The Frontline Nurse’s Experience of Nursing Outlier Patients


Abstract
:1. Introduction
2. Background
2.1. The Competent Nurses
2.2. The “Unavoidable” Occurrence of Outlier Patients
2.3. Nursing With Lower Level of “Duty of Care”
2.4. Nursing With Lower Level of “Standard of Care”
3. Methods
3.1. Research Design
3.2. Criteria for Participant Selection and Recruitment
3.3. Ethics
3.4. Interview Procedure
3.5. Analysis
4. Results
“… management just don’t care that is important to get patient back to their own area specialty … And if they are in a bed, that’s what all it matters. Doesn’t really matter we are all general nurses at the end of the day basically. And if it’s the level of care that you want for your patients in your hospital, that’s fine. But we tend to think these days and age that specialty care is far more important… Because it reduces some hospital length of stay and also increases the patients’ outcome.”(Peter 118–124).
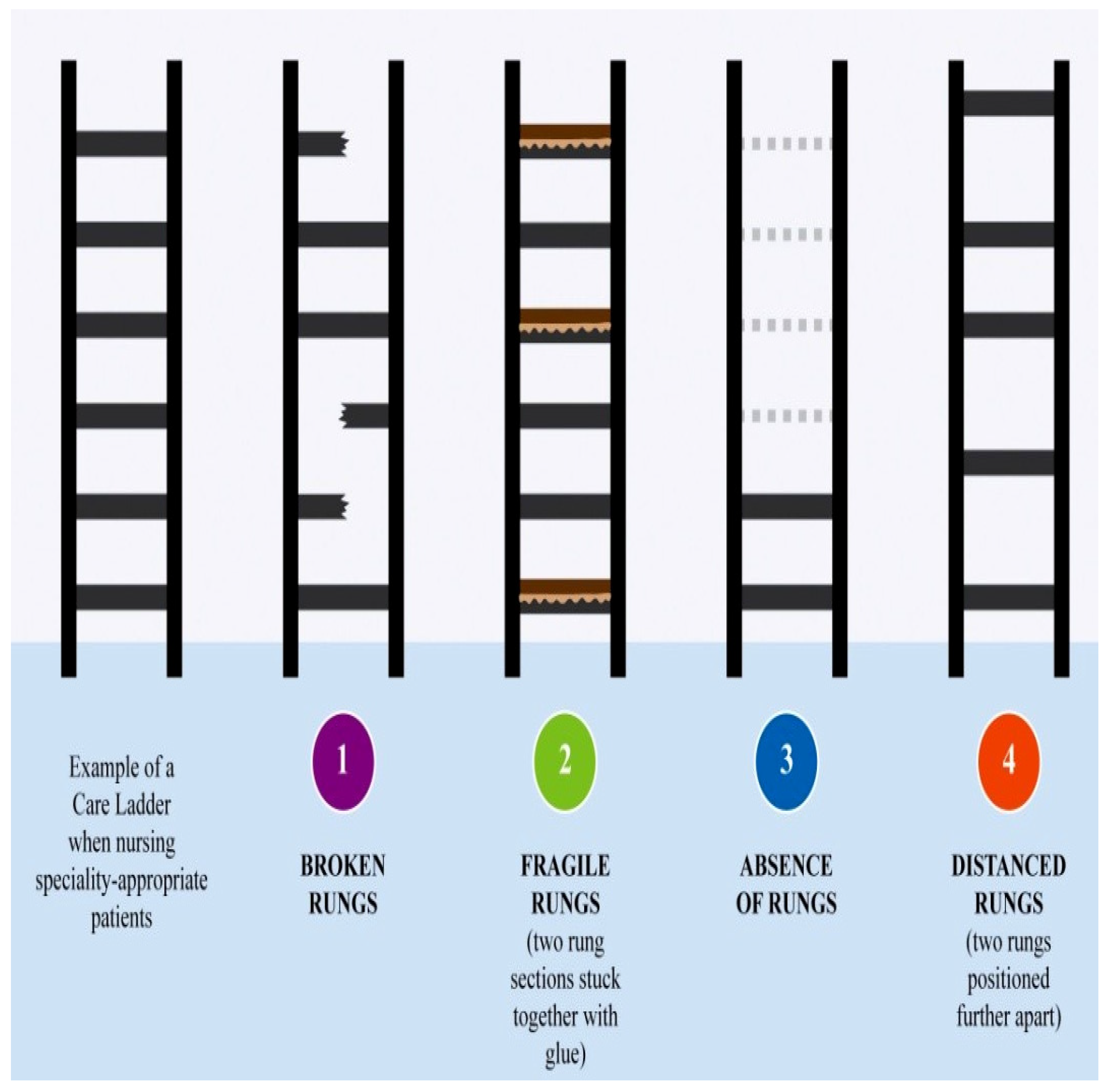
“I hope that basic nursing is carried out everywhere that everyone has the best interest of the patient at heart so that they are getting adequate care … it’s the special skills that nurses required working in specialized care that they (the outlier patients) probably missed out on.”(Ann 61–64).
“It’s frustrating … you feel bad because you are not able to provide good nursing care. You are only able to provide basic nursing care (to outlier patients),”(Madeline 133–134).
