Are Household Expenditures on Food Groups Associated with Children’s Future Heights in Ethiopia, India, Peru, and Vietnam?

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Indicators
2.2.1. Household Food Expenditures
2.2.2. Child Anthropometry
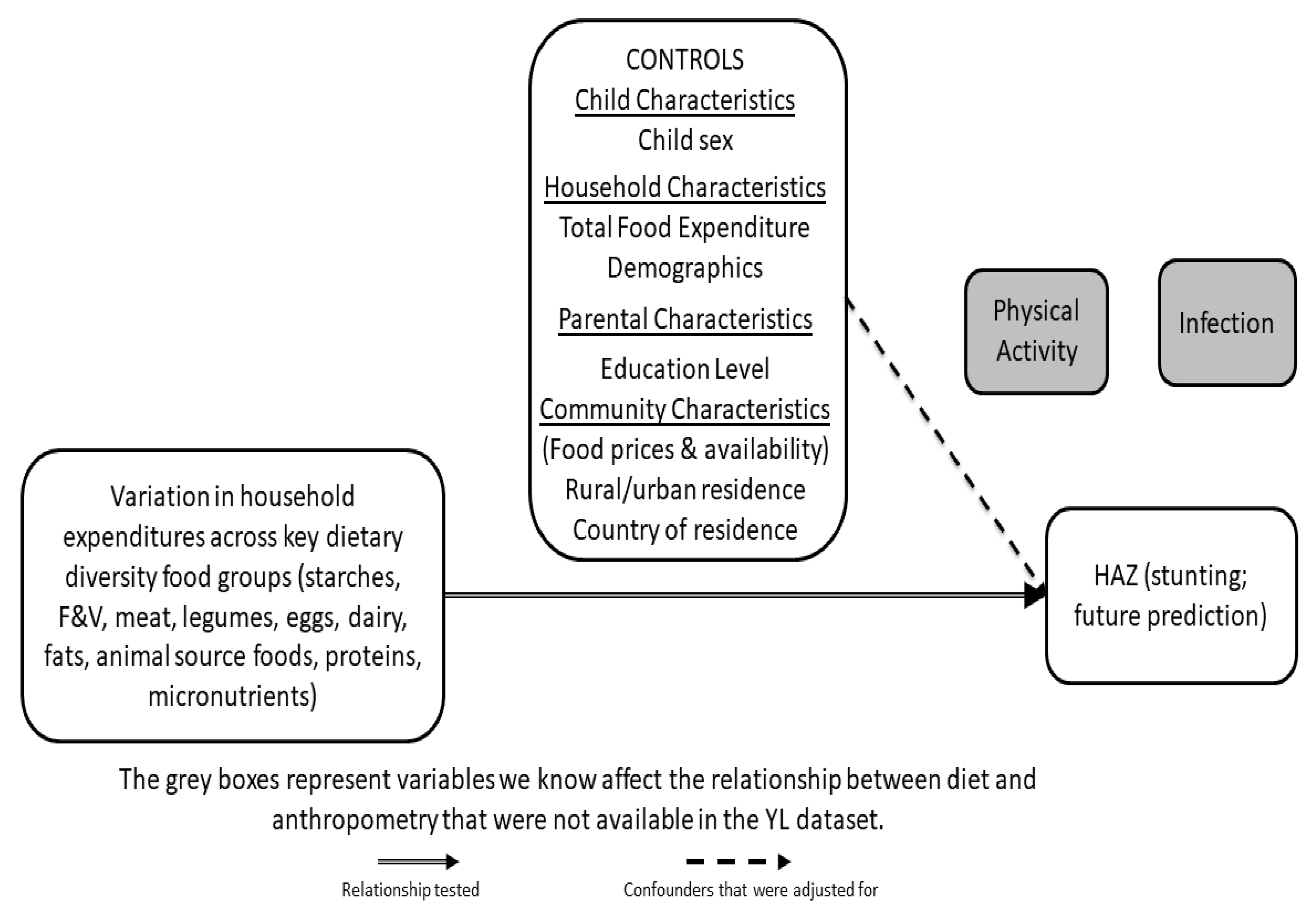
2.2.3. Control Variables
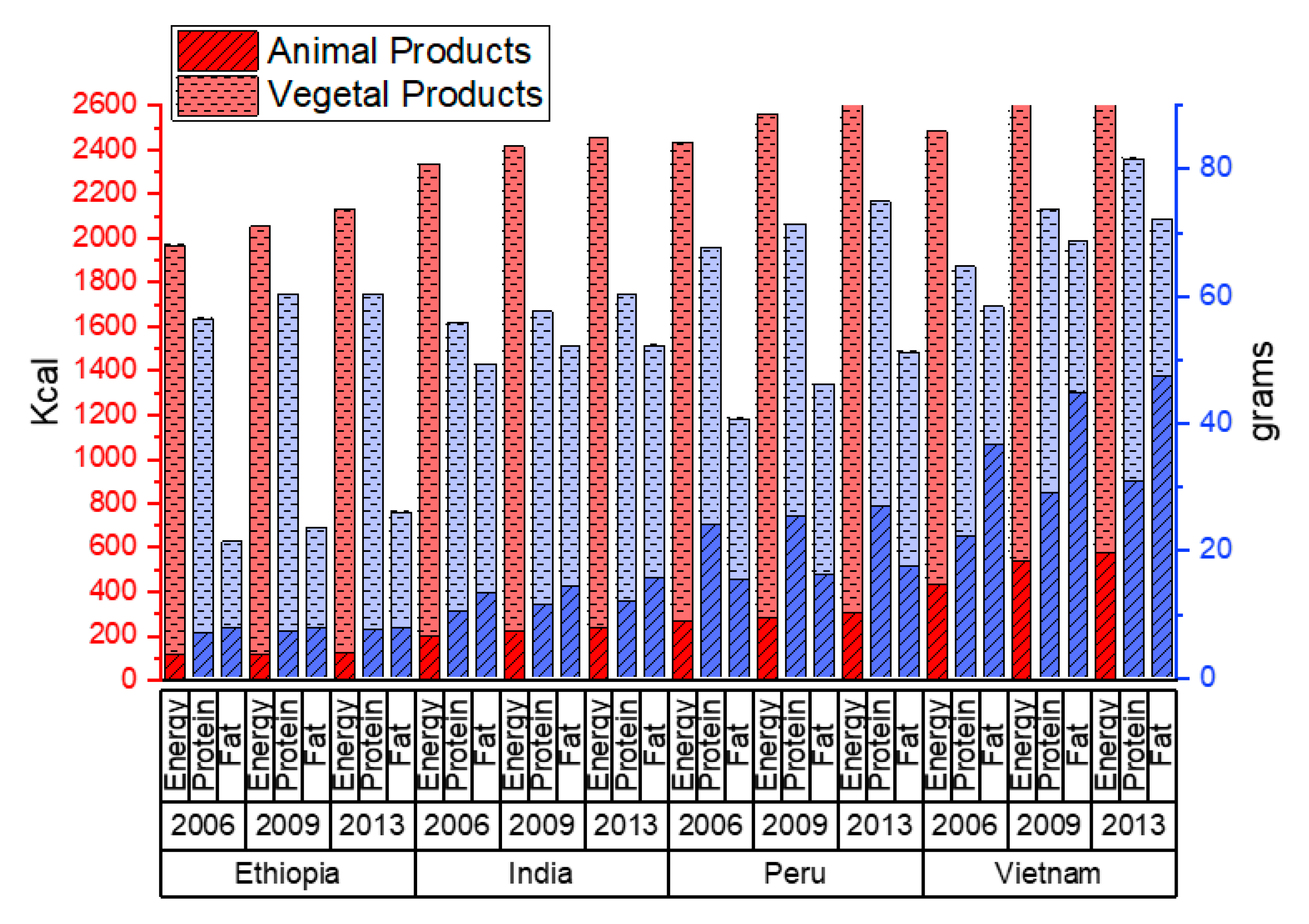
2.2.4. Country-Level Per-Capita Available Calories Data
2.3. Statistical Methods
2.4. Ethical Review
3. Results
3.1. Country-Level Food Energy and Macronutrient Availability
3.2. Descriptive Characteristics
3.3. Differences by Rural/Urban Residence
3.3.1. Ethiopia
3.3.2. India
3.3.3. Peru
3.3.4. Vietnam
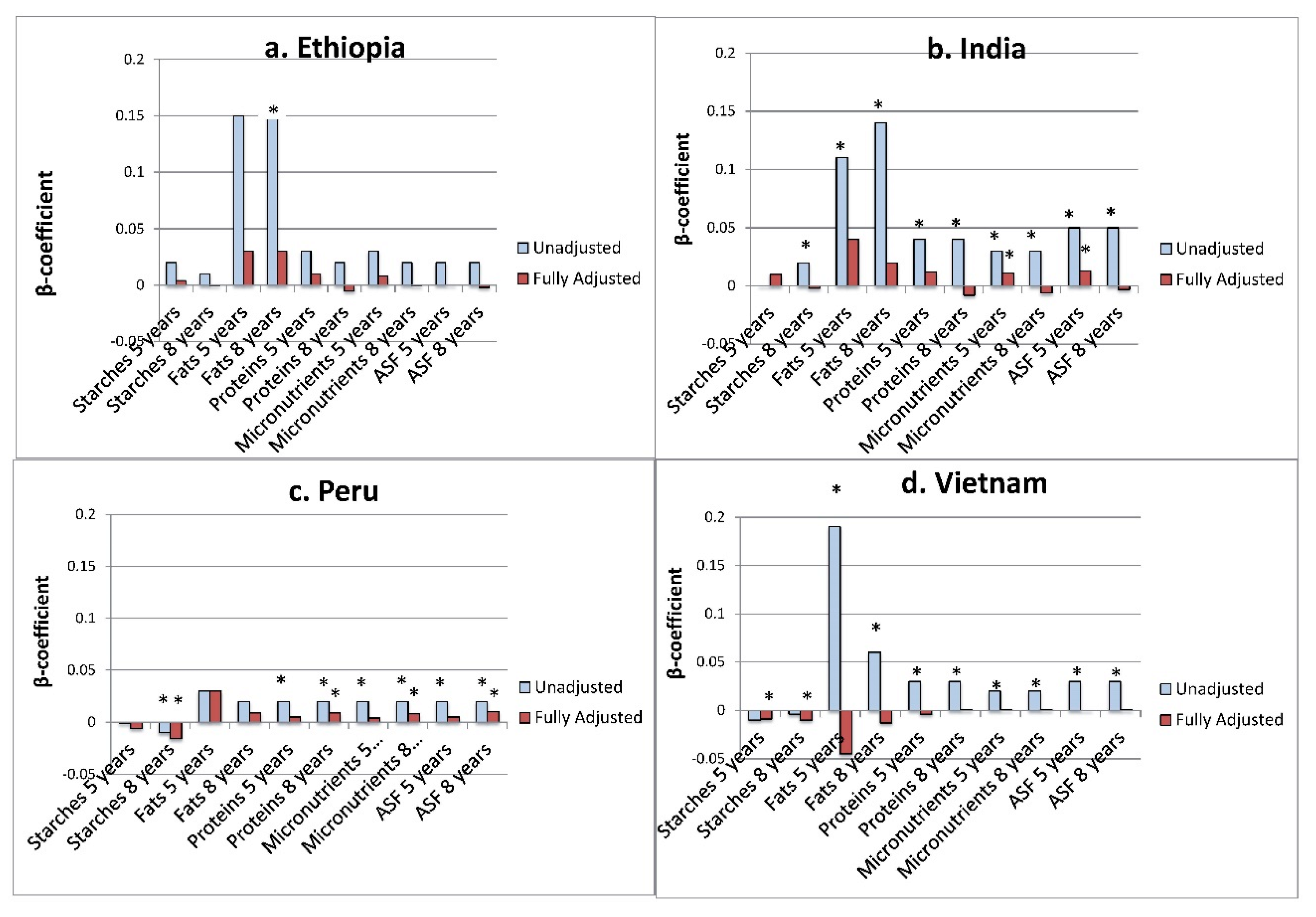
3.4. Unadjusted and Food Group-Only Models
3.4.1. Ethiopia
3.4.2. India
3.4.3. Peru
3.4.4. Vietnam
3.5. Adjusted Models Investigating Association of Key Food Expenditures and Future HAZ
3.5.1. Ethiopia
3.5.2. India
3.5.3. Peru
3.5.4. Vietnam
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- United Nations Children’s Fund; World Health Organization; The World Bank Group (Eds.) UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates, Levels and Trends in Child Malnutrition; Key Findings of the 2020 Edition; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Humphries, D.L.; Dearden, K.A.; Crookston, B.T.; Fernald, L.C.; Stein, A.D.; Woldehanna, T.; Penny, M.E.; Behrman, J.R.; The Young Lives Determinants and Consequences of Child Growth Project Team. Cross-Sectional and Longitudinal Associations between Household Food Security and Child Anthropometry at Ages 5 and 8 Years in Ethiopia, India, Peru, and Vietnam. J. Nutr. 2015, 145, 1924–1933. [Google Scholar]
- Martorell, R. The Nature of Child Malnutrition and its Long-Term Implications. Food Nutr. Bull. 1999, 20, 288–292. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Humphries, D.L.; Dearden, K.A.; Crookston, B.T.; Woldehanna, T.; Penny, M.E.; Behrman, J.R.; Young Lives Determinants and Consequences of Child Growth Project Team. Household food group expenditure patterns are associated with child anthropometry at ages 5, 8 and 12 years in Ethiopia, India, Peru and Vietnam. Econ. Hum. Biol. 2017, 26, 30–41. [Google Scholar] [CrossRef]
- Fiedler, J.L.; Lividini, K. Monitoring population diet quality and nutrition status with household consumption and expenditure surveys: Suggestions for a Bangladesh baseline. Food Secur. 2017, 9, 63–88. [Google Scholar] [CrossRef]
- Fiedler, J.L.; Lividini, K.; Bermudez, O.I.; Smitz, M.F. Household Consumption and Expenditures Surveys (HCES): A primer for food and nutrition analysts in low- and middle-income countries. Food Nutr. Bull. 2012, 33 (Suppl. 3), S170–S184. [Google Scholar] [CrossRef] [Green Version]
- Fiedler, J.L.; Martin-Prevel, Y.; Moursi, M. Relative costs of 24-hour recall and Household Consumption and Expenditures Surveys for nutrition analysis. Food Nutr. Bull. 2013, 34, 318–330. [Google Scholar] [CrossRef]
- Jariseta, Z.R.; Dary, O.; Fiedler, J.L.; Franklin, N. Comparison of estimates of the nutrient density of the diet of women and children in Uganda by Household Consumption and Expenditures Surveys (HCES) and 24-hour recall. Food Nutr. Bull. 2012, 33 (Suppl. 3), S199–S207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engle-Stone, R.; Brown, K.H. Comparison of a Household Consumption and Expenditures Survey with Nationally Representative Food Frequency Questionnaire and 24-hour Dietary Recall Data for Assessing Consumption of Fortifiable Foods by Women and Young Children in Cameroon. Food Nutr. Bull. 2015, 36, 211–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naska, A.; Vasdekis, V.G.; Trichopoulou, A. A preliminary assessment of the use of household budget survey data for the prediction of individual food consumption. Public Health Nutr. 2001, 4, 1159–1165. [Google Scholar] [PubMed]
