A Three-Arm Randomised Controlled Trial of High- and Low-Intensity Implementation Strategies to Support Centre-Based Childcare Service Implementation of Nutrition Guidelines: 12-Month Follow-Up

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
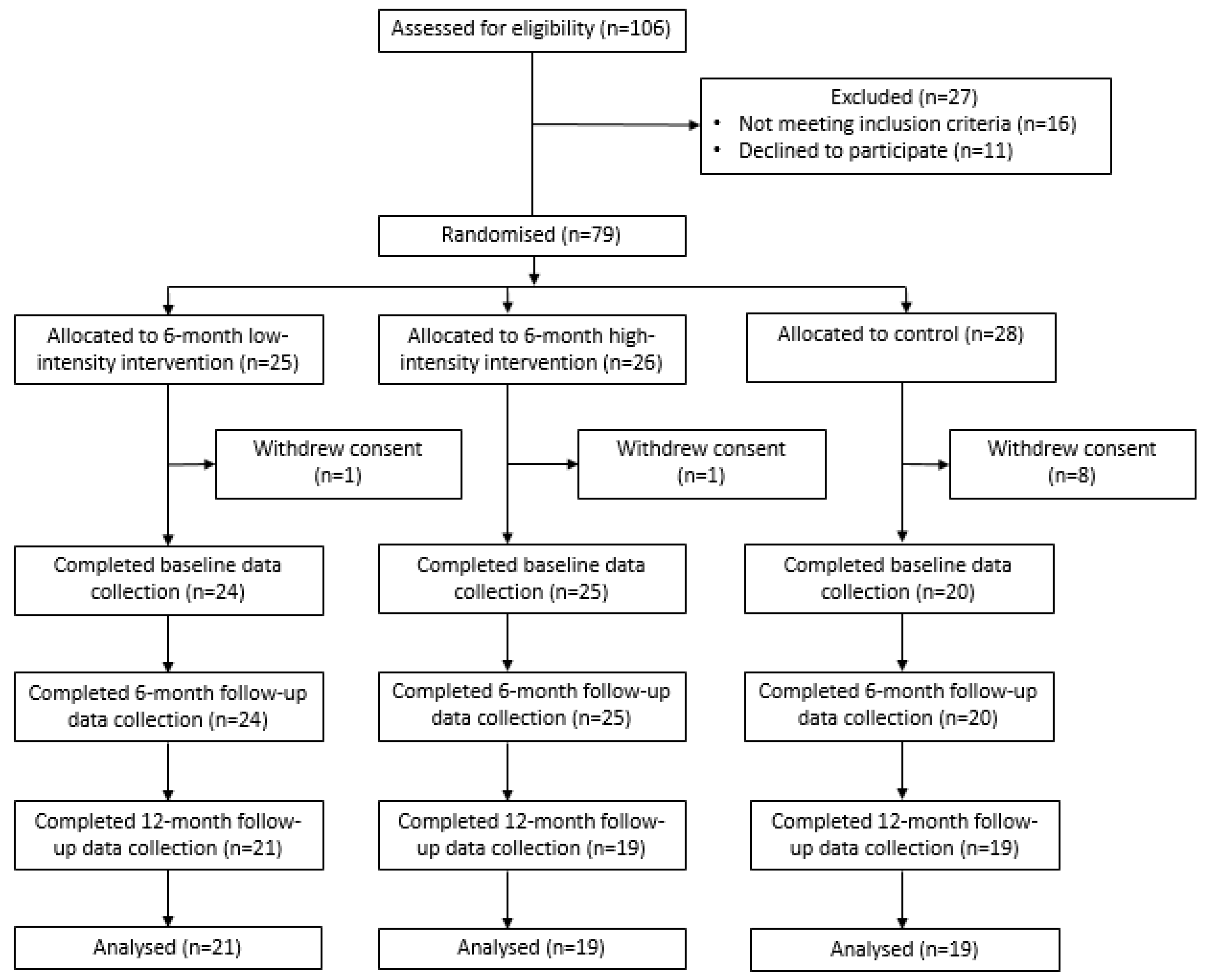
2.2. Design and Setting
2.2.1. Participants
2.2.2. Recruitment Procedures
2.2.3. Randomisation and Allocation
2.3. Interventions
2.3.1. Intervention Development
2.3.2. Implementation Strategies
2.3.3. Control Group
2.4. Measures
2.4.1. Primary Outcomes: Compliance with Nutrition Guidelines
- Overall compliance with nutrition guidelines. Overall menu compliance was defined as the proportion of services providing the minimum recommended number of servings according to the nutrition guidelines for all five AGHE food groups for every child, every day over a two-week menu (10 days).
