Interactions among Obstructive Sleep Apnea Syndrome Severity, Sex, and Obesity on Circulatory Inflammatory Biomarkers in Patients with Suspected Obstructive Sleep Apnea Syndrome: A Retrospective, Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
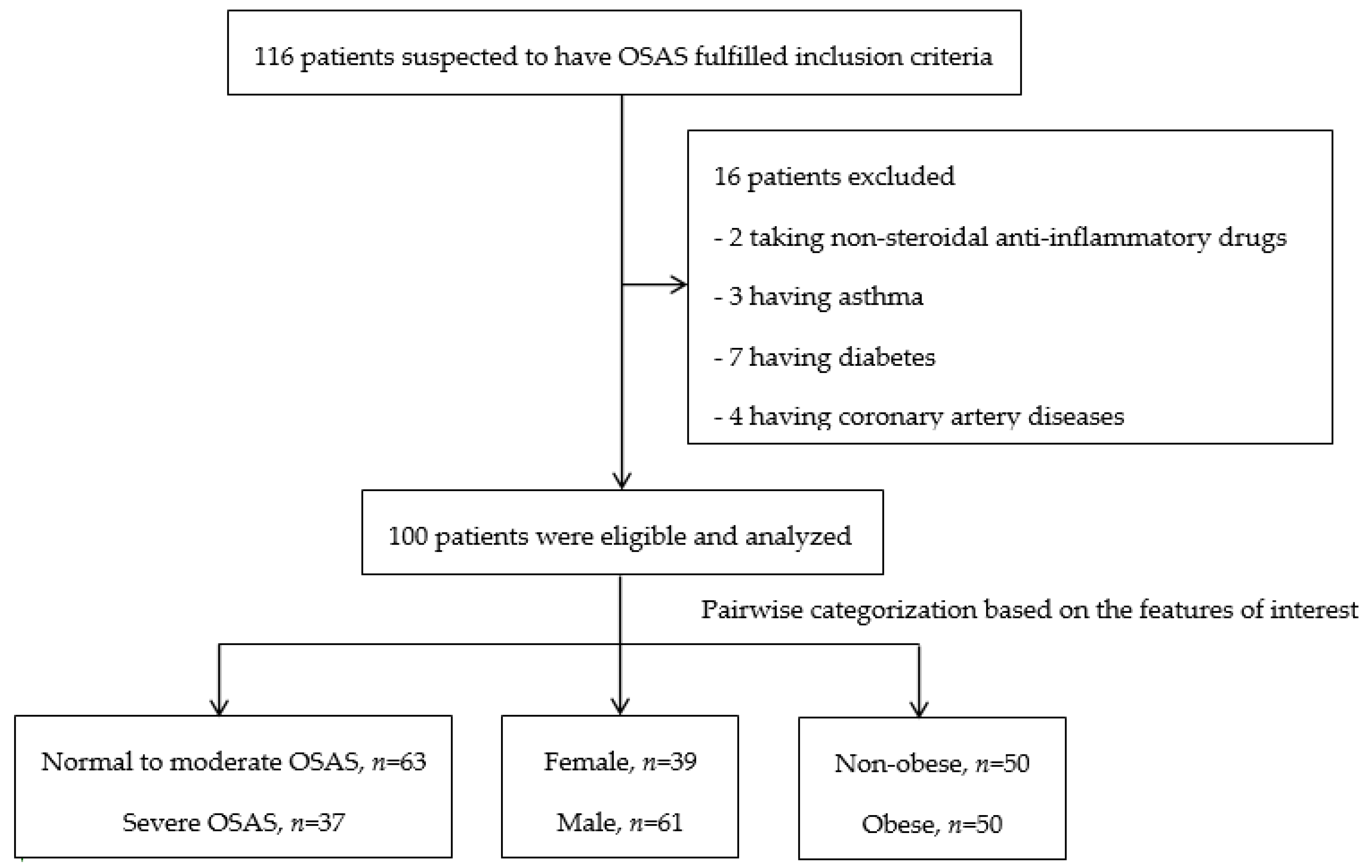
2.1. Study Design, Setting, and Population
2.2. Data Collection
2.3. Full-Night Polysomnography
2.4. Measurement of Blood Inflammatory Biomarker Levels
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Main Findings
4.2. Interpretation of the Findings in Relation to Previously Published Work
4.3. Strengths and Limitations of this Study
4.4. Implications for Future Research, Policy, and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shahar, E.; Whitney, C.W.; Redline, S.; Lee, E.T.; Newman, A.B.; Nieto, F.J.; O’Connor, G.T.; Boland, L.L.; Schwartz, J.E.; Samet, J.M. Sleep-disordered Breathing and Cardiovascular Disease. Am. J. Respir. Crit. Care Med. 2001, 163, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Yacoub, M.; Youssef, I.; O Salifu, M.; McFarlane, S.I. Cardiovascular Disease Risk in Obstructive Sleep apnea: An Update. J. Sleep Disord. Ther. 2018, 7, 1–4. [Google Scholar] [CrossRef]
- Punjabi, N.M. The epidemiology of adult obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- De Beeck, S.O.; Dieltjens, M.; Verbruggen, A.E.; Vroegop, A.V.; Wouters, K.; Hamans, E.; Willemen, M.; Verbraecken, J.; De Backer, W.A.; Van De Heyning, P.H.; et al. Phenotypic Labelling Using Drug-Induced Sleep Endoscopy Improves Patient Selection for Mandibular Advancement Device Outcome: A Prospective Study. J. Clin. Sleep Med. 2019, 15, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar]
- Arnardóttir, E.S.; Maislin, G.; Jackson, N.; Schwab, R.J.; Benediktsdottir, B.; Teff, K.; Juliusson, S.; I Pack, A.; Gislason, T. The role of obesity, different fat compartments and sleep apnea severity in circulating leptin levels: the Icelandic Sleep Apnea Cohort study. Int. J. Obes. 2012, 37, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Gabbay, I.E.; Lavie, P. Age- and gender-related characteristics of obstructive sleep apnea. Sleep Breath. 2011, 16, 453–460. [Google Scholar] [CrossRef]
- Jehan, S.; Zizi, F.; Pandi-Perumal, S.R.; Wall, S.; Auguste, E.; Myers, A.K.; Jean-Louis, G.; McFarlane, S.I. Obstructive sleep apnea and obesity: implications for public health. Sleep Med. Disord. Int. J. 2017, 1, 00019. [Google Scholar] [CrossRef]