- Dary, O.; Jariseta, Z.R. Validation of dietary applications of Household Consumption and Expenditures Surveys (HCES) against a 24-hour recall method in Uganda. Food Nutr. Bull. 2012, 33 (Suppl. 3), S190–S198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, I.; Ariana, P.; Petrou, S.; Penny, M.E.; Duc le, T.; Galab, S.; Woldehanna, T.; Escobal, J.A.; Plugge, E.; Boyden, J. Cohort profile: The Young Lives study. Int. J. Epidemiol. 2013, 42, 701–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oxford Department of International Development. Young Lives: A Longitudinal Study into Children and Youth around the World. Available online: https://www.younglives.org.uk/ (accessed on 26 June 2020).
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices Part II: Measurement; World Health Organization Department of Child and Adolescent Health and Development: Geneva, Switzerland, 2010. [Google Scholar]
- Kennedy, G.; Ballard, T.; Dop, M.; Nutrition Consumer Protection Division FAO. Guidelines for Measuring Household and Individual Dietary Diversity; Food and Agriculture Organization of the United Nations: Rome, Italy, 2013. [Google Scholar]
- Kennedy, G.; Fanou-Fogny, N.; Seghieri, C.; Arimond, M.; Koreissi, Y.; Dossa, R.; Kok, F.J.; Brouwer, I.D. Food groups associated with a composite measure of probability of adequate intake of 11 micronutrients in the diets of women in urban Mali. J. Nutr. 2010, 140, 2070S–2078S. [Google Scholar] [CrossRef] [Green Version]
- Glewwe, P.; Twum-Baah, K.A. The Distribution of Welfare in Ghana, 1987–1988; World Bank Living Standards Measurement Study Working Paper; The World Bank: Washington, DC, USA, 1991; Volume 75. [Google Scholar]
- Reifman, A.; Keyton, K. Winsorize. In Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010; pp. 1636–1638. [Google Scholar]
- WHO Child Growth Standards Based on Length/Height, Weight and Age. Acta Paediatr. 2006, 95, 76–85.
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- de Onis, M.; Blössner, M. WHO Global Database on Child Growth and Malnutrition; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Food and Agriculture Organization. FAOSTAT: Food and Agriculture Data. Available online: http://www.fao.org/faostat/en/#home (accessed on 31 May 2017).
- Al-Agha, A.; Al-Baradi, W.; Al-Rahmani, D.; Simbawa, B. Associations between various nutritional elements and weight, height and bmi in children and adolescents. J. Pat. Care 2016, 2, 2. [Google Scholar]
- Maitra, P.; Rammohan, A.; Ray, R.; Robitaille, M.-C. Food consumption patterns and malnourished Indian children: Is there a link? Food Policy 2013, 38, 70–81. [Google Scholar] [CrossRef]
- Van Stuijvenberg, M.E.; Nel, J.; Schoeman, S.E.; Lombard, C.J.; du Plessis, L.M.; Dhansay, M.A. Low intake of calcium and vitamin D, but not zinc, iron or vitamin A, is associated with stunting in 2- to 5-year-old children. Nutrition 2015, 31, 841–846. [Google Scholar] [CrossRef]
- Uauy, R.; Mize, C.E.; Castillo-Duran, C. Fat intake during childhood: Metabolic responses and effects on growth. Am. J. Clin. Nutr. 2000, 72 (Suppl. 5), 1354s–1360s. [Google Scholar] [CrossRef] [Green Version]
- Campbell, A.A.; de Pee, S.; Sun, K.; Kraemer, K.; Thorne-Lyman, A.; Moench-Pfanner, R.; Sari, M.; Akhter, N.; Bloem, M.W.; Semba, R.D. Household rice expenditure and maternal and child nutritional status in Bangladesh. J. Nutr. 2010, 140, 189S–194S. [Google Scholar] [CrossRef]
- Sari, M.; de Pee, S.; Bloem, M.W.; Sun, K.; Thorne-Lyman, A.L.; Moench-Pfanner, R.; Akhter, N.; Kraemer, K.; Semba, R.D. Higher household expenditure on animal-source and nongrain foods lowers the risk of stunting among children 0–59 months old in Indonesia: Implications of rising food prices. J. Nutr. 2010, 140, 195S–200S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busert, L.K.; Neuman, M.; Rehfuess, E.A.; Dulal, S.; Harthan, J.; Chaube, S.S.; Bhandari, B.; Costello, H.; Costello, A.; Manandhar, D.S.; et al. Dietary Diversity Is Positively Associated with Deviation from Expected Height in Rural Nepal. J. Nutr. 2016, 146, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Rah, J.H.; Akhter, N.; Semba, R.D.; de Pee, S.; Bloem, M.W.; Campbell, A.A.; Moench-Pfanner, R.; Sun, K.; Badham, J.; Kraemer, K. Low dietary diversity is a predictor of child stunting in rural Bangladesh. Eur. J. Clin. Nutr. 2010, 64, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
