Determination of Urinary Cotinine Cut-Off Concentrations for Pregnant Women in the Japan Environment and Children’s Study (JECS)


 , ,
, ,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Sample Collection
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Method Performance
3.2. Concentrations of Cotinine in Maternal Urine Samples
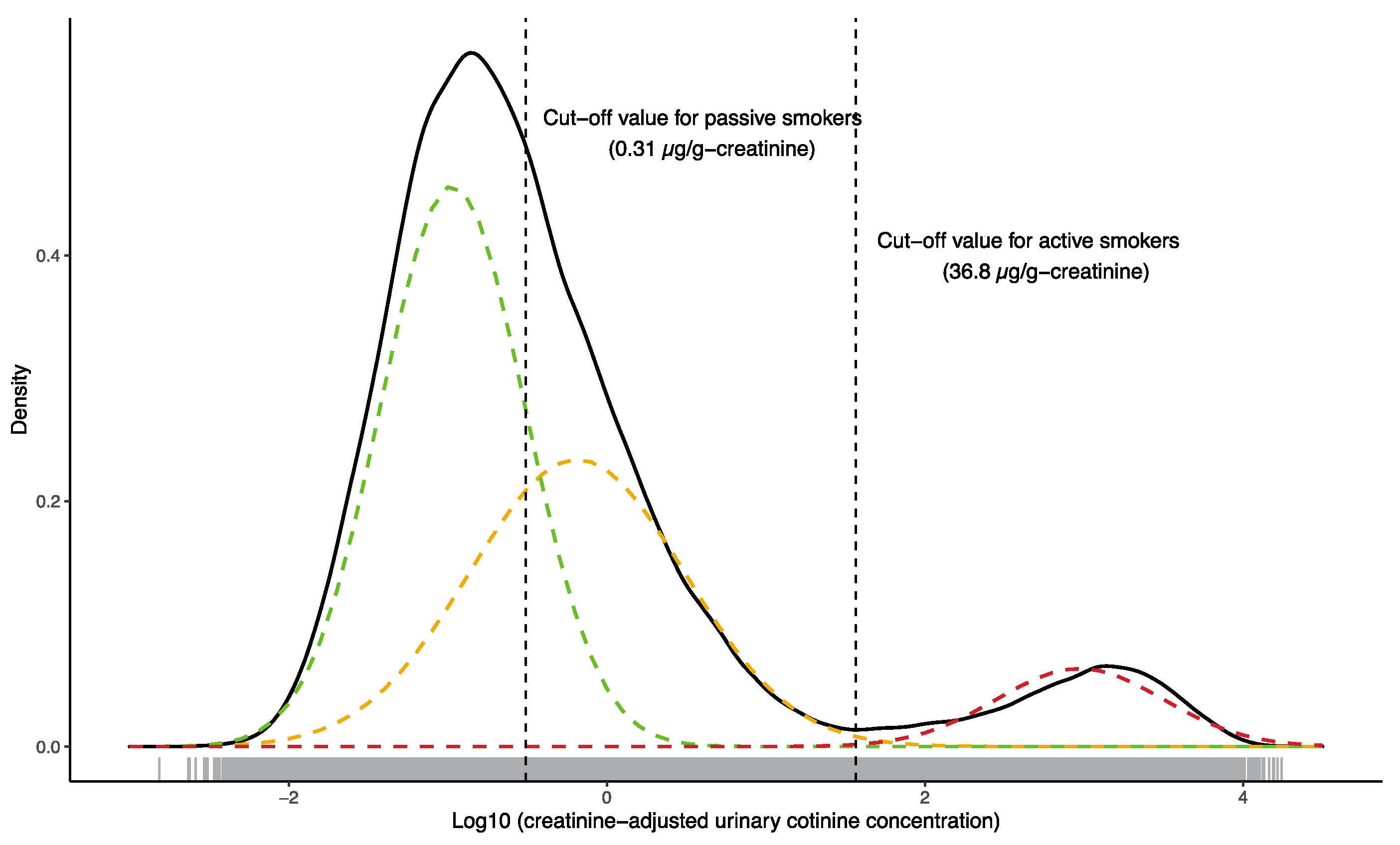
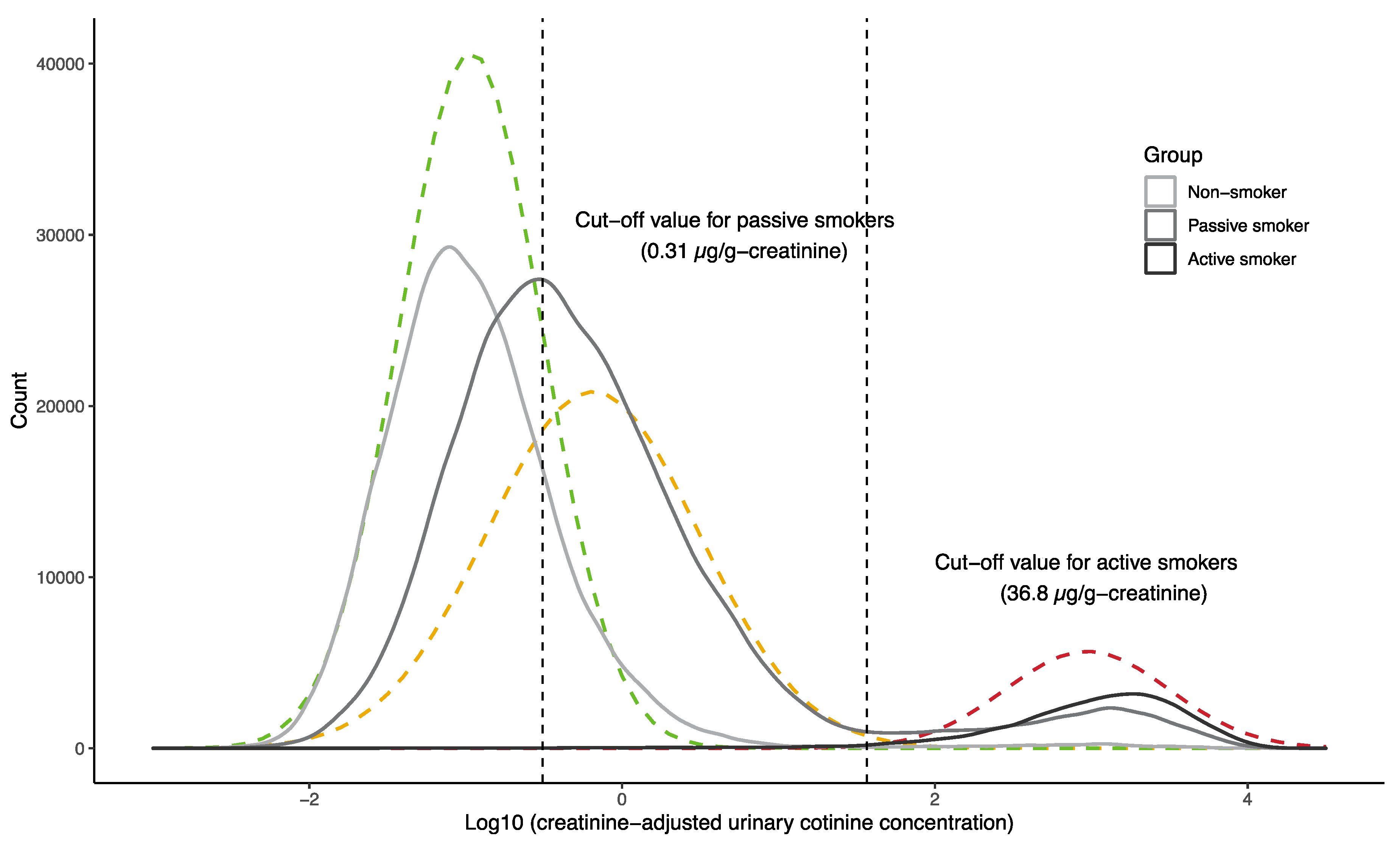
3.3. Cotinine Cut-Off Concentration for Active Smoking
3.4. Cotinine Cut-Off Concentration for Passive Smoking
4. Discussion
4.1. Urinary Cotinine Concentrations
4.2. Urinary Cotinine Cut-Off Concentrations
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Urinary Cotinine Analysis Method
Appendix A.1. Chemicals and Reagents
Appendix A.2. Sample Preparation
Appendix A.3. Instrument Analysis and Calculations
Appendix A.4. Quality Control
References
- Kerry, J.; Mathews, K.A.; O’Conor, M. Smoking in pregnancy: Effects on mother and fetus. BJOG An Int. J. Obstet. Gynaecol. 1984, 91, 111–117. [Google Scholar] [CrossRef]
