Surgical Smoke and Airborne Microbial Contamination in Operating Theatres: Influence of Ventilation and Surgical Phases


Abstract
:1. Introduction
2. Materials and Methods
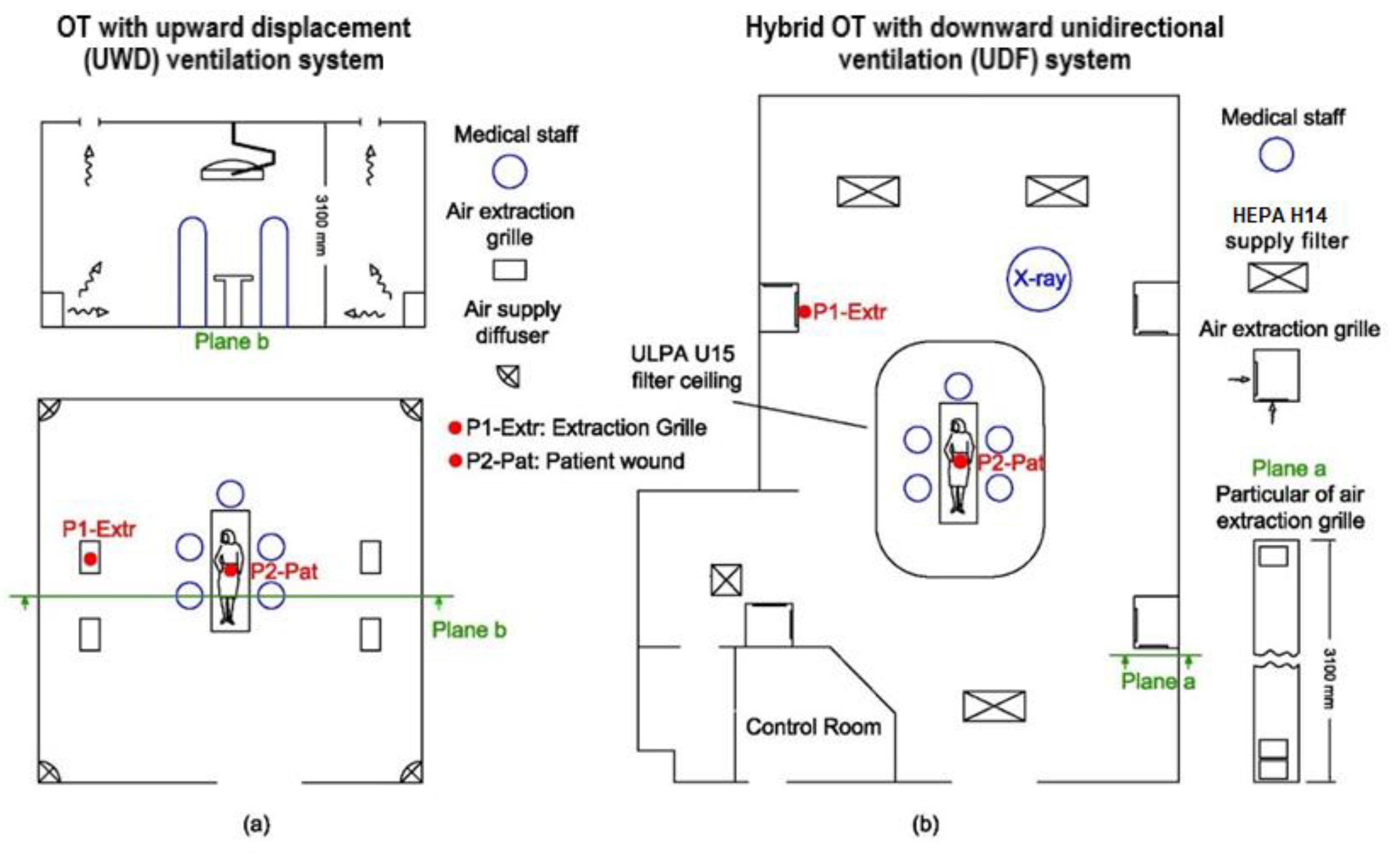
2.1. Operating Theatres
2.2. Instruments and Probe Positioning
2.3. Experimental Procedure and the Role of Medical Staff
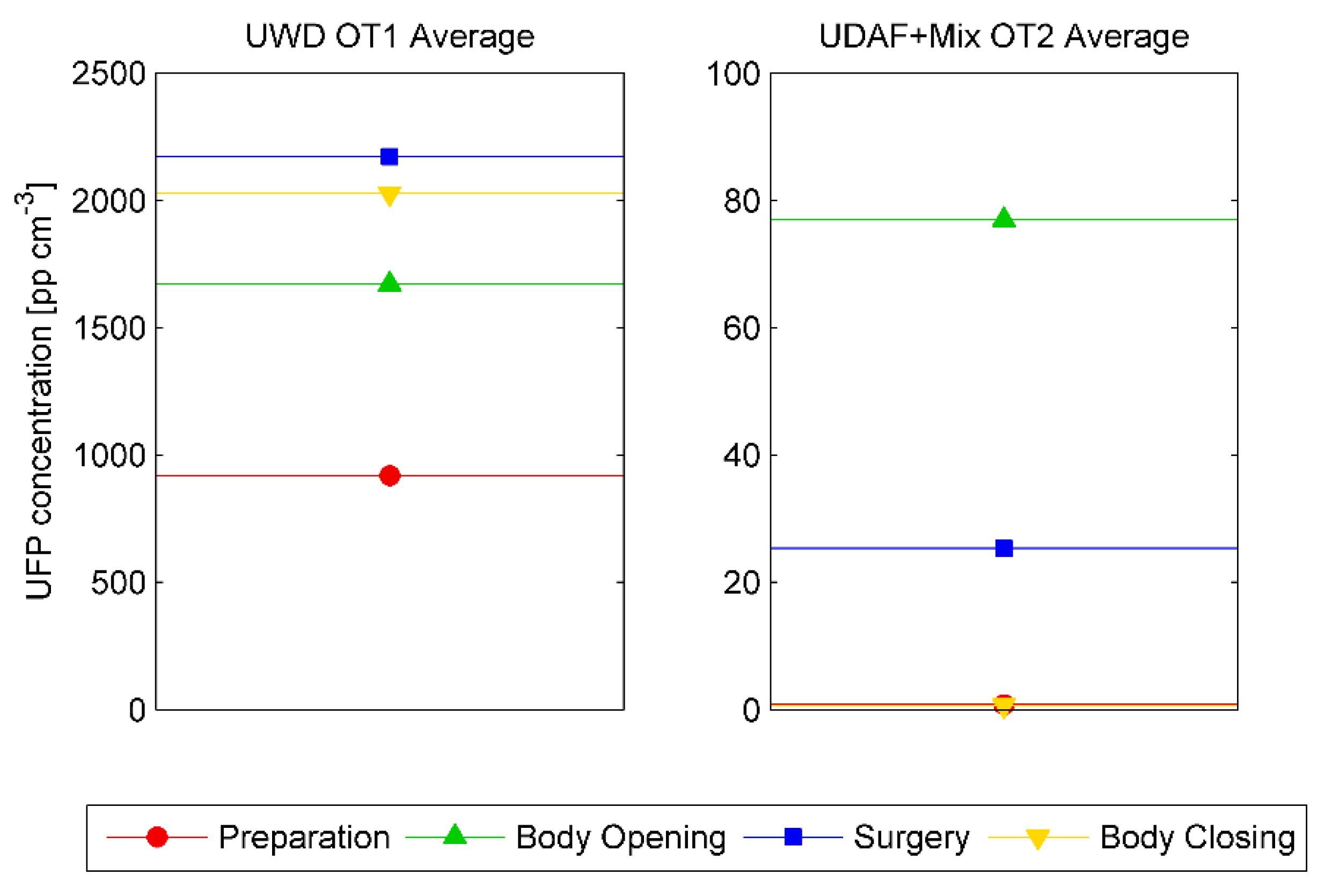
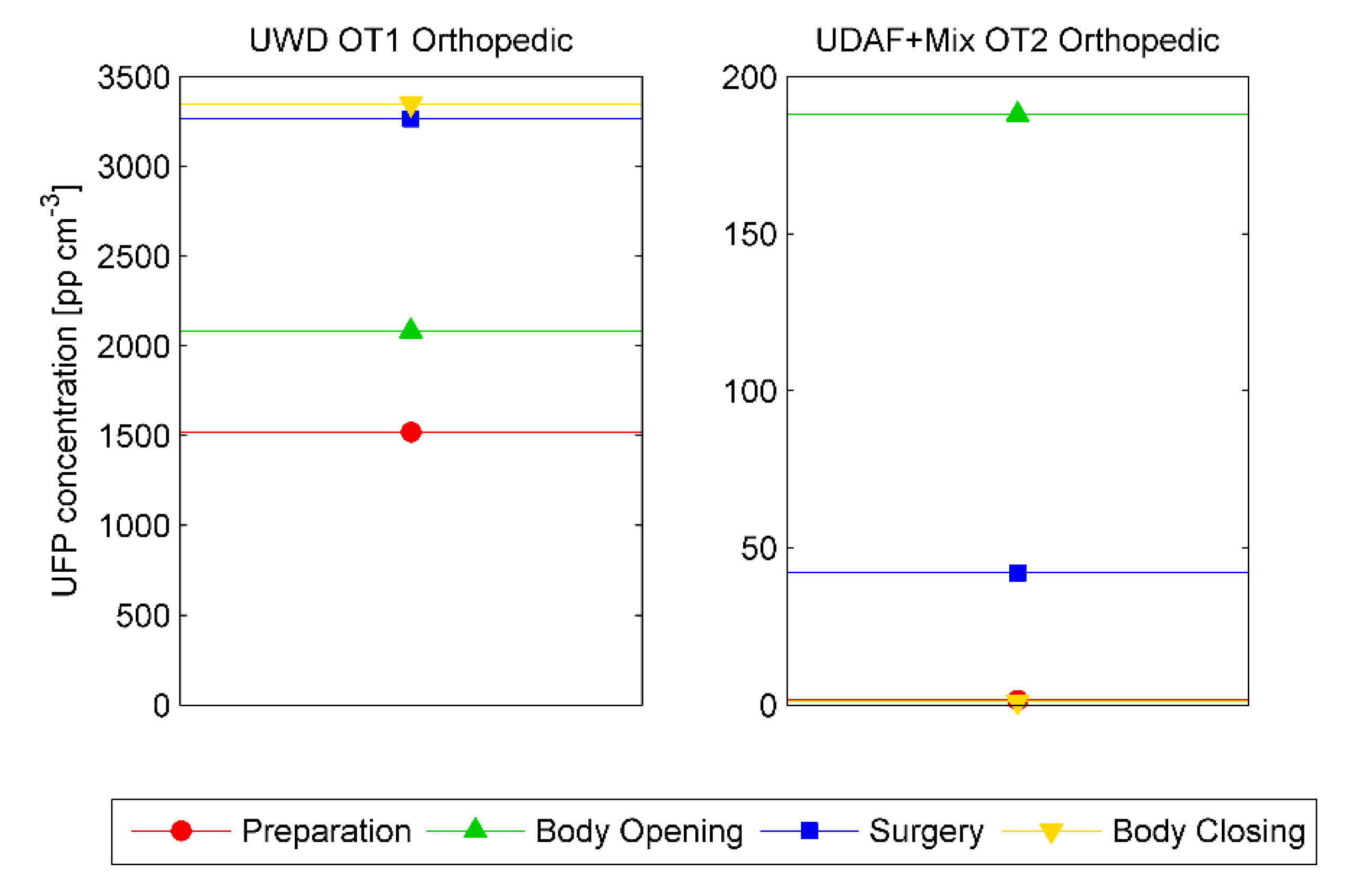
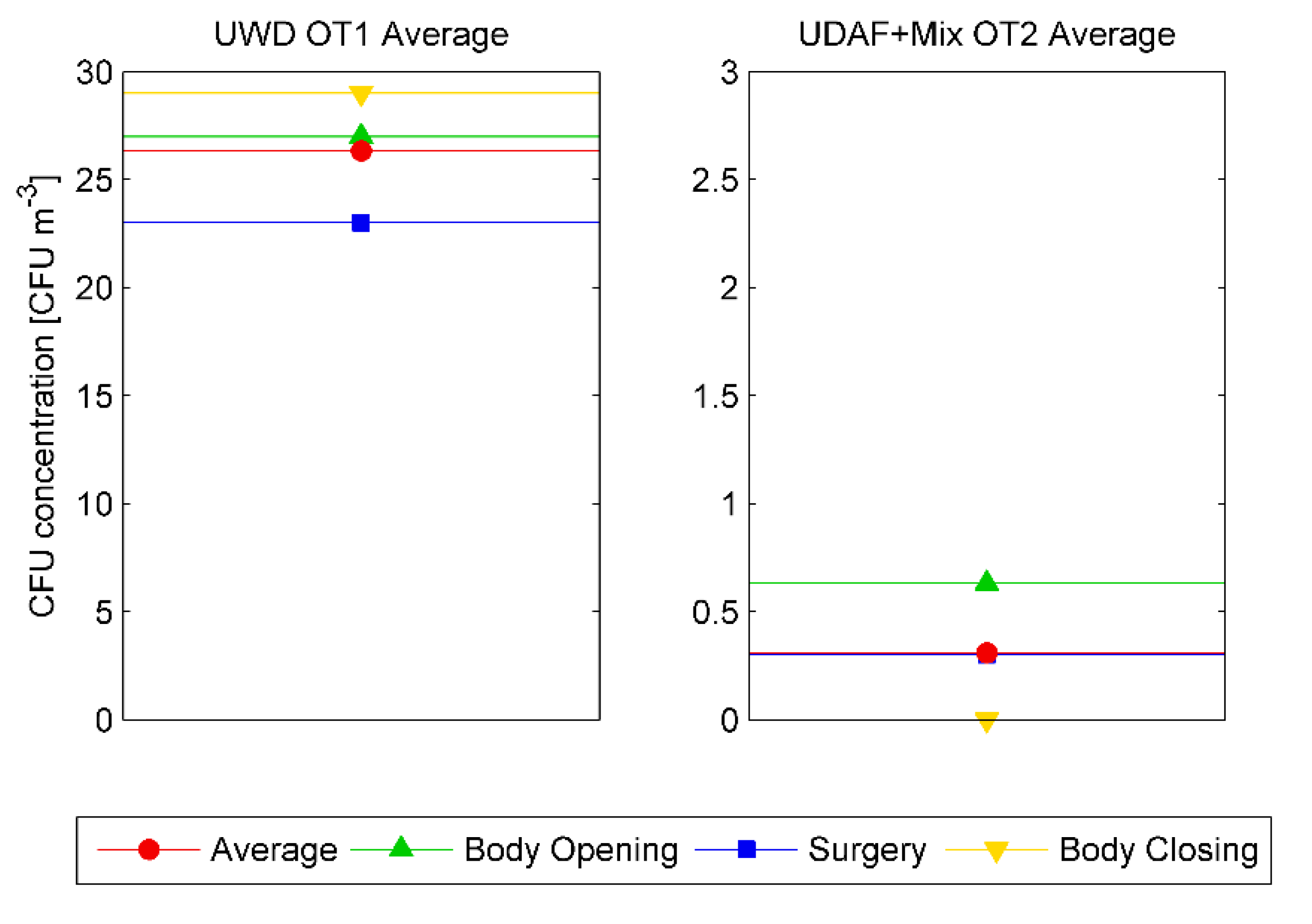
- Preparation:(i) Preparation of the room and the equipment. Equipment and tools are kept sterile passing from the grey outside area to the sterile area (protected zone) and covered with sterile plastic layers. (ii) Patient entry and anesthesia procedure. This step takes place before or after the patient is transferred to the operating table, depending on the type of surgical operation. In the preparation for the operation, the body is shaved, cleaned, disinfected, and covered to expose only the portion to be treated. In this phase the door is opened frequently and the number of personnel in the room is variable, from 2–3 nurses during the preparation of the equipment to a higher number of nurses and anesthetists in the subsequent moments.
- Body openingPatient body is opened, and tissues cut by ESTs as preparatory step for the main surgical phase. This part may take from few minutes to hours, depending on the type of operation. The number of people varies from one or two surgeons, and one or two anesthetists, plus a variable number of nurses.
- Main surgeryThe surgery phase is performed. The use of EST is limited compared to the previous phase. The size of medical staff is generally constant, and the door opening is minimized.
- Body closingThe patient’s wound is closed by surgeons. ESTs usage is limited and mainly dedicated to cauterization of tissues and small vessels. The duration of this phase is usually short, although it may take hours in the case of orthopedic operations.
