Right Ventricular Diastolic Dysfunction after Marathon Run

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shave, R.; Oxborough, D. Exercise-induced cardiac injury: Evidence from novel imaging techniques and highly sensitive cardiac troponin assays. Prog. Cardiovasc. Dis. 2012, 54, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Leyk, D.; Erley, O.; Gorges, W.; Ridder, D.; Rüther, T.; Wunderlich, M.; Sievert, A.; Essfeld, D.; Piekarski, C.; Erren, T. Performance, training and lifestyle parameters of marathon runners aged 20–80 years: Results of the PACE-study. Int. J. Sports Med. 2009, 30, 360–365. [Google Scholar] [CrossRef]
- La Gerche, A.; Rakhit, D.J.; Claessen, G. Exercise and the right ventricle: A potential Achilles’ heel. Cardiovasc. Res. 2017, 113, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Herve, P.; Lau, E.M.; Sitbon, O.; Savale, L.; Montani, D.; Godinas, L.; Lador, F.; Jaïs, X.; Parent, F.; Günther, S.; et al. Criteria for diagnosis of exercise pulmonary hypertension. Eur. Respir. J. 2015, 46, 728–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Gerche, A.; Heidbüchel, H.; Burns, A.T.; Mooney, D.J.; Taylor, A.J.; Pfluger, H.B.; Inder, W.J.; Macisaac, A.I.; Prior, D.L. Disproportionate exercise load and remodeling of the athlete’s right ventricle. Med. Sci. Sports Exerc. 2011, 43, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Axell, R.G.; Hoole, S.P.; Hampton-Till, J.; White, P.A. RV diastolic dysfunction: Time to re-evaluate its importance in heart failure. Heart Fail. Rev. 2015, 20, 363–373. [Google Scholar] [CrossRef]
- Naeije, R.; Badagliacca, R. The overloaded right heart and ventricular interdependence. Cardiovasc. Res. 2017, 113, 1474–1485. [Google Scholar] [CrossRef]
- Elliott, A.D.; La Gerche, A. The right ventricle following prolonged endurance exercise: Are we overlooking the more important side of the heart? A meta-analysis. Br. J. Sports Med. 2015, 49, 724–729. [Google Scholar] [CrossRef]
- Brutsaert, D.L.; Rademakers, F.E.; Sys, S.U. Triple control of relaxation: Implications in cardiac disease. Circulation 1984, 69, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Hirota, Y. A clinical study of left ventricular relaxation. Circulation 1980, 62, 756–763. [Google Scholar] [CrossRef] [Green Version]