- Compliance with nutrition guidelines for individual food groups. Individual food group compliance was defined as the proportion of services providing the minimum recommended number of servings compliant with the nutrition guidelines for each of the five individual AGHE food groups, plus discretionary foods, for every child, every day over a two-week menu (10 days). The nutrition guidelines for the sector recommend childcare services do not provide discretionary foods. In order to be deemed compliant a service needed to have zero discretionary foods on the menu (i.e., if a service provided any discretionary foods on the two-week menu, they were not deemed as compliant).
- 3.
- Menu compliance score (mean number of individual food groups compliant). A score for menu compliance was calculated by summing the number of food groups and discretionary foods provided in sufficient quantity to meet guideline recommendations for each service. Scores could range between 0 and 6, with a score of 1 allocated for each of the five AGHE food groups and discretionary foods that were compliant (e.g., if a service provided adequate servings for all food groups, including zero discretionary foods, they scored a 6).
- 4.
- Mean number of servings of each individual food group provided. The mean number of servings of each AGHE food group and discretionary foods provided on the menu was assessed.
2.4.2. Childcare Service Operational Characteristics
2.4.3. Service Cook Demographics
2.4.4. Sample Size and Power Calculations
2.5. Statistical Analyses
3. Results
3.1. Primary Outcomes at 12 Months
3.1.1. Overall Compliance with Nutrition Guidelines
3.1.2. Compliance with Nutrition Guidelines for Individual Food Groups
- Group interaction: significant differences in the proportion of services compliant with individual food groups were found between groups for vegetables; fruit; breads and cereals; dairy; and discretionary food (Table 3). Following multiple imputation, the difference in compliance for breads and cereals was no longer statistically significant.
- Low-intensity vs. control: relative to control, a significantly greater proportion of services allocated to the low-intensity intervention were compliant for the dairy food group (Table 3). Multiple imputation did not result in any changes to statistical significance for these analyses.
- High-intensity vs. control: relative to control, a significantly greater proportion of services allocated to the high-intensity intervention were compliant for five of the six food groups (vegetables; fruit; breads and cereals; dairy; and discretionary food) (Table 3). Following multiple imputations, the difference in compliance for breads and cereals was no longer statistically significant (odds ratio (OR) = 6.98; 95% confidence interval (CI): 0.72, 67.24; p = 0.09).
- Low-intensity vs. high-intensity: pairwise comparisons indicated there was no significant difference between the high- and low-intensity interventions for compliance with any food group (Table 3). Multiple imputation did not result in any changes to statistical significance for these analyses.
3.1.3. Menu Compliance Score (Mean Number of Individual Food Groups Compliant)
- Group interaction: a significant difference in the mean number of food groups compliant with guidelines was found between groups (Table 4).
- Low-intensity vs. control: relative to control, a significantly greater number of food groups were compliant with guidelines in the low-intensity intervention services (Table 4).
- High-intensity vs. control: relative to control, a significantly greater number of food groups were compliant with guidelines in the high-intensity intervention services (Table 4).
- Low-intensity vs. high-intensity: pairwise comparisons indicated there was no significant difference between the high- and low-intensity interventions for the mean number of food groups compliant on the menu (Table 4).
- Multiple imputation did not result in any changes to statistical significance for these analyses.
3.1.4. Servings of Individual Food Groups
- Group interaction: significant differences in the servings of individual food groups were found between groups for vegetables; fruit; dairy; and discretionary (Table 4).
- Low-intensity vs. control: relative to control, a significant increase in servings of fruit; dairy; and discretionary was found in the low-intensity intervention (Table 4).
- High-intensity vs. control: relative to control, a significant increase in servings of four out of six food groups (vegetables; fruit; dairy; and discretionary) was found in the high-intensity intervention (Table 4).
- Low-intensity vs. high-intensity: pairwise comparisons indicated there was a significant difference between the high- and low-intensity interventions for servings of vegetables (Table 4).