2.4. Ethics
3. Results and Discussion
4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mintz, Y.; Arezzo, A.; Boni, L.; Baldari, L.; Cassinotti, E.; Brodle, R.; Uranues, S.; Zheng, M.; Fingerhut, A. The risk of COVID-19 transmission by laparoscopic smoke may be lower than for laparotomy: A narrative review. Surg. Endosc. 2020, 34, 3298–3305. [Google Scholar] [CrossRef] [PubMed]
- Karuppal, R.; Surendran, S.; Patinharayil, G.; Fazil, V.; Marthy, A. It is time for a more cautious approach to surgical diathermy, especially in COVID-19 outbreak: A schematic review. J. Orthop. 2020, 20, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Thieves, M.; Hirsch, T.; Fischer, K.-D.; Hubert, H.; Beppler, S.; Seipp, H.-M. Reduction of airborne bacterial burden in the OR by installation of unidirectional displacement airflow (UDF) systems. Med. Sci. Monit. 2015, 21, 2367–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, T.; Hubert, H.; Fischer, S.; Lahmer, A.; Lehnhardt, M.; Steinau, H.; Steinstraesser, L.; Seipp, H. Bacterial burden in the operating room: Impact of airflow systems. Am. J. Infect. Control. 2012, 40, e228–e232. [Google Scholar] [CrossRef]
- Agodi, A.; Auxilia, F.; Barchitta, M.; Cristina, M.; D’Alessandro, D.; Mura, I.; Nobile, M.; Pasquarella, C. Operating theatre ventilation systems and microbial air contamination in total joint replacement surgery: Results of the GISIO-ISChIA study. J. Hosp. Infect. 2015, 90, 213–219. [Google Scholar] [CrossRef]
- Joppolo, C.M.; Romano, F. HVAC System Design in Healthcare Facilities and Control of Contaminants: Issues, Tools, and Experiments. In Indoor Air Quality in Healthcare Facilities; SpringerBriefs in Public Health; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Noguchi, C.; Koseki, H.; Horiuchi, H. Factors contributing to airborne particle dispersal in the operating room. BMC Surg. 2017, 17, 78. [Google Scholar] [CrossRef] [Green Version]
- Bhangar, S.; Adams, R.; Pasut, W.; Huffman, J. Chamber bioaerosol study: Human emissions of size-resolved fluorescent biological aerosol particles. Indoor Air 2016, 26, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Romano, F.; Milani, S.; Joppolo, C.M. Airborne particle and microbial human emission rate investigation for cleanroom clothing combinations. Build. Environ. 2020, 180. [Google Scholar] [CrossRef]
- Clark, R. Skin scales among airborne particles. J. Hyg. 1974, 72, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Noble, W.; Habbema, J.; Van Furth, T. Quantitative studies on the dispersal of skin bacteria into the air. J. Med. Microbiol. 1976, 13, 53–61. [Google Scholar] [CrossRef] [Green Version]
- You, R.; Cui, W.; Chen, C.; Zhao, B. Measuring the short-term emission rates of particles in the “personal cloud” with different clothes and activity intensities in a sealed chamber. Aerosol Air Qual. Res. 2013, 13, 911–921. [Google Scholar] [CrossRef]
- Pasquarella, C.; Sansebastiano, G.; Ferretti, S. A mobile laminar airflow unit to reduce air bacterial contamination at surgical area in a conventionally ventilated operating theatre. J. Hosp. Infect. 2007, 66, 313–319. [Google Scholar] [CrossRef]
- Licina, D.; Tian, Y.; Nazaroff, W. Emission rates and the personal cloud effect associated with particle release from the perihuman environment. Indoor Air 2017, 27, 791–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özkaynak, H.; Xue, J.; Spengler, J. Personal exposure to airborne particles and metals: Results from the Particle TEAM study in Riverside, California. J. Expo. Anal. Environ. Epidemiol. 1996, 6, 57–78. [Google Scholar]