- Kastoer, C.; Benoist, L.B.L.; Dieltjens, M.; Torensma, B.; De Vries, L.H.; Vonk, P.E.; Ravesloot, M.J.L.; De Vries, N. Comparison of upper airway collapse patterns and its clinical significance: drug-induced sleep endoscopy in patients without obstructive sleep apnea, positional and non-positional obstructive sleep apnea. Sleep Breath. 2018, 22, 939–948. [Google Scholar] [CrossRef]
- Peppard, P.E.; Young, T.; Palta, M.; Dempsey, J.; Skatrud, J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA 2000, 284, 3015–3021. [Google Scholar] [CrossRef] [Green Version]
- Segal, Y.; Malhotra, A.; Pillar, G. Upper airway length may be associated with the severity of obstructive sleep apnea syndrome. Sleep Breath. 2008, 12, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Campos-Rodriguez, F.; Martínez-García, M.A.; De La Cruz-Moron, I.; Almeida-González, C.V.; Catalán-Serra, P.; Montserrat, J.M. Cardiovascular mortality in women with obstructive sleep apnea with or without continuous positive airway pressure treatment: a cohort study. Ann. Intern. Med. 2012, 156, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Csige, I.; Ujvárosy, D.; Szabó, Z.; Lőrincz, I.; Paragh, G.; Harangi, M.; Somodi, S. The Impact of Obesity on the Cardiovascular System. J. Diabetes Res. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kalin, M.F.; Zumoff, B. Sex hormones and coronary disease: a review of the clinical studies. Steroids 1990, 55, 330–352. [Google Scholar] [CrossRef]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G.N. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Price, J.F.; Fowkes, F.G.R. Risk factors and the sex differential in coronary artery disease. Epidemiology 1997, 8, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Guven, S.F.; Turkkani, M.H.; Ciftci, B.; Çiftçi, T.U.; Erdogan, Y. The relationship between high-sensitivity C-reactive protein levels and the severity of obstructive sleep apnea. Sleep Breath. 2011, 16, 217–221. [Google Scholar] [CrossRef]
- Ryan, S.; Taylor, C.T.; McNicholas, W.T. Predictors of Elevated Nuclear Factor-κB–dependent Genes in Obstructive Sleep Apnea Syndrome. Am. J. Respir. Crit. Care Med. 2006, 174, 824–830. [Google Scholar] [CrossRef]
- Wainstein, M.V.; Mossmann, M.; Araujo, G.N.; Gonçalves, S.C.; Gravina, G.L.; Sangalli, M.; Veadrigo, F.; Matte, R.; Reich, R.; Costa, F.G.; et al. Elevated serum interleukin-6 is predictive of coronary artery disease in intermediate risk overweight patients referred for coronary angiography. Diabetol. Metab. Syndr. 2017, 9, 67. [Google Scholar] [CrossRef]
- Yokoe, T.; Minoguchi, K.; Matsuo, H.; Oda, N.; Minoguchi, H.; Yoshino, G.; Hirano, T.; Adachi, M. Elevated levels of C-reactive protein and interleukin-6 in patients with obstructive sleep apnea syndrome are decreased by nasal continuous positive airway pressure. Circulation 2003, 107, 1129–1134. [Google Scholar] [CrossRef] [Green Version]
