Rowing Training in Breast Cancer Survivors: A Longitudinal Study of Physical Fitness

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Breast Cancer: Prevention and Control. Available online: https://www.who.int/topics/cancer/breastcancer/en (accessed on 11 April 2020).
- International Agency for Research on Cancer. Cancer Today. Available online: https://gco.iarc.fr/today/home (accessed on 14 April 2020).
- International Agency for Research on Cancer. Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow/home (accessed on 14 April 2020).
- Cantarero-Villanueva, I.; Fernández-Lao, C.; Del Moral-Avila, R.; Fernández-de-Las-Peñas, C.; Feriche-Fernández-Castanys, M.B.; Arroyo-Morales, M. Effectiveness of core stability exercises and recovery myofascial release massage on fatigue in breast cancer survivors: A randomized controlled clinical trial. Evid. Based Complement. Alternat. Med. 2012, 2012, 620619. [Google Scholar] [CrossRef] [Green Version]
- Anthis, N.J.; Kavanaugh-Lynch, M.H.E. The Global Challenge to Prevent Breast Cancer: Surfacing New Ideas to Accelerate Prevention Research. Int. J. Environ. Res. Public Health 2020, 17, 1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, J.M.; Montgomery, D. Follow-up after breast cancer. BMJ 2008, 336, 107–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soriano-Maldonado, A.; Carrera-Ruiz, Á.; Díez-Fernández, D.M.; Esteban-Simón, A.; Maldonado-Quesada, M.; Moreno-Poza, N.; del Mar García-Martínez, M.; Alcaraz-García, C.; Vázquez-Sousa, R.; Moreno-Martos, H.; et al. Effects of a 12-week resistance and aerobic exercise program on muscular strength and quality of life in breast cancer survivors: Study protocol for the EFICAN randomized controlled trial. Medicine 2019, 98, e17625. [Google Scholar] [CrossRef] [Green Version]
- Romero-Barquero, C. Actividad física en el tiempo libre previene enfermedades cardiacas/cardiovasculares: Una revisión sistemática. Rev. Iberoam. Cienc. Act. Física y Deporte 2020, 9, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Vázquez Rigueira, P.; Pedrero Chamizo, R.; Aparicio Ugarriza, R.; Santiago Dorrego, C.; Calonge, S.; Gómez, F.; Le Ble, G.P.; Manjón, R.D.; Meléndez, A.; Barrios, L.; et al. Efectos de un programa de ejercicio intradiálisis en pacientes con enfermedad renal crónica. Rev. Iberoam. Cienc. Act. Física y Deporte 2019, 8, 52–66. [Google Scholar] [CrossRef]
