Study of Acute and Sub-Acute Effects of Auditory Training on the Central Auditory Processing in Older Adults with Hearing Loss—A Pilot Study




Abstract
:1. Introduction
2. Methods
2.1. Design, Population and Procedure
2.2. Statistics
2.3. Ethics
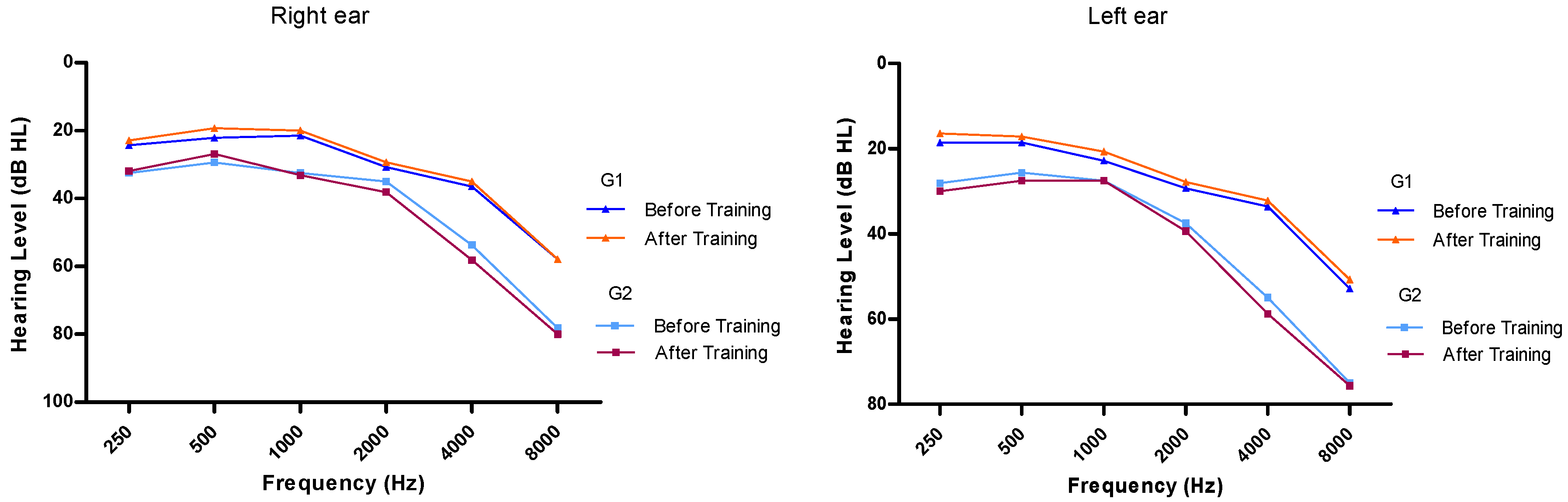
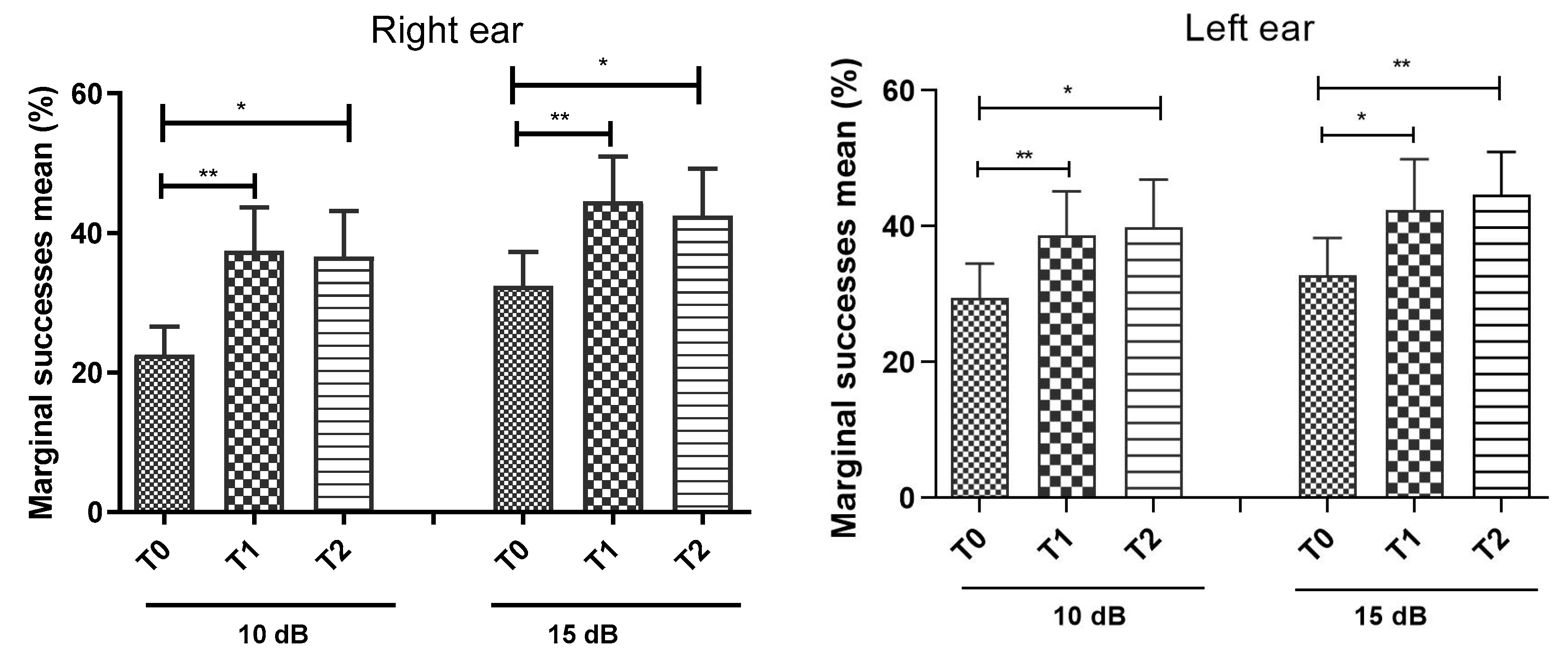
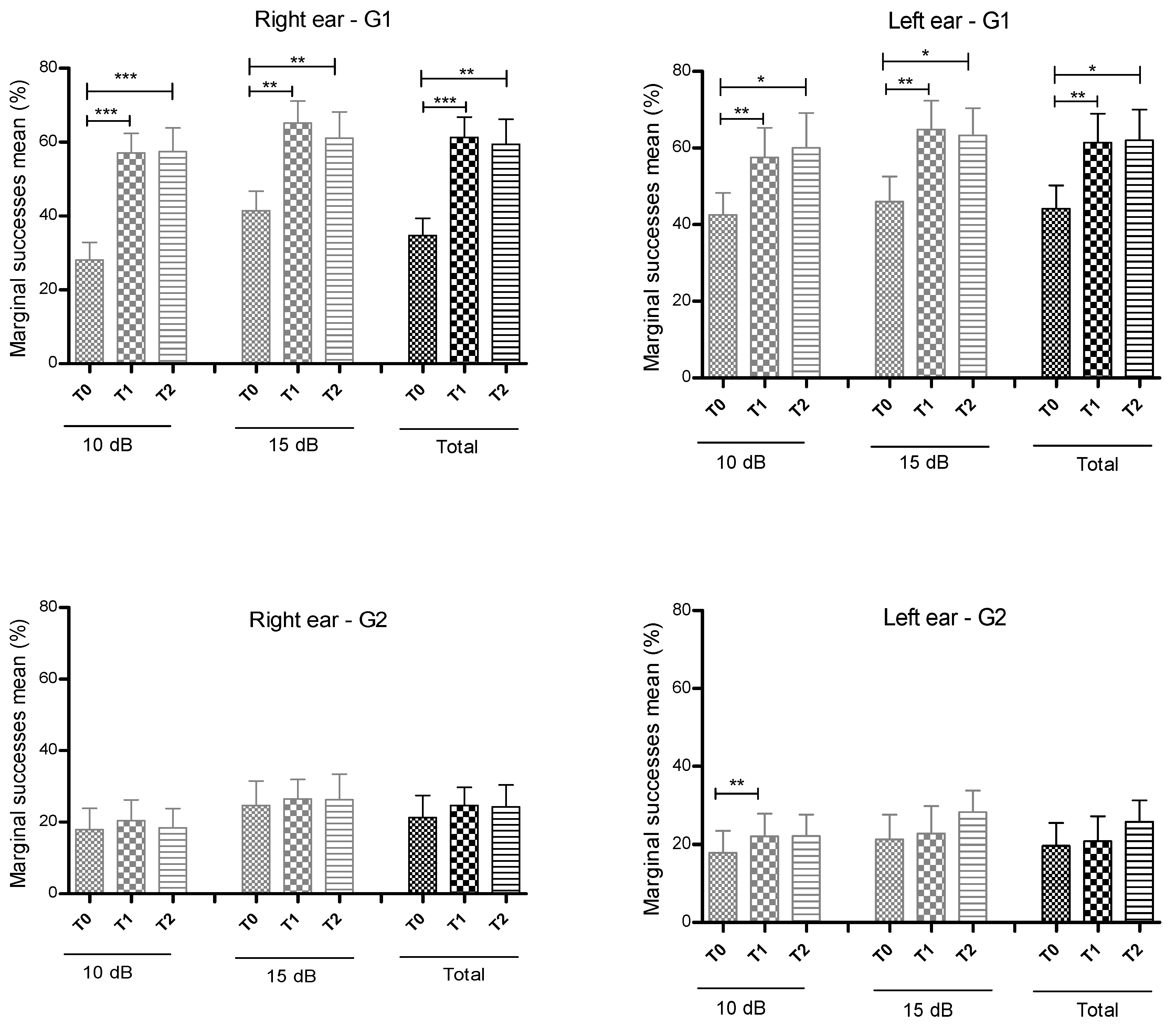
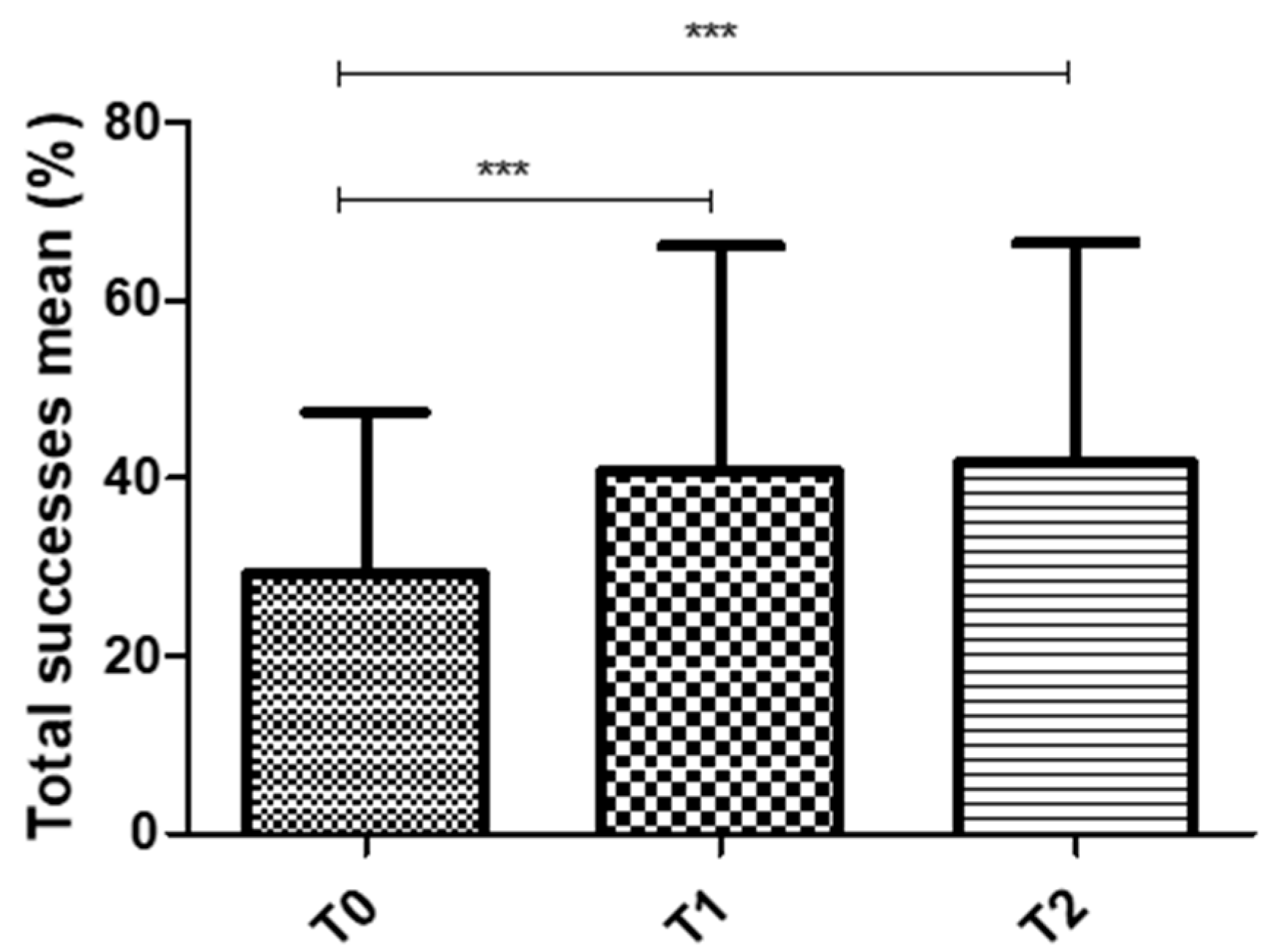
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| dB | Decibel |
| HL | Hearing Level |
| CAP | Central Auditory Processing |
| APD | Auditory Processing Disorder |
| MTHL | Medium Tonal Hearing Loss |
| ACNS | Auditory Central Nervous System |
| SNR | Signal/Noise Ratio |
