Action after Adverse Events in Healthcare: An Integrative Literature Review

 ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
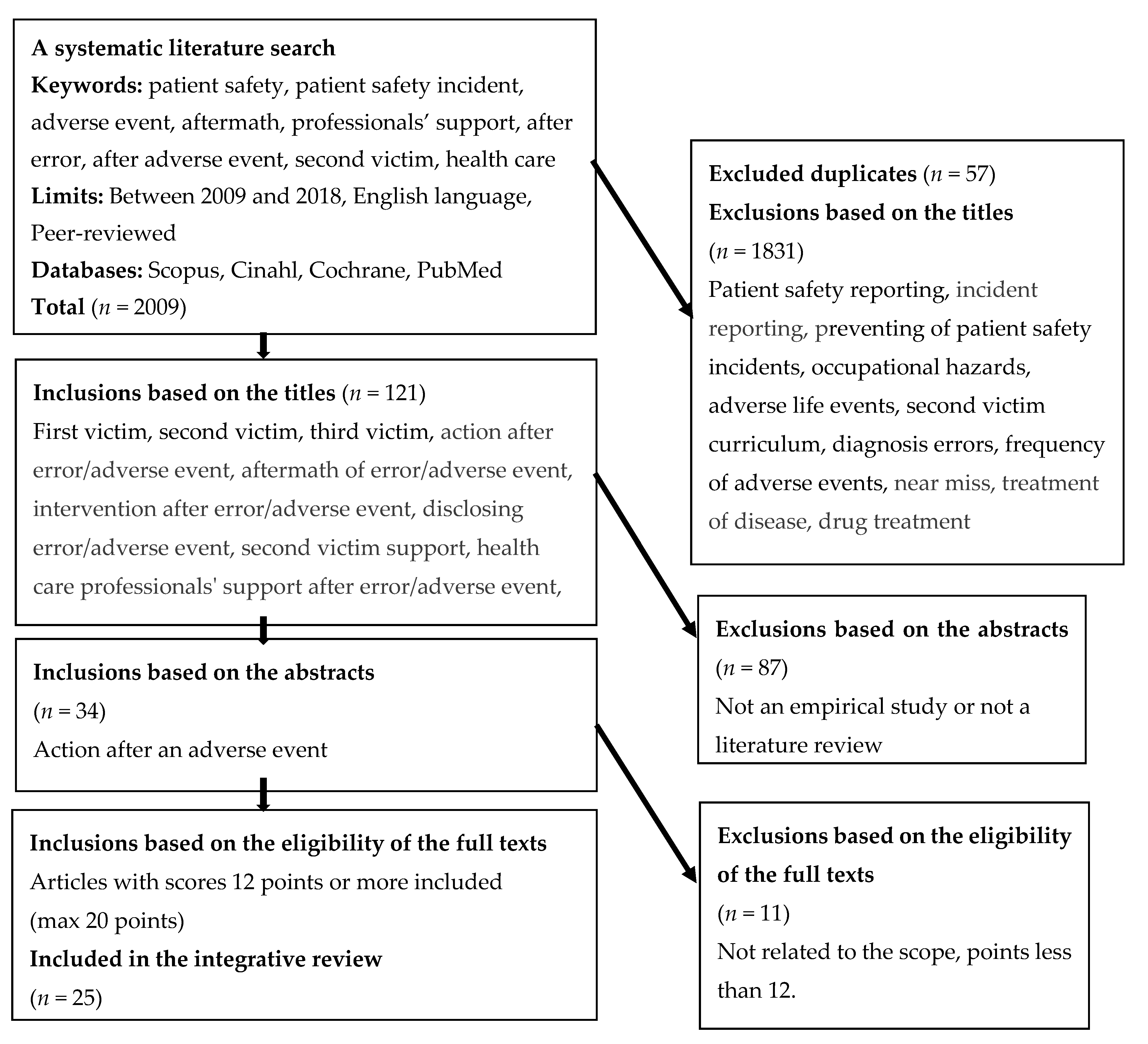
2.2. Search Strategy
2.3. Review and Quality Assessment Process
2.4. Data Analysis
3. Results
3.1. Characteristic for the Studies
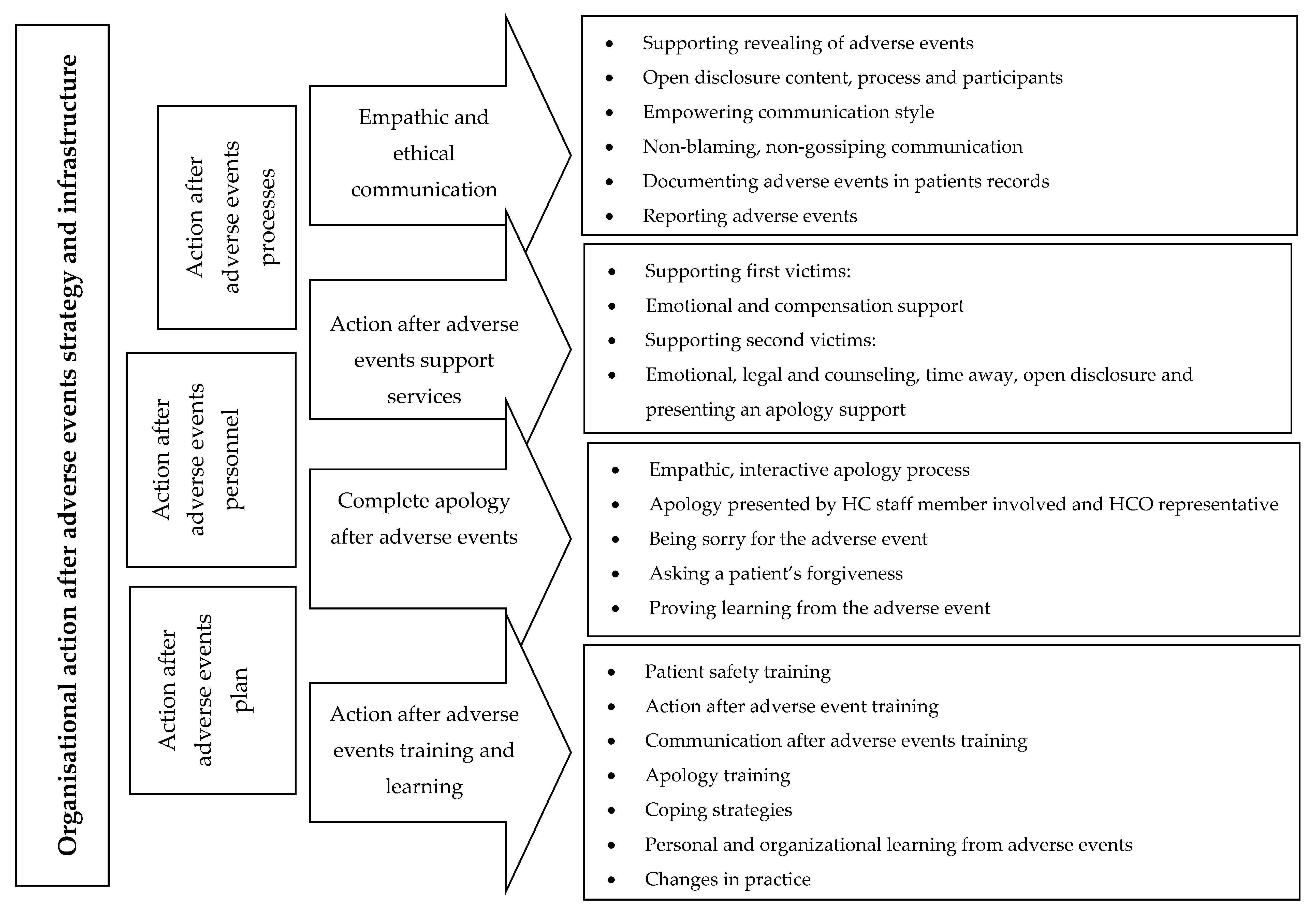
3.2. Key Elements of Responses and Action after AEs Bulleted Lists Look Like This
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vincent, C. Patient Safety, 2nd ed.; Wiley-Blackwell: Chichester, UK, 2010. [Google Scholar]
- Van Gaal, B.G.; Schoonhoven, L.; Mintjes-de Groot, J.A.; Defloor, T.; Habets, H.; Voss, A. Concurrent incidence of adverse events in hospitals and nursing homes. J. Nurs. Sch. 2014, 46, 187–198. [Google Scholar] [CrossRef]
- Disclosure Working Group. Canadian Disclosure Guidelines: Being Open and Honest with Patients and Families [Internet]; Canadian Patient Safety Institute: Edmonton, AB, Canada, 2011; Available online: http://www.patientsafetyinstitute.ca/en/toolsResources/disclosure/Documents/CPSI%20Canadian%20Disclosure%20Guidelines.pdf (accessed on 28 November 2018).
- World Health Organization. Conceptual Framework for the International Classification for Patient Safety (v.1.1) [Internet]; World Health Organization: Geneva, Switzerland, 2009; Available online: http://www.who.int/patientsafety/taxonomy/icps_full_report.pdf (accessed on 1 August 2018).
- De Vries, E.N.; Ramrattan, M.A.; Smorenburg, S.M.; Gouma, D.J.; Boermeester, M.A. The incidence and nature of in-hospital adverse events: A systematic review. BMJ Qual. Saf. 2008, 7, 216–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Patient Safety and Quality of Care Working Group. Key Findings and Recommendations on Reporting and Learning Systems for Patient Safety Incidents across Europe [Internet]; European Commission: Brussels, Belgium, 2014; Available online: http://ec.europa.eu/health//sites/health/files/patient_safety/docs/guidelines_psqcwg_reporting_learningsystems_en.pdf (accessed on 1 August 2018).
