Source of Social Support and Caregiving Self-Efficacy on Caregiver Burden and Patient’s Quality of Life: A Path Analysis on Patients with Palliative Care Needs and Their Caregivers

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sample and Participants
2.2. Procedure
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
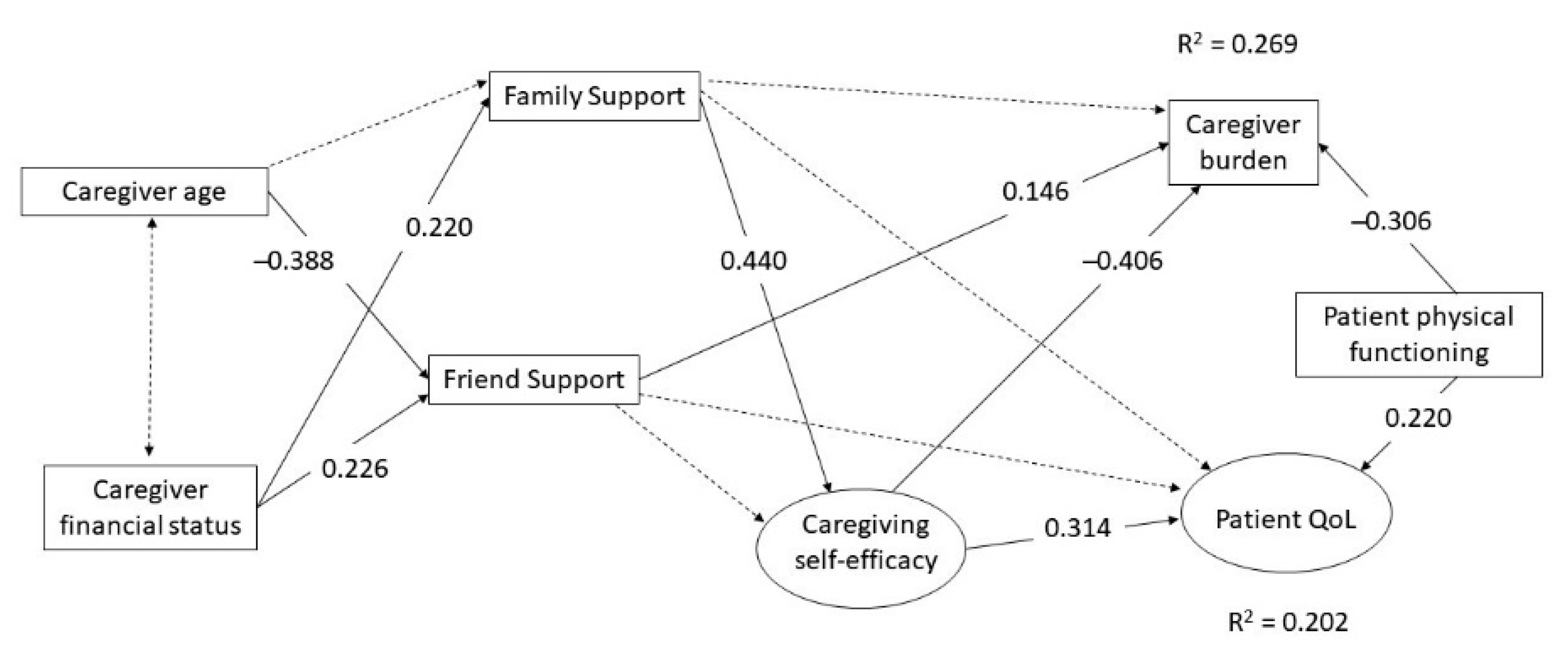
3.2. Path Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Definition of Palliative Care. Available online: https://www.who.int/cancer/palliative/definition/en/ (accessed on 21 May 2020).
- Hall, S.; Petkova, H.; Tsouros, A.D.; Costantini, M.; Higginson, I.J. Palliative Care for Older People: Better Practices. World Health Organization, 2011. Available online: https://www.euro.who.int/en/publications/abstracts/palliative-care-for-older-people-better-practices (accessed on 11 July 2020).