| SPSS | Statistical Product and Service Solutions |
| MOTML | Motor latency |
| SWMBE | mean between-search errors |
| SWMTE | mean total errors |
| SWMMS | mean searching strategy |
| PALFAMS | mean memory score |
| PALTEA | total adjusted errors |
| PALNPR | mean level achieved |
References
- Nunes, C.L. Importância da audição ed. In Processamento Auditivo—Conhecer, Avaliar e Intervir; Papa-Letras: Lisboa, Portugal, 2015; pp. 11–15. [Google Scholar]
- Pujol, R.; Trigueiros-Cunha, N. Viagem ao Mundo da Audição; Bial: Porto, Portugal, 2016. [Google Scholar]
- Nunes, C.L. Processamento Auditivo Central—Definição e Caracterização ed. In Processamento Auditivo—Conhecer, Avaliar e Intervir; Papa-Letras: Lisboa, Portugal, 2015; pp. 17–19. [Google Scholar]
- Musiek, F.; Baran, J. The Auditory System: Anatomy, Physiology and Clinical Correlates; Pearson: Boston, MA, USA, 2007. [Google Scholar]
- Keith, R.W. Diagnosing Central Auditory Processing Disorders in Children ed. Audiology Diagnosis; Thieme: New York, NY, USA, 2000; pp. 337–355. [Google Scholar]
- Sweetow, R.W.; Sabes, J.H. Auditory training and challenges associated with participation and Compliance. J. Am. Acad. Audiol. 2010, 21, 586–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiffin, S.; Gordon-Hickey, S. The influence of speech rate on acceptable noise levels. J. Am. Acad. Audiol. 2018, 29, 596–608. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.M.; Fernandes, C.; Alves, A.R.; Prata, C.; Rocha, C.; Martins, J. A Influência do Treino Auditivo na Comunicação do Idoso ed: Abordagem Geriátrica Ampla na Promoção de um Envelhecimento Ativo e Saudável—Componentes do Modelo de Intervenção; Edições—IPC| Inovar Para Crescer: Coimbra, Protugal, 2019; pp. 75–85. [Google Scholar]
- American Academy of Audiology (AAA). Diagnosis, Treatment and Management of Children and Adults with Central Auditory Processing Disorder. Clinical Practice Guidelines. Available online: www.psha.org/pdfs/toolbox/CAPD-Guidelines_8-2010.pdf (accessed on 25 March 2019).