- Moros, M.T.; Ruidiaz, M.; Caballero, A.; Serrano, E.; Martínez, V.; Tres, A. Effects of an exercise training program on the quality of life of women with breast cancer on chemotherapy. Rev. Médica de Chile 2010, 138, 715–722. [Google Scholar] [CrossRef] [Green Version]
- Mascherini, G.; Tosi, B.; Giannelli, C.; Grifoni, E.; Degl’innocenti, S.; Galanti, G. Breast cancer: Effectiveness of a one-year unsupervised exercise program. J. Sports Med. Phys. Fit. 2019, 59, 283–289. [Google Scholar] [CrossRef]
- Pennington, K.P.; McTiernan, A. The role of physical activity in breast and gynecologic cancer survivorship. Gynecol. Oncol. 2018, 149, 198–204. [Google Scholar] [CrossRef]
- Aranda-Malavés, R.; Tudela-Desantes, A.; González-Ródenas, J. Academic and athletic performance in young athletes from the Sports Technification Centre in Cheste. Educ. Sport Health Phys. Act. 2019, 3, 86–94. [Google Scholar]
- Lope, V.; Martín, M.; Castelló, A.; Casla, S.; Ruiz, A.; Baena-Cañada, J.M.; Casas, A.; Calvo, L.; Bermejo, B.; Muñoz, M.; et al. Physical activity and breast cancer risk by pathological subtype. Gynecol. Oncol. 2017, 144, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Boyne, D.J.; O’Sullivan, D.E.; Olij, B.F.; King, W.D.; Friedenreich, C.M.; Brenner, D.R. Physical Activity, Global DNA Methylation, and Breast Cancer Risk: A Systematic Literature Review and Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1320–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, T.; van Mackelenbergh, M.; Wesch, D.; Mundhenke, C. Physical activity influences the immune system of breast cancer patients. J. Cancer Res. Ther. 2017, 13, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Spei, M.E.; Samoli, E.; Bravi, F.; La Vecchia, C.; Bamia, C.; Benetou, V. Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast 2019, 44, 144–152. [Google Scholar] [CrossRef]
- Lee, J. A meta-analysis of the association between physical activity and breast cancer mortality. Cancer Nurs. 2019, 42, 271–285. [Google Scholar] [CrossRef]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database Syst. Rev. 2018, 1, CD011292. [Google Scholar] [CrossRef] [Green Version]
