Using Electronic Medical Record Data to Better Understand Obesity in Hispanic Neighborhoods in El Paso, Texas

Abstract
:1. Introduction
2. Materials and Methods
2.1. Electronic Medical Record (EMR) and U.S. Census Bureau Data
2.2. Body Mass Index (BMI) Measurement
2.2.1. Hispanic Ethnic Concentration
2.2.2. Economic Confounders
2.2.3. Sociodemographic Confounders
2.3. Analysis
2.4. Geographic-Weighted Regression
2.5. Hot Spot Using ArcGIS
2.6. Path Analysis using Structural Equation Modeling
3. Results
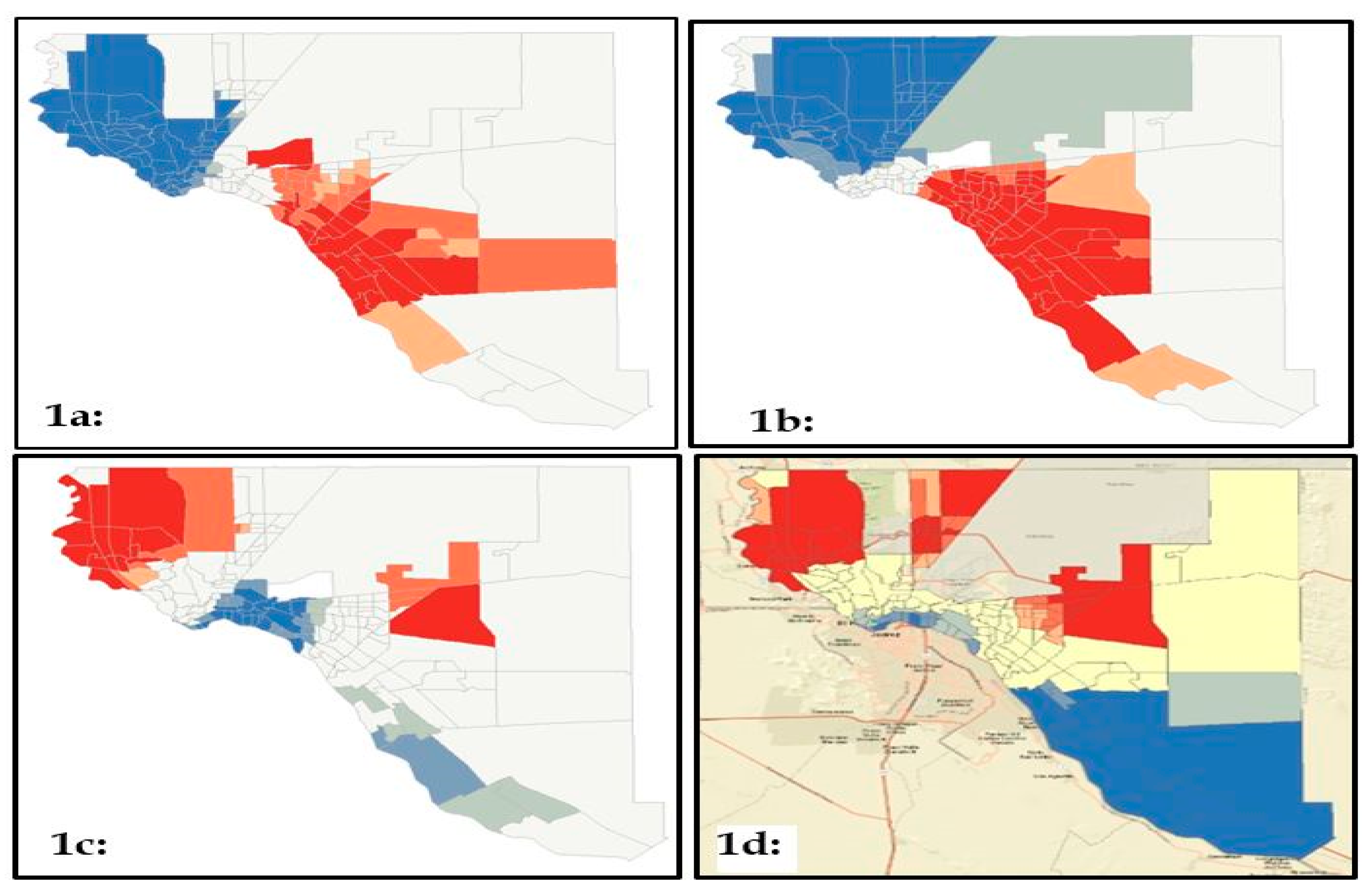
3.1. Geographic-Weighted Regression Analysis
3.2. Hotspots
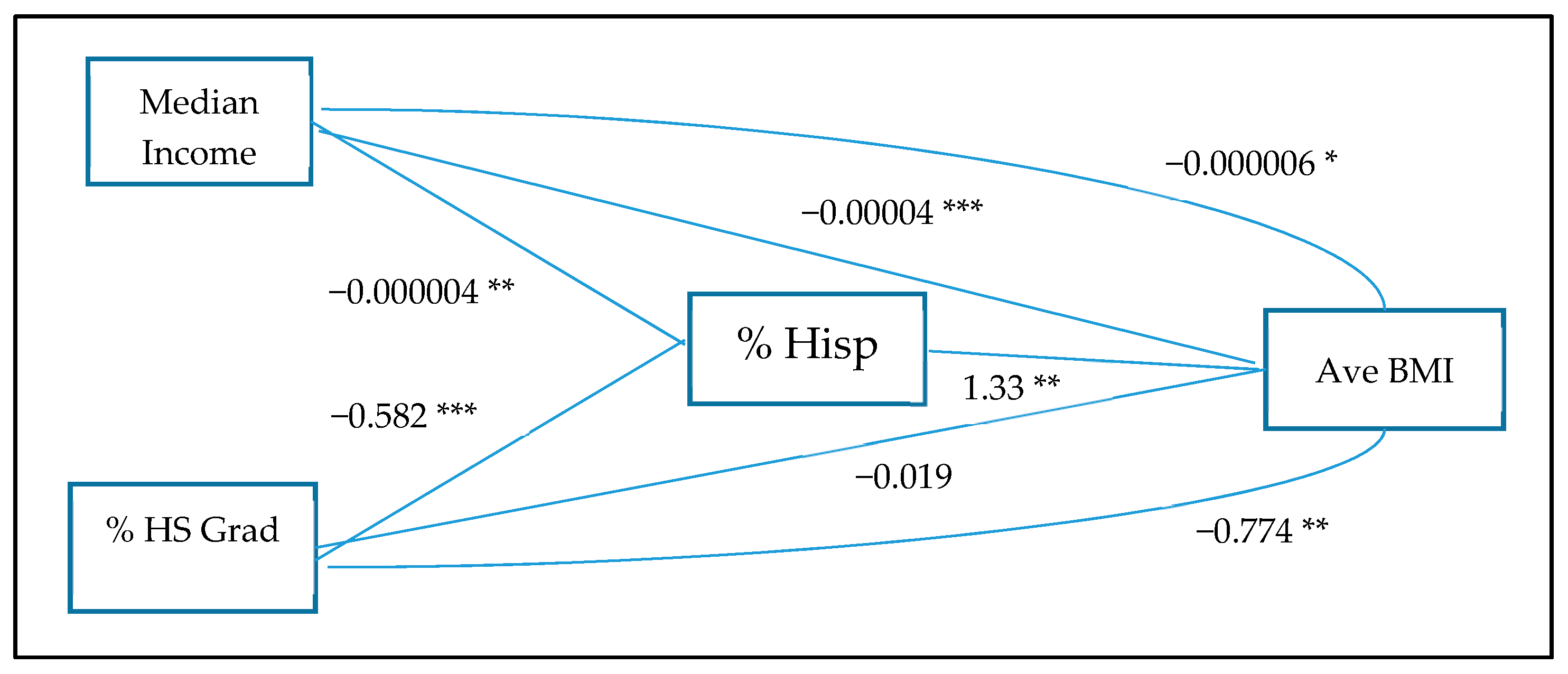
3.3. Path Analysis
4. Discussion
4.1. Hispanic Ethnic Concentration is a Risk Factor for Obesity
4.2. Socioeconomics, Hispanic Ethnic Concentration, and Obesity
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| EMR | Electronic Medical Records |
| BMI | Body Mass Index |
References
- Flores, Y.N.; Zhang, Z.F.; Bastani, R.; Leng, M.; Crespi, C.M.; Ramírez-Palacios, P.; Stevens, H.; Salmerón, J. Risk factors for liver disease among adults of Mexican descent in the United States and Mexico. World J. Gastroenterol. 2018, 24, 4281–4290. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, B.A.; Garcia, M.P.; Corley, D.A.; Doubeni, C.A.; Haas, J.S.; Kamineni, A.; Quinn, V.P.; Wernli, K.; Zheng, Y.; Skinner, C.S.; et al. Racial/ethnic differences in obesity and comorbidities between safety-net- and non safety-net integrated health systems. Medicine (Baltim.) 2017, 96, e6326. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief 2017, 288, 1–8. [Google Scholar]