- Multiple imputation did not result in any changes to statistical significance for these analyses.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017, A systematic analysis for the global burden of disease study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Mikkila, V.; Rasanen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Longitudinal changes in diet from childhood into adulthood with respect to risk of cardiovascular diseases: The cardiovascular risk in young finns study. Eur. J. Clin. Nutr. 2004, 58, 1038–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waxman, A. Prevention of chronic diseases: Who global strategy on diet, physical activity and health. Food Nutr. Bull. 2003, 24, 281–284. [Google Scholar] [CrossRef]
- World Health Organization. Report of the Comminssion on Ending Childhood Obesity. Implementation Plan: Executive Summary; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Mikkelsen, M.V.; Husby, S.; Skov, L.R.; Perez-Cueto, F.J. A systematic review of types of healthy eating interventions in preschools. Nutr. J. 2014, 13, 56. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. 4402.0—Childhood Education and Care, Australia, June 2017. In Statistics; Australian Bureau of Statistics: Canberra, Australia, 2018. [Google Scholar]
- Radcliffe, B.C.; Cameron, C.V.; Baade, P.D. Nutrient intakes for young children: Implications for long-day child-care nutrition recommendations. Nutr. Diet. 2002, 59, 187–190. [Google Scholar]
- Ward, D.S.; Vaughn, A.; Story, M. Expert and stakeholder consensus on priorities for obesity prevention research in early care and education settings. Child. Obes. 2013, 9, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Bell, L.K.; Hendrie, G.A.; Hartley, J.; Golley, R.K. Impact of a nutrition award scheme on the food and nutrient intakes of 2- to 4-year-olds attending long day care. Public Health Nutr. 2015, 18, 2634–2642. [Google Scholar] [CrossRef] [Green Version]
- Australian Government. Australian Government. Australian guide to healthy eating. In Health Do; Government of Australia: Canberra, Australia, 2017. [Google Scholar]
- Benjamin Neelon, S.E.; Briley, M.E. Position of the american dietetic association: Benchmarks for nutrition in child care. J. Am. Diet. Assoc. 2011, 111, 607–615. [Google Scholar] [CrossRef]
- Gerritsen, S.; Dean, B.; Morton, S.M.B.; Wall, C.R. Do childcare menus meet nutrition guidelines? Quantity, variety and quality of food provided in new zealand early childhood education services. Aust. N. Z. J. Public Health 2017, 41, 345–351. [Google Scholar] [CrossRef]
- Grady, A.; Seward, K.; Finch, M.; Fielding, A.; Stacey, F.; Jones, J.; Wolfenden, L.; Yoong, S.L. Barriers and enablers to implementation of dietary guidelines in early childhood education centers in australia: Application of the theoretical domains framework. J. Nutr. Educ. Behav. 2018, 50, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Seward, K.; Finch, M.; Yoong, S.L.; Wyse, R.; Jones, J.; Grady, A.; Wiggers, J.; Nathan, N.; Conte, K.; Wolfenden, L. Factors that influence the implementation of dietary guidelines regarding food provision in centre based childcare services: A systematic review. Prev. Med. 2017, 105, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, S.; Wall, C.; Morton, S. Child-care nutrition environments; results from a survey of policy and practice in New Zealand early childhood education services. Public Health Nutr. 2016, 19, 1531–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyn, R.; Evers, S.; Davis, J.; Maalouf, J.; Griffin, M. Barriers and supports to implementing a nutrition and physical activity intervention in child care: Directors’ perspectoves. J. Nutr. Educ. Behav. 2014, 46, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Wolfenden, L.; Barnes, C.; Jones, J.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Wiggers, J.; Williams, A.J.; Seward, K.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2020, 2, CD011779. [Google Scholar] [CrossRef] [PubMed]
- Seward, K.; Wolfenden, L.; Finch, M.; Wiggers, J.; Wyse, R.; Jones, J.; Yoong, S.L. Improving the implementation of nutrition guidelines in childcare centres improves child dietary intake: Findings of a randomised trial of an implementation intervention. Public Health Nutr. 2017, 21, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morshed, A.; Davis, S.; Keane, P.; Myers, O.; Mishra, S. The impact of the chile intervention on the food served in head start centers in rural New Mexico. J. Sch. Health 2016, 86, 414–423. [Google Scholar] [CrossRef] [Green Version]
- Finch, M.; Seward, K.; Wedesweiler, T.; Stacey, F.; Grady, A.; Jones, J.; Wolfenden, L.; Yoong, S.L. Challenges of increasing childcare center compliance with nutrition guidelines: A randomized controlled trial of an intervention providing training, written menu feedback, and printed resources. Am. J. Health Promot. 2019, 33, 399–411. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better reporting of interventions: Template for intervention description and replication (tidier) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Wolfenden, L.; Yoong, S.L.; Williams, C.M.; Grimshaw, J.; Durrheim, D.N.; Gillham, K.; Wiggers, J. Embedding researchers in health service organizations improves research translation and health service performance: The australian hunter new england population health example. J. Clin. Epidemiol. 2017, 85, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Australian Children’s Education & Care Quality Authority. Guide to the National Quality Framework; ACECQA: Syndey, Australia, 2020.