- Murch, S.D.; La Gerche, A.; Roberts, T.J.; Prior, D.L.; MacIsaac, A.I.; Burns, A.T. Abnormal right ventricular relaxation in pulmonary hypertension. Pulm. Circ. 2015, 5, 370–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silbiger, J.J. Pathophysiology and echocardiographic diagnosis of left ventricular diastolic dysfunction. J. Am. Soc. Echocardiogr. 2019, 32, 216–232. [Google Scholar] [CrossRef] [PubMed]
- Lewicka-Potocka, Z.; Dąbrowska-Kugacka, A.; Lewicka, E.; Kaleta, A.M.; Dorniak, K.; Daniłowicz-Szymanowicz, L.; Fijałkowski, M.; Nabiałek-Trojanowska, I.; Ratkowski, W.; Potocki, W.; et al. The “athlete’s heart” features in amateur male marathon runners. Cardiol. J. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Zimbarra Cabrita, I.; Ruísanchez, C.; Grapsa, J.; Dawson, D.; North, B.; Pinto, F.J.; Gibbs, J.S.; Nihoyannopoulos, P. Validation of the isovolumetric relaxation time for the estimation of pulmonary systolic arterial blood pressure in chronic pulmonary hypertension. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Dabrowska-Kugacka, A.; Claeys, M.J.; Rademakers, F.E. Diastolic indexes during dobutamine stress echocardiography in patients early after myocardial infarction. J. Am. Soc. Echocardiogr. 1998, 11, 26–35. [Google Scholar] [CrossRef]
- Jurcut, R.; Giusca, S.; La Gerche, A.; Vasile, S.; Ginghina, C.; Voigt, J.U. The echocardiographic assessment of the right ventricle: What to do in 2010? Eur. J. Echocardiogr. 2010, 11, 81–96. [Google Scholar] [CrossRef] [Green Version]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Oxborough, D.; Shave, R.; Middleton, N.; Whyte, G.; Forster, J.; George, K. The impact of marathon running upon ventricular function as assessed by 2D, Doppler, and tissue-Doppler echocardiography. Echocardiography 2006, 23, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Roeh, A.; Schuster, T.; Jung, P.; Schneider, J.; Halle, M.; Scherr, J. Two dimensional and real-time three dimensional ultrasound measurements of left ventricular diastolic function after marathon running: Results from a substudy of the BeMaGIC trial. Int. J. Cardiovasc. Imaging 2019, 35, 1861–1869. [Google Scholar] [CrossRef] [PubMed]