- Law, K.L.; Stroud, L.R.; LaGasse, L.L.; Niaura, R.; Liu, J.; Lester, B.M. Smoking during pregnancy and newborn neurobehavior. Pediatrics 2003, 111, 1318–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonardi-Bee, J.; Smyth, A.; Britton, J.; Coleman, T. Environmental tobacco smoke and fetal health: Systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2008, 93, F351–F361. [Google Scholar] [CrossRef] [PubMed]
- Pietinalho, A.; Pelkonen, A.; Rytilä, P. Linkage between smoking and asthma. Allergy Eur. J. Allergy Clin. Immunol. 2009, 64, 1722–1727. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.M.; Golding, J.; Emond, A.M. Adverse effects of maternal lead levels on birth outcomes in the ALSPAC study: A prospective birth cohort study. BJOG An Int. J. Obstet. Gynaecol. 2015, 122, 322–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buteau, S.; Doucet, M.; Tétreault, L.F.; Gamache, P.; Fournier, M.; Brand, A.; Kosatsky, T.; Smargiassi, A. A population-based birth cohort study of the association between childhood-onset asthma and exposure to industrial air pollutant emissions. Environ. Int. 2018, 121, 23–30. [Google Scholar] [CrossRef]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Michikawa, T.; Nitta, H.; Nakayama, S.F.; Yamazaki, S.; Isobe, T.; Tamura, K.; Suda, E.; Ono, M.; Yonemoto, J.; Iwai-Shimada, M.; et al. Baseline profile of participants in the Japan environment and children’s study (JECS). J. Epidemiol. 2018, 28, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, N.; Takimoto, H.; Imai, S.; Miyachi, M.; Nishi, N. Data Resource Profile: The Japan National Health and Nutrition Survey (NHNS). Int. J. Epidemiol. 2015, 44, 1842–1849. [Google Scholar] [CrossRef]
- Suzuki, K.; Shinohara, R.; Sato, M.; Otawa, S.; Yamagata, Z. Association Between Maternal Smoking During Pregnancy and Birth Weight: An Appropriately Adjusted Model From the Japan Environment and Children’s Study. J. Epidemiol. 2016, 26, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Drake, P.; Driscoll, A.K.; Mathews, T.J. Cigarette Smoking During Pregnancy: United States, 2016 Key findings Data from the National Vital Statistics System. Available online: https://www.cdc.gov/nchs/data/databriefs/db305_table.pdf#1 (accessed on 12 February 2020).