- Miller, K.; Siscovick, D.; Sheppard, L.; Shepherd, K. Long-term exposure to air pollution and incidence of cardiovascular events in women. N. Eng. J. Med. 2007, 356, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Romano, F.; Gusten, J.; De Antonellis, S.; Joppolo, C.M. Electrosurgical smoke: Ultrafine particle measurements and work environment quality in different operating theatres. Int. J. Environ. Res. Public Health 2017, 14, 137. [Google Scholar] [CrossRef]
- Carbajo-Rodríguez, H.; Aguayo-Albasini, J.; Soria-Aledo, V.; García-López, C. Surgical smoke: Risks and preventive measures. Cir. Esp. 2009, 85, 274–279. [Google Scholar] [CrossRef]
- Lundblad, S.; Nilsson, L. Diathermy and airborne particles in operating rooms—An investigational measurement study about spreading of airborne particles and the variation of particle levels during operation. Master’s Thesis, Chalmers University of Technology, Gothenburg, Sweden, May 2013. [Google Scholar]
- Romano, F.; Gusten, J.; De Antonellis, S.; Joppolo, C.M. Air contamination control in Hybrid operating theatres. Particle content during different types of surgery with focus on diathermy. Proc. Indoor Air 2016, 998, 3–8. [Google Scholar]
- Ilce, A.; Yuzden, G.; Van Giersbergen, M. The examination of problems experienced by nurses and doctors associated with exposure to surgical smoke and the necessary precautions. J. Clin. Nurs. 2016, 26, 1555–1561. [Google Scholar] [CrossRef]
- Fan, J.; Chan, F.; Chu, K. Surgical smoke. Asian J. Surg. 2009, 32, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Schulz, H.; Harder, V.; Ibald-Mulli, A. Cardiovascular effects of fine and ultrafine particles. J. Aerosol Med. 2005, 18, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Buonanno, G.; Capuano, R.; Cortellessa, G.; Stabile, L. Airborne particle emission rates and doses received in operating rooms from surgical smoke. Build. Environ. 2019, 151, 168–174. [Google Scholar] [CrossRef]
- Nicola, J.; Nicola, E.; Viera, R. Speed of particles ejected from animal skin by CO2 laser pulse, measured by laser Doppler velocimetry. Phys. Med. Biol. 2002, 47, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Brandon, H.; Young, L. Characterization and removal of electrosurgical smoke. Surg. Serv. Manag. 1997, 3, 14–16. [Google Scholar]
- Alp, E.; Bijl, D.; Bleichrodt, R.; Hansson, B.; Voss, A. Surgical smoke and infection control. J. Hosp. Infect. 2006, 62, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Shi, B. Removal of ultrafine particles by intermediate air filters in ventilations systems, evaluation of performance and analysis of applications. Ph.D. Thesis, Chalmers University of Technology, Gothenburg, Sweden, June 2012. [Google Scholar]
- Okoshi, K.; Kobayashi, K.; Kinoshita, K. Health risks associated with exposure to surgical smoke for surgeons and operation room personnel. Surg. Today 2015, 45, 957–965. [Google Scholar] [CrossRef]
- Baggish, M.; Baltoyannis, P.; Sze, E. Protection of the rat lung from the harmful effects of laser smoke. Las. Surg. Med. 1998, 8, 248–253. [Google Scholar] [CrossRef]
- Capizzi, P.; Caly, R.; Battey, M. Microbiologic activity in laser resurfacing plume and debris. Lasers Surg. Med. 1998, 23, 172–174. [Google Scholar] [CrossRef]
- Garden, G.; O’Banion, K.; Bakus, A.; Olson, C. Viral disease transmitted by laser-generated plume (aerosol). Arch. Dermat. 2002, 138, 1303–1307. [Google Scholar] [CrossRef]
- Hollmann, R.; Hort, C.; Kammer, E.; Naegele, M.; Sigrist, M.; Meuli-Simmel, C. Smoke in the operating theater: As unregarded source of danger. Plast. Reconstr. Surg. 2004, 114, 458–463. [Google Scholar] [CrossRef]