- Neilan, T.G.; Yoerger, D.M.; Douglas, P.S.; Marshall, J.E.; Halpern, E.F.; Lawlor, D.; Picard, M.H.; Wood, M.J. Persistent and reversible cardiac dysfunction among amateur marathon runners. Eur. Heart J. 2006, 27, 1079–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neilan, T.G.; Januzzi, J.L.; Lee-Lewandrowski, E.; Ton-Nu, T.T.; Yoerger, D.M.; Jassal, D.S.; Lewandrowski, K.B.; Siegel, A.J.; Marshall, J.E.; Douglas, P.S.; et al. Myocardial injury and ventricular dysfunction related to training levels among nonelite participants in the Boston marathon. Circulation 2006, 114, 2325–2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oğuzhan, A.; Arinç, H.; Abaci, A.; Topsakal, R.; Kemal, E.N.; Ozdoğru, I.; Basar, E.; Ergin, A. Preload dependence of Doppler tissue imaging derived indexes of left ventricular diastolic function. Echocardiography 2005, 22, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Alarrayed, S.; Garadah, T.S.; Alawdi, A.A. The impact of left ventricular preload reduction on cardiac pulsed Doppler indices during hemodialysis and its relation to intra-dialysis hypotension: A pulsed Doppler study. Saudi J. Kidney Dis. Transplant. 2009, 20, 201–207. [Google Scholar]
- Burns, A.T.; Connelly, K.A.; La Gerche, A.; Mooney, D.J.; Chan, J.; MacIsaac, A.I.; Prior, D.L. Effect of heart rate on tissue Doppler measures of diastolic function. Echocardiography 2007, 24, 697–701. [Google Scholar] [CrossRef]
- Alshaher, M.; El-Mallakh, R.; Dawn, B.; Siddiqui, T.; Longaker, R.A.; Stoddard, M.F. Cardiac manifestations of exhaustive exercise in nonathletic adults: Does cardiac fatigue occur? Echocardiography 2007, 24, 237–242. [Google Scholar] [CrossRef]
- Oxborough, D.; Whyte, G.; Wilson, M.; O’Hanlon, R.; Birch, K.; Shave, R.; Smith, G.; Godfrey, R.; Prasad, S.; George, K. A depression in left ventricular diastolic filling following prolonged strenuous exercise is associated with changes in left atrial mechanics. J. Am. Soc. Echocardiogr. 2010, 23, 968–976. [Google Scholar] [CrossRef]
- Wierzbowska-Drabik, K.; Picano, E.; Bossone, E.; Ciampi, Q.; Lipiec, P.; Kasprzak, J.D. The feasibility and clinical implication of tricuspid regurgitant velocity and pulmonary flow acceleration time evaluation for pulmonary pressure assessment during exercise stress echocardiography. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1027–1034. [Google Scholar] [CrossRef]