- Perera, F.P.; Rauh, V.; Whyatt, R.M.; Tang, D.; Tsai, W.Y.; Bernert, J.T.; Tu, Y.H.; Andrews, H.; Barr, D.B.; Camann, D.E.; et al. A summary of recent findings on birth outcomes and developmental effects of prenatal ETS, PAH, and pesticide exposures. Neurotoxicology 2005, 26, 573–587. [Google Scholar] [CrossRef]
- Kim, S. Overview of cotinine cutoff values for smoking status classification. Int. J. Environ. Res. Public Health 2016, 13, 1236. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Braimoh, T.S.; Yila, T.A.; Yoshioka, E.; Kishi, R. Self-reported tobacco smoke exposure and plasma cotinine levels during pregnancy—A validation study in Northern Japan. Sci. Total Environ. 2011, 412–413, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Aurrekoetxea, J.J.; Murcia, M.; Rebagliato, M.; López, M.J.; Castilla, A.M.; Santa-Marina, L.; Guxens, M.; Fernández-Somoano, A.; Espada, M.; Lertxundi, A.; et al. Determinants of self-reported smoking and misclassification during pregnancy, and analysis of optimal cut-off points for urinary cotinine: A cross-sectional study. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupsa, I.R.; Nunes, B.; Ligocka, D.; Elena Gurzau, A.; Jakubowski, M.; Casteleyn, L.; Aerts, D.; Biot, P.; Den Hond, E.; Castaño, A.; et al. Urinary cotinine levels and environmental tobacco smoke in mothers and children of Romania, Portugal and Poland within the European human biomonitoring pilot study. Environ. Res. 2015, 141, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Stragierowicz, J.; Mikołajewska, K.; Zawadzka-Stolarz, M.; Polańska, K.; Ligocka, D. Estimation of cutoff values of cotinine in urine and saliva for pregnant women in Poland. Biomed Res. Int. 2013, 2013. [Google Scholar] [CrossRef]
- Kim, S.; Jung, A. Optimum cutoff value of urinary cotinine distinguishing South Korean adult smokers from nonsmokers using data from the KNHANES (2008–2010). Nicotine Tob. Res. 2013, 15, 1608–1616. [Google Scholar] [CrossRef]
- Habibzadeh, F.; Habibzadeh, P.; Yadollahie, M. On determining the most appropriate test cut-off value: The case of tests with continuous results. Biochem. Medica 2016, 26, 297–307. [Google Scholar] [CrossRef]
- Arbuckle, T.E.; Liang, C.L.; Fisher, M.; Caron, N.J.; Fraser, W.D. Exposure to tobacco smoke and validation of smoking status during pregnancy in the MIREC study. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Du, J.X.; Watkins, T.; Bravo, L.E.; Fontham, E.T.H.; Camargo, M.C.; Correa, P.; Mera, R. 13 C-urea breath test for Helicobacter pylori in young children: Cut-off point determination by finite mixture model. Stat. Med. 2004, 23, 2049–2060. [Google Scholar] [CrossRef]
- Davis, R.A.; Stiles, M.F.; DeBethizy, J.D.; Reynolds, J.H. Dietary nicotine: A source of urinary cotinine. Food Chem. Toxicol. 1991, 29, 821–827. [Google Scholar] [CrossRef]
- Nielsen, S.S.; Franklin, G.M.; Longstreth, W.T.; Swanson, P.D.; Checkoway, H. Nicotine from edible Solanaceae and risk of Parkinson disease. Ann. Neurol. 2013, 74, 472–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, Y.; Takachi, R.; Ishihara, J.; Ishii, Y.; Sasazuki, S.; Sawada, N.; Shinozawa, Y.; Tanaka, J.; Kato, E.; Kitamura, K.; et al. Validity of Short and Long Self-Administered Food Frequency Questionnaires in Ranking Dietary Intake in Middle-Aged and Elderly Japanese in the Japan Public Health Center-Based Prospective Study for the Next Generation (JPHC-NEXT) Protocol Area. J. Epidemiol. 2016, 26, 420–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helsel, D.R. Fabricating data: How substituting values for nondetects can ruin results, and what can be done about it. Chemosphere 2006, 65, 2434–2439. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Casas, M.; Basagaña, X.; Sakhi, A.K.; Haug, L.S.; Philippat, C.; Granum, B.; Manzano-Salgado, C.B.; Brochot, C.; Zeman, F.; de Bont, J.; et al. Variability of urinary concentrations of non-persistent chemicals in pregnant women and school-aged children. Environ. Int. 2018, 121, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare National Growth Survey on Preschool Children (In Japanese). Available online: https://www.mhlw.go.jp/stf/houdou/0000042861.html (accessed on 19 March 2020).