- Patsou, E.D.; Alexias, G.D.; Anagnostopoulos, F.G.; Karamouzis, M.V. Effects of physical activity on depressive symptoms during breast cancer survivorship: A meta-analysis of randomised control trials. ESMO Open 2017, 2, e000271. [Google Scholar] [CrossRef] [Green Version]
- Singh, B.; Spence, R.R.; Steele, M.L.; Sandler, C.X.; Peake, J.M.; Hayes, S.C. A systematic review and meta-analysis of the safety, feasibility, and effect of exercise in women with stage II+ breast cancer. Arch. Phys. Med. Rehabil. 2018, 99, 2621–2636. [Google Scholar] [CrossRef] [Green Version]
- Hong, F.; Ye, W.; Kuo, C.H.; Zhang, Y.; Qian, Y.; Korivi, M. Exercise intervention improves clinical outcomes, but the “time of session” is crucial for better quality of life in breast cancer survivors: A systematic review and meta-analysis. Cancers 2019, 11, 706. [Google Scholar] [CrossRef] [Green Version]
- Panchik, D.; Masco, S.; Zinnikas, P.; Hillriegel, B.; Lauder, T.; Suttmann, E.; Chinchilli, V.; Mc Beth, M.; Hermann, W. Effect of exercise on breast cancer-related lymphedema: What the lymphatic surgeon needs to know. J. Reconstr. Microsurg. 2019, 35, 37–45. [Google Scholar] [CrossRef]
- Quintana López, V.A.; Díaz López, K.J.; Caire Juvera, G. Interventions to improve healthy lifestyles and their effects on psychological variables among breast cancer survivors: A systematic review. Nutr. Hosp. 2018, 35, 979–992. [Google Scholar] [CrossRef] [PubMed]
- Soares Falcetta, F.; de Araújo Vianna Trésel, H.; de Almeida, F.K.; Rangel Ribeiro Falcetta, M.; Falavigna, M.; Dornelles Rosa, D. Effects of physical exercise after treatment of early breast cancer: Systematic review and meta-analysis. Breast Cancer Res. Treat. 2018, 170, 455–476. [Google Scholar] [CrossRef] [PubMed]
- Hardefeldt, P.J.; Penninkilampi, R.; Edirimanne, S.; Eslick, G.D. Physical activity and weight loss reduce the risk of breast cancer: A meta-analysis of 139 prospective and retrospective studies. Clin. Breast Cancer 2018, 18, e601–e612. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Carral, A.; Molina, A.J.; de Pedro, Á.; Ayón, C. Pilates for women with breast cancer: A systematic review and meta-analysis. Complement. Ther. Med. 2018, 41, 130–140. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Q.; Zhang, Y.; Xie, Q.; Tan, X. Physical activity and risk of breast cancer: A meta-analysis of 38 cohort studies in 45 study reports. Value Heal. 2019, 22, 104–128. [Google Scholar] [CrossRef] [Green Version]