- Zen, V.; Fuchs, F.D.; Wainstein, M.V.; Gonçalves, S.C.; Biavatti, K.; E Riedner, C.; Fuchs, F.C.; Wainstein, R.V.; Rhoden, E.L.; Ribeiro, J.P.; et al. Neck circumference and central obesity are independent predictors of coronary artery disease in patients undergoing coronary angiography. Am. J. Cardiovasc. Dis. 2012, 2, 323–330. [Google Scholar]
- Wu, M.-F.; Hsu, J.-Y.; Huang, W.-C.; Shen, G.-H.; Wang, J.-M.; Wen, C.-Y.; Huang, W.-C. Should sleep laboratories have their own predictive formulas for continuous positive airway pressure for patients with obstructive sleep apnea syndrome? J. Chin. Med Assoc. 2014, 77, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.L.; Quan, S. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999, 22, 667–689. [CrossRef]
- Kazumi, T.; Kawaguchi, A.; Sakai, K.; Hirano, T.; Yoshino, G. Young men with high-normal blood pressure have lower serum adiponectin, smaller LDL size, and higher elevated heart rate than those with optimal blood pressure. Diabetes Care 2002, 25, 971–976. [Google Scholar] [CrossRef] [Green Version]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and Cardiovascular Disease: Pathophysiology, Evaluation, and Effect of Weight Loss. Circulation 2006, 113, 898–918. [Google Scholar] [CrossRef] [Green Version]
- Deurenberg-Yap, M.; Schmidt, G.; A Van Staveren, W.; Deurenberg, P. The paradox of low body mass index and high body fat percentage among Chinese, Malays and Indians in Singapore. Int. J. Obes. 2000, 24, 1011–1017. [Google Scholar] [CrossRef] [Green Version]
- Deurenberg, P.; Yap, M.; A Van Staveren, W. Body mass index and percent body fat: a meta analysis among different ethnic groups. Int. J. Obes. 1998, 22, 1164–1171. [Google Scholar] [CrossRef] [Green Version]
- Arnardottir, E.S.; Maislin, G.; Schwab, R.J.; Staley, B.; Benediktsdottir, B.; Ólafsson, Í.; Juliusson, S.; Romer, M.; Gislason, T.; I Pack, A. The Interaction of Obstructive Sleep Apnea and Obesity on the Inflammatory Markers C-Reactive Protein and Interleukin-6: The Icelandic Sleep Apnea Cohort. Sleep 2012, 35, 921–932. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.J.; Choi, K.-M.; Lee, S.K.; Yoon, D.W.; Shin, C.; Lee, S.G. Obstructive Sleep Apnea Is Associated with Elevated High Sensitivity C-Reactive Protein Levels Independent of Obesity: Korean Genome and Epidemiology Study. PLoS ONE 2016, 11, e0163017. [Google Scholar] [CrossRef]
- De Ferranti, S.; Rifai, N. C-reactive protein and cardiovascular disease: a review of risk prediction and interventions. Clin. Chim. Acta 2002, 317, 1–15. [Google Scholar] [CrossRef]