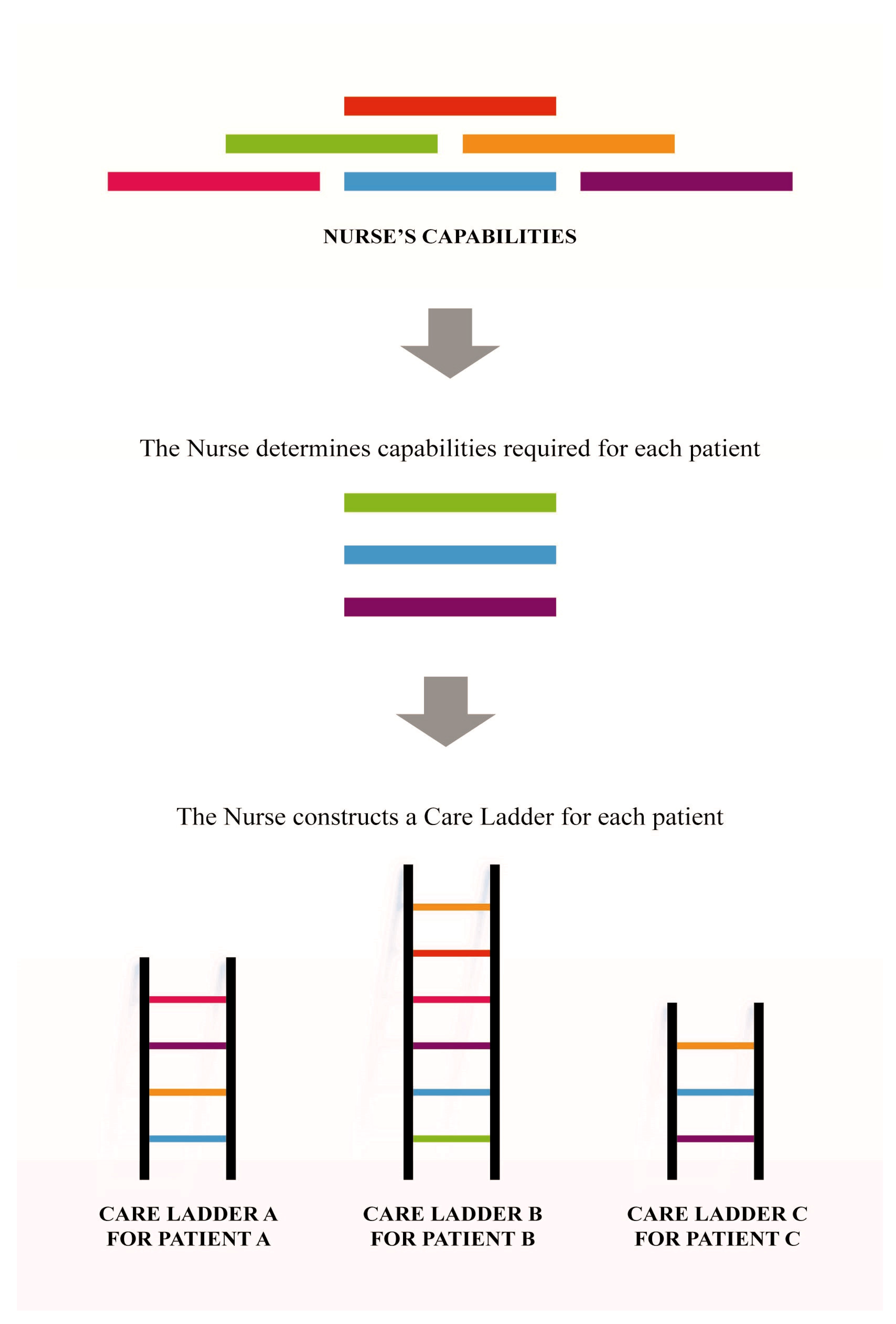
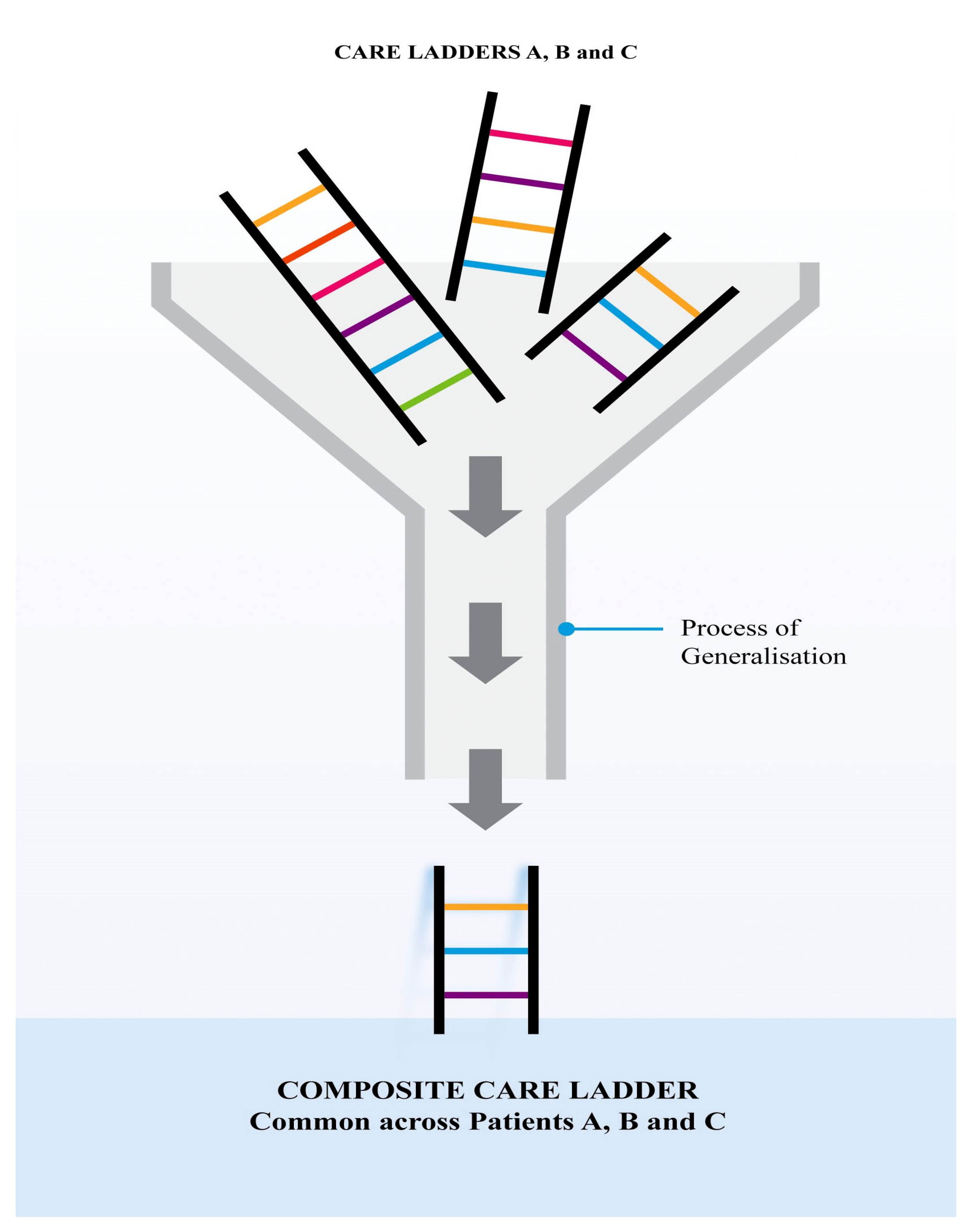
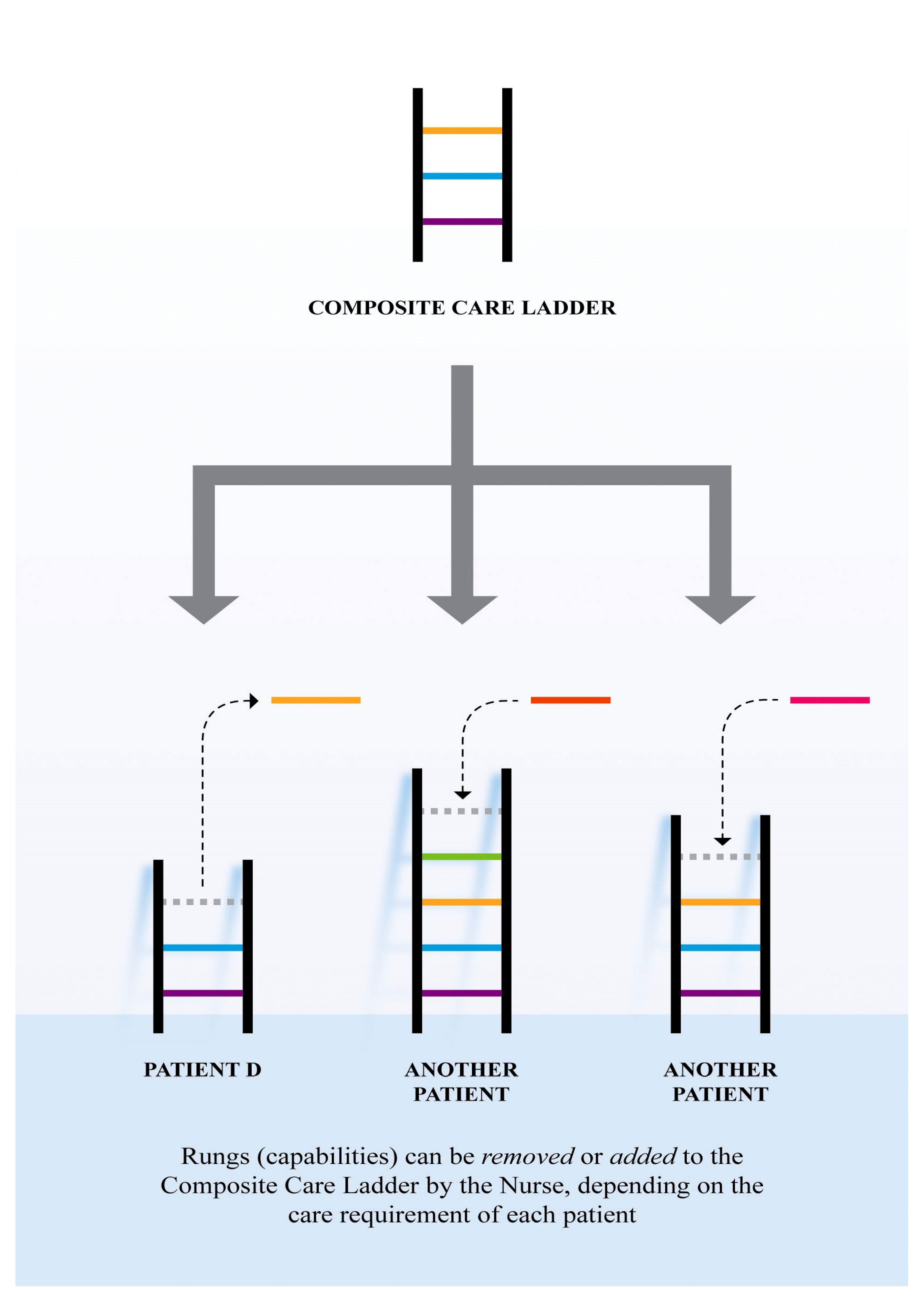
“I would say appropriate is one level up from adequate care. Adequate is just that...you know you give enough … on a ladder … all different levels. You would call basic is the basics… you just do the basics... Keep them alive. Hope that they don’t get any worse. But that is just a minimum. Adequate level is already much better because it encompasses more. You have a much better picture of the whole person. Appropriate care would be really looking at all their needs where it goes to the really high level of nursing care, I would call that first class of nursing care...”(Agnes 200–209).
