regular Shifts | Irregular Shifts | ||||
| Dental brushing (%) | No | 1.4% | 1.1% | 0.66 | 1.5% | 0.4% | 0.167 |
| Yes | 98.6% | 98.9% | 98.5% | 99.6% | |||
| Use of dental care products | No | 58.6% | 54.5% | 0.325 | 53.0% | 45.7% | 0.083 |
| Yes | 41.4% | 45.5% | 47.0% | 54.3% | |||
| Tooth damage | No | 81.5% | 80.2% | 0.674 | 92.6% | 90.1% | 0.279 |
| Yes | 18.5% | 19.8% | 7.4% | 9.9% | |||
| Annual dental examination | No | 65.1% | 66.4% | 0.731 | 73.4% | 65.7% | 0.043 |
| Yes | 34.9% | 33.6% | 26.6% | 34.3% | |||
| Attendance at a dental clinic | No | 43.7% | 37.7% | 0.122 | 50.3% | 48.6% | 0.67 |
| Yes | 56.3% | 62.3% | 49.7% | 51.4% | |||
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Total | 1.14(0.91–1.43) | 0.256 | 1.13 (0.90–1.42) | 0.006 | 1.19 (0.94–1.50) | 0.152 | 1.19 (0.94–1.51) | 0.152 |
| Male | 0.95 (0.69–1.30) | 0.742 | 0.95 (0.69–1.30) | 0.813 | 0.98 (0.71–1.35) | 0.9 | 0.98 (0.71–1.35) | 0.893 |
| Female | 1.58 (1.11–2.24) | 0.011 | 1.48 (1.05–2.10) | 0 | 1.57 (1.10–2.24) | 0.012 | 1.56 (1.10–2.22) | 0.014 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ra, Y.J.; Tak, Y.J.; Kim, Y.J.; Lee, S.Y.; Lee, J.G.; Yi, Y.H.; Cho, Y.H.; Hwang, H.R.; Lee, S.H.; Park, E.J.; et al. Association of Work Patterns and Periodontitis Prevalence in Korean Adults Aged 50 Years or Older: A Nationwide Representative Study. Int. J. Environ. Res. Public Health 2020, 17, 4006. https://doi.org/10.3390/ijerph17114006
Ra YJ, Tak YJ, Kim YJ, Lee SY, Lee JG, Yi YH, Cho YH, Hwang HR, Lee SH, Park EJ, et al. Association of Work Patterns and Periodontitis Prevalence in Korean Adults Aged 50 Years or Older: A Nationwide Representative Study. International Journal of Environmental Research and Public Health. 2020; 17(11):4006. https://doi.org/10.3390/ijerph17114006
Chicago/Turabian StyleRa, Young Jin, Young Jin Tak, Yun Jin Kim, Sang Yeoup Lee, Jeong Gyu Lee, Yu Hyeon Yi, Young Hye Cho, Hye Rim Hwang, Seung Hun Lee, Eun Ju Park, and et al. 2020. "Association of Work Patterns and Periodontitis Prevalence in Korean Adults Aged 50 Years or Older: A Nationwide Representative Study" International Journal of Environmental Research and Public Health 17, no. 11: 4006. https://doi.org/10.3390/ijerph17114006
APA StyleRa, Y. J., Tak, Y. J., Kim, Y. J., Lee, S. Y., Lee, J. G., Yi, Y. H., Cho, Y. H., Hwang, H. R., Lee, S. H., Park, E. J., & Lee, Y. I. (2020). Association of Work Patterns and Periodontitis Prevalence in Korean Adults Aged 50 Years or Older: A Nationwide Representative Study. International Journal of Environmental Research and Public Health, 17(11), 4006. https://doi.org/10.3390/ijerph17114006