- World Health Organization. Palliative Care. Available online: https://www.who.int/en/news-room/fact-sheets/detail/palliative-care (accessed on 21 May 2020).
- Delalibera, M.; Presa, J.; Barbosa, A.; Leal, I. Burden of caregiving and its repercussions on caregivers of end-of-life patients: A systematic review of the literature. Ciência Saúde Coletiva 2015, 20, 2731–2747. [Google Scholar] [CrossRef] [Green Version]
- Carreetero, S.; Garcés, J.; Ródenas, F.; Sanjosé, V. The informal caregiver’s burden of dependent people: Theory and empirical review. Arch. Gerontol. Geriatr. 2009, 49, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.; Pallant, J.; Brand, C. Caregiver strain and factors associated with caregiver self-efficacy and quality of life in a community cohort with multiple sclerisos. Disabil. Rehabil. 2007, 29, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Milbury, K.; Badr, H.; Fossella, F.; Pisters, K.M.; Carmack, C.L. Longitudinal associations between caregiver burden and patient and spouse distress in couples coping with lung cancer. Support. Care Cancer 2013, 21, 2371–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angiola, J.E.; Bowen, A.M. Quality of life in advanced cancer: An acceptance and commitment therapy view. Couns. Psychol. 2013, 41, 313–335. [Google Scholar] [CrossRef]
- Kramer, B.J. Gain in the caregiving experience: Where are we? What next? Gerontologist 1997, 37, 218–232. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.-T.; Lam, L.C.W.; Kwok, T.; Ng, N.S.S.; Fung, A.W.T. Self-efficacy is associated with less burden and more gains from behavioral problems of Alzheimer’s disease in Hong Kong Chinese caregivers. Gerontologist 2013, 53, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Durmaz, H.; Okanli, A. Investigation of the effect of self-efficacy levels of caregiver family members of the individuals with schizophrenia on burden of care. Arch. Psychiat. Nurs. 2014, 28, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Mystakidou, K.; Parpa, E.; Panagiotou, I.; Tsilika, E.; Galanos, A.; Gouliamos, A. Caregivers’ anxiety and self-efficacy in palliative care. Eur. J. Cancer Care. 2013, 22, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Semiatin, A.M.; O’Connor, M.K. The relationship between self-efficacy and positive aspects of caregiving in Alzheimer’s disease caregivers. Aging Ment. Health 2012, 16, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Ugalde, A.; Krishnasamy, M.; Schofield, P. The relationship between self-efficacy and anxiety and general distress in caregivers of people with advanced cancer. J. Palliat. Med. 2014, 17, 939–941. [Google Scholar] [CrossRef] [PubMed]
- Unver, V.; Basak, T.; Tosun, N.; Aslan, O.; Akbayrak, N. Care burden and self-efficacy levels of family caregivers of elderly people in Turkey. Holist. Nurs. Pract. 2016, 30, 166–173. [Google Scholar] [CrossRef]
- Keefe, F.J.; Ahles, T.A.; Porter, L.S.; Sutton, L.M.; McBride, C.M.; Pope, M.S.; McKinstry, E.T.; Furstenberg, C.P.; Dalton, J.; Baucom, D.H. The self-efficacy of family caregivers for helping cancer patients manage pain at end-of-life. Pain 2003, 103, 157–162. [Google Scholar] [CrossRef]
- Thielemann, P.A.; Conner, N.E. Social support as a mediator of depression in caregivers of patients with end-stage disease. J. Hosp. Palliat. Nurs. 2009, 11, 82–90. [Google Scholar] [CrossRef]
- Del-Pino-Casado, R.; Frías-Osuna, A.; Palomino-Moral, P.A.; Ruzafa-Martínez, M.; Ramos-Morcillo, A.J. Social support and subjective burden in caregivers of adults and older adults: A meta-analysis. PLoS ONE 2018, 13, e0189874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drentea, P.; Clay, O.J.; Roth, D.L.; Mittelman, M.S. Predictors of improvement in social support: Five year effects of a structured intervention for caregivers of spouses with Alzheimer’s disease. Soc. Sci. Med. 2006, 63, 957–967. [Google Scholar] [CrossRef]
- Au, A.; Lai, M.K.; Lau, K.M.; Pan, P.C.; Lam, L.; Thompson, L.; Gallagher-Thompson, D. Social support and well-being in dementia family caregivers: The mediating role of self-efficacy. Aging Ment. Health 2009, 13, 761–768. [Google Scholar] [CrossRef]
- Zhang, S.; Edwards, H.; Yates, P.; Li, C.; Guo, Q. Self-efficacy partially mediates between social support and health-related quality of life in family caregivers for dementia patients in Shanghai. Dement. Geriatr. Cogn. Disord. 2014, 37, 34–44. [Google Scholar] [CrossRef]