- (a)
- Synchronizing nursing rhythms;
- (b)
- Practicing with disease and/or condition specific familiarity;
- (c)
- Prioritizing each nursing task;
- (d)
- Predicting care requirements;
- (e)
- Practicing with inter-professional relationality, as they were nursing the outlier patient, as a result/outcome of nursing the outlier patients.
4.1. Becoming Less Capable of Synchronizing Nursing Rhythms
“If that (outlier patient’s specialty) team of doctors used to do their round at 10am (at the team doctor’s specialty ward) because this suits the rest of their day, they will come to see the outliers at two o’clock, for example. Now you are trying to feed the patients. The doctors now want to see the patient or whatever. So, it can affect the nurses’ routine as well. It has to affect the patients...might affect showering, may affect the feeding, may affect the medications, may affect the dressings, it may affect the treatment times because doctors are coming on a different routine to see outliers as they come in as a normal (specialty) ward. So that now the nursing routine, everything to do with patient care (is disrupted) …”(John 44–54).
“… by the time you got to contact them (the clinical nurse educator (CNE) or clinical nurse specialist (CNC) for the outlier patients), there is a delay because you always do that (call the CNE or CNC) once you finish with the routine, like giving medications and up to showers or doing other things ... and then by the time the CNE or CNC comes, they may be in a meeting, so...they cannot come on time ... sometimes they are in the middle of (doing) something too ...”(Rainbow 145–150).
“… (The outlier patient) has specific drains for gastro, for after the operation, but that was not on (our) ward. So that means you have to get that from the other ward, the gastro surgical ward, which is not a big job to get it, but it all added little stressors to getting the job done and looking after the patient.”(Hope 156–159).
“You know all wards … (are in a) very specialized world now ... the departments are completely separate, particularly true for departments of medicine and administration and budget and everything. They wouldn’t necessarily supply equipment from their budget ...”(John 29–33).
“…When it (goes beyond) our quota of equipment (when our ward does not have that particular equipment in stock), it takes longer. Sometimes your mate (nurses in other ward) refuses (to provide) it (for you), so then you go to find another avenue (ward) to get the equipment. And if you are looking for an equipment, (it is) not for fun, it’s part of patient care. So, its costs, kind of affects the patients. He may be waiting for that longer, when he needed that straight away.”(John 217–220).
4.2. Becoming Less Capable of Practicing With Disease And/Or Condition Specific Familiarity
“If it (the outlier patient) is surgical there is a lot of ... drains that you know really little about. And if something goes wrong with any of those drains it’s not easy.”(Rainbow 61–63).
“...there is a lot of this tubing and ...containers and drains...and you don’t even know the names of them. Like they are saying Bellovac. There are different (unfamiliar) names.”(Rainbow 80–82).
“I think I have done everything for this (outlier) patient but I haven’t been able to educate them as much as I normally would if it is a cardiac condition ... It’s just that maybe I could (have) done a bit better…You don‘t know what you don‘t know really.”(Marie 57–60, 292–293).
4.3. Becoming Less Capable of Prioritizing Each Nursing Task
“So I had the added stress of not being able to look after the other patients as well as I should have done ... I think everybody was missing out. I was stressed. But the patient who was in the wrong ward, he (the outlier patient) really suffers more because he was in the wrong ward. And the other patient (specialty-appropriate patients) didn’t get the care and the attention they needed. So it was very stressful and dissatisfy(ing).”(Hope 76–80).
“…When I mentioned that to the doctor, can we not get this patient to High Dependency Unit? Do you think he should be in a different ward? Of course, he totally agreed. When I said, will you do something about it, he just sort of shook his shoulder and left. And when I mentioned that to the team leader, she fully agreed and also did nothing. So, I mention it a few times to her. I mentioned it to the evening shift who took over from me. So yes, I don’t know, maybe I should have done more. Maybe I should have found the nursing supervisor myself, yes. Which again, there is not enough time for sitting on the phone and I really have to look after the patients. So that’s another part of being very dissatisfied and frustrated after days like that.”(Hope 335–344).
4.4. Becoming Less Capable of Predicting
“You don’t feel confident doing it (nursing the outlier patients), and there is no element of predictability, you cannot determine what is going to happen next. You can’t look forward. You are only looking at what (is happening now).”(Rainbow 161–171).
“Well, you feel a bit anxious and stressed … what if something happens ... I might not (have) recognized or there might be something wrong … What if I don’t know the drugs (for this unfamiliar condition/diagnosis of the outlier patients), if I am not sure? Because we are used to knowing everything (about our regular/specialty-appropriate/familiar patients).”(Claire 705–709).
4.5. Becoming Less Capable of Practicing With Inter-Professional Relationality
“So, when we have outliers, we don’t know what those plans are because we are not there with that treating team. Similarly when we have outliers in the other wards, we are really not sure what’s going on. So I see the main disadvantage is the lack of continuity.”(Ann 27–30).
“If it is a (other) specialty areas, for example, renal or cardiology, you are not seeing these people (allied health care members or doctors of the outlier patient’s team) everyday every week ... you don’t establish the same sort of rapport.”(Madeline 104–105).
5. Discussion
5.1. Implications on Nursing Practice: Organizational Commitment of Nurses and the Associated Liability and Accountability
- (a)
- Synchronizing nursing rhythms;
- (b)
- Practicing with disease and/or condition specific familiarity;
- (c)
- Prioritizing each nursing task;
- (d)
- Predicting care requirements;
- (e)
- Practicing with inter-professional relationality as they were nursing the outlier patient.