- Seward, K.; Wolfenden, L.; Finch, M.; Wiggers, J.; Wyse, R.; Jones, J.; Gillham, K.; Yoong, S.L. Multistrategy childcare-based intervention to improve compliance with nutrition guidelines versus usual care in long day care services: A study protocol for a randomised controlled trial. BMJ Open 2016, 6, e010786. [Google Scholar] [CrossRef] [Green Version]
- NSW Ministry of Health. Caring for Children: Birth to 5 Years (Food, Nutrition and Learning Experiences); NSW Health: North Sydney, Australia, 2014.
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, J.; Wyse, R.; Finch, M.; Lecathelinais, C.; Wiggers, J.; Marshall, J.; Falkiner, M.; Pond, N.; Yoong, S.L.; Hollis, J. Effectiveness of an intervention to facilitate the implementation of healthy eating and physical activity policies and practices in childcare services: A randomised controlled trial. Implement. Sci. 2015, 10, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, S.D.; McKenzie, J.E.; O’Connor, D.A.; Grimshaw, J.M.; Mortimer, D.; Francis, J.J.; Michie, S.; Spike, N.; Schattner, P.; Kent, P.; et al. Evaluation of a theory-informed implementation intervention for the management of acute low back pain in general medical practice: The implement cluster randomised trial. PLoS ONE 2013, 8, e65471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, S.D.; Green, S.E.; O’Connor, D.A.; McKenzie, J.E.; Francis, J.J.; Michie, S.; Spike, N.; Schattner, P.; Kent, P.; Buchbinder, R. Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the theoretical domains framework. Implement. Sci. 2012, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Johnston, M.; Francis, J.; Hardeman, W.; Eccles, M. From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Appl. Psychol. 2008, 57, 660–680. [Google Scholar] [CrossRef]
- Huijg, J.M.; Gebhardt, W.A.; Dusseldorp, E.; Verheijden, M.W.; van der Zouwe, N.; Middelkoop, B.J.; van der Zouwe, N.; Middlekoop, B.J.C.; Crone, M.R. Measuring determinants of implementation behavior: Psychometric properties of a questionnaire based on the theoretical domains framework. Implement. Sci. 2014, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Huijg, J.M.; Gebhardt, W.A.; Crone, M.R.; Dusseldorp, E.; Presseau, J. Discriminant content validity of a theoretical domains framework questionnaire for use in implementation research. Implement. Sci. 2014, 9, 11. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Aarons, G.A.; Horwitz, S.; Chamberlain, P.; Hurlburt, M.; Landsverk, J. Mixed method designs in implementation research. Adm. Policy Ment. Health 2011, 38, 44–53. [Google Scholar] [CrossRef] [Green Version]
- Wolfenden, L.; Jones, J.; Williams, C.M.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Wiggers, J.; Williams, A.J.; Seward, K.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2016, 10, CD011779. [Google Scholar] [CrossRef]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.E. A refined compilation of implementation strategies: Results from the expert recommendations for implementing change (eric) project. Implement. Sci. 2015, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Proctor, E.K.; Powell, B.J.; McMillen, J.C. Implementation strategies: Recommendations for specifying and reporting. Implement. Sci. 2013, 8, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsetlund, L.; Bjorndal, A.; Rashidian, A.; Jamtvedt, G.; O’Brien, M.A.; Wolf, F.; Davis, D.; Odgaard-Jensen, J.; Oxman, A.D. Continuing education meetings and workshops: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2009, 2009, CD003030. [Google Scholar] [CrossRef] [PubMed]
- Joyce, B.; Showers, B. Improving in-service training: The messsages from research. Educ. Leadersh. 1980, 37, 6. [Google Scholar]
- Bero, L.A.; Grilli, R.; Grimshaw, J.M.; Harvey, E.; Oxman, A.D.; Thomson, M.A. Closing the gap between research and practice: An overview of systematic reviews of interventions to promote the implementation of research findings. The cochrane effective practice and organization of care review group. BMJ 1998, 317, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Read, C.; Kleiner, B. Which training methods are effective? Manag. Dev. Rev. 1996, 9, 24–29. [Google Scholar] [CrossRef]
- Ivers, N.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.D.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2012, CD000259. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Soumerai, S.B.; Avorn, J. Principles of educational outreach (‘academic detailing’) to improve clinical decision making. JAMA 1990, 263, 549–556. [Google Scholar] [CrossRef]
- Jones, R.A.; Riethmuller, A.; Hesketh, K.; Trezise, J.; Batterham, M.; Okely, A.D. Promoting fundamental movement skill development and physical activity in early childhood settings: A cluster randomized controlled trial. Pediatric Exerc. Sci. 2011, 23, 600–615. [Google Scholar] [CrossRef]
- NSW Department of Health. About Munch & Move 2019. Available online: https://www.healthykids.nsw.gov.au/campaigns-programs/about-munch-move.aspx (accessed on 19 June 2019).
