Does Mental Well-Being Protect against Self-Harm Thoughts and Behaviors during Adolescence? A Six-Month Prospective Investigation


Abstract
:1. Introduction
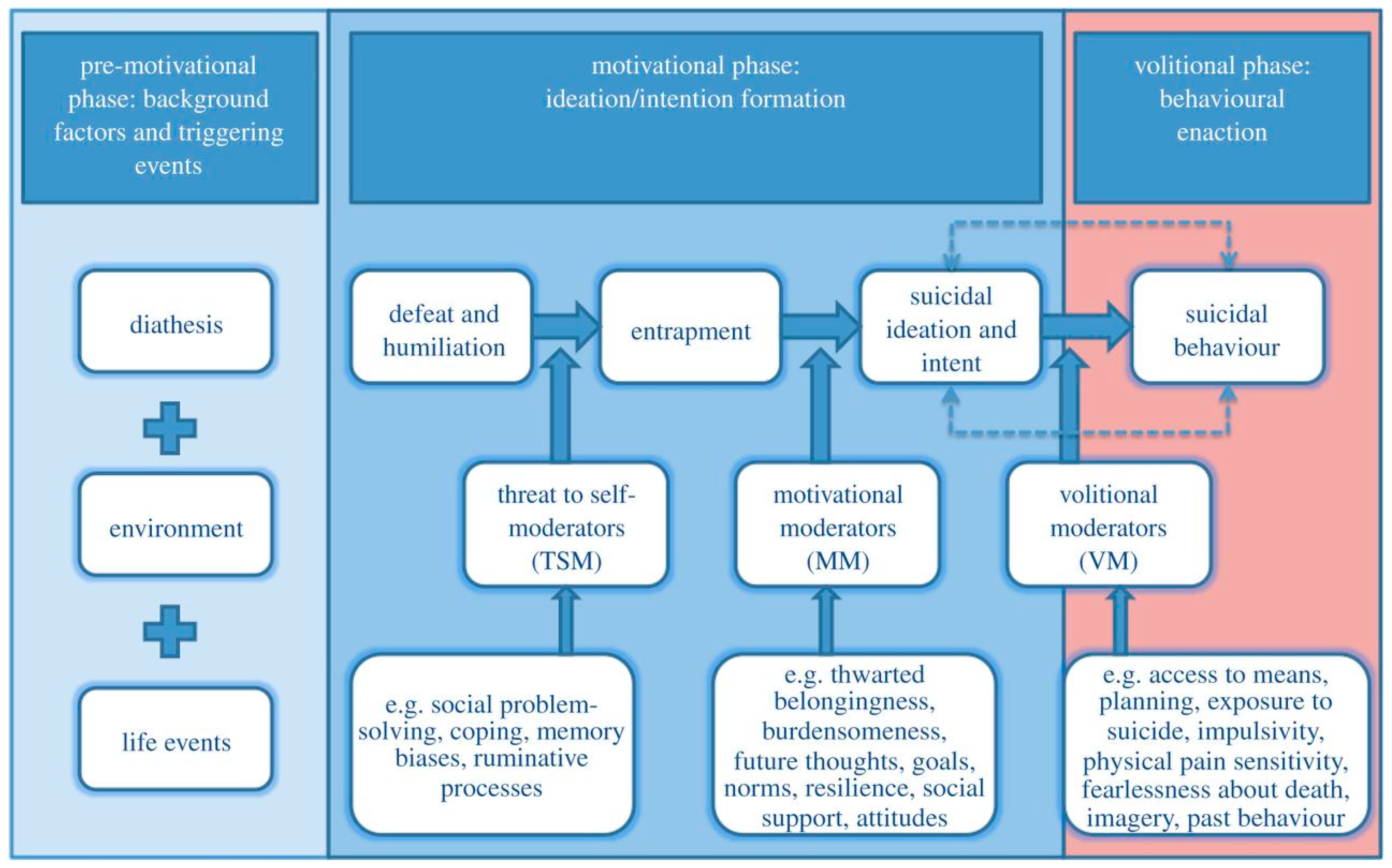
1.1. Integrated Motivational-Volitional Model of Suicidal Behavior (IMV)
1.2. Mental Well-Being During Adolescence
1.3. Does Increased Mental Well-Being Protect Against Self-Harm Risk During Adolescence?
1.4. The Current Study
- To examine whether mental well-being protects against subsequent self-harm thoughts and behaviors;