- Grimley, C.E.; Kato, P.M.; Grunfeld, E.A. Health and health belief factors associated with screening and help-seeking behaviours for breast cancer: A systematic review and meta-analysis of the european evidence. Br. J. Heal. Psychol. 2020, 25, 107–128. [Google Scholar] [CrossRef]
- Abdin, S.; Lavallée, J.F.; Faulkner, J.; Husted, M. A systematic review of the effectiveness of physical activity interventions in adults with breast cancer by physical activity type and mode of participation. Psycho-Oncology 2019, 28, 1381–1393. [Google Scholar] [CrossRef]
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous update project—Systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control 2019, 30, 1183–1200. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise guidelines for cancer survivors: Consensus statement from international multidisciplinary roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Di Blasio, A.; Morano, T.; Cianchetti, E.; Gallina, S.; Bucci, I.; Di Santo, S.; Tinari, C.; Di Donato, F.; Izzicupo, P.; Di Baldassarre, A.; et al. Psychophysical health status of breast cancer survivors and effects of 12 weeks of aerobic training. Complement. Ther. Clin. Pract. 2017, 27, 19–26. [Google Scholar] [CrossRef]
- Keilani, M.; Hasenoehrl, T.; Neubauer, M.; Crevenna, R. Resistance exercise and secondary lymphedema in breast cancer survivors—A systematic review. Support. Care Cancer 2016, 24, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Sweeney, F.C.; Stewart, C.; A Buchanan, T.; Spicer, D.; Tripathy, D.; et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: A randomized controlled trial. Breast Cancer Res. 2018, 20, 124. [Google Scholar] [CrossRef]