- An, R.; Xiang, X. Age–period–cohort analyses of obesity prevalence in US adults. Public Health 2016, 141, 163–169. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Hypertension among Adults Aged 20 and Over, by Selected Characteristics: United States, Selected Years 1988–1994 through 2013–2016 (Table 2); National Center for Health Statistics: Hyattsville, MD, USA, 2018; pp. 1–3.
- Fan, J.; Wen, M.; Li, K. Associations between obesity and neighborhood socioeconomic status: Variations by gender and family income status. SSM Popul. Health 2019, 10, 100529. [Google Scholar] [CrossRef]
- Yang, T.C.; South, S. Neighborhood effects on body mass: Temporal and spatial dimensions. Soc. Sci. Med. 2018, 217, 45–54. [Google Scholar] [CrossRef]
- Haire-Joshu, D.; Hill-Briggs, F. The Next Generation of Diabetes Translation: A Path to Health Equity. Annu. Rev. Public Health 2019, 40, 391–410. [Google Scholar] [CrossRef] [Green Version]
- Philbin, M.M.; Flake, M.; Hatzenbuehler, M.L.; Hirsch, J.S. State-level immigration and immigrant-focused policies as drivers of Latino health disparities in the United States. Soc. Sci. Med. 2018, 199, 29–38. [Google Scholar] [CrossRef]
- Okoro, C.A.; Zhao, G.; Fox, J.B.; Eke, P.I.; Greenlund, K.J.; Town, M. Surveillance for Health Care Access and Health Services Use, Adults Aged 18–64 Years - Behavioral Risk Factor Surveillance System, United States, 2014. MMWR Surveill. Summ. 2017, 66, 1–42. [Google Scholar] [CrossRef]