- Tang, F.; Jang, H.; Lingler, J.; Tamres, L.K.; Erlen, J.A. Stressors and caregivers’ depression: Multiple mediators of self-efficacy, social support, and problem-solving skill. Soc. Work Health Care 2015, 54, 651–668. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.-Y.; Huang, L.-H. The relationship between family functioning and caregiver appraisal of dementia family caregivers: Caregiving self-efficacy as a mediator. Aging Ment. Health 2018, 22, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Tian, Y.; Fan, Y.; Liu, L.; Luo, Y.; Zhou, L.; Yu, H. The mediating roles of caregiver social support and self-efficacy on caregiver burden in Parkinson’s disease. J. Affect. Disord. 2019, 256, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Thoits, P.A. Conceptual, methodological, and theoretical problems in studying social support as a buffer against life stress. J. Health Soc. Behav. 1982, 23, 145–159. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.T.; Lam, L.C.W.; Kwok, T.; Ng, N.S.S.; Fung, W.T. The social networks of Hong Kong Chinese family caregivers of Alzheimer’s disease: Correlates with positive gains and burden. Gerontologist 2013, 53, 998–1008. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, T. Benefit finding through caring: The cancer caregiver experience. Psychol. Health 2013, 28, 250–266. [Google Scholar] [CrossRef]
- Kahriman, F.; Zaybak, A. Caregiver burden and perceived social support among caregivers of patients with cancer. Asian Pac. J. Cancer Prev. 2015, 16, 3313–3317. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Liu, Y.; Zhang, X.; Tam, W.; Mao, J.; Lopez, V. Chinese family caregivers of stroke survivors: Determinants of caregiving burden within the first six months. J. Clin. Nurs. 2017, 26, 4558–4566. [Google Scholar] [CrossRef]
- Ryan, S.; Wong, J.; Chow, R.; Zimmermann, C. Evolving definitions of palliative care: Upstream migration or confusion? Curr. Treat. Options Oncol. 2020, 21, 20. [Google Scholar] [CrossRef]
- Gómez-Batiste, X.; Martínez-Muñoz, M.; Blay, C.; Amblàs, J.; Costa, X.; Espaulella, J.; Espinosa, J.; Figuerola, M.; Esperalba, J. Identifying patients with chronic conditions in need of palliative care in the general population: Development of the NECPAL tool and preliminary prevalence rates in Catalonia. BMJ Support. Palliat. Care 2013, 3, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Lo, R.S.K.; Woo, J.; Zhoc, K.C.H.; Li, C.Y.P.; Yeo, W.; Johnson, P.; Mak, Y.; Lee, J. Cross-cultural validation of the McGill Quality of Life Questionnaire in Hong Kong Chinese. Palliat. Med. 2001, 15, 387–397. [Google Scholar] [CrossRef]
- Leung, S.O.C.; Chan, C.C.H.; Shah, S. Development of a Chinese version of the Modified Barthel Index—Validity and reliability. Clinical. Rehab. 2007, 21, 912–922. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B. Validation of a Caregiver Strain Index. J. Gerontol. 1983, 38, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.C.H.; Chan, C.L.F.; Suen, M. Validation of the Chinese Version of the Modified Caregivers Strain Index among Hong Kong Caregivers: An Initiative of Medical Social Workers. Health Soc. Work 2013, 38, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.P.; Chan, H.Y.L.; Chan, C.W.H.; Kwan, J.S.K.; Yau, S.Z.M.; Chiu, P.K.C.; Lo, R.S.K.; Lee, L.L.Y. Psychometric properties of the Caregiver Inventory for measuring caregiving self-efficacy of caregivers of patients with palliative care needs. Neuropsychiatry 2017, 7, 872–879. [Google Scholar]
- Merluzzi, T.V.; Philip, E.J.; Vachon, D.O.; Heitzmann, C.A. Assessment of self-efficacy for caregiving: The critical role of self-care in caregiver stress and burden. Palliat. Support. Care 2011, 9, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.L. Assessing Chinese adolescents’ social support: The multidimensional scale of perceived social support. Personal. Individ. Differ. 2000, 28, 299–307. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J. Educ. Res. 2006, 99, 323–337. [Google Scholar] [CrossRef]
- Soper, D.S. A-Priori Sample Size Calculator for Structural Equation Models [Software]. Available online: http://www.danielsoper.com/statcalc (accessed on 21 May 2020).