- Kaneita, Y.; Tomofumi, S.; Takemura, S.; Suzuki, K.; Yokoyama, E.; Miyake, T.; Harano, S.; Ibuka, E.; Kaneko, A.; Tsutsui, T.; et al. Prevalence of smoking and associated factors among pregnant women in Japan. Prev. Med. 2007, 45, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Kaneita, Y.; Yokoyama, E.; Sone, T.; Takemura, S.; Suzuki, K.; Kaneko, A.; Ohida, T. Alcohol consumption and abstention among pregnant Japanese women. J. Epidemiol. 2008, 18, 173–182. [Google Scholar] [CrossRef] [Green Version]
- Matsuzaki, M.; Haruna, M.; Ota, E.; Murayama, R.; Yamaguchi, T.; Shioji, I.; Sasaki, S.; Yamaguchi, T.; Murashima, S. Effects of lifestyle factors on urinary oxidative stress and serum antioxidant markers in pregnant Japanese women: A cohort study. Biosci. Trends 2014, 8, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Higashida, Y.; Ohashi, K. Reduction of tobacco smoke exposure for pregnant passive smokers using feedback of urinary cotinine test results. J. Obstet. Gynaecol. Res. 2014, 40, 1015–1022. [Google Scholar] [CrossRef]
- World Health Organization. World Health Statistics 2018: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Yao, Y.; Nakamura, R.; Sari, N. The educational gap in tar and nicotine content in purchases of cigarettes: An observational study using large-scale representative survey data from Japan. Prev. Med. 2019, 129, 105828. [Google Scholar] [CrossRef]
- Inaba, Y.; Ohkubo, T.; Uchiyama, S.; Kunugita, N. Determination of Nicotine, Tobacco-Specific Nitrosamine and Mutagenic Activity of Whole Tobacco in Japanese Cigarettes [Article in Japanese]. Jpn. J. Hyg. 2013, 68, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Pickett, K.E.; Rathouz, P.J.; Kasza, K.; Wakschlag, L.S.; Wright, R. Self-reported smoking, cotinine levels, and patterns of smoking in pregnancy. Paediatr. Perinat. Epidemiol. 2005, 19, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol. Rev. 1996, 18, 188–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, S.; Merino, C.; Paton, B.; Correig, X.; Ramírez, N. Biomarkers of exposure to secondhand and thirdhand Tobacco smoke: Recent advances and future perspectives. Int. J. Environ. Res. Public Health 2018, 15, 2693. [Google Scholar] [CrossRef] [Green Version]
- Inaba, Y.; Uchiyama, S.; Bekki, K.; Kunugita, N. Implementation of Articles 9 and 10 of the Framework Convention on Tobacco Control: Tobacco product regulation in Japan. J. Natl. Inst. Public Heal. 2015, 64, 448–459. [Google Scholar]
- Munch, D.; Branson, P. Statistical Protocol for the Determination of the Single-Laboratory Lowest Concentration Minimum Reporting Level (LCMRL) and Validation of Laboratory Performance at or Below the Minimum Reporting Level (MRL). Available online: https://nepis.epa.gov/Exe/ZyNET.exe/P1005EAE.TXT?ZyActionD=ZyDocument&Client=EPA&Index=2000+Thru+2005&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery= (accessed on 16 February 2020).