- Buckberg, G.; Hoffman, J.I. Right ventricular architecture responsible for mechanical performance: Unifying role of ventricular septum. J. Thorac. Cardiovasc. Surg. 2014, 148, 3166–3171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Gerche, A.; Burns, A.T.; Mooney, D.J.; Inder, W.J.; Taylor, A.J.; Bogaert, J.; Macisaac, A.I.; Heidbüchel, H.; Prior, D.L. Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur. Heart J. 2012, 33, 998–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smolarek, D.; Gruchała, M.; Sobiczewski, W. Echocardiographic evaluation of right ventricular systolic function: The traditional and innovative approach. Cardiol. J. 2017, 24, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Meric, M.; Yesildag, O.; Yuksel, S.; Soylu, K.; Arslandag, M.; Dursun, I.; Zengin, H.; Koprulu, D.; Yilmaz, O. Tissue doppler myocardial performance index in patients with heart failure and its relationship with haemodynamic parameters. Int. J. Cardiovasc. Imaging 2014, 30, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Hamilton-Craig, C.R.; Stedman, K.; Maxwell, R.; Anderson, B.; Stanton, T.; Chan, J.; Yamada, A.; Scalia, G.M.; Burstow, D.J. Accuracy of quantitative echocardiographic measures of right ventricular function as compared to cardiovascular magnetic resonance. Int. J. Cardiol. Heart Vasc. 2016, 23, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Ogihara, Y.; Yamada, N.; Dohi, K.; Matsuda, A.; Tsuji, A.; Ota, S.; Ishikura, K.; Nakamura, M.; Ito, M. Utility of right ventricular Tei-index for assessing disease severity and determining response to treatment in patients with pulmonary arterial hypertension. J. Cardiol. 2014, 63, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Kasikcioglu, E.; Oflaz, H.; Akhan, H.; Kayserilioglu, A. Right ventricular myocardial performance index and exercise capacity in athletes. Heart Vessels 2005, 20, 147–152. [Google Scholar] [CrossRef]
- Tüzün, N.; Ergün, M.; Alioğlu, E.; Edem, E.; Tengiz, I.; Aytemiz, F.; Ercan, E.; İşleğen, Ç. TEI Index in elite sprinters and endurance athletes. J. Sports Med. Phys. Fit. 2015, 55, 988–994. [Google Scholar]



{kind=link}
{kind=link}
| Parameter | Stage I | Stage II | Stage III | ANOVA p-Value | Post-Hoc p-Value | |
|---|---|---|---|---|---|---|
| Mean ± SD 1 or Median (1st; 3rd Quartile) 2 | Stage I vs. II | Stage I vs. III | ||||
| LV EF (%) | 61.8 ± 4.9 | 60.5 ± 4.4 | 60.7 ± 4.5 | * 0.38 | - | - |
| LV GLS (%) | −19.9 ± 2.3 | −19.4 ± 2.1 | −19.7 ± 2.2 | * 0.41 | - | - |
| RV 4CSL (%) | −22.0 ± 2.8 | −20.80 ± 2.6 | −21.49 ± 2.5 | * <0.05 | <0.05 | 0.46 |