- Yu, C.Y.; Woo, A.; Hawkins, C.; Iman, S. The Impacts of Residential Segregation on Obesity. J. Phys. Act. Health 2018, 15, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.J.; Rocha, E.; Abdelbary, B.E.; Gay, J.; Sexton, K. Impact of Hispanic ethnic concentration and socioeconomic status on obesity prevalence in Texas counties. Int. J. Environ. Res. Public Health 2012, 9, 1201–1215. [Google Scholar] [CrossRef] [PubMed]
- Akresh, I.R.; Do, D.P.; Frank, R. Segmented assimilation, neighborhood disadvantage, and Hispanic immigrant health. Soc. Sci. Med. 2016, 149, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Kershaw, K.N.; Albrecht, S.S. Metropolitan-level ethnic residential segregation, racial identity, and body mass index among U.S. Hispanic adults: A multilevel cross-sectional study. BMC Public Health 2014, 14, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Health Statistics. NHANES Survey Methods and Analytic Guidelines. In Questionnaires, Datasets, and Related Documentation; National Center for Health Statistics: Hyattsville, MD, USA, 2020. [Google Scholar]
- Centers for Disease Prevention and Control. Behavioral Risk Factor Surveillance System Overview: BRFSS 2016. In Division of Population Health; Centers for Disease Prevention and Control: Antlanta, GA, USA, 2017. [Google Scholar]
- Frey, W.H. Six Maps that Reveal America’s Expanding Racial Diversity. 2019. Available online: https://www.brookings.edu/research/americas-racial-diversity-in-six-maps/ (accessed on 15 April 2020).