- Khaodhiar, L.; Ling, P.-R.; Blackburn, G.L.; Bistrian, B.R. Serum Levels of Interleukin-6 and C-Reactive Protein Correlate With Body Mass Index Across the Broad Range of Obesity. J. Parenter. Enter. Nutr. 2004, 28, 410–415. [Google Scholar] [CrossRef]
- Kern, P.A.; Ranganathan, S.; Li, C.; Wood, L.; Ranganathan, G. Adipose tissue tumor necrosis factor and interleukin-6 expression in human obesity and insulin resistance. Am. J. Physiol. Metab. 2001, 280, E745–E751. [Google Scholar] [CrossRef]
- Burke, A.P.; Tracy, R.P.; Kolodgie, F.; Malcom, G.T.; Zieske, A.; Kutys, R.; Pestaner, J.; Smialek, J.; Virmani, R. Elevated C-reactive protein values and atherosclerosis in sudden coronary death: association with different pathologies. Circulation 2002, 105, 2019–2023. [Google Scholar] [CrossRef] [Green Version]
- Din-Dzietham, R.; Liu, Y.; Bielo, M.-V.; Shamsa, F. High Blood Pressure Trends in Children and Adolescents in National Surveys, 1963 to 2002. Circulation 2007, 116, 1488–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haverkate, E.; Thompson, S.G.; Pyke, S.D.; Gallimore, J.R. Mark B Pepys Group Production of C-reactive protein and risk of coronary events in stable and unstable angina. Lancet 1997, 349, 462–466. [Google Scholar] [CrossRef]
- Kleinbongard, P.; Heusch, G.; Schulz, R. TNFα in atherosclerosis, myocardial ischemia/reperfusion and heart failure. Pharmacol. Ther. 2010, 127, 295–314. [Google Scholar] [CrossRef]
- Lindahl, B.; Toss, H.; Siegbahn, A.; Venge, P.; Wallentin, L. Markers of Myocardial Damage and Inflammation in Relation to Long-Term Mortality in Unstable Coronary Artery Disease. N. Engl. J. Med. 2000, 343, 1139–1147. [Google Scholar] [CrossRef]
- Van Gaal, L.F.; Mertens, I.L.; De Block, C.E. Mechanisms linking obesity with cardiovascular disease. Nature 2006, 444, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Yudkin, J.S.; Kumari, M.; Humphries, S.E.; Mohamed-Ali, V. Inflammation, obesity, stress and coronary heart disease: is interleukin-6 the link? Atherosclerosis 2000, 148, 209–214. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Kales, A.; Tyson, K.; Chrousos, G.P. Elevation of Plasma Cytokines in Disorders of Excessive Daytime Sleepiness: Role of Sleep Disturbance and Obesity. J. Clin. Endocrinol. Metab. 1997, 82, 1313–1316. [Google Scholar] [CrossRef] [PubMed]
- Bettencourt, P.; Azevedo, A.; Pimenta, J.; Friões, F.; Ferreira, S.; Ferreira, A. N-Terminal–Pro-Brain Natriuretic Peptide Predicts Outcome After Hospital Discharge in Heart Failure Patients. Circulation 2004, 110, 2168–2174. [Google Scholar] [CrossRef] [Green Version]