- American Speech-Language-Association (ASHA). Central Auditory Processing Disorders [Technical Report]. Available online: www.asha.org/policity/tr2005-00043.htm (accessed on 25 March 2019).
- Bellis, T. Assessment and Management of Central Auditory Processing Disorders in the Educational Setting: From Science to Practice; Singular Publishing: San Diego, CA, USA, 1996. [Google Scholar]
- Bellis, T.; Beck, B. Central Auditory Processing in Clinical Practice. Available online: http://www.audiologyonline.com/articles/central-auditory-processing-in-clinical-1281 (accessed on 13 May 2015).
- Rivabem, K. Linguagem Escrita e Distúrbios do Processamento Auditivo Central: Uma Relação de Casualidade Contraditória. Master’s Thesis, Universidade Tuiuti do Panamá para a obtenção do título de Mestre em Distúrbios da Comunicação, Panama City, PA, USA, 2006. [Google Scholar]
- Martins, J. Avaliação do Processamento Auditivo Central e Dificuldades de Aprendizagem. Ph.D. Thesis, Universidade de Lisboa para a obtenção do grau de Doutoramento, Lisboa, Protugal, 2017. [Google Scholar]
- Pereira, L.D.; Schochat, E. Testes Auditivos Comportamentais para Avaliação do Processamento Auditivo Central; Pró-Fono: São Paulo, Brazil, 2011. [Google Scholar]
- Martins, J.; Alves, M.; Pereira, C.; Teixeira, A. Bateria de Testes de Processamento Auditivo Central—Dados Normativos Para a População Adulta—Dados Preliminares; Poster Apresentado no 60° Congresso Nacional da SPORL: Porto, Portugal, 2013. [Google Scholar]
- Rabelo, C.M.; Rocha-Muniz, C.; Schochat, E. Ongoing maturation in the time-compressed speech test. Clinics 2018, 73, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Baran, J.A.; Musiek, F.E. Behavioral assessment of the central auditory nervous system. In Contemporary Perspectives in Hearing Assessment; Musiek, F.E., Rintelmann, W.F., Eds.; Allyn and Bacon: São Paulo, Brazil, 1999; pp. 377–413. [Google Scholar]
- McArdle, R.; Wilson, R.; Burks, C. Speech recognition in multitalker babble using digits, words, and sentences. J. Am. Acad. Audiol. 2005, 16, 726–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Speech-Language Hearing Association. A Task Force on Central Auditory Processing Consensus Development Central auditory processing: Current status of research and implications for clinical practice. Am. J. Audiol. 1996, 5, 41–54. [Google Scholar] [CrossRef]
- Heeke, P.; Vermiglio, A.J.; Velappan, K.; Fang, X. The relationship between Random Gap Detection and Hearing in Noise Test Performances. J. Am. Audiol. 2018, 29, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Stephens, D.; Zhan, F.; Kennedy, V. Is there an Association between noise exposure and King Kopetzy Syndrome? Noise Health 2003, 5, 55–62. [Google Scholar]
- Tremblay, K.L.; Pinto, A.; Fischer, M.E.; Klein, B.E.; Klein, R.; Levy, S.; Tweed, T.S.; Cruickshanks, K.J. Self-reported hearing difficulties among adults with normal audiograms: The beaver Dam offspring Study. Ear Hear. 2015, 36, e290. [Google Scholar] [CrossRef] [Green Version]
- Hamlyn, K.; Welldon, K.; Clark, B.; van Steenbrugge, W.; Kapadia, S. The effect of increased cognitive demand on auditory processing assessment. J. Am. Acad. Audiol. 2018, 29, 788–801. [Google Scholar] [CrossRef]