- Ginani, V.C. Methods, instruments, and parameters for analyzing the menu nutritionally and sensorially: A systematic review. J. Culin. Sci. Technol. 2012, 10, 294–310. [Google Scholar] [CrossRef]
- Dodds, P.; Wyse, R.; Jones, J.; Wolfenden, L.; Lecathelinais, C.; Williams, A.; Yoong, S.L.; Finch, M.; Nathan, N.; Gillham, K. Validity of a measure to assess healthy eating and physical activity policies and practices in australian childcare services. BMC Public Health 2014, 14, 572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finch, M.; Wolfenden, L.; Falkiner, M.; Edenden, D.; Pond, N.; Hardy, L.L.; Milat, J.A.; Wiggers, J. Impact of a population based intervention to increase the adoption of multiple physical activity practices in centre based childcare services: A quasi experimental, effectiveness study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Bureau of Statistics. 2033.0.55.001—Census of population and housing: Socio-economic indexes for areas (seifa), Australia 2016. In Statistics; Australian Bureau of Statistics: Canberra, Australia, 2016. [Google Scholar]
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS); Australian Bureau of Statistics: Canberra, Australia, 2018.
- Maalouf, J.; Evers, S.C.; Griffin, M.; Lyn, R. Assessment of mealtime environments and nutrition practices in child care centers in georgia. Child. Obes. 2013, 9, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Jennings, A.; McEvoy, S.; Corish, C. Nutritional practices in full-day-care pre-schools. J. Hum. Nutr. Diet. 2011, 24, 245–259. [Google Scholar] [CrossRef] [PubMed]
- Strecher, V.J.; Seijts, G.H.; Kok, G.J.; Latham, G.P.; Glasgow, R.; DeVellis, B.; Meertens, R.M.; Bulger, D.W. Goal setting as a strategy for health behavior change. Health Educ. Q. 1995, 22, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Buttivant, H.; Knai, C. Improving food provision in child care in england: A stakeholder analysis. Public Health Nutr. 2011, 15, 554–560. [Google Scholar] [CrossRef] [Green Version]
- Yoong, S.L.; Grady, A.; Wiggers, J.; Flood, V.; Rissel, C.; Finch, M.; Searles, A.; Salajan, D.; O’Rourke, R.; Daly, J. A randomised controlled trial of an online menu planning intervention to improve childcare service adherence to dietary guidelines: A study protocol. BMJ Open 2017, 7, e017498. [Google Scholar] [CrossRef]
- Grady, A.; Wolfenden, L.; Rissel, C.; Green, S.; Reilly, K.; Yoong, S.L. Effectiveness of a dissemination strategy on the uptake of an online menu planning program: A controlled trial. Health Promot. J. Aust. 2019, 30, 20–25. [Google Scholar] [CrossRef]
- Wolfenden, L.; Nathan, N.; Janssen, L.M.; Wiggers, J.; Reilly, K.; Delaney, T.; Williams, C.M.; Bell, C.; Wyse, R.; Sutherland, R.; et al. Multi-strategic intervention to enhance implementation of healthy canteen policy: A randomised controlled trial. Implement. Sci. 2017, 12, 6. [Google Scholar] [CrossRef] [Green Version]
- Nathan, N.; Wolfenden, L.; Bell, A.C.; Wyse, R.; Morgan, P.J.; Butler, M.; Sutherland, R.; Milat, J.A.; Hector, D.; Wiggers, J. Effectiveness of a multi-strategy intervention in increasing the implementation of vegetable and fruit breaks by australian primary schools: A non-randomized controlled trial. BMC Public Health 2012, 12, 651. [Google Scholar] [CrossRef] [Green Version]
- Yoong, S.L.; Nathan, N.; Wolfenden, L.; Wiggers, J.; Reilly, K.; Oldmeadow, C.; Wyse, R.; Sutherland, R.; Delaney, T.; Butler, P.; et al. Café: A multicomponent audit and feedback intervention to improve implementation of healthy food policy in primary school canteens: A randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and strategies in guideline implementation-a scoping review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hesnley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implement. Sci. 2015, 10, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proschan, M.A. A multiple comparison procedure for three- and four-armed controlled clinical trials. Stat. Med. 1999, 18, 787–798. [Google Scholar] [CrossRef]