- Thomas, G.A.; Cartmel, B.; Harrigan, M.; Fiellin, M.; Capozza, S.; Zhou, Y.; Ercolano, E.; Gross, C.P.; Hershman, D.; Ligibel, J.; et al. The effect of exercise on body composition and bone mineral density in breast cancer survivors taking aromatase inhibitors. Obesity 2017, 25, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Baumann, F.T.; Reike, A.; Reimer, V.; Schumann, M.; Hallek, M.; Taaffe, D.R.; Newton, R.U.; Galvao, D.A. Effects of physical exercise on breast cancer-related secondary lymphedema: A systematic review. Breast Cancer Res. Treat. 2018, 170, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fong, A.J.; Saxton, H.R.; Kauffeldt, K.D.; Sabiston, C.M.; Tomasone, J.R. “We’re all in the same boat together”: Exploring quality participation strategies in dragon boat teams for breast cancer survivors. Disabil. Rehabil. 2020, 3, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Giganti, M.G.; Tresoldi, I.; Sorge, R.; Melchiorri, G.; Triossi, T.; Masuelli, L.; Lido, P.; Albonici, L.; Foti, C.; Modesti, A.; et al. Physical exercise modulates the level of serum MMP-2 and MMP-9 in patients with breast cancer. Oncol. Lett. 2016, 12, 2119–2126. [Google Scholar] [CrossRef] [Green Version]
- Melchiorri, G.; Viero, V.; Triossi, T.; Sorge, R.; Tancredi, V.; Cafaro, D.; Andretis, C.; Vulpialni, M.C.; Saraceni, V.M. New approach to evaluate late arm impairment and effects of dragon boat activity in breast cancer survivors. Medicine 2017, 96, e8400. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, T.L.; Yakiwchuk, C.V.; Griffin, K.L.; Gray, R.E.; Fitch, M.I. Survivor dragon boating: A vehicle to reclaim and enhance life after treatment for breast cancer. Health Care Women Int. 2007, 28, 122–140. [Google Scholar] [CrossRef] [PubMed]
- McDonough, M.H.; Patterson, M.C.; Weisenbach, B.B.; Ullrich-French, S.; Sabiston, C.M. The difference is more than floating: Factors affecting breast cancer survivors´ decisions to join and maintain participation in dragon boat teams and support groups. Disabil. Rehabil. 2019, 41, 1788–1796. [Google Scholar] [CrossRef]
- DAS, A.; Mandal, M.; Syamal, A.K.; Majumdar, P. Monitoring changes of cardio-respiratory parameters during 2000 m rowing performance. Int. J. Exerc. Sci. 2019, 12, 483–490. [Google Scholar]
- Yoshiga, C.C.; Higuchi, M. Rowing performance of female and male rowers. Scand. J. Med. Sci. Sports 2003, 13, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Aramendi, J.M. Remo olímpico y remo tradicional: Aspectos biomecánicos, fisiológicos y nutricionales. Arch. Med. Deporte 2014, 159, 51–59. [Google Scholar]