- Andersson, Å.; Frank, C.; Willman, A.M.L.; Hansebo, G. Adverse events in nursing: A retrospective study of reports of patient and relative experiences. Int. Nurs. Rev. 2015, 62, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Wahlberg, Å.; Sachs, M.A.; Johannesson, K.B.; Hallberg, G.; Jonsson, M.; Skoog Svanberg, A.; Högberg, U. Self-reported exposure to severe events on the labour ward among Swedish midwives and obstetricians: A cross-sectional retrospective study. Int. J. Nurs. Stud. 2017, 65, 8–16. [Google Scholar] [CrossRef]
- Donaghy, C.; Doherty, R.; Irwin, T. Patient safety: A culture of openness and supporting staff. Surgery 2018, 36, 09–514. [Google Scholar] [CrossRef]
- Edrees, H.; Connors, C.; Paine, L.; Norvell, M.; Taylor, H.; Wu, A.W. Implementing the RISE second victim support programme at the Johns Hopkins Hospital: A case study. BMJ Open 2016, 6, e011708. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.W. Medical error: The second victim: The doctor who makes the mistake needs help too. BMJ 2000, 320, 726–727. [Google Scholar] [CrossRef]
- Scott, S.D.; Hirschinger, L.E.; Cox, K.R.; McCoig, M.M.; Hahn-Cover, K.; Epperly, K.M.; Epperly, K.M.; Phillips, E.C.; Hall, L.W. Caring for our own: Deploying a systemwide second victim rapid response team. Jt. Comm. J. Qual. Patient Saf. 2010, 36, 233–240. [Google Scholar] [CrossRef]
- Hall, L.W.; Scott, S.D. The second victim of adverse health care events. Nurs. Clin. N. Am. 2012, 47, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.E.; Agan, D.L.; Chakedis, S.; Skrobik, Y. Workplace blame and related concepts: An analysis of three case studies. Chest 2015, 148, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Seys, D.; Wu, A.W.; Van Gerven, E.; Vleugels, A.; Euwema, M.; Panella, M.; Scott, S.D.; Conway, J.; Sermeus, W.; Vanhaecht, K. Health care professionals as second victims after adverse events: A systematic review. Eval. Health Prof. 2013, 36, 135–162. [Google Scholar] [CrossRef] [PubMed]
- Mohamadi-Bolbanabad, A.; Morade, G.; Piroozi, B.; Safari, H.; Asadi, H.; Nasseri, K.; Mohammadi, H.; Afkhamzadeh, A. The second victims’ experience and related factors among medical staff. Int. J. Workplace Health Manag 2019, 12, 134–145. [Google Scholar] [CrossRef]
- MacLeod, L. “Second victim” casualties and how physician leaders can help. Physician Exec. 2014, 40, 8–12. [Google Scholar] [PubMed]
- Conway, J.; Federico, F.; Stewart, K.; Campbell, M. Respectful Management of Serious Clinical Adverse Events, 2nd ed.; [Internet]; IHI Innovation Series White Paper; Institute for Healthcare Improvement: Cambridge, MA, USA, 2011; Available online: http://www.ihi.org/resources/Pages/IHIWhitePapers/RespectfulManagementSeriousClinicalAEsWhitePaper.aspx (accessed on 23 November 2018).
- McVeety, J.; Keeping-Burke, L.; Harrison, M.B.; Godfrey, C.; Ross-White, A. Patient and family member perspectives of encountering adverse events in health care: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2014, 12, 315–373. [Google Scholar] [CrossRef]
- Ullström, S.; Sachs, M.A.; Hansson, J.; Øvretveit, J.; Brommels, M. Suffering in silence: A qualitative study of second victims of adverse events. BMJ Qual. Saf. 2013, 23, 325–331. [Google Scholar] [CrossRef] [Green Version]
- Kable, A.K.; Spigelman, A.D. Why clinicians involved with adverse events need much better support. Int. J. Health Gov. 2018, 23, 312–315. [Google Scholar] [CrossRef]
- Kable, A.; Kelly, B.; Adams, J. Effects of adverse events in health care on acute care nurses in an Australian context: A qualitative study. Nurs. Health Sci. 2018, 20, 238–246. [Google Scholar] [CrossRef]
- Krzan, K.D.; Merandi, J.; Morvay, S.; Mirtallo, J. Implementation of a “second victim” program in a pediatric hospital. Am. J. Health Syst. Pharm. 2015, 72, 563–567. [Google Scholar] [CrossRef]
- Rodriquez, J.; Scott, S.D. When Clinicians Drop Out and Start Over after Adverse Events. Jt. Comm. J. Qual. Patient Saf. 2018, 44, 137–145. [Google Scholar] [CrossRef]
- Mira, J.J.; Carrillo, I.; Lorenzo, S.; Ferrús, L.; Silvestre, C.; Pérez-Pérez, P.; Olivera, G.; Iglesias, F.; Zavala, E.; Maderuelo-Fernández, J.; et al. The aftermath of adverse events in Spanish primary care and hospital health professionals. BMC Health Serv. Res. 2015, 15, 151. [Google Scholar] [CrossRef] [Green Version]
- Slawomirski, L.; Auraaen, A.; Klazinga, N. The Economic of Patient Safety. Strengthening a Value-Based Approach to Reducing Patient Harm at National Level; OECD: Paris, France, 2017. [Google Scholar]
- World Health Organization Regional Office for Europe. Patient Safety, Data and Statistics. Available online: http://www.euro.who.int/en/health-topics/Health-systems/patient-safety/data-and-statistics (accessed on 12 November 2019).