- Thorne-Lyman, A.L.; Valpiani, N.; Sun, K.; Semba, R.D.; Klotz, C.L.; Kraemer, K.; Akhter, N.; de Pee, S.; Moench-Pfanner, R.; Sari, M. Household dietary diversity and food expenditures are closely linked in rural Bangladesh, increasing the risk of malnutrition due to the financial crisis. J. Nutr. 2010, 140, 182S–188S. [Google Scholar] [CrossRef] [Green Version]
- Motbainor, A.; Worku, A.; Kumie, A. Stunting Is Associated with Food Diversity while Wasting with Food Insecurity among Underfive Children in East and West Gojjam Zones of Amhara Region, Ethiopia. PLoS ONE 2015, 10, e0133542. [Google Scholar] [CrossRef]
- Mahmudiono, T.; Sumarmi, S.; Rosenkranz, R.R. Household dietary diversity and child stunting in East Java, Indonesia. Asia Pac. J. Clin. Nutr. 2017, 26, 317–325. [Google Scholar]
- Abuya, B.A.; Ciera, J.; Kimani-Murage, E. Effect of mother’s education on child’s nutritional status in the slums of Nairobi. BMC Pediatr. 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Makoka, D.; Masibo, P.K. Is there a threshold level of maternal education sufficient to reduce child undernutrition? Evidence from Malawi, Tanzania and Zimbabwe. BMC Pediatr. 2015, 15, 96. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; de Pee, S.; Sun, K.; Sari, M.; Akhter, N.; Bloem, M.W. Effect of parental formal education on risk of child stunting in Indonesia and Bangladesh: A cross-sectional study. Lancet 2008, 371, 322–328. [Google Scholar] [CrossRef]
- Pfeiffer, J.; Gloyd, S.; Ramirez Li, L. Intrahousehold resource allocation and child growth in Mozambique: An ethnographic case-control study. Soc. Sci. Med. 2001, 53, 83–97. [Google Scholar] [CrossRef]
- Senbanjo, I.O.; Olayiwola, I.O.; Afolabi, W.A.; Senbanjo, O.C. Maternal and child under-nutrition in rural and urban communities of Lagos state, Nigeria: The relationship and risk factors. BMC Res. Notes 2013, 6, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, C.S.; Zanello, G.; Shankar, B. Rural-urban disparities in child nutrition in Bangladesh and Nepal. BMC Public Health 2013, 13, 581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mussa, R. A matching decomposition of the rural-urban difference in malnutrition in Malawi. Health Econ. Rev. 2014, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauludyani, A.V.; Fahmida, U.; Santika, O. Relationship between household expenditures on strategic foods and prevalence of undernutrition among children 0 to 23 months of age in Indonesia. Food Nutr. Bull. 2014, 35, 440–448. [Google Scholar] [CrossRef]
- Dewey, K.G.; Arimond, M. Lipid-based nutrient supplements: How can they combat child malnutrition? PLoS Med. 2012, 9, e1001314. [Google Scholar] [CrossRef]
- Dewey, K.G.; Mridha, M.K.; Matias, S.L.; Arnold, C.D.; Cummins, J.R.; Khan, M.S.; Maalouf-Manasseh, Z.; Siddiqui, Z.; Ullah, M.B.; Vosti, S.A. Lipid-based nutrient supplementation in the first 1000 d improves child growth in Bangladesh: A cluster-randomized effectiveness trial. Am. J. Clin. Nutr. 2017, 105, 944–957. [Google Scholar] [CrossRef] [Green Version]
- Mridha, M.K.; Matias, S.L.; Chaparro, C.M.; Paul, R.R.; Hussain, S.; Vosti, S.A.; Harding, K.L.; Cummins, J.R.; Day, L.T.; Saha, S.L.; et al. Lipid-based nutrient supplements for pregnant women reduce newborn stunting in a cluster-randomized controlled effectiveness trial in Bangladesh. Am. J. Clin. Nutr. 2016, 103, 236–249. [Google Scholar] [CrossRef] [Green Version]
- Ciresi, A.; Giordano, C. Vitamin D across growth hormone (GH) disorders: From GH deficiency to GH excess. Growth Horm. IGF Res. 2017, 33, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.L.; Stein, A.D. The Impact of Nutritional Interventions beyond the First 2 Years of Life on Linear Growth: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Perichart-Perera, O.; Balas-Nakash, M.; Rodriguez-Cano, A.; Munoz-Manrique, C.; Monge-Urrea, A.; Vadillo-Ortega, F. Correlates of dietary energy sources with cardiovascular disease risk markers in Mexican school-age children. J. Am. Diet. Assoc. 2010, 110, 253–260. [Google Scholar] [CrossRef]