- Ljunggren, M.; Lindahl, B.; Theorell-Haglöw, J.; Lindberg, E. Association between Obstructive Sleep Apnea and Elevated Levels of Type B Natriuretic Peptide in a Community-Based Sample of Women. Sleep 2012, 35, 1521–1527. [Google Scholar] [CrossRef]
- Maeder, M.T.; Ammann, P.; Rickli, H.; Schoch, O.D.; Korte, W.; Hürny, C.; Myers, J.; Münzer, T. N-terminal pro-B-type natriuretic peptide and functional capacity in patients with obstructive sleep apnea. Sleep Breath. 2007, 12, 7–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roca, G.Q.; Redline, S.; Punjabi, N.; Claggett, B.; Ballantyne, C.M.; Solomon, S.D.; Shah, A.M. Sleep Apnea Is Associated with Subclinical Myocardial Injury in the Community. The ARIC-SHHS Study. Am. J. Respir. Crit. Care Med. 2013, 188, 1460–1465. [Google Scholar] [CrossRef] [Green Version]
- Randby, A.; Namtvedt, S.K.; Einvik, G.; Hrubos-Strøm, H.; Hagve, T.-A.; Somers, V.K.; Omland, T. Obstructive Sleep Apnea Is Associated with Increased High-Sensitivity Cardiac Troponin T Levels. Chest 2012, 142, 639–646. [Google Scholar] [CrossRef]
- Strehmel, R.; Valo, M.; Teupe, C. Natriuretic Peptide and High-Sensitive Troponin T Concentrations Correlate with Effectiveness of Short-Term CPAP in Patients with Obstructive Sleep Apnea and Coronary Artery Disease. Clin. Med. Insights Circ. Respir. Pulm. Med. 2016, 10, 33–39. [Google Scholar] [CrossRef]
- Recoquillon, S.; Pépin, J.-L.; Vielle, B.; Andriantsitohaina, R.; Bironneau, V.; Chouet-Girard, F.; Fleury, B.; Goupil, F.; Launois, S.; Martinez, M.C.; et al. Effect of mandibular advancement therapy on inflammatory and metabolic biomarkers in patients with severe obstructive sleep apnoea: A randomised controlled trial. Thorax 2018, 74, 496–499. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | All (n = 100) | Normal to Moderate OSAS (n = 63) | Severe OSAS (n = 37) | Female (n = 39) | Male (n = 61) | Non-Obese (n = 50) | Obese (n = 50) |
|---|---|---|---|---|---|---|---|
| Sex | |||||||
| Male | 61 (61%) | 39 (61.9%) | 22 (59.5%) | 0 (0%) | 61 (100%) | 29 (58%) | 32 (64%) |
| Female | 39 (39%) | 24 (38.1%) | 15 (40.5%) | 39 (100%) | 0 (0%) | 21 (42%) | 18 (36%) |
| Age (years) | 45.5 ± 9.8 | 45.2 ± 8.7 | 46.3 ± 11.5 | 47.4 ± 7.7 | 44.3 ± 10.9 | 46.5 ± 9.4 | 44.5 ± 10.2 |
| WC (cm) a | 94.5 ± 12.6 | 93.3 ± 13.3 | 96.4 ± 11.3 | 91.6 ± 14.5 | 96.3 ± 11.0 | 85.9 ± 8.5 | 103.0 ± 10.0 |
| SBP (mmHg) | 136.8 ± 17.8 | 135.4 ± 20.1 | 138.6 ± 14.6 | 134.8 ± 16.4 | 137.9 ± 18.8 | 130.9 ± 14.3 | 144.6 ± 19.4 |
| DBP (mmHg) | 86.4 ± 14.4 | 84.9 ± 13.7 | 88.3 ± 15.1 | 83.8 ± 13.9 | 87.8 ± 14.6 | 81.9 ± 10.9 | 92.4 ± 16.3 |