| TAPSE (mm) | 25.0 ± 3.6 | 24.0 ± 3.7 | 25.0 ± 2.7 | * 0.56 | - | - |
| RV FAC (%) | 43 (37; 45) | 39 (35; 44) | 41 (36; 45) | ^ 0.19 | - | - |
| RVd MID (cm) | 3.4 ± 0.6 | 3.7 ± 0.5 | 3.5 ± 0.5 | * <0.01 | <0.01 | 0.08 |
| RVd BAS (cm) | 3.8 ± 0.4 | 3.8 ± 0.5 | 3.9 ± 0.5 | * 0.44 | - | - |
| LVd BAS (cm) | 4.8 ± 0.4 | 4.6 ± 0.3 | 4.9 ± 0.3 | * <0.001 | <0.01 | 0.88 |
| RVd/LVd BAS | 0.77 ± 0.1 | 0.82 ± 0.1 | 0.79 ± 0.1 | * <0.05 | <0.05 | 0.59 |
| Parameter | Stage I | Stage II | Stage III | ANOVA p-Value | Post-Hoc p-Value | |
|---|---|---|---|---|---|---|
| Mean ± SD 1 or Median (1st; 3rd Quartile) 2 | Stage I vs. II | Stage I vs. III | ||||
| S’_LW (cm/sec) | 11 ± 3 | 11 ± 3 | 11 ± 3 | * 0.88 | - | - |
| E’_LW (cm/sec) | 15 (12; 17) | 12 (10; 15) | 14 (13; 16) | ^ <0.001 | <0.05 | ns |
| A’_LW (cm/sec) | 8 (7;9) | 10 (9; 11) | 8 (7; 9) | ^ <0.001 | <0.05 | ns |
| E’/A’_LW | 1.8 (1.4; 2.1) | 1.2 (1.0; 1.5) | 1.9 (1.6; 2.3) | ^ <0.001 | <0.05 | ns |
| IVRT_LW (ms) | 53 ± 17 | 54 ± 19 | 56 ± 15 | * 0.99 | - | - |
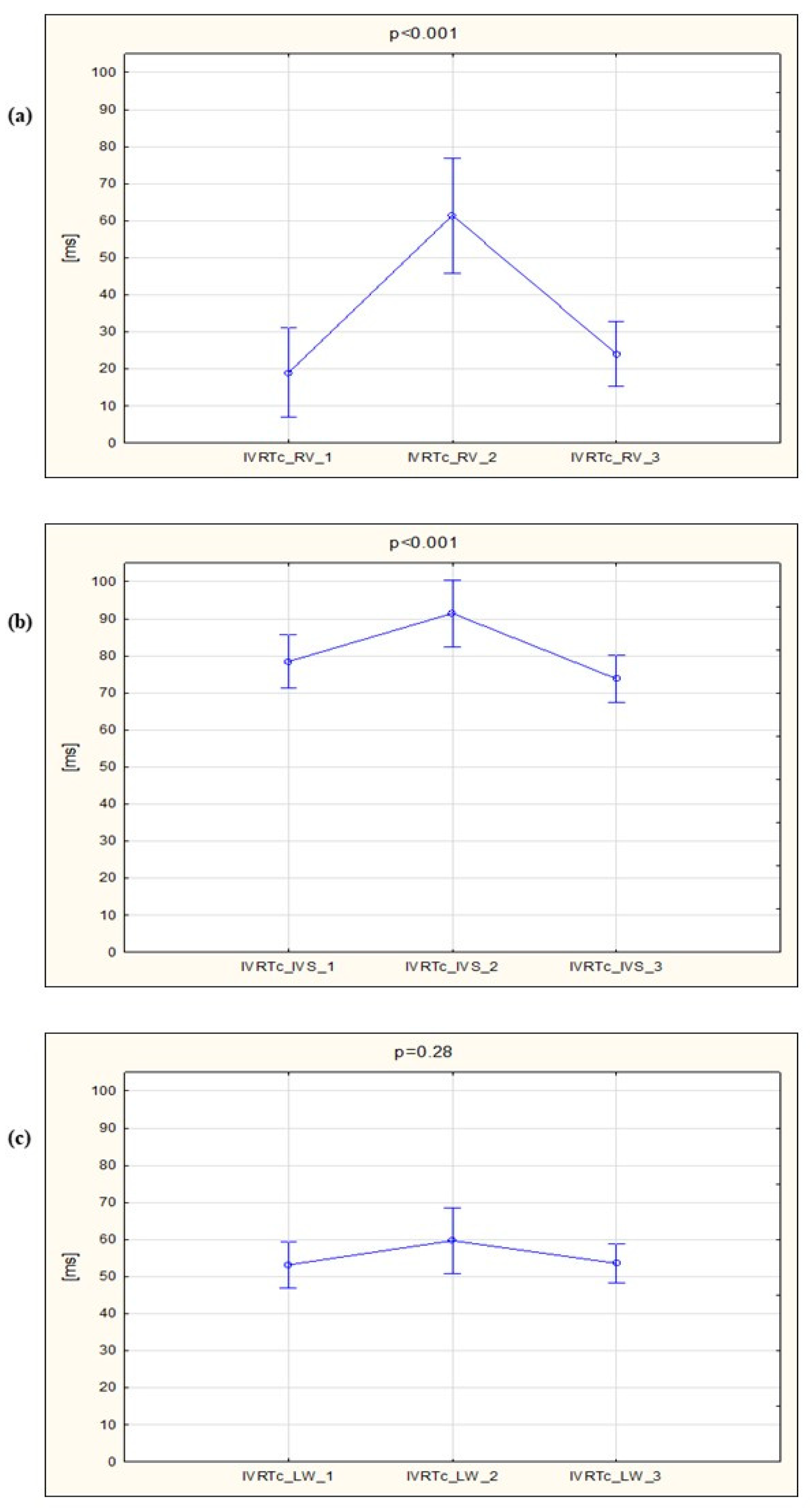
| IVRTc_LW | 53 ± 17 | 59 ± 23 | 54 ± 15 | * 0.28 | - | - |
| MPI_LW | 0.41 ± 0.08 | 0.45 ± 0.17 | 0.42 ± 0.07 | * 0.20 | - | - |
| S’_IVS (cm/sec) | 8 (8; 9) | 9 (8; 10) | 9 (7; 10) | ^ 0.24 | - | - |
| E’_IVS (cm/sec) | 11 ± 2 | 10 ± 2 | 11 ± 2 | * <0.001 | <0.01 | 0.73 |
| A’_IVS (cm/sec) | 8 (8; 10) | 10 (9; 11) | 8 (7; 10) | ^ <0.001 | <0.05 | ns |
| E’/A’_IVS | 1.3 ± 0.4 | 1.0 ± 0.3 | 1.4 ± 0.4 | * <0.001 | <0.001 | 0.26 |
| IVRT_IVS (ms) | 82 (65; 95) | 80 (68; 94) | 78 (64; 86) | ^ 0.46 | - | - |
| IVRTc_IVS | 78 (66; 92) | 92 (77; 108) | 73 (65; 85) | ^ <0.001 | <0.05 | ns |
| MPI_IVS | 0.55 (0.44; 0.59) | 0.53 (0.44; 0.6) | 0.47 (0.44; 0.54) | ^ 0.09 | - | - |
| E_MV (cm/sec) | 71 (67; 87) | 67 (55; 77) | 78 (68; 92) | ^ <0.01~ | ns | ns |
| A_MV (cm/sec) | 51 ± 10 | 65 ± 14 | 56 ± 11 | * <0.001 | <0.001 | 0.29 |
| E/A_MV | 1.5 ± 0.4 | 1.1 ± 0.3 | 1.5 ± 0.4 | * <0.001 | <0.001 | 0.7 |
| E_MV/E’_LW | 5.4 ± 1.2 | 5.5 ± 1.6 | 5.6 ± 1.8 | * 0.66 | - | - |
| E_MV/E’_IVS | 7.1 ± 1.5 | 7.0 ± 1.8 | 7.6 ± 2.0 | * 0.34 | - | - |
| E_MV/E’_AVG | 6.3 (5.2; 7.0) | 5.8 (5.0; 7.2) | 6.2 (5.4; 7.3) | ^ 0.74 | - | - |
| Parameter | Stage I | Stage II | Stage III | ANOVA p-Value | Post-Voc p-Value | |
|---|---|---|---|---|---|---|
| Mean ± SD 1 or Median (1st; 3rd Quartile) 2 | Stage I vs. II | Stage I vs. III | ||||