- Harris, S.R. “We’re all in the same boat”: A review of the benefits of dragon boat racing for women living with breast cancer. Evid. Based Complement. Altern. Med. 2012, 2012, 167651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unruh, A.M.; Elvin, N. In the eye of the dragon: Women’s experience of breast cancer and the occupation of dragon boat racing. Can. J. Occup. Ther. 2004, 71, 138–149. [Google Scholar] [CrossRef]
- Sabiston, C.M.; McDonough, M.H.; Crocker, P.R. Psychosocial experiences of breast cancer survivors involved in a dragon boat program: Exploring links to positive psychological growth. J. Sport Exerc. Psychol. 2007, 29, 419–438. [Google Scholar] [CrossRef]
- Fernández-García, J.C.; Gálvez-Fernández, I.; Gavala-González, J. Estudio longitudinal sobre la pérdida de peso en mujeres jóvenes. J. Sport Health Res. 2019, 11 (Suppl. 1), 105–114. [Google Scholar]
- Harriss, D.; Macsween, A.; Atkinson, G. Standards for Ethics in Sport and Exercise Science Research: 2018 Update. Int. J. Sports Med. 2017, 38, 1126–1131. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association Declaration of Helsinki. JAMA 2013, 310, 2191. [CrossRef] [Green Version]
- Lemmink, K.A.; Kemper, H.C.; de Greef, M.H.; Rispens, P.; Stevens, M. The validity of the sit-and-reach test and the modified sit-and-reach test in middle-aged to older men and women. Res. Q. Exerc. Sport 2003, 74, 331–336. [Google Scholar] [CrossRef]
- Jakobsen, L.H.; Rask, I.K.; Kondrup, J. Validation of handgrip strength and endurance as a measure of physical function and quality of life in healthy subjects and patients. Nutrition 2010, 26, 542–550. [Google Scholar] [CrossRef]
- Sayers, S.P.; Harackiewicz, D.V.; Harman, E.A.; Frykman, P.N.; Rosenstein, M.T. Cross-validation of three jump power equations. Med. Sci. Sports Exerc. 1999, 31, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Haynes, T.; Bishop, C.; Antrobus, M.; Brazier, J. The validity and reliability of the My Jump 2 app for measuring the reactive strength index and drop jump performance. J. Sports Med. Phys. Fit. 2019, 59, 253–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cote, C.G.; Casanova, C.; Marín, J.M.; Lopez, M.V.; Pinto-Plata, V.; de Oca, M.M.; Dordetlly, L.J.; Nekach, H.; Celli, B.R. Validation and comparison of reference equations for the 6-min walk distance test. Eur. Respir. J. 2008, 31, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontol. 