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; for the PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Hawker, S.; Payne, S.; Kerr, C.; Powell, J. Appraising the evidence: Reviewing disparate data systematically. Qual. Health Res. 2002, 12, 1284–1299. [Google Scholar] [CrossRef]
- Jokelainen, M.; Turunen, H.; Tossavainen, K.; Jamookeeah, D.; Coco, K. A systematic review of mentoring nursing students in clinical placements. J. Clin. Nurs. 2011, 20, 2854–2867. [Google Scholar] [CrossRef] [PubMed]
- Pearson, P.; Steven, A.; Howe, A.; Sheikh, A.; Ashcroft, D.; Smith, P.; on behalf of Patient Safety Education Study Group. Learning about patient safety: Organizational context and culture in the education of health care professionals. J. Health Serv. Res. Policy 2010, 15, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Tella, S.; Liukka, M.; Jamookeeah, D.; Smith, N.J.; Partanen, P.; Turunen, H. What do nursing students learn about patient safety? An integrative literature review. J. Nurs. Educ. 2014, 53, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Itoh, K. Patient views and attitudes to physician’s actions after medical errors in China. J. Patient Saf. 2012, 8, 153–160. [Google Scholar] [CrossRef]
- Mira, J.J.; Lorenzo, S.; Carrillo, I.; Ferrús, L.; Pérez-Pérez, P.; Iglesias, F.; Silvestre, C.; Olivera, G.; Zavala, E.; Nuño-Solinís, R.; et al. on behalf of the Research Group on Second and Third Victims. Interventions in health organisations to reduce the impact of adverse events in second and third victims. BMC Health Serv. Res. 2015, 15, 341. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, R.; Iedema, R.; Piper, D.; Manias, E.; Williams, A.; Tuckett, A. Disclosing clinical adverse events to patients: Can practice inform policy? Health Expect. 2010, 13, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Koller, D.; Espin, S. Views of children, parents, and health-care providers on pediatric disclosure of medical errors. J. Child Health Care 2018, 22, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Hågensen, G.; Nilsen, G.; Mehus, G.; Henriksen, N. The struggle against perceived negligence. A qualitative study of patients’ experiences of adverse events in Norwegian hospitals. BMC Health Serv. Res. 2018, 18, 302. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Lorenzo, S.; Carrillo, I.; Ferrús, L.; Silvestre, C.; Astier, P.; Iglesias-Alonso, F.; Maderuelo-Fernández, J.Á.; Pérez-Pérez, P.; Torijano, M.L.; et al. Lessons learned for reducing the negative impact of adverse events on patients, health professionals and healthcare organizations. Int. J. Qual. Health Care 2017, 29, 450–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treiber, L.A.; Jones, J.H. The second victims of infusion therapy-related medication errors. J. Infus. Nurs. 2018, 41, 156–163. [Google Scholar] [CrossRef]
- Burlison, J.D.; Scott, S.D.; Browne, E.K.; Thompson, S.G.; Hoffman, J.M. The Second Victim Experience and Support Tool: Validation of an organizational resource for assessing second victim effects and the quality of support resources. J. Patient Saf. 2017, 13, 93–102. [Google Scholar] [CrossRef]
- Edrees, H.H.; Paine, L.A.; Feroli, E.R.; Wu, A.W. Health care workers as second victims of medical errors. Pol. Arch. Intern. Med. 2011, 121, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Ferrús, L.; Silvestre, C.; Olivera, G.; Mira, J.J. Qualitative study about the experiences of colleagues of health professionals involved in an adverse event. J. Patient Saf. 2016. [Google Scholar] [CrossRef]
- Joesten, L.; Cipparrone, N.; Okuno-Jones, S.; DuBose, E.R. Assessing the perceived level of institutional support for the second victim after a patient safety event. J. Patient Saf. 2015, 11, 73–78. [Google Scholar] [CrossRef]
- Lewis, E.J.; Baernholdt, M.; Hamric, A. Nurses’ experience of medical errors: An integrative literature review. J. Nurs. Care Qual. 2013, 28, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Davies, S.; Coldridge, L. ‘No man’s land’: An exploration of the traumatic experiences of student midwives in practice. Midwifery 2015, 31, 858–864. [Google Scholar] [CrossRef]
- Harrison, R.; Lawton, R.; Perlo, J.; Gardner, P.; Armitage, G.; Shapiro, J. Emotion and coping in the aftermath of medical error: A cross-country exploration. J. Patient Saf. 2015, 11, 28–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seys, D.; Scott, S.; Wu, A.; Van Gerven, E.; Vleugels, A.; Euwema, M.; Panella, M.; Conway, J.; Sermeus, W.; Vanhaecht, K. Supporting involved health care professionals (second victims) following an adverse health event: A literature review. Int. J. Nurs. Stud. 2013, 50, 678–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edrees, H.H.; Wu, A.W. Does one size fit all? Assessing the need for organizational second victim support programs. J. Patient Saf. 2017. [Google Scholar] [CrossRef] [PubMed]
- Delacroix, S. Exploring the experience of nurse practitioners who have committed medical errors: A phenomenological approach. J. Am. Acad. Nurse Pract. 2017, 29, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Van Gerven, E.; Bruyneel, L.; Panella, M.; Euwema, M.; Sermeus, W.; Vanhaecht, K. Psychological impact and recovery after involvement in a patient safety incident: A repeated measures analysis. BMJ Open. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kachalia, A.; Bates, D.W. Disclosing medical errors: The view from the USA. Surgeon 2014, 12, 64–67. [Google Scholar] [CrossRef]
- Youngson, G.G. Medical error and disclosure—A view from the U.K. Surgeon 2014, 4, 68–72. [Google Scholar] [CrossRef]
- Wu, A.W.; McCay, L.; Levinson, W.; Iedema, R.; Wallace, G.; Boyle, D.J.; McDonald, T.B.; Bismark, M.; Kraman, S.S.; Forbes, E.; et al. Disclosing adverse events to patients: International norms and trends. J. Patient Saf. 2017, 13, 43–49. [Google Scholar] [CrossRef]
- Frankel, A.; Haraden, C.; Federico, F.; Lenoci-Edwards, J. A Framework for Safe, Reliable and Effective Care; White Paper; Institute for Healthcare Improvement and Safe & Reliable Healthcare: Cambridge, MA, USA, 2017. [Google Scholar]