- Villalpando, S.; Lara Zamudio, Y.; Shamah-Levy, T.; Mundo-Rosas, V.; Manzano, A.C.; Lamadrid-Figueroa, H. Substitution of whole cows’ milk with defatted milk for 4 months reduced serum total cholesterol, HDL-cholesterol and total apoB in a sample of Mexican school-age children (6–16 years of age). Br. J. Nutr. 2015, 114, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Dangour, A.D.; Watson, L.; Cumming, O.; Boisson, S.; Che, Y.; Velleman, Y.; Cavill, S.; Allen, E.; Uauy, R. Interventions to improve water quality and supply, sanitation and hygiene practices, and their effects on the nutritional status of children. Cochrane Database Syst. Rev. 2013, 8, CD009382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fikadu, T.; Assegid, S.; Dube, L. Factors associated with stunting among children of age 24 to 59 months in Meskan district, Gurage Zone, South Ethiopia: A case-control study. BMC Public Health 2014, 14, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinsugi, C.; Matsumura, M.; Karama, M.; Tanaka, J.; Changoma, M.; Kaneko, S. Factors associated with stunting among children according to the level of food insecurity in the household: A cross-sectional study in a rural community of Southeastern Kenya. BMC Public Health 2015, 15, 441. [Google Scholar] [CrossRef] [Green Version]
- Griffen, A.S. Height and calories in early childhood. Econ. Hum. Biol. 2016, 20, 55–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishna, A.; Fink, G.; Berkman, L.F.; Subramanian, S.V. Short- and long-run associations between birth weight and children’s height. Econ. Hum. Biol. 2016, 21, 156–166. [Google Scholar] [CrossRef]
- Dearden, K.A.; Schott, W.; Crookston, B.T.; Humphries, D.L.; Penny, M.E.; Behrman, J.R.; Young Lives Determinants and Consequences of Child Growth Project Team. Children with access to improved sanitation but not improved water are at lower risk of stunting compared to children without access: A cohort study in Ethiopia, India, Peru, and Vietnam. BMC Public Health 2017, 17, 110. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Ethiopia | 5 Years (Round 2) | 8 Years (Round 3) | 12 Years (Round 4) |
|---|---|---|---|
| n = 1744 | n = 1742 | n = 1733 | |
| HAZ, mean (95% CI) | −1.48 (−1.53, 1.43) | −1.22 (−1.27, −1.17) | −1.47 (−1.52, −1.42) |
| Female, n (%) | 815 (46.7) | 814 (46.7) | 809 (46.7) |
| Rural Residence, n (%) | 1047 (60.0) | 1046 (60.1) | 1028 (59.3) |
| Maternal Schooling, n (%) | |||
| No schooling | 887 (51.3) | 886 (51.3) | 884 (51.4) |
| 1–6 years | 521 (30.1) | 520 (30.1) | 520 (30.3) |
| 7–12 years | 290 (16.8) | 290 (16.8) | 284 (16.5) |
| 12+ years | 32 (1.9) | 32 (1.9) | 31 (1.8) |
| Paternal Schooling, n (%) | |||
| No schooling | 432 (25.8) | 431 (25.8) | 431 (25.9) |
| 1–6 years | 768 (45.9) | 767 (45.9) | 768 (46.2) |
| 7–12 years | 372 (22.3) | 372 (22.3) | 365 (21.9) |
| 12+ years | 100 (6.0) | 100 (6.0) | 100 (6.0) |
| India | 5 Years (Round 2) | 8 Years (Round 3) | 12 Years (Round 4) |
| n = 1804 | n = 1806 | n = 1801 | |
| HAZ, mean (95% CI) | 1.65 (−1.70, −1.61) | −1.46 (−1.50, -1.41) | −1.44 (−1.49, −1.39) |
| Female, N (%) | 842 (46.7) | 842 (46.6) | 837 (46.5) |
| Rural Residence, N (%) | 1337 (74.1) | 1324 (73.3) | 1299 (72.1) |
| Maternal Schooling, N (%) | |||
| No schooling | 914 (50.8) | 916 (50.8) | 913 (50.8) |
| 1-6 years | 363 (20.2) | 363 (20.1) | 363 (20.2) |
| 7-12 years | 475 (26.4) | 475 (26.4) | 473 (26.3) |
| 12+ years | 48 (2.7) | 48 (2.7) | 48 (2.7) |
| Paternal Schooling, N (%) | |||
| No schooling | 591 (32.8) | 593 (32.9) | 592 (32.9) |
| 1-6 years | 435 (24.2) | 435 (24.1) | 434 (24.1) |
| 7-12 years | 647 (35.9) | 647 (35.9) | 644 (35.8) |
| 12+ years | 128 (7.1) | 128 (7.1) | 128 (7.1) |
| Peru | 5 Years (Round 2) | 8 Years (Round 3) | 12 Years (Round 4) |
| n= 1795 | n= 1788 | n= 1775 | |
| HAZ, mean (95% CI) | −1.53 (−1.58, −1.48) | −1.15 (−1.20, −1.10) | −1.02 (−1.07, −0.97) |
| Female, n (%) | 896 (49.9) | 896 (50.1) | 883 (49.8) |
| Rural Residence, n (%) | 795 (44.3) | 498 (27.9) | 471 (26.5) |
| Maternal Schooling, n (%) | |||
| No schooling | 149 (8.4) | 149 (8.4) | 145 (8.2) |
| 1–6 years | 640 (35.9) | 637 (35.9) | 634 (36.0) |
| 7–12 years | 751 (42.2) | 748 (42.2) | 744 (42.3) |
| 12+ years | 241 (13.5) | 240 (13.5) | 238 (13.5) |
| Paternal Schooling, n (%) | |||
| No schooling | 24 (1.4) | 24 (1.4) | 24 (1.4) |
| 1–6 years | 553 (31.8) | 552 (31.9) | 546 (31.7) |