- Cook, R.J.; Farewell, V.T. Multiplicity considerations in the design and analysis of clinical trials. J. R. Stat. Soc. Ser. A (Statistics in Society) 1996, 159, 93–110. [Google Scholar] [CrossRef]
- Committee For Proprietary Medicinal Products (CPMP). Points to Consider on Multiplicity Issues in Clinical Trials (cpmp/ewp/908/99); The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use: London, UK, 2002. [Google Scholar]
- Freidlin, B.; Korn, E.L.; Gray, R.; Martin, A. Multi-arm clinical trials of new agents: Some design considerations. Clin. Cancer Res. 2008, 14, 4368–4371. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.H.; George, S.L. Between-arm comparisons in randomized phase ii trials. J. Biopharm. Stat. 2009, 19, 456–468. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Implementation Strategy | Description according to ERIC a [35] | Application within the Interventions according to Proctor [36] | Low- Intensity [20] | High-Intensity [18] |
|---|---|---|---|---|
| Provision of staff training [37,38,39,40] | Conduct educational meetings: hold meetings targeted toward different stakeholder groups (e.g., providers, administrators, other organizational stakeholders, and community, patient/consumer, and family stakeholders) to teach them about the innovation. | Actor: implementation support officer. Action: A one-day face-to-face menu-planning workshop was provided to service managers and cooks with the aim to improve their knowledge and skills in the application of nutrition guidelines to food preparation and provision. The workshop incorporated both didactic and interactive components including small group discussions, case studies, problem-solving and idea sharing, facilitator feedback and opportunities to practice planning a menu in accordance with guidelines. Experienced implementation support officers and dietitians facilitated the workshop. Target: service managers and cooks. Temporality: one-day face-to-face training workshop at intervention commencement (one week). Dose: One-off workshop. | ✓ | ✓ |
| Provision of resources [25] | Distribute educational materials: distribute educational materials (including guidelines, manuals, and toolkits) in person, by mail, and/or electronically. | Actor: implementation support officer. Action: all intervention services received a resource pack which included the Caring for Children resource [25], menu planning checklists, recipe ideas, budgeting fact sheets, and goal setting and action planning templates, to support guideline implementation. Target: service managers and cooks. Temporality: provided during the one-day face-to-face training workshop at intervention commencement (one week). Dose: one-off provision of resource pack, which could be accessed on an ongoing basis over the six month intervention period. | ✓ | ✓ |
| Audit and feedback [41] | Audit and provide feedback: collect and summarize clinical performance data over a specified time period and give it to providers to monitor, evaluate, and modify provider behaviour. | Actor: trained dietitian. Action: a trained dietitian completed an audit of services two-week menu, with written feedback via email (high-intensity and low-intensity) and verbal feedback via face-to-face support visits (high-intensity only) provided to service managers and cooks. Feedback included overall menu and individual food group compliance with nutrition guidelines, servings of each food group per child per day, and tips for increasing menu compliance. Target: service managers and cooks. Temporality: high-intensity—immediately post-baseline data collection and at three months; low-intensity—immediately post-baseline data collection. Dose: high intensity—twice within the first three months of the intervention period; low intensity—once within the first three months of the intervention period. | ✓ (once, written only) | ✓ (twice, written and verbal) |