- Brborovic, O.; Brborvic, H.; Nola, I.A.; Miloševic, M. Culture of blame—An ongoing burden for doctors and patient safety. Int. J. Environ. Res. Public Health 2019, 16, 4826. [Google Scholar] [CrossRef] [Green Version]
- Moumtzoglou, A. Factors impeding nurses from reporting adverse events. J. Nurs. Manag. 2010, 18, 542–547. [Google Scholar] [CrossRef]
- Sujan, M. An organisation without a memory: A qualitative study of hospital staff perceptions on reorting and organisational learning for patient safety. Reliab. Eng. Syst. Saf. 2015, 144, 45–52. [Google Scholar] [CrossRef] [Green Version]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. (Zagreb) 2012, 22, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Woodward, S. Implementing Patient Safety: Addressing Culture, Conditions and Values to Help People Work Safely; Routledge, Tylor and Francis: New York, NY, USA, 2020. [Google Scholar]
- Morrow, J.M.; Gustavson, A.M.; Jones, J. Speaking up behaviours (safety voices) of healthcare workers: A metasynthesis of qualitative research. Int. J. Nurs. Stud. 2016, 64, 42–51. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author(s) (Year), Country | Purpose and Aims of the Study | Research Methods/ Instrument/Sample (n = 25) | Findings | Evaluation Scores/Scope |
|---|---|---|---|---|
| Scott et al. (2010), USA [12] | To describe a deployment of an institutional rapid response system (RRS) for second victims | Interview and 10 item web-based survey Interviews with 31 healthcare professionals Survey (n = 898), medical students, physicians and professional nurses | Six distinct recovery stages were delineated. Almost 40% of the respondents had previously heard the term second victim; 30% have had personal problems within the past 12 months, such as anxiety, depression or concerns about their ability to perform their jobs. Thirty-five per cent of respondents reported receiving support from colleagues and peers when it was offered and 29% received support from supervisory personnel. Eight themes from the narratives to describe general support infrastructure characteristics to aid second victim recovery were identified. | 12.5 Second victim |
| Seys et al. (2013a), USA [15] | To identify supportive interventional strategies for second victims | Literature review 21 research articles and 10 non-research articles Inclusion criteria and search strategy described PRISMA method was used for reporting | Numerous supportive actions for second victims described in the literature. Strategies included support organised at the individual, organisational, national or international levels. Second victim support is needed to care for healthcare workers and to improve quality of care. Support can be provided at the individual and organisational levels. Programs need to include support immediately post adverse event as well as on a middle- and long-term basis | 14 Second victim |
| McVeety et al. (2014), Canada [19] | To analyse and synthesise best evidence on the perspectives of patients and family members who encountered adverse events | Review, 14 studies that used qualitative methodologies included Inclusion criterions and search strategy described, Joanna Briggs Institute Qualitative Appraisal and Review Instrument (JBI-QARI) and Appraisal Checklist for Interpretive and Critical Research | Nine themes were identified relating to patient and family perceptions and experiences of an adverse event: communication, the disclosure process, apology, consequences and impact, fear of reprisal and/or interference with care, learned helplessness, measures of safeguarding, self-discovery and awareness of errors, and violations of trust. | 16 First victim |
| Ullström et al. (2014), Sweden [20] | To investigate how healthcare professionals are affected by their involvement in adverse events, with emphasis on the organisational support they need and how well the organisation meets those needs. | Semi-structured interview guide with 30 questions. Qualitative content analysis and systematic classification was used Healthcare professionals (n = 21) | Impact on the healthcare professional was related to the organisation’s response to the event. | 15 Second and third victim |
| Kable et al. (2018) Australia [22] | To understand the effects of adverse events on nurses in acute health-care settings. | A qualitative, descriptive study design; 10 nurses, semi-structural interview. | Nurses need organisational responses to adverse events, including collegial support and provision of information after adverse event occur. | 17 Second victim. |
| Rodriquez and Scott. (2018) USA [24] | To examine experiences of healthcare professionals who changed paths after an adverse event. | Web-based survey with total of 105 individual responded; 77 (73,3%) were eligible to complete the survey. | Healthcare professionals reported a pattern of inadequate social support after adverse event. More transparency and support to help professionals recover is needed. | 14 Second victim |
| Mira et al. (2015a), Spain [25] | To identify and analyse organisation-level strategies adopted in both primary care and hospitals in Spain To address the impact of serious AE on second and third victims | A cross-sectional survey study. The questionnaire explored five intervention areas: safety culture; health organisation crisis management plans for serious AE; measures to ensure transparency in communication with patients (and relatives) who experience an AE; care and support for second victims and actions to protect the reputation of the health organisation (the third victim). Developed by consensus among the research team on the basis of reviews Managers of hospital and primary care centres (n = 197), patient safety coordinators in hospitals or primary care (n = 209) | Deficient provision of support for second victims was acknowledged by 71% and 61% of the participants from hospitals and primary care, respectively; these respondents reported that there was no support protocol for second victims in place in their organisations. Regarding third victim initiatives, 35% of hospital and 43% of primary care professionals indicated that no crisis management plan for serious AE existed in their organisation, and, in the case of primary care, there was no crisis committee in 34% of cases. The degree of implementation of second and third victim support interventions was perceived to be greater in hospitals (mean 14.1, SD 3.5) than in primary care (mean 11.8, SD 3.1) (p < 0.001) | 17.5 Second and third victim |