| BMI (kg/m2) a | 27.8 ± 5.3 | 27.4 ± 5.4 | 28.4 ± 5.1 | 28.1 ± 6.7 | 27.6 ± 4.2 | 23.7 ± 2.2 | 31.9 ± 4.3 |
| ≥27 | 50 (50%) | 31 (49.2%) | 19 (51.4%) | 18 (46.2%) | 32 (52.5%) | 0 (0%) | 50 (100%) |
| <27 | 50 (50%) | 32 (51.4%) | 18 (48.6%) | 21 (53.8%) | 29 (47.5%) | 50 (100%) | 0 (0%) |
| Parameter | All (n = 100) | Normal to Moderate OSAS (n = 63) | Severe OSAS (n = 37) | Female (n = 39) | Male (n = 61) | Non-Obese (n = 50) | Obese (n = 50) |
|---|---|---|---|---|---|---|---|
| AHI (events/hour) b | 23.9 ± 23.5 | 8.9 ± 8.6 | 49.5 ± 18.1 | 24.2 ± 23.0 | 23.8 ± 24.1 | 20.7 ± 19.3 | 27.2 ± 26.9 |
| >30 | 37 (37%) | 0 (0%) | 37 (100%) | 15 (38.5%) | 22 (36.1%) | 18 (36%) | 19 (38%) |
| ≤30 | 63 (63%) | 63 (100%) | 0 (0%) | 24 (61.5%) | 39 (63.9%) | 32 (64%) | 31 (62%) |
| OAI (events/hour) κ,b | 8.9 ± 13.2 | 2.6 ± 4.3 | 19.4 ± 16.4 | 7.6 ± 10.0 | 9.7 ± 15.0 | 8.4 ± 10.0 | 9.3 ± 16.0 |
| CAI (events/hour) κ,b | 1.3 ± 2.6 | 0.6 ± 1.9 | 2.5 ± 3.2 | 1.0 ± 1.9 | 1.5 ± 2.9 | 1.8 ± 3.3 | 0.8 ± 1.6 |
| MAI (events/hour) κ,b,c | 1.5 ± 6.2 | 0.2 ± 0.7 | 3.8 ± 9.9 | 0.2 ± 0.4 | 2.4 ± 7.9 | 1.7 ± 7.7 | 1.3 ± 4.3 |
| HI (events/hour) κ,a,b | 12.4 ± 14.1 | 5.7 ± 5.1 | 24.0 ± 16.8 | 15.5 ± 17.8 | 10.5 ± 10.8 | 8.8 ± 9.0 | 16.1 ± 17.1 |
| Arousal index (events/hour) κ,b | 16.5 ± 18.3 | 7.4 ± 5.9 | 31.9 ± 21.7 | 15.4 ± 6.9 | 17.1 ± 19.2 | 14.5 ± 14.1 | 18.3 ± 21.6 |
| Stages of sleep | |||||||
| N1 (%) κ,a,b | 24.3 ± 14.3 | 20.6 ± 11.3 | 30.5 ± 16.7 | 23.2 ± 14.0 | 25.0 ± 14.6 | 21.0 ± 12.4 | 27.6 ± 15.5 |
| N2 (%) | 50.2 ± 12.9 | 50.5 ± 11.0 | 49.7 ± 15.4 | 48.7 ± 14.1 | 51.1 ± 11.9 | 50.7 ± 11.8 | 49.7 ± 13.8 |
| N3 (%) b,c | 12.8 ± 8.9 | 15.2 ± 9.0 | 8.6 ± 7.1 | 15.5 ± 8.7 | 11.1 ± 8.7 | 14.2 ± 9.4 | 11.4 ± 8.3 |
| R (%) κ | 12.7 ± 6.5 | 13.6 ± 6.0 | 11.1 ± 7.0 | 12.6 ± 6.9 | 12.7 ± 6.2 | 14.1 ± 5.8 | 11.4 ± 6.8 |
| Sleep efficiency (%) κ | 86.4 ± 11.0 | 86.9 ± 10.6 | 85.5 ± 11.7 | 85.4 ± 13.0 | 87.0 ± 9.5 | 87.4 ± 10.1 | 85.4 ± 11.7 |
| SpO2nadir (%) κ,b | 81.3 ± 9.4 | 85.3 ± 6.4 | 74.4 ± 9.9 | 81.6 ± 10.2 | 81.1 ± 9.0 | 83.1 ± 8.2 | 79.5 ± 10.3 |
| SpO2mean a,b | 94.1 ± 4.0 | 95.7 ± 1.4 | 91.5 ± 5.4 | 94.2 ± 5.4 | 94.1 ± 2.8 | 94.9 ± 2.4 | 93.3 ± 5.0 |
| TST (min) κ | 324.8 ± 44.0 | 328.0 ± 42.2 | 319.1 ± 47.0 | 320.4 ± 48.2 | 327.6 ± 41.2 | 331.7 ± 42.7 | 317.8 ± 44.5 |
| ESS | 10.2 ± 4.4 | 9.7 ± 4.5 | 11.1 ± 4.3 | 10.4 ± 4.6 | 10.0 ± 4.4 | 9.6 ± 4.3 | 10.8 ± 4.6 |
| Variable | All (n = 100) | Normal to Moderate OSAS (n = 63) | Severe OSAS (n = 37) | Female ( n = 39) | Male (n = 61) | Non-Obese (n = 50) | Obese (n = 50) |
|---|---|---|---|---|---|---|---|