{kind=link}
{kind=link}
| Demographic Characteristics | n (%) |
|---|---|
| Maternal age (n = 90,033, years, median (range)) | 31.0 (14.0–50.0) |
| Gestational week (n = 90,049, weeks, median (range)) | 27.0 (15.0–41.0) |
| Household income (n = 83,755) | |
| <4 million yen (~37,000 USD) | 27,694 (33.1) |
| 4–6 million yen | 33,781 (40.3) |
| >6 million yen (~55,000 USD) | 22,280 (26.6) |
| Maternal smoking status (n = 89,895) | |
| No | 85,742 (95.4) |
| Yes | 4153 (4.6) |
| Partner smoking status (n = 89,463) | |
| No | 47,611 (53.2) |
| Yes | 41,852 (46.8) |
| Passive smoking (n = 89,788) | |
| None | 55,859 (62.2) |
| One day per week | 10,647 (11.9) |
| Two to three days per week | 7404 (8.2) |
| Four to six days per week | 4372 (4.9) |
| Seven days per week | 11,506 (12.8) |
| Number of cigarettes smoked per day(n = 4114, cigarettes per day, median (range)) | 10 (0–60) |
| Urinary cotinine concentration | |
| (µg/g-creatinine, median interquartile range (IQR)) | 0.24 (0.083–0.96) |
| (ng/mL, median (IQR)) | 0.15 (0.057–0.63) |
| Urinary creatinine concentration (mg/dl, median (IQR)) | 74.3 (42.3–116.4) |
| True Condition | |||
|---|---|---|---|
| ≥36.8 µg/g-Creatinine | <36.8 µg/g-Creatinine | ||
| Questionnaire (Smoking) | Yes | 4017 | 136 |
| No | 3659 | 82,083 | |
| Sensitivity | 0.523 | ||
| Specificity | 0.998 | ||
| Positive Predictive Value | 0.967 | ||
| Negative Predictive Value | 0.957 | ||
| Partner Smoking | Passive Smoking 7 Days | ≥4 Days | ≥2 Days | ≥1 Day | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ≥COV | <COV | ≥COV | <COV | ≥COV | <COV | ≥COV | <COV | ≥COV | <COV | ||
| Questionnaire Response | Yes | 23,464 | 14,602 | 7734 | 1178 | 10,605 | 2262 | 15,067 | 4687 | 19,797 | 10,294 |
| No | 11,413 | 35,624 | 27,143 | 49,048 | 24,272 | 47,964 | 19,810 | 45,539 | 15,080 | 39,932 | |
| Sensitivity | 0.673 | 0.222 | 0.304 | 0.432 | 0.568 | ||||||
| Specificity | 0.709 | 0.977 | 0.955 | 0.907 | 0.795 | ||||||
| Positive Predictive Value | 0.616 | 0.868 | 0.824 | 0.763 | 0.658 | ||||||
| Negative Predictive Value | 0.757 | 0.644 | 0.664 | 0.697 | 0.726 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishihama, Y.; Nakayama, S.F.; Tabuchi, T.; Isobe, T.; Jung, C.-R.; Iwai-Shimada, M.; Kobayashi, Y.; Michikawa, T.; Sekiyama, M.; Taniguchi, Y.; et al. Determination of Urinary Cotinine Cut-Off Concentrations for Pregnant Women in the Japan Environment and Children’s Study (JECS). Int. J. Environ. Res. Public Health 2020, 17, 5537. https://doi.org/10.3390/ijerph17155537
Nishihama Y, Nakayama SF, Tabuchi T, Isobe T, Jung C-R, Iwai-Shimada M, Kobayashi Y, Michikawa T, Sekiyama M, Taniguchi Y, et al. Determination of Urinary Cotinine Cut-Off Concentrations for Pregnant Women in the Japan Environment and Children’s Study (JECS). International Journal of Environmental Research and Public Health. 2020; 17(15):5537. https://doi.org/10.3390/ijerph17155537
Chicago/Turabian StyleNishihama, Yukiko, Shoji F. Nakayama, Takahiro Tabuchi, Tomohiko Isobe, Chau-Ren Jung, Miyuki Iwai-Shimada, Yayoi Kobayashi, Takehiro Michikawa, Makiko Sekiyama, Yu Taniguchi, and et al. 2020. "Determination of Urinary Cotinine Cut-Off Concentrations for Pregnant Women in the Japan Environment and Children’s Study (JECS)" International Journal of Environmental Research and Public Health 17, no. 15: 5537. https://doi.org/10.3390/ijerph17155537
APA StyleNishihama, Y., Nakayama, S. F., Tabuchi, T., Isobe, T., Jung, C. -R., Iwai-Shimada, M., Kobayashi, Y., Michikawa, T., Sekiyama, M., Taniguchi, Y., Nitta, H., Yamazaki, S., & on behalf of the Japan Environment and Children’s Study Group. (2020). Determination of Urinary Cotinine Cut-Off Concentrations for Pregnant Women in the Japan Environment and Children’s Study (JECS). International Journal of Environmental Research and Public Health, 17(15), 5537. https://doi.org/10.3390/ijerph17155537