- Bentler, P.M. EQS Structural Equations Program. Manual; Multivariate Software Inc.: Encino, CA, USA, 2006. [Google Scholar]
- Satorra, A.; Benlter, P.M. Corrections to test statistics and standard errors in covariance structure analysis. In Latent Variables Analysis: Applications for Developmental Research; Von Eye, A., Clogg, C.C., Eds.; Sage: Thousand Oaks, CA, USA, 1994; pp. 399–419. [Google Scholar]
- Hoyle, R.H. The structural equation modeling approach: Basic concepts and fundamental issues. In Structural Equation Modeling: Concepts, Issues, and Applications, 1st ed.; Hoyle, R.H., Ed.; Sage Inc.: Thousand Oaks, CA, USA, 1995; pp. 1–15. ISBN 13 978-0803953185. [Google Scholar]
- Gellis, Z.D. Kin and nonkin social supports in a community sample of Vietnamese immigrants. Soc. Work 2003, 48, 248–258. [Google Scholar] [CrossRef]
- Leung, A.K.Y.; Cohen, D. Within- and between-cultural variation: Individual differences and the cultural logics of honor, face and dignity cultures. J. Personal. Soc. Psychol. 2011, 100, 507–526. [Google Scholar] [CrossRef]
- Mortenson, S.; Lui, M.; Burleson, B.R.; Lui, Y. A fluency of feeling: Exploring cultural and individual differences (and similarities) related to skilled emotional support. J. Cross Cult. Psychol. 2006, 37, 366–384. [Google Scholar] [CrossRef]
- Brannan, D.; Biswas-Diener, R.; Mohr, C.D.; Mortazavi, S.; Stein, N. Friends and family: A cross-cultural investigation of social support and subjective well-being among college students. J. Posit. Psychol. 2013, 8, 65–75. [Google Scholar] [CrossRef]
- Megar, K. Quality of life in chronic disease patients. Health Psychol. Res. 2013, 1, e27. [Google Scholar] [CrossRef]
- Carbonneau, H.; Caron, C.; Desrosiers, J. Development of a conceptual framework of positive aspects of caregiving in dementia. Dementia 2010, 9, 327–353. [Google Scholar] [CrossRef]
- Bonin-Guillaume, S.; Durand, A.C.; Yahi, F.; Curiel-Berruyer, M.; Lacroix, O.; Cretel, E.; Alazia, M.; Sambuc, R.; Gentile, S. Predictive factors for early unplanned rehospitalization of older adults after an ED visit: Role of the caregiver burden. Aging Clin. Exp. Res. 2015, 27, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Ejem, D.B.; Drentea, P.; Clay, O.J. The effects of caregiver emotional stress on the depressive symptomatology of the care recipient. Aging Ment. Health 2015, 19, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Jones, P.S.; Winslow, B.W. The relationship between mutuality, filial piety, and depression in family caregivers in China. J. Transcult. Nurs. 2017, 28, 455–463. [Google Scholar] [CrossRef]
- Burke, T.; Galvin, M.; Pinto-Grau, M.; Lonergan, K.; Madden, C.; Mays, I.; Carney, S.; Hardiman, O.; Pender, N. Caregivers of patients with amyotrophic lateral sclerosis: Investigating quality of life, caregiver burden, service engagement, and patient survival. J. Neurol. 2017, 264, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.Y.L.; Yu, D.S.F.; Leung, D.Y.P.; Chan, A.W.K.; Hui, E. Quality of life and palliative care needs of elderly patients with advanced heart failure. J. Geriatr. Cardiol. 2016, 13, 420–424. [Google Scholar] [PubMed]