- To determine if mental well-being is associated with subsequent perceptions of defeat, internal entrapment and external entrapment;
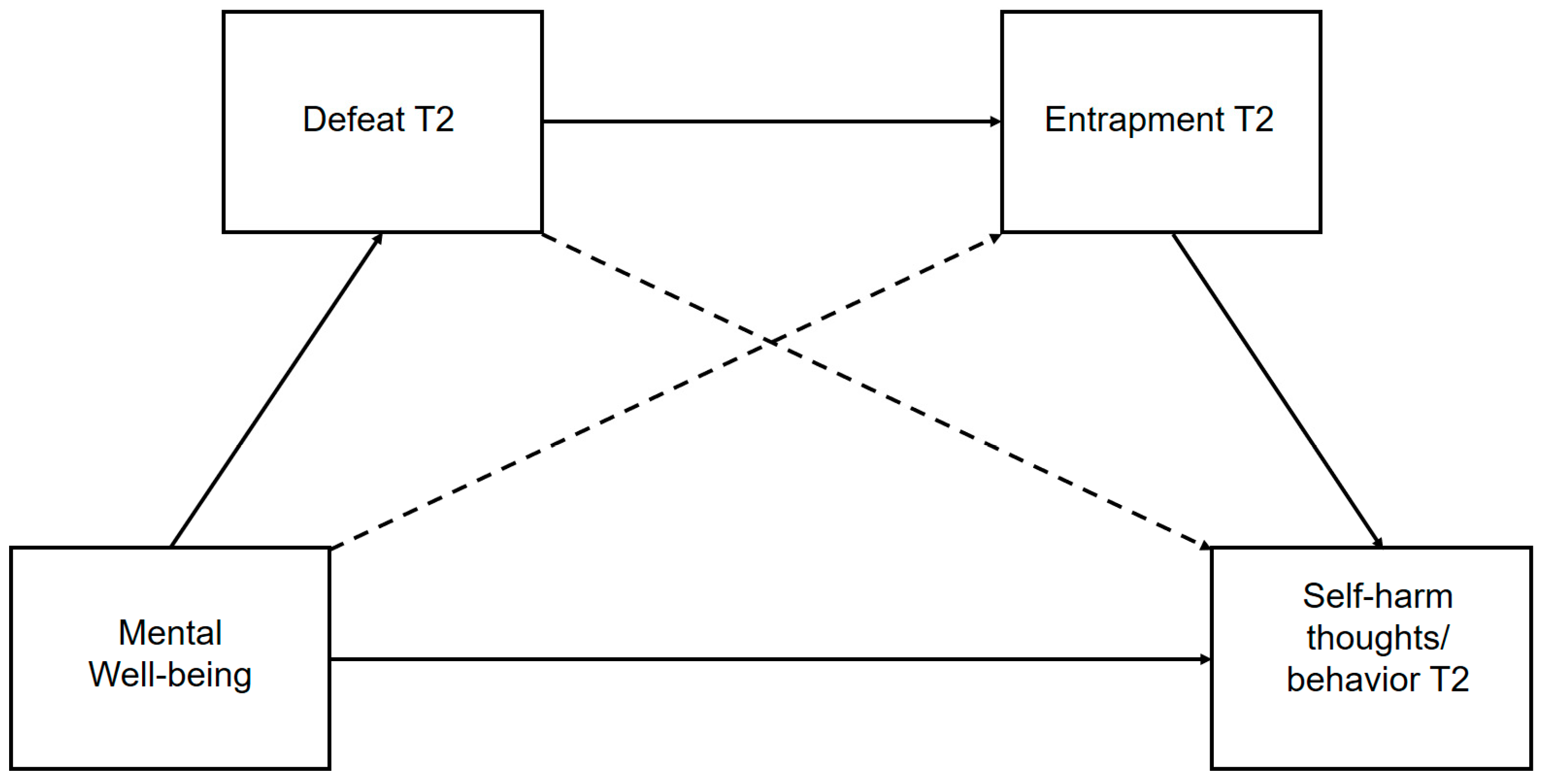
- To test hypothesized multistep pathways derived from the IMV that link mental well-being (as a potential pre-motivational factor) and subsequent self-harm thoughts and behaviors, via perceptions of defeat and entrapment (Figure 2);
- To establish whether mental well-being moderates the relationship between entrapment and subsequent self-harm thoughts.