| Implementation support [42,43] | Provide ongoing consultation: provide ongoing consultation with one or more experts in the strategies used to support implementing the innovation. | Actor: implementation support officer. Action: services were each allocated an implementation support officer to provide tailored and expert advice and assistance to facilitate guideline implementation. Each implementation support officer offered two face-to-face support visits with the service manager and cook, at the service, following the menu planning workshop. In addition, two newsletters were distributed to services. Target: service managers and cooks. Temporality: face-to-face contacts made at two-four weeks following workshop and at three months; newsletters distributed at three months and five months. Dose: twice during the six month intervention period. | X | ✓ |
| Securing executive support [44] | Obtain formal commitments: obtain written commitments from key partners that state what they will do to implement the innovation. Mandate change: have leadership declare the priority of the innovation and their determination to have it implemented. | Actor: implementation support officer, service manager. Action: a memorandum of understanding, detailing each party’s responsibilities to implement the nutrition guidelines and participate in the intervention was signed by the implementation support officer, the service manager and the service cook. Service managers were encouraged to communicate support and endorsement of nutrition guideline adherence to other service staff and to update the service nutrition policy accordingly (if required). Targets: service managers, cooks, service staff. Temporality: memorandum of understanding signed within the face-to-face meeting at two–four weeks post workshop. Dose: one-off memorandum of understanding during the first face-to-face contact; ongoing communication of support and endorsement of the guidelines throughout the six months of the intervention period. | X | ✓ |
| Characteristic | Low Intensity (N = 24) n (%) | High Intensity (N = 25) n (%) | Control (N = 20) n (%) |
|---|---|---|---|
| Service operational characteristics | |||
| Average no. of children the service provides food for each day (mean (SD)) | 54.9 (17.7) | 62.4 (23.1) | 53.6 (19.9) |
| Services in high socioeconomic area | 7 (29.2) | 10 (40.0) | 4 (20.0) |
| Service location | |||
| Major city + inner regional | 20 (83.3) | 23 (92.0) | 17(85.0) |
| Outer regional/remote Australia | 4 (16.6) | 2 (8.0) | 2 (10.0) |
| Service cook characteristics | |||
| University or Technical and Further Education (TAFE) qualification | 13 (54.2) | 13 (52.0) | 18 (90.0) * |
| <40 years of age | 9 (42.9) a | 7 (29.2) b | 5 (26.3) c |
| >5 years employed within the childcare setting | 10 (43.5) d | 9 (37.5) b | 7 (35.0) |
| Works ≤20 h per week | 4 (17.4) d | 2 (8.0) | 5 (25.0) |
| Outcome | Baseline | 12-Month Follow-Up | Group Interaction Analysis | Low-Intensity vs. Control Pairwise Analysis | High-intensity vs. Control Pairwise Analysis | Low-intensity vs. High-Intensity Pairwise Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Compliance | Low Intensity (N = 24) n (%) | High Intensity (N = 25) n (%) | Control (N = 20) n (%) | Low Intensity (N = 21) n (%) | High Intensity (N = 19) n (%) | Control (N = 19) n (%) | p-Value | Odds Ratio (95% Confidence Interval (CI)) | p-Value | Odds Ratio (95%CI) | p-Value | Odds Ratio (95%CI) | p-Value |
| Overall compliance (5/5 food groups) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 3 (15.8) | 0 (0) | - | - | - | - | - | - | - |
| Compliance with individual food groups | |||||||||||||
| Vegetables | 0 (0) | 0 (0) | 0 (0) | 3 (14.3) | 6 (31.6) | 0 (0) | 0.02 | 3.77 (0.55;∞) | 0.27 | 10.74 [1.87;∞] | 0.02 | 2.70 [0.47;19.82] | 0.35 |
| Fruit | 1 (4.2) | 4 (16.0) | 5 (25.0) | 6 (28.6) | 10 (52.6) | 1 (5.3) | <0.01 | 7.74 [0.76;408.41] | 0.10 | 18.95 [2.13;944.77] | <0.01 | 2.44 [0.56;11.37] | 0.29 |
| Breads and Cereals | 4 (16.7) | 3 (12.0) | 2 (10.0) | 5 (23.8) | 5 (26.3) | 0 (0) | <0.05 | 7.42 [1.26;∞] | 0.06 | 8.42 [1.42;∞] | 0.04 | 1.15 [0.22;6.10] | 1.00 |
| Meat/meat alternatives | 0 (0) | 1 (4.0) | 0 (0) | 4 (19.1) | 4 (21.1) | 1 (5.3) | 0.32 | 4.10 [0.36;219.93] | 0.41 | 4.93 [0.43;267.03] | 0.31 | 1.21 [0.19;7.79] | 1.00 |