- Martin, J.S.; Jerger, J.F. Some effects of aging on central auditory processing. J. Rehabil. Res. Dev. 2005, 42, 25–44. [Google Scholar] [CrossRef]
- Veras, R.; Mattos, L. Audiologia do envelhecimento: Revisão da literatura e perspetivas atuais. Rev. Bras. Otorrinol. 2007, 73, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Ruschel, C.V.; Carvalho, C.R.; Guarinello, A.C. The efficiency of an auditory rehabilitation program in eldery people with presbiacusys and their family. Rev. Soc. Bras. Fonoaudiol. 2007, 12, 95–98. [Google Scholar] [CrossRef] [Green Version]
- Bocca, E.; Caetano, C. Central Hearing Processes ed. Modern Development in Audiology; Academic Press: New York, NY, USA, 1963; pp. 337–370. [Google Scholar]
- Moore, D.R.; Fergunson, M.A.; Edmonson-Jones, A.M.; Ratib, S.; Riley, A. Nature of auditoy processing disorder in children. Pediatrics 2010, 126, e382–e390. [Google Scholar] [CrossRef] [PubMed]
- Musiek, F.; Rintelman, W.F. Avaliação Comportamental do Sistema Nervoso Central ed:. Perspetivas Atuais em Avaliação Auditiva; Manole, Lda: São Paulo, Brazil, 2001; pp. 343–362. [Google Scholar]
- Machado, S.F. Processamento Auditivo—Uma Nova Abordagem; Plexus Editora: São Paulo Brazil, 2003. [Google Scholar]
- Neves, V.T.; Feitosa, M.A. Controversies or complexity in the relationship between temporal auditory processing and aging? Braz. J. Otorhinolaringol. 2003, 69, 242–249. [Google Scholar]
- Cruz, A.C.A.; Andrade, A.N.; Gil, D. A eficácia do treinamento auditivo formal em adultos com distúrbio do processamento auditivo (central). Rev. CEFAC 2013, 15, 1427–1434. [Google Scholar] [CrossRef] [Green Version]
- Nunes, C.L. Treino Auditivo na Perturbação do Processamento Auditivo ed: Processamento Auditivo-Conhecer, Avaliar e Intervir; Lisboa—Papa-Letras: Lisboa, Portugal, 2015; pp. 113–116. [Google Scholar]
- Pereira, L.D. Processamento auditivo. Temas em Desenvolvimento 1993, 12, 7–14. [Google Scholar]
- Schochat, E.; Carvalho, L.Z.; Megale, R.L. Treinamento auditivo: Avaliação da manutenção das habilidades. Pró-fono 2002, 14, 93–98. [Google Scholar]
- Gil, D. Treinamento Auditivo Formal em Adultos com Deficiência Auditiva. Ph.D. Thesis, Universidade Federal de São Paulo, São Paulo, Brazil, 2006. [Google Scholar]
- Robbins, T.; James, M.; Owen, A.; Sahakian, B.J.; Mclnnes, L.; Rabbitt, P. Cambridge Neuropsychological Test Automated Battery (CANTAB): A factor analytic study of a large sample of normal elderly volunteers. Dementia Geriatr. Cogn. Disord. 1994, 5, 266–281. [Google Scholar] [CrossRef]
- Robbins, T.; James, M.; Owen, A.; Sahakian, B.J.; Lawrence, A.D.; McInnes, L.; Rabbitt, P.M. A study of performance on tests from the CANTAB battery sensitive to frontal lobe dysfunction in a large sample of normal volunteers: Implications for theories of executive functioning and cognitive aging. J. Int. Neuropsychol. Soc. 1998, 4, 474–490. [Google Scholar] [CrossRef]
- BIAP Recommendation n° 02/1 Audiometric Classification of Hearing Impairments. [Em linha] Bureau International d’Áudio-Phonologie. 1997. Available online: http://www.biap.org/biapanglais/rec021eng.htm (accessed on 26 November 2019).