| Gu and Itoh (2012), China [35] | To explore Chinese patients’ views on physician disclosure actions after an adverse event and their acceptance of different types of apologies from the physician who caused the event. | Questionnaire with seven sections concerning responding views of issue related to medical errors and patient safety Inpatients and families (n = 934) | A large difference identified in the level of patient acceptance between a physician’s “full” or “partial” apology. It is suggested that Chinese hospitals should adopt an “open” policy, which should include a “sincere” apology to the patient who experienced a medical error in order to maintain mutual trust between the staff and patients. | 17 First victim |
| Mira et al. (2015b), Spain [36] | To assess the effect of adverse events that occur in primary care and hospital settings on health professionals in personal and professional terms | A cross-sectional study Online survey, randomly selected sample; 1087 health professionals completed the questionnaires (610 from primary care and 477 from hospitals) | In total, 430 health professionals had informed a patient of an error. Error reporting to patients was carried out by those with the strongest safety culture, under 50 years of age and primary care staff. Primary care (n = 318) and hospital (n = 346) health professionals reported having gone through the second-victim experience. The emotional responses were: feelings of guilt, anxiety, re-living the event, tiredness, insomnia and persistent feelings of insecurity. In doctors, the most common responses were feelings of guilt and re-living the event, while nurses showed greater solidarity in terms of supporting the second victim in both PC and hospital settings. | 18 Second victim |
| Sorensen et al. (e-pub 2009), Australia [37] | To understand patients’ and health professionals’ experience of Open Disclosure and how practice can inform policy | Semi-structured open-ended interview. Grounded theory was used to analyse the data Nurses, managers, policy coordinators, patients and family members (n = 154) | Five major elements influenced patients’ and professionals’ experiences of openly disclosing adverse events namely: initiating the disclosure, apologising for the adverse event, taking the patient’s perspective, communicating the adverse event and being culturally aware. | 15.5 First and second victim |
| Koller and Espin (2018) Canada [38] | To capture perspectives on paediatric disclosure and identify gaps in knowledge for best practices and policy uptake. | Focus group interview with semi-structured questions; 5 parents, 14 children and adolescents and 27 healthcare providers. | Patients and families need full disclosure and right to know about errors. Health-care professionals need more clarity in policies. Most agreed that a case-by-case approach was necessary for supporting variations in how medical errors are disclosed. | 19 First victim |
| Hågensen et al. (2018) Norway [39] | To present patients’ perspectives of disclosure of and healthcare organisations’ response to adverse events. | Qualitative study; 15 in-depth interviews. | Three main topics regarding patients’ experiences of adverse events are: (1) ignored concerns or signs of complications; (2) lack of responsibility and error correction; and (3) lack of support, loyalty and learning opportunities. | 20 First victim |
| Mira et al. (2017), Spain [40] | To summarise the knowledge about the aftermath of adverse events and to develop a recommendation set to reduce their negative impact in contexts where there is no previous experience and apology laws are not present. | Three information sources were used; review studies (n = 14 publications), institutional websites (16 websites were reviewed) and experts’ opinions and experience on patient safety (four focus group sessions with 27 participants). | Recommendations focused on eight areas: (1) Safety and organisational policies; (2) Patient care; (3) Proactive approach to preventing reoccurrence; (4) Supporting the clinician and healthcare team; (5) Activation of resources to provide an appropriate response; (6) Informing patients and/or family members; (7) Incident analysis; and (8) Protecting the reputation of health professionals and of the organisation. | 19 First, Second and third victim |
| Treiber et al. (2018) USA [41] | To discuss the second victim syndrome and its impacts on nurses. | Online survey with multiple-choice and open-ended items were sent to 842 resent nursing graduates 168 responses were received. | Fifty-six per cent reported making at least one medication error. After making a medical error nurses had emotional responses, such as fear and disappointment. Nurses described often been supported by peers, nursing manager and preceptors. | 12 Second victim |
| Burlison et al. (2017), USA [42] | To present the development and psychometric evaluation of the Second Victim Experience and Support Tool (SVEST), a survey instrument that can assist healthcare organisations to implement and track the performance of second victim support resources | Quantitative study Second Victim Experience and Support Tool (SVEST) questionnaire development, 5-point Likert scale Nurses, physicians, pharmacists and medical technicians in specialised paediatric hospital (n = 305) | The SVEST (The Second Victim Experience and Support Tool) can be used by healthcare organisations to evaluate second victim experiences of the quality of existing support resources. Means: Psychological distress 2.6, physical distress 2.3, colleague support 2.2, supervisor support 2.8, institutional support 2.3, non-work-related support 2.4, professional efficacy 2.5, turnover intentions 2.1, absenteeism 1.8 The most desired second victim option: A discussion with a respected peer 81% The second most desired option: A discussion with the manager 74% | 19.5 Second victim |