- Fox, R.S.; Mills, S.D.; Roesch, S.C.; Soetrez-Alvarez, D.; Gonzalez, P.; Bekteshi, V.; Cai, J.; Lounsbury, D.W.; Talavera, G.A.; Peneda, F.J.; et al. Perceptions of Cancer Risk/Efficacy and Cancer-Related Risk Behaviors: Results From the HCHS/SOL Sociocultural Ancillary Study. Health Educ. Behav. 2018, 45, 790–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salinas, J.J.; Sexton, K. A border versus non-border comparison of food environment, poverty, and ethnic composition in Texas urban settings. Front. Public Health 2015, 3, 63. [Google Scholar] [CrossRef] [Green Version]
- Salinas, J.J.; Abdelbary, B.; Klaas, K.; Tapia, B.; Sexton, K. Socioeconomic context and the food landscape in Texas: Results from hotspot analysis and border/non-border comparison of unhealthy food environments. Int. J. Environ. Res. Public Health 2014, 11, 5640–5650. [Google Scholar] [CrossRef]
- Census Bureau. Data Profiles 2015, American Community Survey; Census Bureau: Hetland, MA, USA, 2016.
- STATA ME16. Stata Corporation; Statacorp LLC: College Station, TX, USA, 2018. [Google Scholar]
- ESRI. ArcGIS. ArcMap 10.7.1; ESRI: Redlands, CA, USA, 2019. [Google Scholar]
- Foster, B.A.; Maness, T.M.; Aquino, C.A. Trends and Disparities in the Prevalence of Childhood Obesity in South Texas between 2009 and 2015. J. Obes. 2017, 1424968. [Google Scholar] [CrossRef]
- Kirby, J.B.; Liang, L.; Chen, H.J.; Wang, Y. Race, place, and obesity: The complex relationships among community racial/ethnic composition, individual race/ethnicity, and obesity in the United States. Am. J. Public Health 2012, 102, 1572–1578. [Google Scholar] [CrossRef]
- Forrest, K.Y.; Leeds, M.J.; Ufelle, A.C. Epidemiology of Obesity in the Hispanic Adult Population in the United States. Fam. Community Health 2017, 40, 291–297. [Google Scholar] [CrossRef]
- Li, K.; Wen, M.; Henry, K.A. Ethnic density, immigrant enclaves, and Latino health risks: A propensity score matching approach. Soc. Sci. Med. 2017, 189, 44–52. [Google Scholar] [CrossRef]
- Murphy, J.E.; Smock, L.; Hunter-Adams, J. Relationships between English Language Proficiency, Health Literacy, and Health Outcomes in Somali Refugees. J. Immigr. Minor. Health 2019, 21, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.L.; Moy, K.H.; Yoshikawa, H. Perceived ethnic and language-based discrimination and Latina immigrant women’s health. J. Health Psychol. 2017, 22, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, M.; Asti, L.; Nacion, K.M.; Chisolm, D.J. The Role of Health Literacy in Predicting Multiple Healthcare Outcomes among Hispanics in a Nationally Representative Sample: A Comparative Analysis by English Proficiency Levels. J. Immigr. Minor. Health 2016, 18, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.J.; de Heer, H.D.; Lapeyrouse, L.M.; Heyman, J.M.; Balcázar, H.G. Insurance Status Is a Greater Barrier Than Income or Acculturation to Chronic Disease Screening in the Mexican Origin Population in El Paso, Texas. Hisp. Health Care Int. 2015, 13, 197–208. [Google Scholar] [CrossRef]
- Salinas, J.J.; Hilfinger-Messias, D.K.; Morales-Campos, D.; Parra-Medina, D. English language proficiency and physical activity among Mexican-origin women in South Texas and South Carolina. J. Health Care Poor Underserved 2014, 25, 357–375. [Google Scholar] [CrossRef] [Green Version]
- Salinas, J.J.; Sheffield, K.M. English language use, health and mortality in older Mexican Americans. J. Immigr. Minor. Health 2011, 13, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Santos-Lozada, A.R.; Martinez, M.J. How Have You Been? or Como estás: Does Language of Interview Influences Self-Rated Health Among Hispanic Subgroups? J. Immigr. Minor. Health 2018, 20, 766–775. [Google Scholar] [CrossRef]