| WBC (/uL) κ,a,c | 7052.41 ± 2701.399 | 7152.22 ± 2941.925 | 6852.78 ± 2206.573 | 6180.83 ± 1641.815 | 7749.67 ± 3172.926 | 6089.17 ± 2190.213 | 7823.00 ± 2854.859 |
| Cholesterol (mg/dL) | 191.2 ± 37.3 | 187.9 ± 36.4 | 197.2 ± 38.5 | 194.6 ± 41.9 | 189.2 ± 34.2 | 192.1 ± 39.3 | 190.5 ± 35.5 |
| Triglycerides(mg/dL) | 145.2 ± 80.1 | 134.7 ± 70.3 | 163.0 ± 92.7 | 136.7 ± 76.6 | 150.6 ± 82.4 | 133.8 ± 80.2 | 156.6 ± 79.1 |
| HDL (mg/dL) κ,a,c | 52.3 ± 12.0 | 51.2 ± 12.6 | 54.9 ± 10.2 | 58.6 ± 11.0 | 45.4 ±9.0 | 57.3 ± 12.0 | 48.0 ± 10.3 |
| LDL (mg/dL) | 119.5 ± 28.6 | 124.4 ± 28.3 | 110.2 ± 28.0 | 126.3 ± 31.3 | 114.0 ± 25.8 | 118.6 ± 33.8 | 120.4 ± 23.9 |
| CRP (mg/dL) κ,a | 0.259 ± 0.33 | 0.227 ± 0.31 | 0.314 ± 0.37 | 0.319 ± 0.42 | 0.221 ± 0.26 | 0.163 ± 0.29 | 0.36 ± 0.35 |
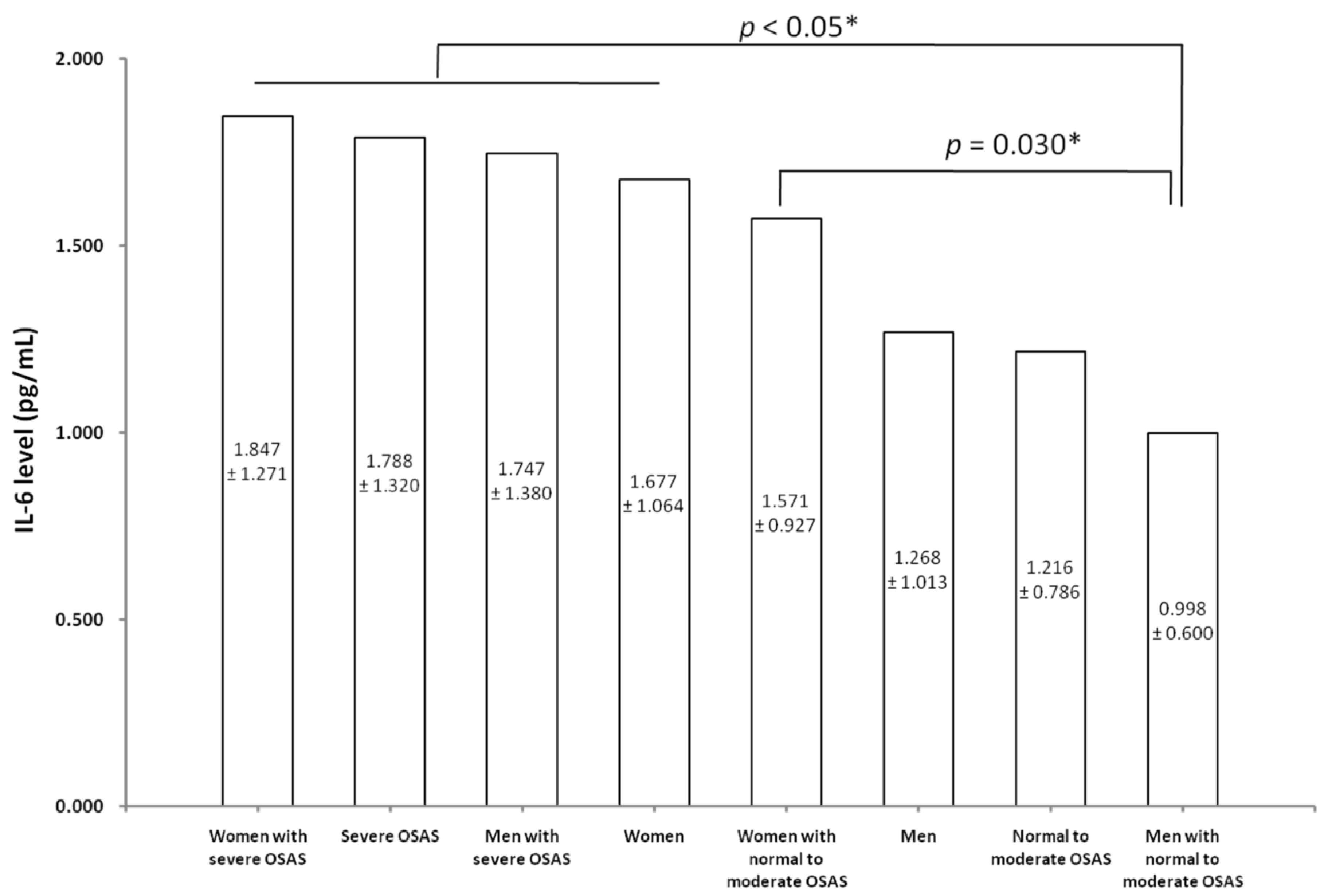
| IL-6 (pg/mL) κ,a,b,c | 1.428 ± 1.05 | 1.216 ± 0.79 | 1.787 ± 1.32 | 1.677 ± 1.06 | 1.268 ± 1.01 | 0.978 ± 0.59 | 1.877 ± 1.21 |
| TNF-α (pg/mL) | 1.160 ± 0.42 | 1.140 ± 0.41 | 1.194 ± 0.43 | 1.222 ± 0.41 | 1.120 ± 0.42 | 1.153 ± 0.44 | 1.167 ± 0.40 |
| Features | CRP (mg/dL) | IL-6 (pg/mL) | TNF-α (pg/mL) |
|---|---|---|---|
| Normal to moderate OSAS, male and non-obese (n = 17) | 0.142 ± 0.253 | 0.681 ± 0.259 | 0.915 ± 0.354 |
| Normal to moderate OSAS, male and obese (n = 22) | 0.224 ± 0.236 | 1.243 ± 0.676 | 1.238 ± 0.408 |
| Normal to moderate OSAS, female and non-obese (n = 15) | 0.182 ± 0.409 | 1.099 ± 0.638 | 1.237 ± 0.451 |
| Normal to moderate OSAS, female and obese (n = 9) | 0.467 ± 0.294 | 2.358 ± 0.801 | 1.166 ± 0.356 |
| Severe OSAS, male and non-obese (n = 12) | 0.152 ± 0.214 | 1.098 ± 0.553 | 1.308 ± 0.476 |
| Severe OSAS, male and obese (n = 10) | 0.430 ± 0.276 | 2.526 ± 1.684 | 0.967 ± 0.336 |
| Severe OSAS, female and non-obese (n = 6) | 0.191 ± 0.227 | 1.280 ± 0.920 | 1.307 ± 0.321 |
| Severe OSAS, female and obese (n = 9) | 0.483 ± 0.574 | 2.226 ± 1.377 | 1.196 ± 0.494 |
| Factor a | CRP (n = 100) κ | IL-6 (n = 100) κ | TNF-α (n = 100) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SS | df | MS | F | p-value | SS | df | MS | F | p-value | SS | df | MS | F | p-value | |
| A | 0.814 | 1 | 0.814 | 2.126 | 0.148 | 0.208 | 1 | 0.208 | 4.123 | 0.045 * | 0.065 | 1 | 0.065 | 0.389 | 0.534 |
| B | 0.613 | 1 | 0.613 | 1.601 | 0.209 | 0.285 | 1 | 0.285 | 5.639 | 0.020 * | 0.303 | 1 | 0.303 | 1.809 | 0.182 |
| C | 7.620 | 1 | 7.620 | 19.913 | 0.001 * | 1.839 | 1 | 1.839 | 36.370 | 0.000 * | 0.053 | 1 | 0.053 | 0.317 | 0.575 |
| A × B | 0.128 | 1 | 0.128 | 0.335 | 0.564 | 0.347 | 1 | 0.347 | 6.869 | 0.010 * | 0.001 | 1 | 0.001 | 0.004 | 0.951 |