- Ge, L.; Mordiffi, S.Z. Factors associated with higher caregiver burden among family caregivers of elderly cancer patients: A systematic review. Cancer Nurs. 2017, 40, 471–478. [Google Scholar] [CrossRef]
- Cramarossa, G.; Chow, E.; Zhang, L.; Bedard, G.; Zeng, L.; Sahgal, A.; Vassiliou, V.; Satoh, T.; Foro, P.; Ma, B.B.; et al. Predictive factors for overall quality of life in patients with advanced cancer. Support. Care Cancer 2013, 21, 1709–1716. [Google Scholar] [CrossRef]
- Vahidi, M.; Mahdavi, N.; Asghari, E.; Ebrahimi, H.; Eivazi Ziaei, J.; Hosseinzadeh, M.; Namdar Areshtanab, H.; Kermani, I.A. Other side of breast cancer: Factors associated with caregiver burden. Asian Nurs. Res. 2016, 10, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, A.; Mirhosseini, S.; Basirinezhad, M.H.; Ebrahimi, H. Relationship between caring burden and quality of life in caregivers of cancer patients in Iran. Support. Care Cancer 2019, 24, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Liu, C.; Baladon, L.; Rubio-Valera, M. Multidimensional determinants of the caregiving burden among Chinese male caregivers of older family members in Hong Kong. Aging Ment. Health 2018, 22, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Casado-Mejia, R.; Ruiz-Arias, E. Influence of gender and care strategy in family caregivers strain: A cross-sectional study. J. Nurs. Scholarsh. 2016, 48, 587–597. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Patients | Caregivers |
|---|---|---|
| Age, Mean ± SD | 76.8 ± 10.4 | 57.1 ± 14.6 |
| Male, n (%) | 91 (40.4%) | 79 (35.1%) |
| Married/Cohabitation, n (%) | 138 (61.3%) | 187 (83.1%) |
| Educational level, n (%) | ||
| No formal education | 95 (42.2%) | 20 (8.9%) |
| Primary education | 72 (32.0%) | 50 (22.2%) |
| Secondary education or above | 56 (24.8%) | 154 (68.4%) |
| Missing | 2 (0.9%) | 1 (0.4%) |
| Perceived financial status, n (%) | ||
| Completely not enough | 14 (6.2%) | 19 (8.4%) |
| Not enough | 45 (20.0%) | 39 (17.3%) |
| Neutral | 119 (52.9%) | 138 (61.3%) |
| Enough | 34 (15.1%) | 22 (9.8%) |
| Completely enough | 10 (4.4%) | 7 (3.1%) |
| Missing | 3 (1.3%) | |
| Receiving regular outpatient palliative care at hospital | 62 (27.6%) | |
| Leading class of diagnosis, n (%) | ||
| Diabetes | 40 (17.8%) | |
| Heart diseases | 115 (51.1%) | |
| Neurological diseases | 6 (2.7%) | |
| Kidney diseases | 7 (3.1%) | |
| Cancer | 43 (19.1%) | |
| Lung diseases | 11 (4.9%) | |
| Bone diseases | 3 (1.3%) | |
| MBI, Mean ± SD | 85.3 ± 19.5 | |
| MMSE, Mean ± SD | 22.1 ± 5.2 | |
| Relationship with the patient, n (%) | ||
| Child | 116 (51.6%) | |
| Spouse | 83 (36.9%) | |
| Others | 26 (11.6%) | |
| Perceived health status, Mean ± SD | 3.28 ± 0.97 | |
| Has a domestic helper, n (%) | 57 (25.3%) |
| Participants | Variable | Possible Range | Mean ± SD | Median (Min, Max) |
|---|---|---|---|---|
| Caregivers | Caregiver burden | 0–13 | 5.81 ± 3.8 | 6.0 (0, 13) |