5.2. Implications on Nursing Practice: Allevating Measures in Place, Studied Phenomenon Remains Prominent
5.3. Implications for Nursing Practice: Specialty Practice Being Challenged
5.4. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kohn, R.; Harhay, M.O.; Bayes, B.; Song, H.; Halpern, S.D.; Kerlin, M.P.; Greysen, S.R. Influence of bedspacing on outcomes of hospitalised medicine service patients: A retrospective cohort study. BMJ Qual. Saf. 2020. [Google Scholar] [CrossRef]
- Stylianou, N.; Fackrell, R.; Vasilakis, C. Are medical outliers associated with worse patient outcomes? A retrospective study within a regional NHS hospital using routine data. BMJ Open 2017, 7, e015676. [Google Scholar] [CrossRef] [Green Version]
- La Regina, M.; Guarneri, F.; Romano, E.; Orlandini, F.; Nardi, R.; Mazzone, A.; Fontanella, A.; Campanini, M.; Manfellotto, D.; Bellandi, T.; et al. What Quality and Safety of Care for Patients Admitted to Clinically Inappropriate Wards: A Systematic Review. J. Gen. Intern. Med. 2019, 34, 1314–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAlister, F.A.; Shojania, K.G. Inpatient bedspacing: Could a common response to hospital crowding cause increased patient mortality? BMJ Qual. Saf. 2018, 27, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garling, P. First Report of the Special Commission of Inquiry: Acute Care Services in NSW Public Hospitals. Available online: https://www.dpc.nsw.gov.au/assets/dpc-nsw-gov-au/publications/Acute-Care-Services-in-NSW-hospitals-listing-437/472484bb89/Volume-3-Special-Commission-of-Inquiry-into-Acute-Care-Services-in-NSW.pdf (accessed on 13 May 2020).
- Heidegger, M. The End of Philosophy; Stambaugh, J., Translator; University of Chicago Press: Illinois, IL, USA, 2003. [Google Scholar]
- Benner, P. From novice to expert. Am. J. Nurs. 1982, 82, 402–407. [Google Scholar] [PubMed]
- Ozdemir, N.G. The Development of Nurses’ Individualized Care Perceptions and Practices: Benner’s Novice to Expert Model Perspective. Int. J. Caring Sci. 2019, 12, 1279. [Google Scholar]
- Walkowiak, D.; Domaradzki, J. Needs assessment study of rare diseases education for nurses and nursing students in Poland. Orphanet J. Rare Dis. 2020, 15, 1–13. [Google Scholar] [CrossRef]
- Dudding-Byth, T. A powerful team: The family physician advocating for patients with a rare disease. Aust. Fam. Physician 2015, 44, 634. [Google Scholar]
- Thompson, J.; Goldin, G. The Hospital: A Social and Architectural History; Yale University Press: Connecticut, CT, USA, 1975. [Google Scholar]
- Chaboyer, W.; Dunn, S.V.; Najman, J. Developing specialty knowledge: The case of Australian critical care nursing. Intensive Crit. Care Nurs. 2000, 16, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Russell, R. From Nightingale to Now; W.B. Saunders/Bailliere Tindall: Sydney, Australia, 1990. [Google Scholar]
- Dixit, S.K.; Sambasivan, M. A review of the Australian healthcare system: A policy perspective. SAGE Open Med. 2018, 6, 2050312118769211. [Google Scholar] [CrossRef] [Green Version]
- NSW Health. Patient Flow Systems. Available online: https://www.health.nsw.gov.au/pfs/Pages/default.aspx (accessed on 13 May 2020).
- Australian Institute of Health and Welfare. Hospital Resources 2015-16: Australian Hospital Statistics. Available online: https://www.aihw.gov.au/getmedia/d37a56cb-dc6b-4b28-a52f-8e00f606ce67/21035.pdf.aspx?inline=true (accessed on 13 May 2020).
- Australian Medical Association. Public Hospital Report Card: An AMA Analysis of Australia’s Public Hospital System. Available online: https://ama.com.au/sites/default/files/documents/AMA%20Hospital%20Report%2018%20FINAL-1.pdf (accessed on 13 May 2020).
- Hospital Authority. Medical Inpatient Bed Occupancy Rates and Numbers of Medical Inpatient Patient Days in Acute Hospitals under Hospital Authority (from 21 to 27 January 2018). Available online: https://gia.info.gov.hk/general/201802/28/P2018022800614_279039_1_1519814299384.pdf (accessed on 13 May 2020).
- National Health Service in England. Bed Availability and Occupancy: Statistical Press Notice, Quarter 3 2018-19. Available online: https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2019/02/KH03-Q3-2018-19-Statistical-Press-Notice-FINAL-7shs.pdf (accessed on 13 May 2020).
- Jones, R. Hospital bed occupancy demystified. Br. J. Healthc. Manag. 2011, 17, 242–248. [Google Scholar] [CrossRef]
- Rankin, J.; Campbell, M. Managing to Nurse: Inside Canada’s Healthcare Reform; University of Toronto Press: Toronto, ON, Canada, 2006. [Google Scholar]
- Lakshmi, C.; Sivakumar, A.L. Application of queueing theory in health care: A literature review. Oper. Res. Health Care 2013, 2, 25–39. [Google Scholar]
- Perimal-Lewis, L.; Li, J.Y.; Hakendorf, P.H.; Ben-Tovim, D.I.; Qin, S.; Thompson, C.H. Relationship between in-hospital location and outcomes of care in patients of a large general medical service. Intern. Med. J. 2013, 43, 712–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santamaria, J.D.; Tobin, A.E.; Anstey, M.H.; Smith, R.J.; Reid, D.A. Do outlier inpatients experience more emergency calls in hospital? An observational cohort study. Med. J. Aust. 2014, 200, 45–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Royal College of Nursing. Principles of Nursing Practice. 2019. Available online: https://www.rcn.org.uk/professional-development/principles-of-nursing-practice (accessed on 13 May 2020).