- Hallmo, P.; Naess, O. Laryngeal papillomatosis with human papillomavirus DNA contracted by a laser surgeon. Eur. Arch. Otorhinolaryngol. 1991, 248, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Mowbray, N.; Ansell, J.; Horwood, J.; Cornish, J.; Rizkallah, P.; Parker, A.; Wall, P.; Spinelli, A.; Torkington, J. Safe management of surgical smoke in the age of COVID-19. Br. J. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brągoszewska, E. The dose of fungal aerosol inhaled by workers in a waste-sorting plant in Poland: A case study. Int. J. Environ. Res. Public Health 2020, 17, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brągoszewska, E.; Biedroń, I. Indoor Air Quality and Potential Health Risk Impacts of Exposure to Antibiotic Resistant Bacteria in an Office Rooms in Southern Poland. Int. J. Environ. Res. Public Health 2018, 15, 2604. [Google Scholar] [CrossRef] [Green Version]
- Moustafa, M. Exposure Dose of Bacteria and Fungi in a Public Primary School in Beni Suef, Upper Egypt. J. Adv. Biol. 2019, 12, 2331–2340. [Google Scholar] [CrossRef]
- Sohaili, J.; Muniyansi, S.K.; Mohamad, R. Dose Response and Exposure Assessment of Household Hazardous Waste in Household Hazardous Waste Management; IntechOpen Limited: London, UK, 2017. [Google Scholar]
- Tan, W.; Zhu, H.; Zhang, N.; Dong, D.; Wang, S.; Ren, F.; Xiang, J.; Wu, R.; Lv, Y. Characterization of the PM2.5 concentration in surgical smoke in different tissues during hemihepatectomy and protective measures. Environ. Toxicol. Pharmacol. 2019, 72, 103248. [Google Scholar] [CrossRef]
- Mohamed, S.; Buonanno, G.; Massarotti, N.; Mauro, A. Ultrafine particle transport inside an operating equipped with turbulent diffusers. J. Build. Perform. Simul. 2020, 13, 443–455. [Google Scholar] [CrossRef]
- Occupational Safety and Health Administration (OSHA). Laser/Electrosurgery Plume; OSHA: Washington, DC, USA, 2016. Available online: https://www.osha.gov/SLTC/etools/hospital/surgical/surgical.html (accessed on 12 December 2016).
- National Institute for Occupational Safety and Health (NIOSH). Control of Smoke from Laser/Electric Surgical Procedures; NIOSH Pub. No. 96–128; NIOSH: Atlanta, GA, USA, 2016. Available online: http://www.cdc.gov/niosh/docs/hazardcontrol/hc11.html (accessed on 11 December 2016).
- Association of periOperative Registered Nurses (AORN). Recommended practices for laser safety in perioperative practice settings. In Standards, Recommended Practices, and Guidelines; AORN Inc.: Denver, CO, USA, 2014; pp. 141–154. [Google Scholar]
- Association of Surgical Technologists (AST). AST Standards of Practice for Use of Electrosurgery; AST: Littleton, CO, USA, 2016; Available online: http://www.ast.org/uploadedFiles/Main_Site/Content/About_Us/Standard%20Electrosurgery.pdf (accessed on 11 December 2016).
- American National Standard Institute (ANSI). American National Standard for Safe Use of Lasers in Health Care Facilities; ANSI: Washington, DC, USA, Z136.3-2005; Available online: https://webstore.ansi.org/Standards/LIA/ANSIZ1362018 (accessed on 27 June 2014).
- Liu, N.; Filipp, N.; Wood, K. The utility of local smoke evacuation in reducing surgical smoke exposure in spine surgery: A prospective self-controlled study. Spine J. 2020, 20, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Arli, S. Knowledge of the Operating Room Team Members about Surgical Smoke Safety. Int. J. Caring Sci. 2020, 13, 489–497. [Google Scholar]
- Hensman, C.; Baty, D.; Willis, R.; Cuschieri, A. Chemical composition of smoke produced by high-frequency electrosurgery in a closed gaseous environment: An in vitro study. Surg. Endosc. 1998, 12, 1017–1019. [Google Scholar] [CrossRef]
- Breier, A.; Brandt, C.; Sohr, D. Laminar airflow ceiling size: No impact on infection rates following hip and knee prosthesis. Infect. Control. Hosp. Epidemiol. 2011, 321, 1097. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, A.; Kothari, A.; Bannister, G. Investigating bacterial growth in surgical theatres: Establishing the effect of laminar airflow on bacterial growth on plastic, metal and wood surfaces. Ann. R. Coll. Surg. Engl. 2008, 90, 417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gastmeier, P.; Breier, A.; Brandt, C. Influence of laminar airflow on prosthetic joint infections: A systematic review. J. Hosp. Infect. 2012, 81, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, P.; Kubilay, N.Z.; Allegranzi, B.; Egger, M.; Gastmeier, P. Effect of laminar airflow ventilation on surgical site infections: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 553–561. [Google Scholar] [CrossRef]