| Dairy | 9 (37.5) | 10 (40.0) | 5 (25.0) | 9 (42.9) | 13 (68.4) | 1 (5.3) | <0.01 | 12.20 [1.37;601.68] | 0.02 | 31.49 [3.47;1596.22] | <0.01 | 2.67 [0.62;12.64] | 0.23 |
| Discretionary | 3 (12.5) | 0 (0) | 0 (0) | 7 (33.3) | 11 (57.9) | 2 (10.5) | <0.01 | 2.37 [0.29;29.90] | 0.61 | 10.86 [1.77;123.66] | <0.01 | 4.60 [0.95;26.95] | 0.06 |
| Outcome | Baseline | 12-Month Follow-Up | Group Interaction Analysis | Low-Intensity vs. Control Pairwise Analysis | High-Intensity vs. Control Pairwise Analysis | Low-Intensity vs. High-Intensity Pairwise Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Measure | Low Intensity (N = 24) Mean (SD) | High Intensity (N = 25) Mean (SD) | Control (N = 20) Mean (SD) | Low Intensity (N = 21) Mean (SD) | High Intensity (N = 19) Mean (SD) | Control (N = 19) Mean (SD) | p-Value | Mean Difference (95%CI) | p-Value | Mean Difference (95%CI) | p-Value | Mean Difference (95%CI) | p-Value |
| Number of food groups compliant | 0.71 (0.95) | 0.72 (0.79) | 0.60 (0.88) | 1.62 (1.53) | 2.58 (1.98) | 0.26 (0.56) | <0.01 | 1.35 [0.40;2.30] | <0.01 | 2.29 [1.32;3.26] | <0.01 | 0.94 [−0.01;21.89] | 0.05 |
| Servings of individual food groups | |||||||||||||
| Vegetables | 1.48 (0.54) | 1.18 (0.50) | 1.05 (0.57) | 1.77 (0.67) | 2.36 (0.92) | 1.32 (0.64) | <0.01 | 0.36 [−0.14;0.88] | 0.17 | 0.98 [0.48;1.48] | <0.01 | 0.62 [0.14;1.10] | 0.01 |
| Fruit | 0.77 (0.19) | 0.83 (0.51) | 0.91 (0.45) | 1.06 (0.36) | 1.18 (0.33) | 0.86 (0.28) | <0.01 | 0.22 [0.01;0.43] | 0.04 | 0.34 [0.13;0.55] | <0.01 | 0.11 [−0.09;0.32] | 0.27 |
| Breads and Cereals | 2.17 (0.54) | 2.00 (0.65) | 2.13 (0.72) | 2.37 (0.75) | 2.34 (0.46) | 2.20 (0.74) | 0.64 | 0.17 [−0.24;0.58] | 0.41 | 0.17 [−0.25;0.59] | 0.42 | 0.00 [−0.41;0.41] | 0.99 |
| Meat/meat alternatives | 0.54 (0.12) | 0.55 (0.23) | 0.50 (0.18) | 0.70 (0.19) | 0.78 (0.18) | 0.63 (0.23) | 0.21 | 0.05 [−0.07;0.18] | 0.39 | 0.12 [−0.01;0.25] | 0.08 | 0.06 [−0.06;0.19] | 0.32 |
| Dairy | 1.21 (0.36) | 1.19 (0.43) | 1.13 (0.54) | 1.36 (0.39) | 1.39 (0.29) | 0.92 (0.32) | <0.01 | 0.43 [0.21;0.65] | <0.01 | 0.47 [0.24;0.69] | <0.01 | 0.04 [−0.18;0.25] | 0.75 |
| Discretionary | 0.60 (0.45) | 0.63 (0.44) | 0.65 (0.35) | 0.25 (0.31) | 0.13 (0.21) | 0.68 (0.42) | <0.01 | −0.41 [−0.60;−0.22] | <0.01 | −0.50 [−0.69;−0.31] | <0.01 | −0.09 [−0.28;0.10] | 0.34 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grady, A.; Seward, K.; Finch, M.; Wolfenden, L.; Wyse, R.; Wiggers, J.; Lecathelinais, C.; Yoong, S.L. A Three-Arm Randomised Controlled Trial of High- and Low-Intensity Implementation Strategies to Support Centre-Based Childcare Service Implementation of Nutrition Guidelines: 12-Month Follow-Up. Int. J. Environ. Res. Public Health 2020, 17, 4664. https://doi.org/10.3390/ijerph17134664
Grady A, Seward K, Finch M, Wolfenden L, Wyse R, Wiggers J, Lecathelinais C, Yoong SL. A Three-Arm Randomised Controlled Trial of High- and Low-Intensity Implementation Strategies to Support Centre-Based Childcare Service Implementation of Nutrition Guidelines: 12-Month Follow-Up. International Journal of Environmental Research and Public Health. 2020; 17(13):4664. https://doi.org/10.3390/ijerph17134664
Chicago/Turabian StyleGrady, Alice, Kirsty Seward, Meghan Finch, Luke Wolfenden, Rebecca Wyse, John Wiggers, Christophe Lecathelinais, and Sze Lin Yoong. 2020. "A Three-Arm Randomised Controlled Trial of High- and Low-Intensity Implementation Strategies to Support Centre-Based Childcare Service Implementation of Nutrition Guidelines: 12-Month Follow-Up" International Journal of Environmental Research and Public Health 17, no. 13: 4664. https://doi.org/10.3390/ijerph17134664
APA StyleGrady, A., Seward, K., Finch, M., Wolfenden, L., Wyse, R., Wiggers, J., Lecathelinais, C., & Yoong, S. L. (2020). A Three-Arm Randomised Controlled Trial of High- and Low-Intensity Implementation Strategies to Support Centre-Based Childcare Service Implementation of Nutrition Guidelines: 12-Month Follow-Up. International Journal of Environmental Research and Public Health, 17(13), 4664. https://doi.org/10.3390/ijerph17134664