- American Nurses Association. Scope of Practice. Available online: https://www.nursingworld.org/practice-policy/scope-of-practice/ (accessed on 13 May 2020).
- Australian Health Practitioner Regulation Agency. For Registered Health Practitioners: Code of Conduct. Available online: https://www.ahpra.gov.au/documents/default.aspx?record=WD13%2f10315&dbid=AP&chksum=Vmrrc4PfLa61SqNGWG0gPg%3d%3d (accessed on 13 May 2020).
- Nursing and Midwifery Board of Australia. Registered Nurses Standards for Practice. Available online: https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/Professional-standards/registered-nurse-standards-for-practice.aspx (accessed on 13 May 2020).
- Clinical Excellence Commission. Safety Huddles: Implementation Guide. Available online: http://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0005/403925/Safety-Huddle-Implementation-Guide.pdf (accessed on 13 May 2020).
- Dowie, I. Legal, ethical and professional aspects of duty of care for nurses. Nurs. Stand. 2017, 32, 47–52. [Google Scholar] [CrossRef]
- Williamson, M.; Ghazaly, M.; Bhatt, N.; Nehra, D. Looking after patients, not looking for patients. Bull. R. Coll. Surg. Engl. 2015, 97, 260–262. [Google Scholar] [CrossRef]
- Goulding, L.; Adamson, J.; Watt, I.; Wright, J. Lost in hospital: A qualitative interview study that explores the perceptions of NHS inpatients who spent time on clinically inappropriate hospital wards. Health Expect. 2015, 18, 982–994. [Google Scholar] [CrossRef] [Green Version]
- Evans, H.; Adhiyaman, V. An audit of medical outliers in a north Wales district general hospital. Future Healthc. J. 2017, 4, s13. [Google Scholar] [CrossRef] [PubMed]
- Hassen, Y.; Singh, P.; Pucher, P.H.; Johnston, M.J.; Darzi, A. Identifying quality markers of a safe surgical ward: An interview study of patients, clinical staff, and administrators. Surgery 2018, 163, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Serafini, F.; Fantin, G.; Brugiolo, R.; Lamanna, O.; Aprile, A.; Presotto, F. Outlier admissions of medical patients: Prognostic implications of outlying patients. The experience of the Hospital of Mestre. Ital. J. Med. 2015, 299–302. [Google Scholar] [CrossRef]
- Nursing and Midwifery Board of Australia. Fact Sheet: Advanced Nursing Practice and Specialty Areas within Nursing. Available online: https://www.nursingmidwiferyboard.gov.au/codes-guidelines-statements/faq/fact-sheet-advanced-nursing-practice-and-specialty-areas.aspx (accessed on 13 May 2020).
- Allen, D. The Invisible Work of Nurses: Hospitals, Organisations and Healthcare; Routledge: London, UK, 2014. [Google Scholar]
- Morley, G.; Ives, J.; Bradbury-Jones, C. Moral distress and austerity: An avoidable ethical challenge in healthcare. Health Care Anal. 2019, 27, 185–201. [Google Scholar] [CrossRef] [Green Version]
- Robson, H.; Attard, C. Staff burnout and staff turnover on inpatient wards. Oxford Textb. Inpatient Psychiatry 2019, 277. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidegger, M. Being and Time; Macquarrie, J.; Robinson, E., Translators; Harper & Row: New York, NY, USA, 1962. [Google Scholar]
- Merleau-Ponty, M. Phenomenology of Perception; Smith, C., Translator; Routledge: New York, NY, USA, 2005. [Google Scholar]
- van Manen, M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy; The Althouse Press: Walnut Creek, CA, USA, 2001. [Google Scholar]
- Gadamer, H. Philosophical Hermeneutics; Linge, D., Translator; University of Carlifornia Press: London, UK, 1977. [Google Scholar]
- Minichiello, V.; Aroni, R.; Timewell, E.; Alexander, L. Indepth Interviewing: Principles, Techniques, Analysis, 2nd ed.; Longman: Melbourne, Australia, 1995. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16. [Google Scholar] [CrossRef]
- Annells, M. Hermeneutic phenomenology: Philosophical perspectives and current use in nursing research. J. Adv. Nurs. 1996, 23, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Gosden, C. Social Being and Time; Blackwell: Oxford, UK, 1994. [Google Scholar]
- van Manen, M. Writing in the Dark: Phenomenological Studies in Interpretive Inquiry; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Squires, J.E.; Graham, I.D.; Grinspun, D.; Lavis, J.; Légaré, F.; Bell, R.; Bornstein, S.; Brien, S.E.; Dobrow, M.; Greenough, M.; et al. Inappropriateness of health care in Canada: A systematic review protocol. Syst. Rev. 2019, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- The Nursing Council of Hong Kong. Scope of Professional Practice. Available online: https://www.nchk.org.hk/filemanager/en/pdf/scope_english.pdf (accessed on 14 June 2020).