| A × C | 0.154 | 1 | 0154 | 0.402 | 0.528 | 0.002 | 1 | 0.002 | 0.030 | 0.862 | 0.657 | 1 | 0.657 | 3.924 | 0.051 |
| B × C | 0.004 | 1 | 0.004 | 0.012 | 0.914 | 0.003 | 1 | 0.003 | 0.056 | 0.814 | 0.036 | 1 | 0.036 | 0.214 | 0.645 |
| A × B × C | 0.482 | 1 | 0.482 | 1.259 | 0.265 | 0.038 | 1 | 0.038 | 0.757 | 0.386 | 0.516 | 1 | 0.516 | 3.083 | 0.082 |
| SSE | 34.821 | 91 | 0.383 | 4.651 | 92 | 0.051 | 15.231 | 91 | 0.167 | ||||||
| SST | 141.576 | 99 | 8.030 | 100 | 150.358 | 99 | |||||||||
| Variable | Factor | Three-Way Analysis | Post Hoc Test | Results | p-Value | Power |
|---|---|---|---|---|---|---|
| CRP | Obesity | Main effect | Marginal means | Obesity > Non-obesity | 0.001 * | 0.92 |
| IL-6 | Sex | Simple main effect | Cell means | 0.88 | ||
| N-M OSAS | Female > Male | 0.004 * | ||||
| Severe OSAS | Female > Male | 0.824 | ||||
| IL-6 | OSAS severity | Simple main effect | Cell means | |||
| Male | Severe OSAS > N-M OSAS | 0.005 * | 0.83 | |||
| Female | Severe OSAS > N-MOSAS | 0.438 | ||||
| IL-6 | Obesity | Main effect | Marginal means | Obesity > Non-obesity | 0.000 * | 0.99 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-F.; Chen, Y.-H.; Chen, H.-C.; Huang, W.-C. Interactions among Obstructive Sleep Apnea Syndrome Severity, Sex, and Obesity on Circulatory Inflammatory Biomarkers in Patients with Suspected Obstructive Sleep Apnea Syndrome: A Retrospective, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4701. https://doi.org/10.3390/ijerph17134701
Wu M-F, Chen Y-H, Chen H-C, Huang W-C. Interactions among Obstructive Sleep Apnea Syndrome Severity, Sex, and Obesity on Circulatory Inflammatory Biomarkers in Patients with Suspected Obstructive Sleep Apnea Syndrome: A Retrospective, Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(13):4701. https://doi.org/10.3390/ijerph17134701
Chicago/Turabian StyleWu, Ming-Feng, Yu-Hsuan Chen, Hui-Chen Chen, and Wei-Chang Huang. 2020. "Interactions among Obstructive Sleep Apnea Syndrome Severity, Sex, and Obesity on Circulatory Inflammatory Biomarkers in Patients with Suspected Obstructive Sleep Apnea Syndrome: A Retrospective, Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 13: 4701. https://doi.org/10.3390/ijerph17134701
APA StyleWu, M. -F., Chen, Y. -H., Chen, H. -C., & Huang, W. -C. (2020). Interactions among Obstructive Sleep Apnea Syndrome Severity, Sex, and Obesity on Circulatory Inflammatory Biomarkers in Patients with Suspected Obstructive Sleep Apnea Syndrome: A Retrospective, Cross-Sectional Study. International Journal of Environmental Research and Public Health, 17(13), 4701. https://doi.org/10.3390/ijerph17134701