| Caregiving self-efficacy | ||||
| Care of the care recipient | 1–9 | 7.08 ± 1.37 | 7.1 (1.4, 9) | |
| Managing information and self-care | 1–9 | 6.37 ± 1.51 | 6.4 (1, 9) | |
| Managing emotional interaction with care Recipient | 1–9 | 6.46 ± 1.71 | 6.5 (1, 9) | |
| Family Support | 1–7 | 5.11 ± 1.16 | 5.3 (1.3, 7) | |
| Friend Support | 1–7 | 4.09 ± 1.33 | 4.3 (1, 7) | |
| Patients | Physical functioning | 0–100 | 84.93 ± 19.71 | 92.0 (0, 100) |
| Quality of life | ||||
| Physical | 0–10 | 5.21 ± 1.83 | 5.0 (1.3, 10) | |
| Psychological | 0–10 | 7.96 ± 2.16 | 8.7 (1, 10) | |
| Existence | 0–10 | 6.24 ± 2.01 | 6.3 (0, 10) | |
| Support | 0–10 | 7.08 ± 1.87 | 7.0 (0, 10) | |
| Sex | 0–10 | 8.40 ± 3.00 | 10.0 (0,10) |
| Path | Direct Effect | Indirect Effect | Total Effect |
|---|---|---|---|
| To caregiver burden | |||
| Family support | - | −0.162 * | −0.162 * |
| Friend support | 0.166 * | - | 0.166 * |
| Caregiving self-efficacy | −0.406 * | - | −0.406 * |
| Caregiver’s age | - | −0.064 * | −0.054 |
| Caregiver’s financial status | - | 0.002 | −0.007 |
| Patient’s physical functioning | −0.306 * | - | −0.306 * |
| To patient’s quality of life | |||
| Family support | - | 0.158 * | 0.158 * |
| Friend support | - | - | - |
| Caregiving self-efficacy | 0.314 * | 0.314 * | 0.314 * |
| Caregiver’s age | - | - | - |
| Caregiver’s financial status | - | 0.035 | 0.071 |
| Patient’s physical functioning | 0.220 * | - | 0.220 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, D.Y.P.; Chan, H.Y.L.; Chiu, P.K.C.; Lo, R.S.K.; Lee, L.L.Y. Source of Social Support and Caregiving Self-Efficacy on Caregiver Burden and Patient’s Quality of Life: A Path Analysis on Patients with Palliative Care Needs and Their Caregivers. Int. J. Environ. Res. Public Health 2020, 17, 5457. https://doi.org/10.3390/ijerph17155457
Leung DYP, Chan HYL, Chiu PKC, Lo RSK, Lee LLY. Source of Social Support and Caregiving Self-Efficacy on Caregiver Burden and Patient’s Quality of Life: A Path Analysis on Patients with Palliative Care Needs and Their Caregivers. International Journal of Environmental Research and Public Health. 2020; 17(15):5457. https://doi.org/10.3390/ijerph17155457
Chicago/Turabian StyleLeung, Doris Y. P., Helen Y. L. Chan, Patrick K. C. Chiu, Raymond S. K. Lo, and Larry L. Y. Lee. 2020. "Source of Social Support and Caregiving Self-Efficacy on Caregiver Burden and Patient’s Quality of Life: A Path Analysis on Patients with Palliative Care Needs and Their Caregivers" International Journal of Environmental Research and Public Health 17, no. 15: 5457. https://doi.org/10.3390/ijerph17155457
APA StyleLeung, D. Y. P., Chan, H. Y. L., Chiu, P. K. C., Lo, R. S. K., & Lee, L. L. Y. (2020). Source of Social Support and Caregiving Self-Efficacy on Caregiver Burden and Patient’s Quality of Life: A Path Analysis on Patients with Palliative Care Needs and Their Caregivers. International Journal of Environmental Research and Public Health, 17(15), 5457. https://doi.org/10.3390/ijerph17155457