- Birks, M.; Davis, J.; Smithson, J.; Cant, R. Registered nurse scope of practice in Australia: An integrative review of the literature. Contemp. Nurse 2016, 52, 522–543. [Google Scholar] [CrossRef]
- Griffith, R. The elements of negligence liability in nursing. Br. J. Nurs. 2020, 29, 176–177. [Google Scholar] [CrossRef]
- Black, B.P. Professional Nursing E-Book: Concepts and Challenges; Elsevier: Missouri, MO, USA, 2020. [Google Scholar]
- Jacoby, S.R.; Scruth, E.A. Negligence and the Nurse: The Value of the Code of Ethics for Nurses. Clin. Nurse Spec. 2017, 31, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Darehed, D. The Impact of Organizational and Temporal Factors on Acute Stroke Care in Sweden. Ph.D. Thesis, Umeå universitet, Umeå, Sweden, 2020. [Google Scholar]
- Nolan, M.T.; Mock, V. Measuring Patient Outcomes; Sage Publications: London, UK, 2000. [Google Scholar]
- Mello, M.M.; Frakes, M.D.; Blumenkranz, E.; Studdert, D.M. Malpractice liability and health care quality: A review. JAMA 2020, 323, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Sage, W.M.; Underhill, K. Malpractice Liability and Quality of Care: Clear Answer, Remaining Questions. JAMA 2020, 323, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.L.; Hamilton, P.; Murry, N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. Int. J. Nurs. Stud. 2015, 52, 1121–1137. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.H.; Lee, J.Y.; You, S.J.; Song, K.J.; Hong, K.J. Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes. Int. J. Nurs. Pract. 2020, 26, e12803. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Tucker, A.L.; Graue, R.; Moravick, S.; Yang, J.J. Capacity pooling in hospitals: The hidden consequences of off-service placement. Manag. Sci. 2019. [Google Scholar] [CrossRef]
- Gomez-Rosado, J.C.; Li, Y.H.; Valdés-Hernández, J.; Oliva-Mompeán, F.; Capitán-Morales, L.C. Analysis of Frequency, Type of Complications and Economic Costs of Outlying Patients in General and Digestive Surgery. Cirugía Española Engl. Ed. 2019, 97, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Izady, N.; Mohamed, I. A Clustered Overflow Configuration of Inpatient Beds in Hospitals. Manuf. Serv. Oper. Manag. 2019. [Google Scholar] [CrossRef] [Green Version]
- Gorli, M.; Mengis, J.; Liberati, E.G. A New Space for Patients–How Space Enters Innovation Translation Processes. In Controversies in Healthcare Innovation; Palgrave Macmillan: London, UK, 2018; pp. 21–52. [Google Scholar]
- Landa, P.; La Regina, M.; Tànfani, E.; Orlandini, F.; Campanini, M.; Fontanella, A.; Manfellotto, D.; Testi, A. Modelling Hospital Medical Wards to Address Patient Complexity: A Case-Based Simulation-Optimization Approach. In International Conference on Human-Centred Software Engineering; Springer: Cham, Switzerland, 2019; pp. 25–39. [Google Scholar]
- Fukada, M. Nursing competency: Definition, structure and development. Yonago Acta Med. 2018, 61, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Vernon, R.; Chiarella, M.; Papps, E.; Lark, A. Assuring competence or ensuring performance. Collegian 2019, 26, 399–406. [Google Scholar] [CrossRef]
- Johannnsdottir, F.; Hardardottir, L. Operational Difficulties in Newly Merged Hospital Wards a Case Study at The Department of Plastic and Hand Surgery, Sahlgrenska University Hospital. Master’s Thesis, Chalmers University of Technology, Göteborg, Sweden, 2011. [Google Scholar]
- Jameton, A. Nursing Practice: The Ethical Issues; Prentice-Hall: New Jersey, NJ, USA, 1984. [Google Scholar]
- Morley, G.; Ives, J.; Bradbury-Jones, C.; Irvine, F. What is ‘moral distress’? A narrative synthesis of the literature. Nurs. Ethics 2019, 26, 646–662. [Google Scholar] [CrossRef] [Green Version]
- Corley, M.C.; Minick, P.; Elswick, R.K.; Jacobs, M. Nurse moral distress and ethical work environment. Nurs. Ethics 2005, 12, 381–390. [Google Scholar] [CrossRef]
- Heinen, M.; Van Oostveen, C.; Peters, J.; Vermeulen, H.; Huis, A. An integrative review of leadership competencies and attributes in advanced nursing practice. J. Adv. Nurs. 2019, 75, 2378–2392. [Google Scholar] [CrossRef] [PubMed]
- Castner, J.; Wu, Y.W.B.; Dean-Baar, S. Multi-level model of missed nursing care in the context of hospital merger. West. J. Nurs. Res. 2015, 37, 441–461. [Google Scholar] [CrossRef] [PubMed]
- Manetti, W. Sound clinical judgment in nursing: A concept analysis. Nurs. Forum 2019, 54, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.I.; Kim, S.W.; Chin, H.J. Patient Participation in Patient Safety and Its Relationships with Nurses’ Patient-Centered Care Competency, Teamwork, and Safety Climate. Asian Nurs. Res. 2019, 13, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, M.S.N.; Corln, C.; Bagonis, R.N.; Lewandowski, R.N. Evidence Based Solutions: Creating Specialty Units; Thomas Jefferson University Hospital: Philadelphia, PA, USA, 2019. [Google Scholar]
- Copanitsanou, P.; Fotos, N.; Brokalaki, H. Effects of work environment on patient and nurse outcomes. Br. J. Nurs. 2017, 26, 172–176. [Google Scholar] [CrossRef]
- Shin, S.; Park, J.H.; Bae, S.H. Nurse staffing and nurse outcomes: A systematic review and meta-analysis. Nurs. Outlook 2018, 66, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Creta, A. Assessing and Decreasing Perceptions of Missed Nursing Care in an Acute Care Setting by Improving Teamwork. Nurs. Res. 2015, 64, E34. [Google Scholar]