| Edrees et al. (2011), USA [43] | To emphasise the importance of support structures for second victims in the handling of patient adverse events and in building a culture of safety within hospitals. | A cross-sectional survey using a two-part Second Victim Questionnaire Nurses, nursing or other managers, physicians, pharmacists, therapists, clinical support, technologists (n = 140 in part one and n = 95 in part two) | There is a need for second victim support strategy in healthcare organisations. Informal emotional support and peer support are among the most requested and most useful strategies. Other desired support: Prompt debriefing, crisis intervention stress management (75%), an opportunity to discuss ethical concerns related to an event or process (46%), a safe opportunity to contribute to the prevention of similar events in the future (45%) | 13.5 Second victim |
| Ferrús et al. (2016), Spain [44] | To identify what occurs among healthcare providers after an adverse event and what colleagues could do to help them | A qualitative study applying consensus search techniques Focus group and metaplan Physicians (n = 15), nurses (n = 12) | Consensus about second victims requiring support from their colleagues and managers; many times, second victims perceive rejection. They experience fear, repetitive thoughts and loneliness. Formal information channels favour implementation of improvements. HCPs perceived that information on measures for preventing another adverse event is inaccessible. Managers reported that a change in behaviour is necessary to improve patient safety culture. Common informal channels included cafeterias and hallways. Colleagues of second victims’ reactions included surprise and pursuit to avoid involvement. | 16 Second victim |
| Joesten et al. (2015), USA [45] | To establish a baseline of perceived availability of institutional support services or interventions and experiences following an adverse patient safety event (PSE) | Quantitative study, The Medically Induced Trauma Support Services Staff Support Survey (MITSS) Nurses (n = 82), physicians (n = 12) | Overall, 10–30% of respondents reported that various support services or interventions were actively offered. Respondents reported having experienced several distressing symptoms after PSE, such as worrying memories (56%) and concerns about lawsuits (37%). Most of them experienced more support from colleagues than from their manager or department chair. Less than 32% felt that they could report concerns without fear of punitive action or retribution. | 14 Second victim |
| Lewis et al. (2013), USA [46] | To report the effect of medical errors on nurses | Integrative literature review 21 articles included Inclusion criteria and search strategy described Whittemore and Knafl’s methodology used | Characteristics of units were important in nurses’ experience of medical errors. Nurse characteristics were essential, for example, number of nursing practice years. Veteran nurses were more likely to make constructive changes. Two interventions were: (1) disclosure of a medical error to the patient; and (2) support available to the nurse. Responses to the intervention outcomes were: (1) burnout, including emotional exhaustion, depersonalisation and low personal accomplishment; (2) moral distress; (3) intention to leave the profession; and (4) positive constructive changes after medical errors. | 15.5 Second victim |
| Davies et al. (2015), UK [47] | To explore student midwives’ perceptions of what was traumatic for them and how they were supported after such events | Qualitative descriptive approach, using semi-structured interviews Student midwives (n = 11) | Five main themes: (1) Students’ anxiety about entering the profession including students being forced to adopt practices that devaluate their commitment; (2) Existential space between a patient and qualified midwife occupied by students, having traumatic tensions in the student role; (3) Emergency events were traumatic with students feeling unprepared and having too much responsibility; (4) Aftermath of emergency events concerning the impact of the event on students; and (5) Learning to cope related to the way student coped with such incidents, as well as other stresses in the role. | 13.5 Second victim |
| Harrison et al. (2015), UK/ USA [48] | To investigate: (a) the professional or personal disruption experienced after making an error; (b) the emotional response and coping strategies used; (c) the relationship between emotions and coping strategy selections; (d) influential factors in clinicians’ responses; and (e) perceptions of organisational support | Cross-sectional, cross-country survey, The Health Professional Experience of Error Questionnaire (HPEEQ) tool Nurses (n = 145), physicians (n = 120) | Professional and personal disruption reported as a result of making an error. Negative feelings common, but positive feelings like alertness, determination and attentiveness also identified. Emotional response and coping strategy selection appeared to differ by professional group; nurses had stronger negative feelings after an error, but selection did not differ by perceived harm or location. Problem-focused coping strategies were favoured. Organisational support services perceived as helpful, especially peers, but there were fears over confidentiality. Factors that influence clinician recovery should be considered in the provision of comprehensive support programs. | 17 Second victim |