| 7–12 years | 855 (49.2) | 850 (49.1) | 846 (49.2) |
| 12+ years | 307 (17.7) | 306 (17.7) | 305 (17.7) |
| Vietnam | 5 years (Round 2) | 8 years (Round 3) | 12 years (Round 4) |
| n= 1788 | n= 1754 | n= 1684 | |
| HAZ, mean (95% CI) | −1.35 (−1.40, −1.30) | −1.11 (−1.16, −1.06) | −1.06 (−1.11, −1.00) |
| Female, n (%) | 871 (48.7) | 854 (48.7) | 818 (48.6) |
| Rural Residence, n (%) | 1435 (80.3) | 1418 (80.8) | 1369 (81.3) |
| Maternal Schooling, n (%) | |||
| No schooling | 181 (10.2) | 176 (10.1) | 177 (10.6) |
| 1–6 years | 637 (35.9) | 627 (36.0) | 611 (36.6) |
| 7–12 years | 832 (46.9) | 816 (46.9) | 771 (46.2) |
| 12+ years | 124 (7.0) | 121 (7.0) | 111 (6.7) |
| Paternal Schooling, n (%) | |||
| No schooling | 119 (6.8) | 113 (6.6) | 114 (6.9) |
| 1–6 years | 550 (31.6) | 543 (31.7) | 525 (31.9) |
| 7–12 years | 926 (53.1) | 910 (53.2) | 871 (53.0) |
| 12+ years | 148 (8.5) | 145 (8.5) | 135 (8.2) |
| Country and Food Groups | 5 Years-Rural | 5 Years-Urban | 8 Years-Rural | 8 Years-Urban | 12 Years-Rural | 12 Years-Urban |
|---|---|---|---|---|---|---|
| Ethiopia | Median (IQR 1) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) |
| Starches | 7.67 (7.49) | 9.44 (7.88) *** | 8.39 (8.11) | 10.30 (7.95) *** | 8.55 (7.93) | 10.59 (6.08) *** |
| FV | 0.36 (0.74) | 0.53 (0.78) *** | 0.29 (0.75) | 0.51 (0.73) *** | 0.41 (0.63) | 0.87 (1.19) *** |
| Meat | 0.00 (0.52) | 0.00 (1.46) ** | 0.00 (0.00) | 0.00 (1.43) *** | 0.00 (0.38) | 0.00 (2.77) *** |
| Legumes | 0.80 (1.65) | 1.16 (1.46) *** | 0.86 (1.17) | 0.92 (0.96) ** | 0.83 (1.11) | 1.27 (1.38) *** |
| Eggs | 0.00 (0.00) | 0.00 (0.28) ** | 0.00 (0.22) | 0.00 (0.33) | 0.00 (0.23) | 0.00 (0.56) *** |
| Dairy | 0.00 (1.14) | 0.00 (1.18) | 0.00 (1.16) | 0.00 (1.05) | 0.00 (1.38) | 0.00 (1.38) |
| Fats | 0.73 (0.81) | 1.38 (1.50) *** | 0.57 (0.59) | 1.10 (1.11) *** | 0.57 (0.53) | 1.30 (1.25) *** |
| India | ||||||
| Starches | 7.03 (4.64) | 5.39 (4.24) *** | 5.27 (5.26) | 6.22 (5.24) ** | 5.17 (5.12) | 6.04 (5.20) * |
| FV | 2.52 (2.11) | 2.79 (2.28) ** | 3.21 (2.58) | 3.59 (2.66) *** | 3.57 (2.42) | 4.05 (2.58) *** |
| Meat | 1.98 (2.97) | 2.05 (2.77) | 2.29 (2.70) | 2.17 (2.82) ** | 2.19 (2.45) | 2.15 (3.09) |
| Legumes | 1.21 (1.00) | 0.87 (0.71) *** | 1.44 (1.22) | 1.32 (1.07) ** | 1.02 (0.81) | 0.95 (0.74) ** |
| Eggs | 0.31 (0.57) | 0.37 (0.39) * | 0.31 (0.52) | 0.35 (0.54) | 0.30 (0.52) | 0.30 (0.50) |
| Dairy | 0.91 (2.12) | 2.32 (2.30) *** | 0.89 (1.81) | 2.96 (3.32) *** | 1.36 (2.18) | 2.90 (2.72) *** |
| Fats | 1.66 (1.01) | 1.73 (1.05) | 1.50 (1.19) | 1.83 (1.35) *** | 1.56 (1.18) | 1.82 (1.19) *** |
| Peru | ||||||
| Starches | 13.59 (8.94) | 13.37 (7.33) | 16.83 (9.65) | 13.56 (7.36) *** | 17.95 (11.98) | 14.19 (8.45) *** |
| FV | 1.80 (2.05) | 2.96 (3.25) *** | 2.96 (3.15) | 3.36 (3.65) ** | 3.93 (3.87) | 4.57 (4.86) *** |
| Meat | 4.51 (7.66) | 8.53 (8.20) *** | 7.54 (9.60) | 9.63 (9.08) *** | 9.71 (11.14) | 11.13 (9.75) *** |
| Legumes | 1.25 (1.75) | 1.13 (1.28) | 1.78 (1.97) | 1.24 (1.42) *** | 2.06 (2.25) | 1.36 (1.54) *** |
| Eggs | 0.77 (1.04) | 1.05 (1.12) *** | 1.03 (1.21) | 1.17 (1.14) | 1.53 (1.64) | 1.38 (1.29) ** |
| Dairy | 2.17 (3.82) | 5.25 (6.50) *** | 3.18 (4.54) | 4.48 (5.26) *** | 4.04 (4.48) | 5.02 (5.68) *** |
| Fats | 1.29 (1.16) | 1.18 (0.91) *** | 1.69 (1.33) | 1.39 (1.08) *** | 1.69 (1.73) | 1.25 (1.34) *** |
| Vietnam | ||||||
| Starches | 8.90 (4.41) | 8.11 (4.74) *** | 9.97 (5.46) | 8.78 (5.75) *** | 10.82 (6.91) | 11.53 (10.04) * |
| FV | 3.12 (3.02) | 4.89 (5.87) *** | 3.61 (3.40) | 6.69 (6.47) *** | 4.05 (4.28) | 7.60 (8.07) *** |
| Meat | 8.90 (8.01) | 12.30 (11.15) *** | 10.19 (8.81) | 15.97 (12.74) *** | 13.68 (11.93) | 21.07 (19.72) *** |
| Legumes | 0.00 (0.30) | 0.00 (0.71) *** | 0.00 (0.49) | 0.00 (0.43) | 0.00 (0.37) | 0.00 (0.68) *** |
| Eggs | 0.80 (1.54) | 0.91 (1.06) * | 0.60 (1.40) | 1.20 (1.12) *** | 1.32 (1.39) | 1.44 (1.34) ** |
| Dairy | 0.61 (3.24) | 5.98 (9.61) *** | 2.03 (5.62) | 4.98 (8.59) *** | 0.00 (3.26) | 4.43 (11.47) *** |
| Fats | 0.75 (0.68) | 1.03 (0.70) *** | 1.21 (1.16) | 1.57 (1.00) *** | 1.51 (1.49) | 2.30 (2.21) *** |