- Schneider, Z.; Whitehead, D.; LoBiondo-Wood, G.; Faan, P.R.; Haber, J.; Faan, P.R. Nursing and Midwifery Research: Methods and Appraisal for Evidence Based Practice; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Clark, L.; Birkhead, A.S.; Fernandez, C.; Egger, M.J. A transcription and translation protocol for sensitive cross-cultural team research. Qual. Health Res. 2017, 27, 1751–1764. [Google Scholar] [CrossRef]
- Burhans, L.; Alligood, M. Quality nursing care in the words of the nurses. J. Adv. Nurs. 2010, 66, 1689–1697. [Google Scholar] [CrossRef]
- Cypress, B.S. Rigor or reliability and validity in qualitative research: Perspectives, strategies, reconceptualization, and recommendations. Dimens. Crit. Care Nurs. 2017, 36, 253–263. [Google Scholar] [CrossRef]
- Vicary, S.; Young, A.; Hicks, S. A reflective journal as learning process and contribution to quality and validity in interpretative phenomenological analysis. Qual. Soc. Work 2017, 16, 550–565. [Google Scholar] [CrossRef] [Green Version]
- van Manen, M. Practicing phenomenological writing. Phenomenol. Pedagog. 1984, 2, 36–69. [Google Scholar] [CrossRef]
- Gadamer, H.; Weinsheimer, J.; Marshall, D. Truth and Method; Sheed and Ward: London, UK, 1975. [Google Scholar]
- Ryan, F.; Coughlan, M.; Cronin, P. Step-by-step guide to critiquing research. Part 2: Qualitative research. Br. J. Nurs. 2007, 16, 738–744. [Google Scholar] [CrossRef]
- Errasti-Ibarrondo, B.; Jordán, J.A.; Díez-Del-Corral, M.P.; Arantzamendi, M. Van Manen’s phenomenology of practice: How can it contribute to nursing? Nurs. Inq. 2019, 26, e12259. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pseudonym | Gender | Age by Decade | Years of Nursing Experience | Area of Practice |
|---|---|---|---|---|
| Rainbow | F | 50’s | 12 | Coronary Care Unit |
| Agnes | F | 50’s | 31 | Rehabilitation/Acute Stroke Unit |
| Ann | F | 60’s | >30 | Discharge planning |
| John | M | 50’s | 38 | Respiratory ward |
| Madeline | F | 40’s | 23 | Respiratory ward |
| Marie | F | 30’s | 17 | Medical ward |
| Peter | M | 50’s | >30 | Cardiac ward |
| Claire | F | 50’s | 34 | Gynecology ward |
| Mary | F | 30’s | 7 | Transplant ward |
| Hope | F | 50’s | 32 | Neurology |
| Kay | F | 50’s | 38 | Pediatric |
| Research Phases | Phenomenological Data Analysis |
|---|---|
| 1. During the interview | Listen to participant’s description of their experience of nursing the outlier patients Develop first interpretation of what participants have said |
| 2. Following each interview session | Write summary for each interview session Record reflective notes (memoing) according to my experience as a nurse and as a researcher Record immediate apparent concepts and themes (if any) |
| 3. During transcription | Use my personal experience as a starting point for data interpretation Record my later understanding of what participants have said |
| 4. During the line-by-line analysis with interview scripts | Discover the commonalities and differences among subthemes emerged Uncover initial thematic aspect by referring to the summaries and reflection written previously |
| Initial Themes | Initial Sub-Themes |
|---|---|
| 1. Nurse’s reported feeling from experience of nursing the outlier patients | In Doubt; Belittled; Hesitate; Fearful; Dissatisfied; (Learnt) Helplessness; In Doubt; Devastating; Acceptance/Indifference; Uncertainty; Frustrated re: patient care/outcome; Frustrated re: Uncertainty; Frustrated re: pressure; Frustrated re: lack of support/uncaring attitude; Being ignored; Frustrated re: staff and resources; Stress re: Lack of support; Frustrated; Not confident; Abuse; Stress re: intense workload; Not prepared; Guilt; Difficult; Bad; Unfamiliar; Feeling stress; Limited; Failure; Feeling hard; Not easy; Tense inside; Not welcoming/Don’t like/lack of interest; Not positive; Odd/Different; Stress: patient not getting care; Worry; Frustrated; Inadequate; Inappropriate; Anger re: uncaring attitude; Painful; Awful; Disappointed/unhappy; Unease |
| 2. Perceived care ladder | Basic-Optimal/good; Basic-Human; Basic- Continuity; Something missing; Basic- Comprehensive; Generic- Specialized; Basic- Adequate- Specialized-Appropriate |
| 3. Perceived care of outlier patients | Minimal care; Missing in care; Not basic care; Inappropriate care/inadequate; Compromised care; Best possible nursing; No predictability; not good nursing care/only basics; Not continuity of care; Not just babysitting/require intensive look after |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, J.; West, S.; Boughton, M. The Frontline Nurse’s Experience of Nursing Outlier Patients. Int. J. Environ. Res. Public Health 2020, 17, 5232. https://doi.org/10.3390/ijerph17145232
Cheung J, West S, Boughton M. The Frontline Nurse’s Experience of Nursing Outlier Patients. International Journal of Environmental Research and Public Health. 2020; 17(14):5232. https://doi.org/10.3390/ijerph17145232
Chicago/Turabian StyleCheung, Jasmine, Sandra West, and Maureen Boughton. 2020. "The Frontline Nurse’s Experience of Nursing Outlier Patients" International Journal of Environmental Research and Public Health 17, no. 14: 5232. https://doi.org/10.3390/ijerph17145232
APA StyleCheung, J., West, S., & Boughton, M. (2020). The Frontline Nurse’s Experience of Nursing Outlier Patients. International Journal of Environmental Research and Public Health, 17(14), 5232. https://doi.org/10.3390/ijerph17145232