- Do, D.P.; Frank, R.; Zheng, C.; Iceland, J. Hispanic Segregation and Poor Health: It’s Not Just Black and White. Am. J. Epidemiol. 2017, 186, 990–999. [Google Scholar] [CrossRef]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Mary, T.; Bassett, M.T. Structural Racism and Health Inequities in the USA: Evidence and Interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Becerra, B.J.; Arias, D.; Becerra, M.B. Low Health Literacy among Immigrant Hispanics. J. Racial Ethn. Health Disparities 2017, 4, 480–483. [Google Scholar] [CrossRef]
- Alba, R.; Deane, G.; Denton, N.; Disha, I.; McKenzie, B.; Napierala, J. The role of immigrant enclaves for Latino residential inequalities. J. Ethn. Migr. Stud. 2014, 40, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.J.; Su, D.; Al, S. Border health in the shadow of the Hispanic paradox: Issues in the conceptualization of health disparities in older Mexican Americans living in the Southwest. J. Cross Cult. Gerontol. 2013, 28, 251–266. [Google Scholar] [CrossRef] [PubMed]
- López-Cevallos, D.F.; Gonzalez, P.; Bethel, J.W. Is there a link between wealth and cardiovascular disease risk factors among Hispanic/Latinos? Results from the HCHS/SOL sociocultural ancillary study. Ethn. Health 2018, 23, 902–913. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Solet, D. Disparities in obesity rates: Analysis by ZIP code area. Soc. Sci. Med. 2007, 65, 2458–2463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Fakhouri, T.H.; Carroll, M.D. Prevalence of Obesity among Adults, by Household Income and Education-United States, 2011–2014. MMWR Morb. Mortal. Wkly Rep. 2017, 66, 1369–1373. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Fakhouri, T.H. Prevalence of Obesity among Youths by Household Income and Education Level of Head of Household-United States 2011–2014. MMWR Morb. Mortal. Wkly Rep. 2018, 67, 186–189. [Google Scholar] [CrossRef]
- Kim, D.; Wang, F.; Arcan, C. Geographic Association between Income Inequality and Obesity among Adults in New York State. Prev. Chronic. Dis. 2018, 15, E123. [Google Scholar] [CrossRef] [Green Version]
- Rogers, R.; Eagle, T.F.; Sheetz, A. The Relationship between Childhood Obesity, Low Socioeconomic Status, and Race/Ethnicity: Lessons from Massachusetts. Child. Obes. 2015, 11, 691–695. [Google Scholar] [CrossRef]
- Oddo, V.M.; Walkinshaw, L.P.; Jones-Smith, J.C. Casino Ownership and Health-Related Community Resources Among Native American Tribes in California. Prev. Chronic Dis. 2019, 16, E14. [Google Scholar] [CrossRef] [Green Version]
- Jones-Smith, J.C.; Dow, W.H.; Chichlowska, K. Association between casino opening or expansion and risk of childhood overweight and obesity. JAMA 2014, 311, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Aoki, Y.; Ogden, C.L. Differences in Obesity Prevalence by Demographic Characteristics and Urbanization Level Among Adults in the United States, 2013–2016. JAMA 2018, 319, 2419–2429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, D.R.; Fischer, H.; Arterburn, D. Associations of overweight/obesity and socioeconomic status with hypertension prevalence across racial and ethnic groups. J. Clin. Hypertens. (Greenwich) 2018, 20, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Jayawardene, W.P.; Lohrmann, D.K.; Dickinson, S.; Torabi, M.R. Population-Level Measures to Predict Obesity Burden in Public Schools: Looking Upstream for Midstream Actions. Am. J. Health Promot. 2018, 32, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Vital signs: State-specific obesity prevalence among adults–United States, 2009. MMWR Morb. Mortal. Wkly Rep. 2010, 59, 951–955. [Google Scholar]
- Smith, K.V.; Goldman, N. Socioeconomic differences in health among older adults in Mexico. Soc. Sci. Med. 2007, 65, 1372–1385. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Education. Public High School Graduation Rates. In The Condition of Education 2019; U.S. Department of Education: Washington, DC, USA, 2019; pp. 1–7. [Google Scholar]
- National Education Association. Hispanics: Education Issues. Available online: http://www.nea.org/home/HispanicsEducation%20Issues.htm (accessed on 18 April 2020).