| (a) Ethiopia—Expenditures at 5 Years with HAZ at 8 Years as the Dependent Variable—Predicting Future HAZ at Round 3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Food Groups | Single Food Groups | Protein | Micronutrients | ASFs | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0159 | R-Sq: 0.0191 | R-Sq: 0.0055 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.12 | <0.001 | 0.0077 | 0.08 | 0.011 | ||||
| Legumes | 0.08 | <0.001 | 0.0136 | 0.08 | <0.001 | 0.07 | <0.001 | ||
| Meat | 0.02 | 0.046 | 0.0018 | 0.004 | 0.73 | 0.001 | 0.922 | 0.01 | 0.404 |
| Eggs | 0.19 | 0.007 | 0.0038 | 0.09 | 0.218 | 0.07 | 0.388 | 0.13 | 0.06 |
| Dairy | 0.04 | 0.006 | 0.004 | 0.03 | 0.094 | 0.02 | 0.28 | 0.03 | 0.086 |
| Starches | 0.02 | <0.001 | 0.0123 | ||||||
| Fats | 0.15 | <0.001 | 0.0249 | ||||||
| Proteins | 0.03 | <0.001 | 0.0108 | ||||||
| Micronutrients | 0.03 | <0.001 | 0.0128 | ||||||
| Animal Source Foods | 0.02 | 0.002 | 0.0049 | ||||||
| Ethiopia—Expenditures at 8 Years with HAZ at 12 Years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrients | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0036 | R-Sq: 0.0107 | R-Sq: 0.0042 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.13 | <0.001 | 0.0089 | 0.12 | <0.001 | ||||
| Legumes | 0.01 | 0.623 | −0.0004 | 0.005 | 0.826 | −0.01 | 0.816 | ||
| Meat | 0.04 | 0.002 | 0.0053 | 0.04 | 0.004 | 0.04 | 0.008 | 0.04 | 0.004 |
| Eggs | 0.07 | 0.278 | 0.0001 | −0.005 | 0.942 | −0.05 | 0.481 | −0.004 | 0.796 |
| Dairy | 0.02 | 0.252 | 0.0002 | 0.004 | 0.816 | −0.01 | 0.653 | 0.004 | 0.956 |
| Starches | 0.01 | <0.001 | 0.0066 | ||||||
| Fats | 0.16 | <0.001 | 0.0183 | ||||||
| Proteins | 0.02 | 0.009 | 0.0035 | ||||||
| Micronutrients | 0.02 | 0.001 | 0.0055 | ||||||
| Animal Source Foods | 0.02 | 0.006 | 0.0039 | ||||||
| (b) India—Expenditures at 5 Years with HAZ at 8 Years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrient | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0419 | R-Sq: 0.0416 | R-Sq: 0.0429 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.02 | 0.051 | 0.0016 | −0.01 | 0.5 | ||||
| Legumes | −0.02 | 0.519 | −0.0003 | −0.04 | 0.147 | −0.03 | 0.197 | ||
| Meat | 0.03 | 0.003 | 0.0044 | 0.02 | 0.046 | 0.02 | 0.039 | 0.02 | 0.066 |
| Eggs | 0.09 | 0.166 | 0.0005 | −0.03 | 0.692 | −0.02 | 0.793 | −0.04 | 0.599 |
| Dairy | 0.1 | <0.001 | 0.0405 | 0.1 | <0.001 | 0.1 | <0.001 | 0.1 | <0.001 |
| Starches | 0.0001 | 0.982 | −0.0006 | ||||||
| Fats | 0.11 | <0.001 | 0.011 | ||||||
| Proteins | 0.04 | <0.001 | 0.0232 | ||||||
| Micronutrients | 0.03 | <0.001 | 0.0182 | ||||||
| Animal Source Foods | 0.05 | <0.001 | 0.0281 | ||||||
| India—Expenditures at 8 Years with HAZ at 12 Years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrients | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.048 | R-Sq: 0.0479 | R-Sq: 0.0467 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.04 | <0.001 | 0.0069 | 0.01 | 0.365 | ||||
| Legumes | −0.004 | 0.85 | −0.0005 | −0.04 | 0.068 | −0.04 | 0.047 | ||
| Meat | 0.02 | 0.119 | 0.0008 | 0.01 | 0.275 | 0.01 | 0.347 | 0.01 | 0.394 |
| Eggs | 0.14 | 0.035 | 0.002 | 0.01 | 0.909 | 0.001 | 0.986 | 0.001 | 0.988 |
| Dairy | 0.1 | <0.001 | 0.0473 | 0.1 | <0.001 | 0.1 | <0.001 | 0.1 | <0.001 |
| Starches | 0.02 | <0.001 | 0.0061 | ||||||
| Fats | 0.14 | <0.001 | 0.0212 | ||||||
| Proteins | 0.04 | <0.001 | 0.0219 | ||||||
| Micronutrients | 0.03 | <0.001 | 0.0213 | ||||||
| Animal Source Foods | 0.05 | <0.001 | 0.0276 | ||||||
| (c) Peru—Expenditures at 5 Years with HAZ at 8 Years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrient | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0758 | R-Sq: 0.0774 | R-Sq: 0.0737 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.06 | <0.001 | 0.0334 | 0.02 | 0.047 | ||||
| Legumes | 0.01 | 0.59 | −0.0004 | −0.04 | 0.026 | −0.04 | 0.016 | ||
| Meat | 0.02 | <0.001 | 0.0304 | 0.01 | 0.009 | 0.01 | 0.066 | 0.01 | 0.02 |
| Eggs | 0.09 | <0.001 | 0.0095 | −0.004 | 0.88 | −0.01 | 0.675 | −0.01 | 0.665 |
| Dairy | 0.06 | <0.001 | 0.0718 | 0.05 | <0.001 | 0.05 | <0.001 | 0.05 | <0.001 |
| Starches | −0.001 | 0.785 | −0.0005 | ||||||
| Fats | 0.03 | 0.238 | 0.0002 | ||||||
| Proteins | 0.02 | <0.001 | 0.0544 | ||||||
| Micronutrients | 0.02 | <0.001 | 0.0569 | ||||||