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Börg, G. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 337–381. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Years from Diagnosis | Breast (%) | Stage (%) | Surgery (%) | |||
|---|---|---|---|---|---|---|---|
| 53.70 ± 7.88 | 6.57 ± 5.02 | Right | 26.09 | I | 4.35 | Preservation | 53.52 |
| II | 30.43 | Total Mastectomy | 39.13 | ||||
| Left | 73.91 | III | 52.17 | ||||
| IV | 8.7 | Double Mastectomy | 4.35 | ||||
| Stage | Content |
|---|---|
| 1 | Initial phase with mobility exercises, proprioceptive exercises and postural control exercises. Main phase with rowing training. Final phase with stretching. Börg scale 5–6. |
| 2 | Initial phase with mobility exercises, proprioceptive exercises and postural control exercises. Main phase with rowing training. Final phase with stretching. Börg scale 6–7. |
| 3 | Initial phase with mobility exercises, proprioceptive exercises and postural control exercises. Main phase with rowing training. Final phase with stretching. Börg scale 7–8. |
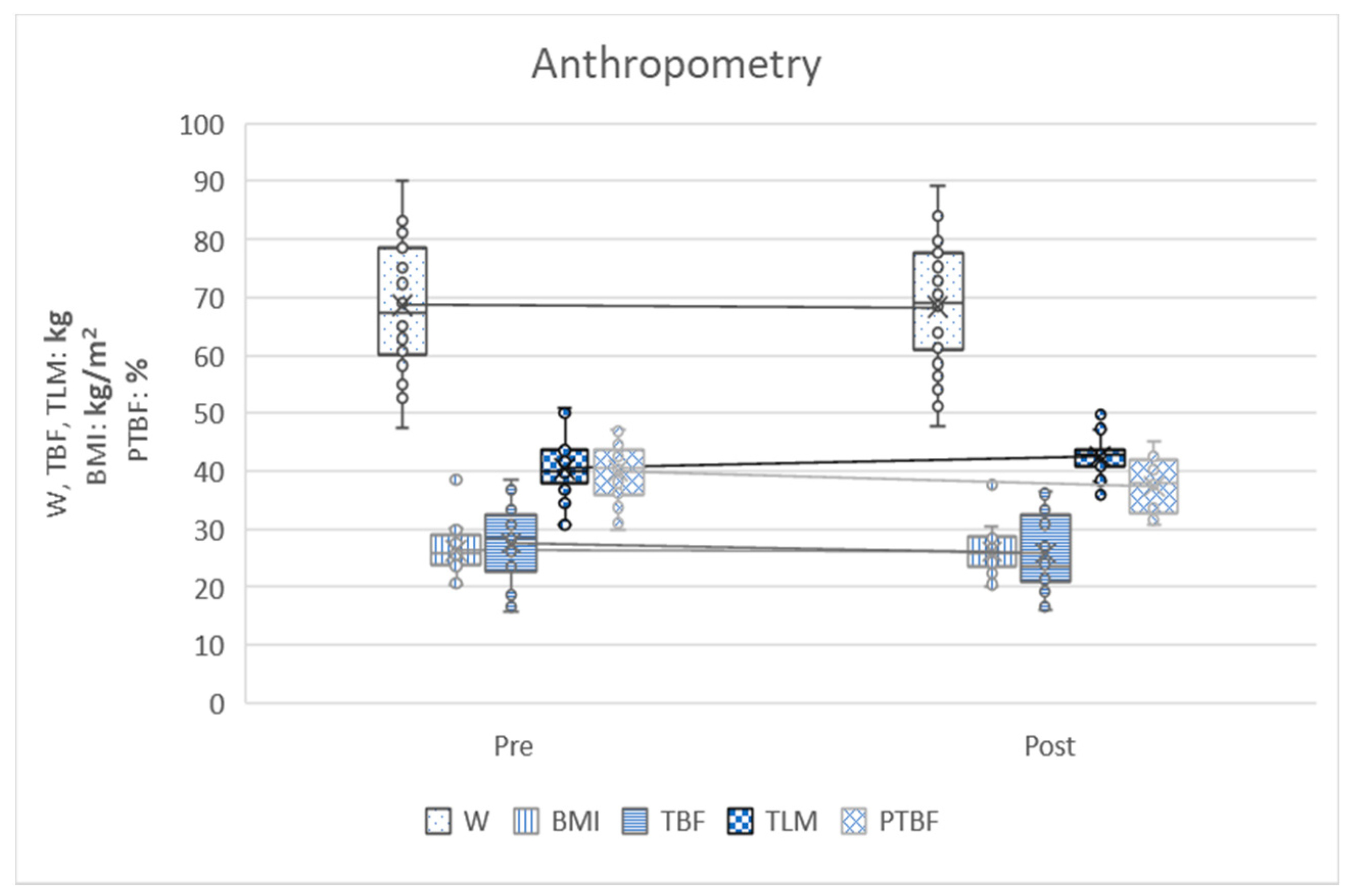
| Variables | Pretest | Post-test | Diff Post-Pre | t-Student | Effect Size | p |
|---|---|---|---|---|---|---|
| Weight (kg) | 68.67 ± 10.98 | 68.29 ± 10.79 | −0.37 ± 2.58 | −0.798 | 0.14 | 0.431 |
| BMI (kg/m2) | 26.34 ± 3.78 | 26.19 ± 3.67 | −0.14 ± 1.02 | −0.786 | 0.14 | 0.438 |
| Total body fat (kg) | 27.62 ± 6.79 | 25.85 ± 6.29 | −1.77 ± 7.60 | −1.28 | 0.23 | 0.211 |
| Total lean mass (kg) | 40.43 ± 4.61 | 42.61 ± 3.45 | 2.18 ± 4.81 | 2.486 | 0.45 | 0.019 * |
| Percentage of total body fat (%) | 40.07 ± 4.84 | 37.44 ± 4.88 | −2.63 ± 5.43 | −2.657 | 0.48 | 0.013 * |
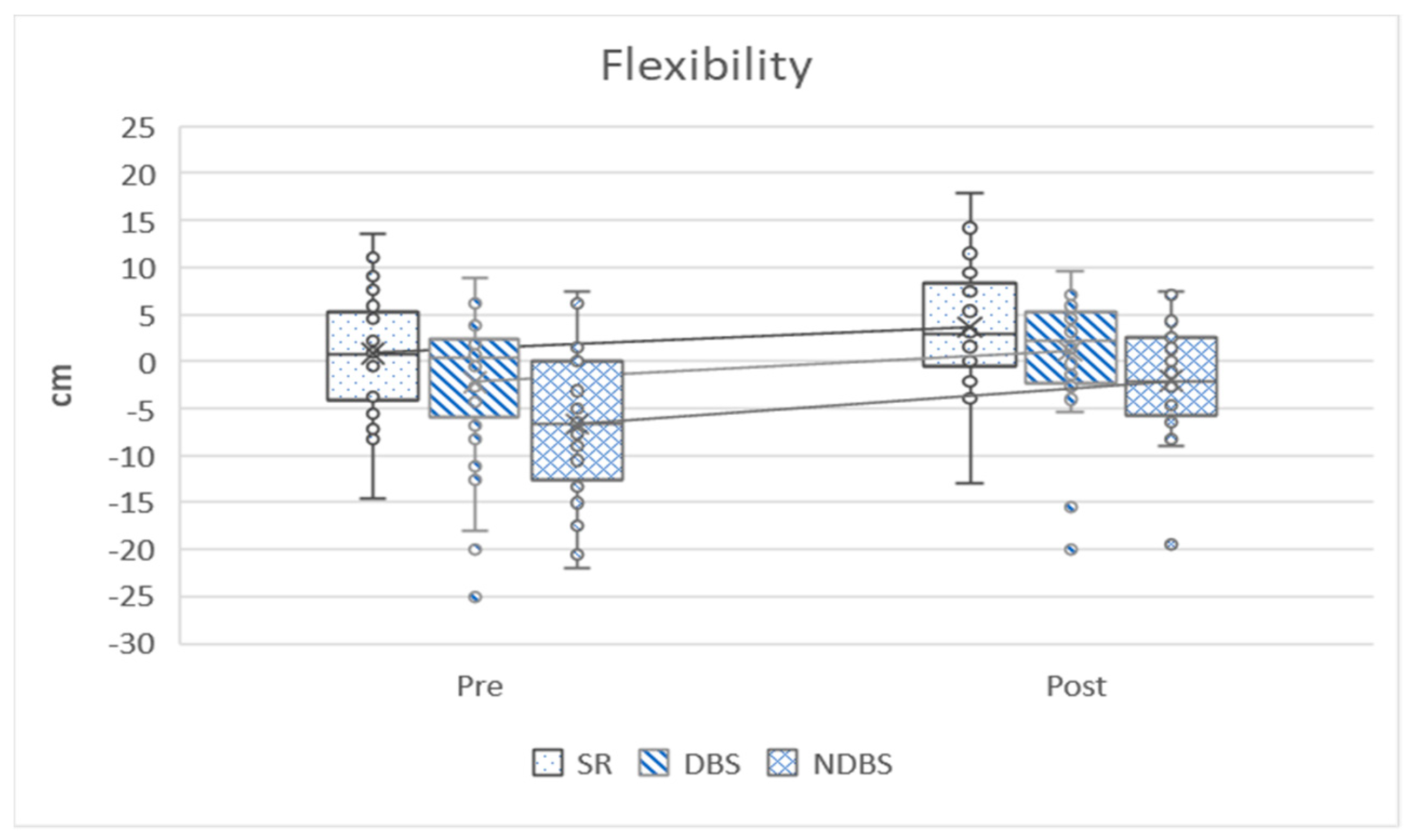
| Sit and reach test (cm) | 0.87 ± 6.61 | 3.69 ± 6.57 | 2.82 ± 1.87 | 8.242 | 1.51 | 0.000 ** |
| Dominant back scratch test (cm) | −2.19 ± 8.22 | 1.10 ± 6.54 | 3.29 ± 3.15 | 5.726 | 1.04 | 0.000 ** |