| Seys et al. (2013b), USA [49] | To determine definitions of second victim, research the prevalence and the impact of adverse event on the second victim and the coping strategies used | Literature review 32 research articles and 9 non-research articles were identified | Second victims’ common reactions after adverse events can be emotional, cognitive and behavioural. The coping strategies used by second victims have an impact on their patients, colleagues and themselves. Defensive as well as constructive changes have been reported in practice after adverse events. It is critical that support networks are in place to protect the patient and involved healthcare providers when an adverse event occurs. | 15 Second victim |
| Edrees and Wu (2017) USA [50] | To assess the extent of the second victim problem in acute care hospitals, the availability of emotional support services and the need for organisational support programs. | In-depth semi-structured interviews. Patient safety representatives (n = 43). | All participants reported that they are aware of second victim problems. Almost all agreed that hospitals should have a support program for second victims. | 15,5 Second victim |
| Delacroix (2017), USA [51] | To discern nurse practitioners’ behaviours, perceptions and coping mechanisms in response to having made a medical error | Qualitative study, face-to-face semi-structured interviews (n = 10). | Four themes emerged from interviews: (1) The paradox of error victimisation, two subthemes were presented (fear for the patients’ welfare and fearing an uncertain professional future; (2) The primacy of responsibility and mindfulness, three subthemes were presented (I am responsible, acute reactions and mindfulness); (3) Yearning for forgiveness and supportive other, this theme was categorised in two subthemes (non-supportive just culture and seeking forgiveness and support); and (4) Coping with a new reality is context dependent, what was split up to two subthemes (atypical coping and constructive coping). | 15.5 Second victim |
| Van Gerven et al. (2016), Belgium [52] | To evaluate the prevalence and content of organisations’ support systems for healthcare professionals involved in an adverse event. | Quantitative descriptive design Dutch-speaking hospitals (n = 59) | Thirty organisations had a systematic plan to support second victims. The chief nursing officer was seen as one of the main contact people when something went wrong. In terms of the quality of the protocols, only a minority followed part of the international resources. | 16 Second and third victim |
| FIRST VICTIM ELEMENTS | ATTENTION OF REVEALING AN ADVERSE EVENT | HCPs listening to patients’ and family members’ concerns about an error Patients or family members fearing to speak up HCPs fearing to speak up HCPs’ empowering or disempowering patients and family members |
| COMMUNICATION AFTER AN ADVERSE EVENT | Considering cultural differences in communication Providing open communication Documenting in the patient records Observing different kind of family dynamics | |
| FIRST VICTIM SUPPORT | Emotionally supporting patients/families after adverse events Compensation support | |
| COMPLETE APOLOGY FOR FIRST VICTIMS | Apology with empathy Apology being an interactive process Presenter of apology HCPs/HCOs being sorry for adverse event experience Patient forgiving an adverse event Apology including learning from an event and a change in action First victims’ trust in healthcare services | |
| SECOND VICTIM ELEMENTS | SECOND VICTIM SUPPORT TYPE | Informal second victim support Formal second victim support Emotional second victim support |
| SECOND VICTIMS’ COPING STRATEGIES | Individuality of second victim coping strategies Seeking second victim emotional support coping strategies Problem-solving second victim coping strategies | |
| SECOND VICTIM SUPPORT SERVICES | Availability of second victim support services Second victim legal and counselling support Time away second victim support Open disclosure support | |
| SECOND VICTIMS’ PROFESSIONAL CHANGES AFTER ADVERSE EVENTS | Defensive changes after adverse events Constructive changes after adverse events | |
| SECOND VICTIMS’ LEARNING ABOUT ADVERSE EVENT PHENOMENON | Second victim learning from an adverse event Learning about second victim phenomenon Learning to communicate about adverse events | |
| THIRD VICTIM ELEMENTS | ORGANISATIONAL “ACTION AFTER ADVERSE EVENT” STRATEGY | Action after adverse event plan High moral communication strategy Active providing of support services Organisational apology policy Organisational learning from adverse event |
| ORGANISATIONAL “ACTION AFTER ADVERSE EVENT” INFRASTRUCTURE | Action after adverse event personnel Support infrastructure Processes of “action after adverse event” | |
| OPEN DISCLOSURE ABOUT ADVERSE EVENT | Process of open communication Content of open disclosure | |
| “ACTION AFTER ADVERSE EVENT” TRAINING | Patient safety training Adverse events related training Communication after adverse events training |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liukka, M.; Steven, A.; Vizcaya Moreno, M.F.; Sara-aho, A.M.; Khakurel, J.; Pearson, P.; Turunen, H.; Tella, S. Action after Adverse Events in Healthcare: An Integrative Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 4717. https://doi.org/10.3390/ijerph17134717
Liukka M, Steven A, Vizcaya Moreno MF, Sara-aho AM, Khakurel J, Pearson P, Turunen H, Tella S. Action after Adverse Events in Healthcare: An Integrative Literature Review. International Journal of Environmental Research and Public Health. 2020; 17(13):4717. https://doi.org/10.3390/ijerph17134717
Chicago/Turabian StyleLiukka, Mari, Alison Steven, M Flores Vizcaya Moreno, Arja M Sara-aho, Jayden Khakurel, Pauline Pearson, Hannele Turunen, and Susanna Tella. 2020. "Action after Adverse Events in Healthcare: An Integrative Literature Review" International Journal of Environmental Research and Public Health 17, no. 13: 4717. https://doi.org/10.3390/ijerph17134717
APA StyleLiukka, M., Steven, A., Vizcaya Moreno, M. F., Sara-aho, A. M., Khakurel, J., Pearson, P., Turunen, H., & Tella, S. (2020). Action after Adverse Events in Healthcare: An Integrative Literature Review. International Journal of Environmental Research and Public Health, 17(13), 4717. https://doi.org/10.3390/ijerph17134717