- Van Gestel, E.; Linssen, E.; Creta, M.; Poels, K.; Godderis, L.; Weyler, J.; De Schryver, A.; Vanoirbeek, J. Assessment of the absorbed dose after exposure to surgical smoke in an operating room. Toxicol. Lett. 2020, 328, 45–51. [Google Scholar] [CrossRef]
- Meda, D. Air Contamination Control in Hybrid OTs. Particle Content during Different Types of Surgery with Focus on Diathermy. Master’s Thesis, Politecnico di Milano, Milano, Italy, March 2014. [Google Scholar]
- ISO 27891. Aerosol Particle Number Concentration—Calibration of Condensation Particle Counters; International Organizazion for Standardization: Genewa, Switzerland, 2015. [Google Scholar]
- Montagna, M.T.; Rutigliano, S.; Trerotoli, P.; Napoli, C.; Apollonio, F.; D’Amico, A.; De Giglio, O.; Diella, G.; Lopuzzo, M.; Marzella, A.; et al. Evaluation of air contamination in Orthopaedic Operating Theatres in hospitals in Southern Italy: The IMPACT project. Int. J. Environ. Res. Public Health 2019, 16, 3581. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OT | Ventilation System | Area | Volume | Supply Airflow Rate | ACH | Surgical Lamps | Terminal Filters |
|---|---|---|---|---|---|---|---|
| (m2) | (m3) | (m3/h) | (h−1) | (#) | (-) | ||
| OT1 | UWD | 36 | 108 | 2.016 | 19 | 2 | H14 (UWD) |
| OT2 | UDAF+Mixing | 100 | 270 | 15.480 | 57 | 2 | U15 (UDAF)+ H14 (Mixing) |
| Test Parameters | ||||||
|---|---|---|---|---|---|---|
| OT | OT1 | OT1 | OT2 | OT2 | OT2 | OT2 |
| Surgical Operation Type | Neurological | Orthopedic | EVAR | Liver Resection | Orthopedic | Cancer Removal |
| Number of Surgeries Monitored | 1 | 3 | 4 | 1 | 3 | 1 |
| Total Hours Recorded (h) | 6 | 7 | 22 | 6 | 16 | 4 |
| Mean Number of Personnel * | 8 | 6 | 8 | 9 | 6 | 10 |
| Door Open Frequency * (1/min) | 0.17 | 0.24 | 0.36 | 0.32 | 0.24 | 0.17 |
| Results | ||||||
| UFP 0,02–1 µm * (pp/cm3) (min; max) | 1.52 (0; 34) | 940.1 (0; 9258) | 0.16 (0; 65) | 18.7 (0; 2392) | 18.1 (0; 5280) | 0.68 (0; 28) |
| CFU * (CFU/m3) (min; max) | 23 (10; 34) | 27 (6; 48) | 0.4 (0; 1) | 0.1 (0; 2) | 0.7 (0; 2) | 0 (0; 0) |
| Operation Phase | OT1 | OT2 |
|---|---|---|
| Preparation | 6 | 6 |
| Body opening | 7 | 10 |
| Surgery | 7 | 8 |
| Body closure | 6 | 6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, F.; Milani, S.; Gustén, J.; Joppolo, C.M. Surgical Smoke and Airborne Microbial Contamination in Operating Theatres: Influence of Ventilation and Surgical Phases. Int. J. Environ. Res. Public Health 2020, 17, 5395. https://doi.org/10.3390/ijerph17155395
Romano F, Milani S, Gustén J, Joppolo CM. Surgical Smoke and Airborne Microbial Contamination in Operating Theatres: Influence of Ventilation and Surgical Phases. International Journal of Environmental Research and Public Health. 2020; 17(15):5395. https://doi.org/10.3390/ijerph17155395
Chicago/Turabian StyleRomano, Francesco, Samanta Milani, Jan Gustén, and Cesare Maria Joppolo. 2020. "Surgical Smoke and Airborne Microbial Contamination in Operating Theatres: Influence of Ventilation and Surgical Phases" International Journal of Environmental Research and Public Health 17, no. 15: 5395. https://doi.org/10.3390/ijerph17155395
APA StyleRomano, F., Milani, S., Gustén, J., & Joppolo, C. M. (2020). Surgical Smoke and Airborne Microbial Contamination in Operating Theatres: Influence of Ventilation and Surgical Phases. International Journal of Environmental Research and Public Health, 17(15), 5395. https://doi.org/10.3390/ijerph17155395