| Animal Source Foods | 0.02 | <0.001 | 0.0582 | ||||||
| Peru—Expenditures at 8 Years with HAZ at 12 Years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrient | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0747 | R-Sq: 0.0775 | R-Sq: 0.0634 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.06 | <0.001 | 0.0292 | 0.02 | 0.013 | ||||
| Legumes | −0.04 | 0.04 | 0.0019 | −0.09 | <0.001 | −0.09 | <0.001 | ||
| Meat | 0.03 | <0.001 | 0.0393 | 0.02 | <0.001 | 0.02 | <0.001 | 0.02 | <0.001 |
| Eggs | 0.09 | <0.001 | 0.0073 | 0.01 | 0.733 | 0.0001 | 0.995 | −0.01 | 0.724 |
| Dairy | 0.06 | <0.001 | 0.0529 | 0.05 | <0.001 | 0.04 | <0.001 | 0.05 | <0.001 |
| Starches | −0.01 | 0.027 | 0.0023 | ||||||
| Fats | 0.02 | 0.359 | −0.0001 | ||||||
| Proteins | 0.02 | <0.001 | 0.0506 | ||||||
| Micronutrients | 0.02 | <0.001 | 0.0538 | ||||||
| Animal Source Foods | 0.02 | <0.001 | 0.058 | ||||||
| (d) Vietnam—Expenditures at 5 Years with HAZ at 8 Years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrient | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0932 | R-Sq: 0.0972 | R-Sq: 0.0937 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.07 | <0.001 | 0.0584 | 0.02 | 0.004 | ||||
| Legumes | 0.13 | <0.001 | 0.0065 | 0.01 | 0.734 | 0.01 | 0.793 | ||
| Meat | 0.03 | <0.001 | 0.0619 | 0.02 | <0.001 | 0.02 | <0.001 | 0.02 | <0.001 |
| Eggs | 0.09 | <0.001 | 0.0093 | 0.02 | 0.464 | 0.004 | 0.858 | 0.02 | 0.452 |
| Dairy | 0.05 | <0.001 | 0.0765 | 0.04 | <0.001 | 0.03 | <0.001 | 0.04 | <0.001 |
| Starches | −0.01 | 0.364 | −0.0001 | ||||||
| Fats | 0.19 | <0.001 | 0.0172 | ||||||
| Proteins | 0.03 | <0.001 | 0.0925 | ||||||
| Micronutrients | 0.02 | <0.001 | 0.097 | ||||||
| Animal Source Foods | 0.03 | <0.001 | 0.0923 | ||||||
| Vietnam—Expenditures at 8 years with HAZ at 12 years as the Dependent Variable | |||||||||
| Food Groups | Single Food Groups | Protein | Micronutrient | ASF | |||||
| Coefficient | p-Value | R-Sq | R-Sq: 0.0985 | R-Sq: 0.1008 | R-Sq: 0.0986 | ||||
| Coefficient | p-Value | Coefficient | p-Value | Coefficient | p-Value | ||||
| Fruits and Vegetables | 0.06 | <0.001 | 0.0439 | 0.02 | 0.025 | ||||
| Legumes | 0.13 | 0.008 | 0.0037 | 0.04 | 0.369 | 0.03 | 0.484 | ||
| Meat | 0.04 | <0.001 | 0.0817 | 0.03 | <0.001 | 0.03 | <0.001 | 0.03 | <0.001 |
| Eggs | 0.21 | <0.001 | 0.0458 | 0.13 | <0.001 | 0.12 | <0.001 | 0.13 | <0.001 |
| Dairy | 0.03 | <0.001 | 0.0252 | 0.01 | 0.107 | 0.005 | 0.325 | 0.01 | 0.082 |
| Starches | −0.004 | 0.505 | −0.0003 | ||||||
| Fats | 0.06 | 0.015 | 0.003 | ||||||
| Proteins | 0.03 | <0.001 | 0.0822 | ||||||
| Micronutrients | 0.02 | <0.001 | 0.0856 | ||||||
| Animal Source Foods | 0.03 | <0.001 | 0.0818 | ||||||
| (a) Ethiopia | Expenditures at 5 Years Associated with HAZ at 8 Years | Expenditures at 8 Years Associated with HAZ at 12 Years | ||||||
|---|---|---|---|---|---|---|---|---|
| Fats | Model 1a | Model 2a | Model 1b | Model 2b | ||||
| Model Adjusted R-Squared | 0.0249 | 0.0629 | 0.0183 | 0.0575 | ||||
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| Fats | 0.15 | <0.001 | 0.03 | 0.291 | 0.16 | <0.001 | 0.02 | 0.627 |
| Individual Variable | ||||||||
| Female | 0.13 | 0.006 | −0.02 | 0.673 | ||||
| Community Variable | ||||||||
| Rural/Urban Status | −0.19 | 0.001 | −0.30 | <0.001 | ||||
| Household Variable | ||||||||
| Total Food Expenditures | 0.01 | 0.01 | 0.003 | 0.204 | ||||
| Maternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.14 | 0.017 | 0.15 | 0.008 | ||||
| 7–12 years | 0.2 | 0.024 | 0.18 | 0.036 | ||||
| 12+ years | −0.02 | 0.903 | 0.12 | 0.522 | ||||
| Paternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.14 | 0.016 | 0.09 | 0.125 | ||||
| 7–12 years | 0.19 | 0.018 | ||||||
| 12+ years | 0.26 | 0.039 | ||||||
| (b) India | Expenditures at 5 Years Associated with HAZ at 8 Years | Expenditures at 8 Years Associated with HAZ at 12 Years | ||||||
| Fats | Model 1a | Model 2a | Model 1b | Model 2b | ||||
| Model Adjusted R-Squared | 0.011 | 0.1215 | 0.0212 | 0.1008 | ||||
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| Fats | 0.11 | <0.001 | 0.07 | 0.015 | 0.14 | <0.001 | 0.06 | 0.025 |
| Individual Variable | ||||||||