| Non-dominant back scratch test (cm) | −6.64 ± 7.47 | −2.05 ± 5.72 | 4.59 ± 3.90 | 6.44 | 1.18 | 0.000 ** |
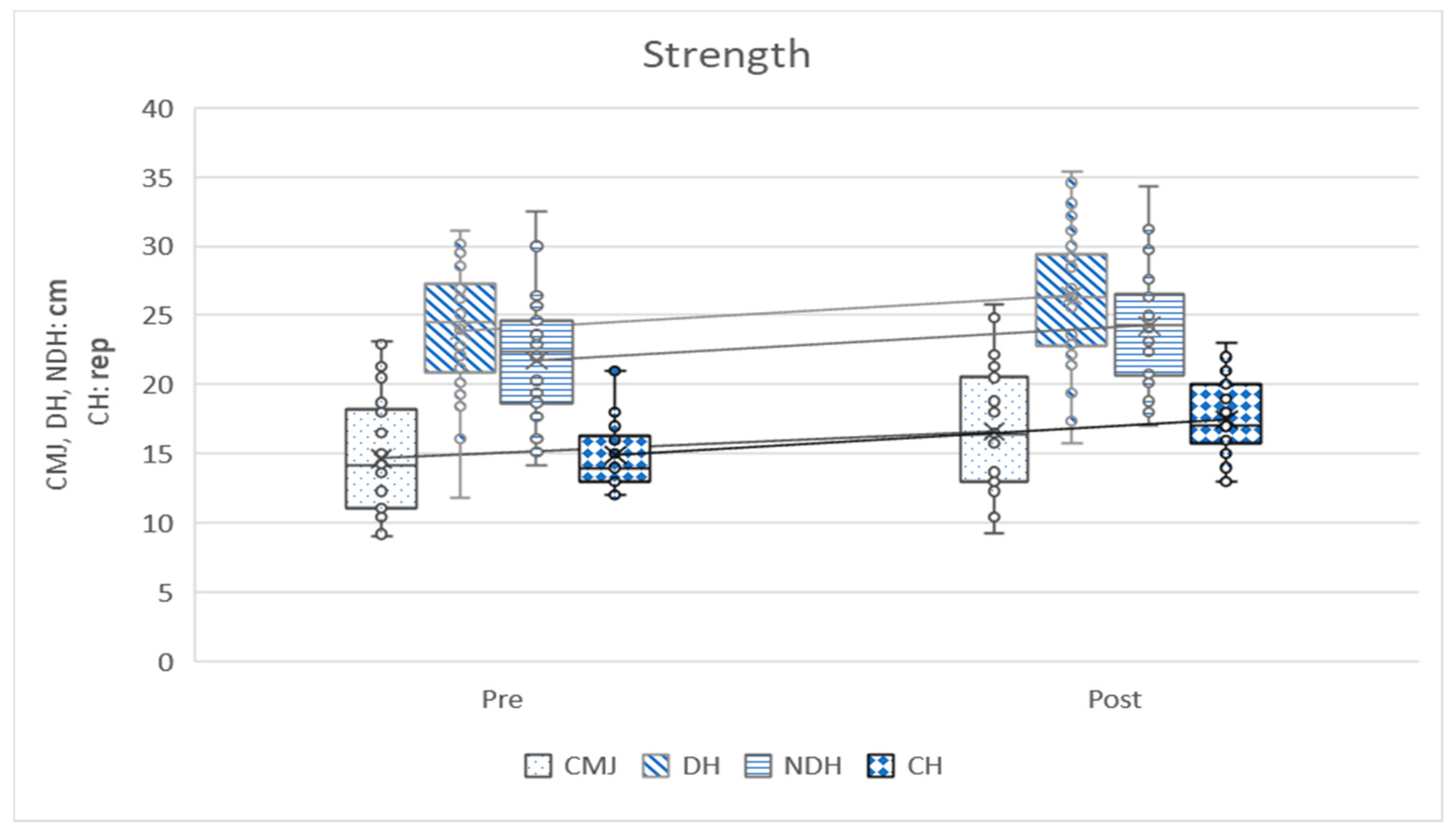
| Counter movement jump test (cm) | 14.67 ± 4.30 | 16.58 ± 4.28 | 1.91 ± 1.71 | 6.128 | 1.12 | 0.000 ** |
| Dominant hand grip test (kgf) | 23.89 ± 4.56 | 26.44 ± 5.00 | 2.54 ± 1.56 | 8.933 | 1.63 | 0.000 ** |
| Non-dominant hand grip test (kgf) | 21.73 ± 4.37 | 24.26 ± 4.06 | 2.53 ± 1.91 | 7.229 | 1.32 | 0.000 ** |
| Chair stand test (rep) | 14.90 ± 2.41 | 17.46 ± 2.75 | 2.56 ± 1.71 | 8.194 | 1.50 | 0.000 ** |
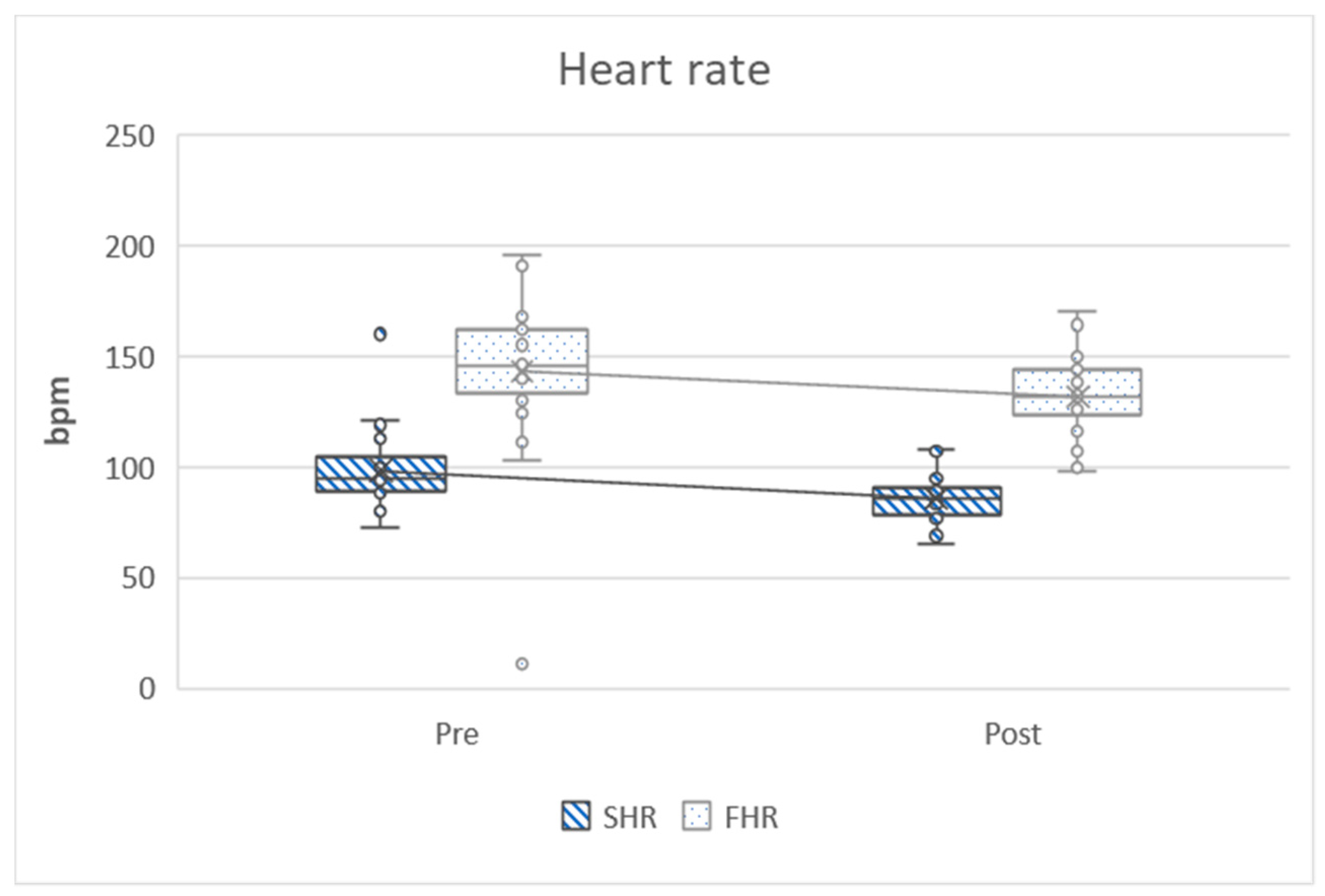
| Starting heart rate at six-minute walking test (bpm) | 98.43 ± 16.72 | 85.80 ± 9.79 | −12.63 ± 14.68 | −4.712 | 0.86 | 0.000 ** |
| Final heart rate at six-minute walking test (bpm) | 143.26 ± 32.64 | 131.80 ± 18.62 | −11.46 ± 28.39 | −2.212 | 0.40 | 0.000 ** |
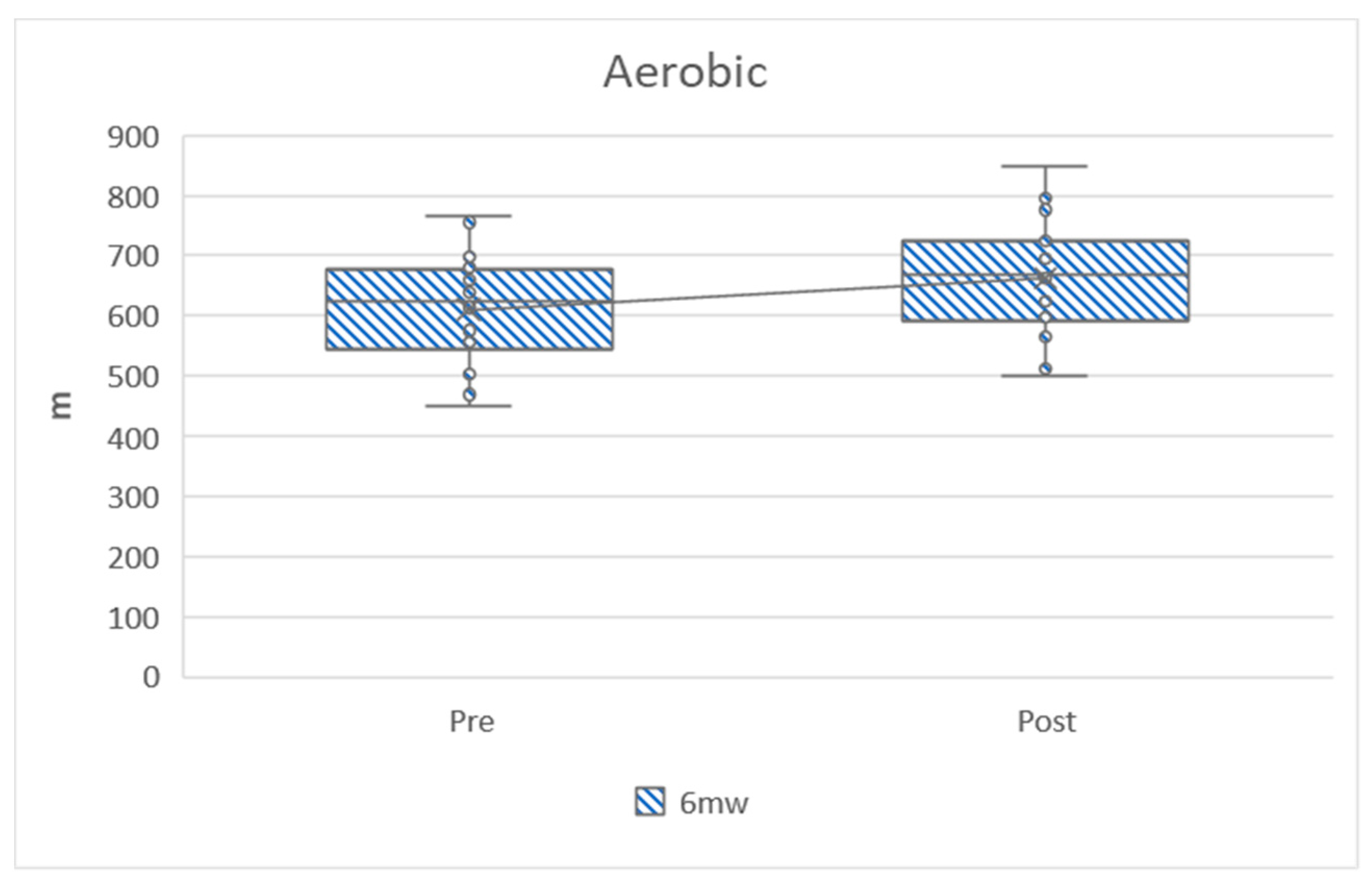
| Distance in six-minute walking test (m) | 611.23 ± 87.01 | 662.80 ± 85.82 | 51.56 ± 48.26 | 5.852 | 1.07 | 0.000 ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavala-González, J.; Gálvez-Fernández, I.; Mercadé-Melé, P.; Fernández-García, J.C. Rowing Training in Breast Cancer Survivors: A Longitudinal Study of Physical Fitness. Int. J. Environ. Res. Public Health 2020, 17, 4938. https://doi.org/10.3390/ijerph17144938
Gavala-González J, Gálvez-Fernández I, Mercadé-Melé P, Fernández-García JC. Rowing Training in Breast Cancer Survivors: A Longitudinal Study of Physical Fitness. International Journal of Environmental Research and Public Health. 2020; 17(14):4938. https://doi.org/10.3390/ijerph17144938
Chicago/Turabian StyleGavala-González, Juan, Ismael Gálvez-Fernández, Pere Mercadé-Melé, and José Carlos Fernández-García. 2020. "Rowing Training in Breast Cancer Survivors: A Longitudinal Study of Physical Fitness" International Journal of Environmental Research and Public Health 17, no. 14: 4938. https://doi.org/10.3390/ijerph17144938
APA StyleGavala-González, J., Gálvez-Fernández, I., Mercadé-Melé, P., & Fernández-García, J. C. (2020). Rowing Training in Breast Cancer Survivors: A Longitudinal Study of Physical Fitness. International Journal of Environmental Research and Public Health, 17(14), 4938. https://doi.org/10.3390/ijerph17144938