- Pichora-Fuller, M.K.; Singh, G. Effects of Age on Auditory and Cognitive Processing: Implications for Hearing Aid Fitting and Audiologic Rehabilitation. Westminst. Publ. Inc. 2006, 10, 29–59. [Google Scholar] [CrossRef]
- Ferguson, M.A.; Henshaw, H. Auditory training can improve working, memory, attention, and communication in adverse conditions for adults with hearing loss. Front. Psychol. 2015, 6, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, S.; White-Schwoch, T.; Choi, H.J.; Kraus, N. Training changes processing of speech clues in older adults with hearing loss. Front. Syst. Neurosci. 2013, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caporali, S.A.; Silva, J.A. Reconhecimento da fala no ruído em jovens e idosos com perda auditiva. Rev. Bras. Otorrinolaringol. 2004, 70, 525–532. [Google Scholar] [CrossRef]
- Morais, A.; Rocha-Muniz, C.; Schochat, E. Efficacy of Auditory Training in Elderly Subjects. Front. Aging Neurosci. 2015, 7, 78. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | G1 (n = 7) | G2 (n = 8) | p-Value |
|---|---|---|---|
| Gender | |||
| Female % (n) Male % (n) | 71.4 (5) 28.6 (2) | 50 (4) 50 (4) | n.s |
| Age. years | 73.6 ± 12.3 | 83.0 ± 7.8 | n.s |
| Cognitive Function | |||
| MOTML | 1168.7 ± 340.7 | 1357.1 ± 380.7 | n.s |
| SWMBE | 22.4 ± 5.1 | 23.9 ± 5.6 | n.s |
| SWMTE | 22.4 ± 5.1 | 24.5 ± 5.8 | n.s |
| SWMS | 10.4 ± 0.8 | 10.3 ± 1.5 | n.s |
| PALFAMS | 3.7 ± 1.8 | 2.8 ± 2.3 | n.s |
| PALTEA | 58.4 ± 7.8 | 59.5 ± 7.9 | n.s |
| PALNPR | 4.0 ± 1.6 | 4.3 ± 1.3 | n.s |
| MTHL 1 | |||
| Right ear. dB | 27.7 ± 10.1 | 37.7 ± 9.0 | 0.04 |
| Left ear. dB | 26.1 ± 9.2 | 36.4 ± 6.7 | 0.021 |
| Speech in noise test 2 | |||
| Right ear | |||
| SNR 10 dB. % | 28.0 ± 12.7 | 17.9 ± 16.8 | n.s |
| SNR 15 dB. % | 41.4 ± 14.0 | 24.6 ± 19.4 | n.s |
| Total. % | 34.7 ± 12.4 | 21.3 ± 17.5 | n.s |
| Left ear | |||
| SNR 10 dB. % | 42.6 ± 15.2 | 17.9 ± 15.7 | 0.029 |
| SNR 15 dB. % | 46.0 ± 17.3 | 21.3 ± 17.8 | 0.029 |
| Total. % | 44.1 ± 16.1 | 19.6 ± 16.4 | 0.021 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matos Silva, C.; Fernandes, C.; Rocha, C.; Pereira, T. Study of Acute and Sub-Acute Effects of Auditory Training on the Central Auditory Processing in Older Adults with Hearing Loss—A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 4944. https://doi.org/10.3390/ijerph17144944
Matos Silva C, Fernandes C, Rocha C, Pereira T. Study of Acute and Sub-Acute Effects of Auditory Training on the Central Auditory Processing in Older Adults with Hearing Loss—A Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(14):4944. https://doi.org/10.3390/ijerph17144944
Chicago/Turabian StyleMatos Silva, Carla, Carolina Fernandes, Clara Rocha, and Telmo Pereira. 2020. "Study of Acute and Sub-Acute Effects of Auditory Training on the Central Auditory Processing in Older Adults with Hearing Loss—A Pilot Study" International Journal of Environmental Research and Public Health 17, no. 14: 4944. https://doi.org/10.3390/ijerph17144944
APA StyleMatos Silva, C., Fernandes, C., Rocha, C., & Pereira, T. (2020). Study of Acute and Sub-Acute Effects of Auditory Training on the Central Auditory Processing in Older Adults with Hearing Loss—A Pilot Study. International Journal of Environmental Research and Public Health, 17(14), 4944. https://doi.org/10.3390/ijerph17144944