| Female | 0.12 | 0.005 | 0.04 | 0.376 | ||||
| Community Variable | ||||||||
| Rural/Urban Status | −0.40 | <0.001 | −0.34 | <0.001 | ||||
| Household Variable | ||||||||
| Total Food Expenditures | 0.001 | 0.795 | 0.001 | 0.572 | ||||
| Maternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.17 | 0.005 | 0.11 | 0.075 | ||||
| 7–12 years | 0.22 | <0.001 | 0.12 | 0.063 | ||||
| 12+ years | 0.6 | <0.001 | 0.48 | 0.003 | ||||
| Paternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.11 | 0.071 | 0.17 | 0.005 | ||||
| 7–12 years | 0.18 | 0.003 | 0.29 | <0.001 | ||||
| 12+ years | 0.37 | <0.001 | 0.4 | <0.001 | ||||
| (c) Peru | Expenditures at 5 Years Associated with HAZ at 8 Years | Expenditures at 8 Years Associated with HAZ at 12 Years | ||||||
| Fats | Model 1a | Model 2a | Model 1b | Model 2b | ||||
| Model Adjusted R-Squared | 0.0002 | 0.2194 | −0.0001 | 0.2003 | ||||
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| Fats | 0.03 | 0.238 | 0.05 | 0.042 | 0.02 | 0.359 | 0.04 | 0.101 |
| Individual Variable | ||||||||
| Female | 0.03 | 0.511 | −0.06 | 0.206 | ||||
| Community Variable | ||||||||
| Rural/Urban Status | −0.47 | <0.001 | −0.47 | <0.001 | ||||
| Household Variable | ||||||||
| Total Food Expenditures | −0.0003 | 0.727 | 0.003 | <0.001 | ||||
| Maternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.26 | 0.003 | 0.24 | 0.013 | ||||
| 7–12 years | 0.64 | <0.001 | 0.6 | <0.001 | ||||
| 12+ years | 0.84 | <0.001 | 0.72 | <0.001 | ||||
| Paternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.11 | 0.57 | -0.001 | 0.997 | ||||
| 7–12 years | 0.2 | 0.296 | 0.16 | 0.443 | ||||
| 12+ years | 0.35 | 0.085 | 0.37 | 0.094 | ||||
| (d) Vietnam | Expenditures at 5 Years Associated with HAZ at 8 Years | Expenditures at 8 Years Associated with HAZ at 12 Years | ||||||
| Starches | Model 1a | Model 2a | Model 1b | Model 2b | ||||
| Model Adjusted R-Squared | −0.0001 | 0.2013 | −0.0003 | 0.175 | ||||
| β | p-Value | β | p-Value | β | p-Value | Β | p-Value | |
| Starches | −0.01 | 0.364 | −0.01 | 0.014 | −0.004 | 0.505 | −0.01 | 0.047 |
| Individual Variable | ||||||||
| Female | 0.09 | 0.056 | 0.01 | 0.852 | ||||
| Community Variable | ||||||||
| Rural/Urban Status | −0.36 | <0.001 | −0.32 | <0.001 | ||||
| Household Variable | ||||||||
| Total Food Expenditures | 0.01 | <0.001 | 0.01 | <0.001 | ||||
| Maternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.55 | <0.001 | 0.65 | <0.001 | ||||
| 7–12 years | 0.64 | <0.001 | 0.68 | <0.001 | ||||
| 12+ years | 0.96 | <0.001 | 0.92 | <0.001 | ||||
| Paternal Education | ||||||||
| No Schooling | Reference | Reference | ||||||
| 1–6 years | 0.32 | 0.002 | 0.22 | 0.061 | ||||
| 7–12 years | 0.39 | <0.001 | 0.37 | 0.003 | ||||
| 12+ years | 0.5 | 0.001 | 0.54 | 0.001 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weingarten, S.E.; Dearden, K.A.; Crookston, B.T.; Penny, M.E.; Behrman, J.R.; Humphries, D.L. Are Household Expenditures on Food Groups Associated with Children’s Future Heights in Ethiopia, India, Peru, and Vietnam? Int. J. Environ. Res. Public Health 2020, 17, 4739. https://doi.org/10.3390/ijerph17134739
Weingarten SE, Dearden KA, Crookston BT, Penny ME, Behrman JR, Humphries DL. Are Household Expenditures on Food Groups Associated with Children’s Future Heights in Ethiopia, India, Peru, and Vietnam? International Journal of Environmental Research and Public Health. 2020; 17(13):4739. https://doi.org/10.3390/ijerph17134739
Chicago/Turabian StyleWeingarten, Sarah E., Kirk A. Dearden, Benjamin T. Crookston, Mary E. Penny, Jere R. Behrman, and Debbie L. Humphries. 2020. "Are Household Expenditures on Food Groups Associated with Children’s Future Heights in Ethiopia, India, Peru, and Vietnam?" International Journal of Environmental Research and Public Health 17, no. 13: 4739. https://doi.org/10.3390/ijerph17134739
APA StyleWeingarten, S. E., Dearden, K. A., Crookston, B. T., Penny, M. E., Behrman, J. R., & Humphries, D. L. (2020). Are Household Expenditures on Food Groups Associated with Children’s Future Heights in Ethiopia, India, Peru, and Vietnam? International Journal of Environmental Research and Public Health, 17(13), 4739. https://doi.org/10.3390/ijerph17134739