| S’_RV (cm/sec) | 14 (13; 16) | 14 (13.5; 16) | 15 (13; 16) | ^ 0.51 | - | - |
| E’_RV (cm/sec) | 12 (11; 15) | 12 (9; 14) | 14 (13; 16) | ^ <0.05 ~ | ns | ns |
| A’_RV (cm/sec) | 13 (10; 14) | 16 (13; 20) | 13 (12; 16) | ^ <0.01 | <0.05 | ns |
| E’/A’_RV | 1.0 (0.9; 1.2) | 0.7 (0.6; 0.9) | 1.2 (0.9; 1.3) | ^ <0.001 | <0.05 | ns |
| IVRT_RV (ms) | 0 (0; 29) | 52 (32; 70) | 21 (9; 34) | ^ <0.001 | <0.05 | ns |
| IVRTc_RV (ms) | 0 (0; 27) | 58 (39; 78) | 20 (0; 35) | ^ <0.001 | <0.05 | ns |
| MPI_RV | 0.28 (0.22; 0.37) | 0.48 (0.35; 0.64) | 0.33 (0.25; 0.41) | ^ <0.001 | <0.05 | ns |
| E_TV (cm/sec) | 55 ± 13 | 49 ± 11 | 56 ± 11 | * 0.18 | - | - |
| A_TV (cm/sec) | 33 ± 10 | 46 ± 15 | 31 ± 8 | * <0.001 | <0.001 | 0.99 |
| E/A_TV | 1.7 ± 0.4 | 1.2 ± 0.3 | 1.9 ± 0.6 | * <0.001 | <0.001 | 0.55 |
| E_TV/E’_RV | 4.5 ± 1.1 | 4.2 ± 1.7 | 3.9 ± 1.0 | * 0.44 | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewicka-Potocka, Z.; Dąbrowska-Kugacka, A.; Lewicka, E.; Gałąska, R.; Daniłowicz-Szymanowicz, L.; Faran, A.; Nabiałek-Trojanowska, I.; Kubik, M.; Kaleta-Duss, A.M.; Raczak, G. Right Ventricular Diastolic Dysfunction after Marathon Run. Int. J. Environ. Res. Public Health 2020, 17, 5336. https://doi.org/10.3390/ijerph17155336
Lewicka-Potocka Z, Dąbrowska-Kugacka A, Lewicka E, Gałąska R, Daniłowicz-Szymanowicz L, Faran A, Nabiałek-Trojanowska I, Kubik M, Kaleta-Duss AM, Raczak G. Right Ventricular Diastolic Dysfunction after Marathon Run. International Journal of Environmental Research and Public Health. 2020; 17(15):5336. https://doi.org/10.3390/ijerph17155336
Chicago/Turabian StyleLewicka-Potocka, Zuzanna, Alicja Dąbrowska-Kugacka, Ewa Lewicka, Rafał Gałąska, Ludmiła Daniłowicz-Szymanowicz, Anna Faran, Izabela Nabiałek-Trojanowska, Marcin Kubik, Anna Maria Kaleta-Duss, and Grzegorz Raczak. 2020. "Right Ventricular Diastolic Dysfunction after Marathon Run" International Journal of Environmental Research and Public Health 17, no. 15: 5336. https://doi.org/10.3390/ijerph17155336
APA StyleLewicka-Potocka, Z., Dąbrowska-Kugacka, A., Lewicka, E., Gałąska, R., Daniłowicz-Szymanowicz, L., Faran, A., Nabiałek-Trojanowska, I., Kubik, M., Kaleta-Duss, A. M., & Raczak, G. (2020). Right Ventricular Diastolic Dysfunction after Marathon Run. International Journal of Environmental Research and Public Health, 17(15), 5336. https://doi.org/10.3390/ijerph17155336