- Santos, R.; Huerta, G.; Karki, M.; Cantarero, A. Social Determinants of Overweight and Obesity Rates by Elementary School in a Predominantly Hispanic School District. J. Pediatr. Nurs. 2017, 37, 8–12. [Google Scholar] [CrossRef]
- Centers for Disease Prevention and Control (CDC). About the National Health and Nutrition Examination Survey. National Center for Health Statistics 2017. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 21 April 2020).
- Office of Disease Prevention and Health Promotion (ODPHP). Behavioral Risk Factor Surveillance System. Data Sources 2020. Available online: https://www.healthypeople.gov/2020/data-source/behavioral-risk-factor-surveillance-system (accessed on 22 April 2020).



{kind=link}
{kind=link}
| Models | Coefficient | p-Value | Adjusted R2 |
|---|---|---|---|
| Unadjusted | 2.56 | 0.000 | 0.27 |
| Full | 0.097 | 0.863 | 0.50 |
| Economic | |||
| Poverty | 2.30 | 0.000 | 0.27 |
| Median Income | 1.33 | 0.002 | 0.34 |
| % Homeowner | 2.57 | 0.000 | 0.26 |
| Ethnicity | |||
| % Immigrant | 2.85 | 0.000 | 0.28 |
| % Limited English | 3.01 | 0.000 | 0.31 |
| Demographic | |||
| Total Population | 2.53 | 0.000 | 0.27 |
| Median Age | 2.59 | 0.000 | 0.28 |
| High School Graduation | 1.71 | 0.001 | 0.29 |
| Health Insurance Coverage | 2.19 | 0.000 | 0.27 |
| % Walking Commuter | 2.48 | 0.000 | 0.27 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salinas, J.J.; Sheen, J.; Carlyle, M.; Shokar, N.K.; Vazquez, G.; Murphy, D.; Alozie, O. Using Electronic Medical Record Data to Better Understand Obesity in Hispanic Neighborhoods in El Paso, Texas. Int. J. Environ. Res. Public Health 2020, 17, 4591. https://doi.org/10.3390/ijerph17124591
Salinas JJ, Sheen J, Carlyle M, Shokar NK, Vazquez G, Murphy D, Alozie O. Using Electronic Medical Record Data to Better Understand Obesity in Hispanic Neighborhoods in El Paso, Texas. International Journal of Environmental Research and Public Health. 2020; 17(12):4591. https://doi.org/10.3390/ijerph17124591
Chicago/Turabian StyleSalinas, Jennifer J., Jon Sheen, Malcolm Carlyle, Navkiran K. Shokar, Gerardo Vazquez, Daniel Murphy, and Ogechika Alozie. 2020. "Using Electronic Medical Record Data to Better Understand Obesity in Hispanic Neighborhoods in El Paso, Texas" International Journal of Environmental Research and Public Health 17, no. 12: 4591. https://doi.org/10.3390/ijerph17124591
APA StyleSalinas, J. J., Sheen, J., Carlyle, M., Shokar, N. K., Vazquez, G., Murphy, D., & Alozie, O. (2020). Using Electronic Medical Record Data to Better Understand Obesity in Hispanic Neighborhoods in El Paso, Texas. International Journal of Environmental Research and Public Health, 17(12), 4591. https://doi.org/10.3390/ijerph17124591