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analytic Strategy
3. Results
3.1. Preliminary Results
3.2. Does Mental Well-Being Protect Against Subsequent Self-Harm Thoughts and Behaviors?
3.3. Is Mental Well-Being Associated with Reduced Perceptions of Defeat and Entrapment?
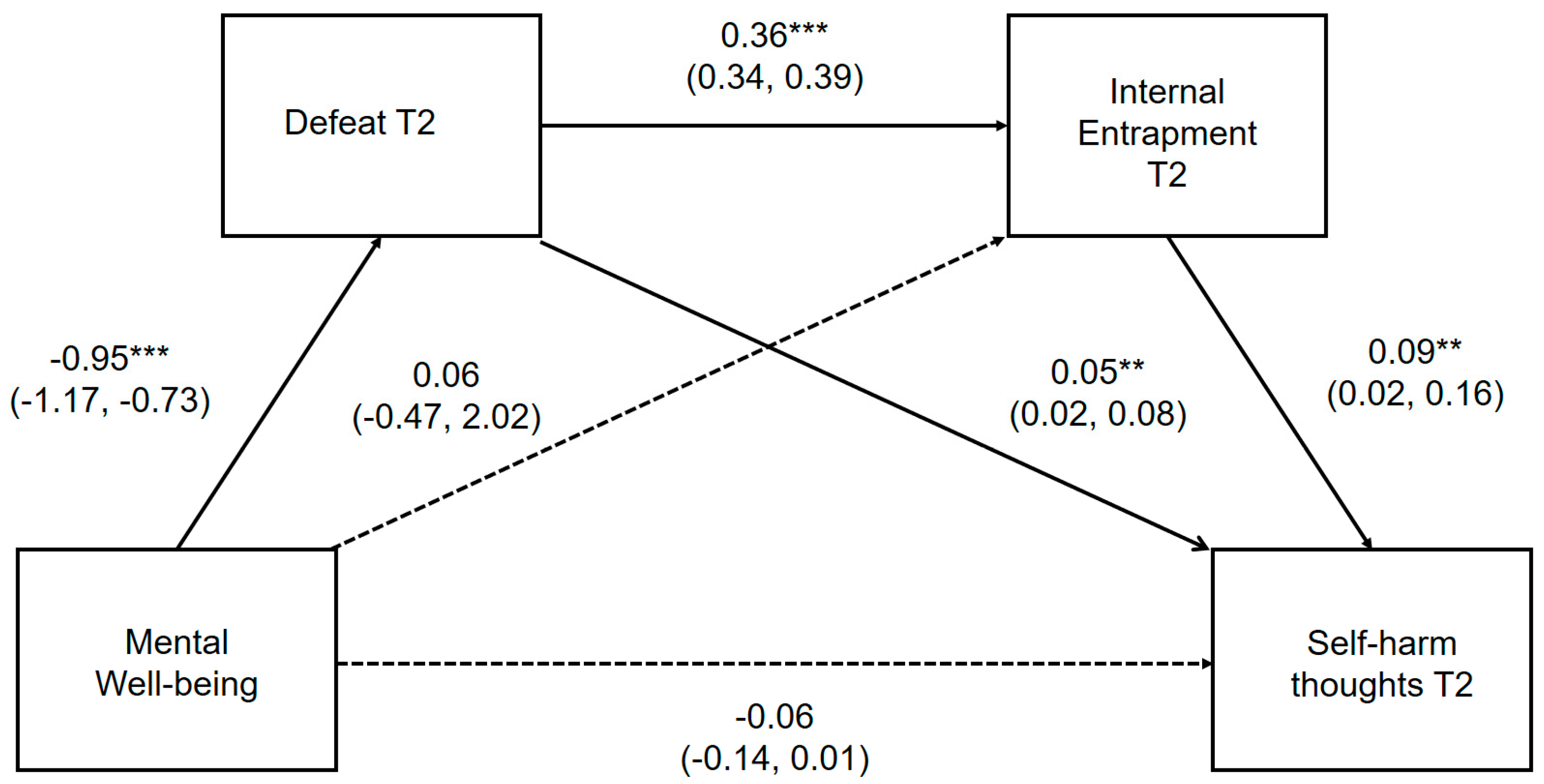
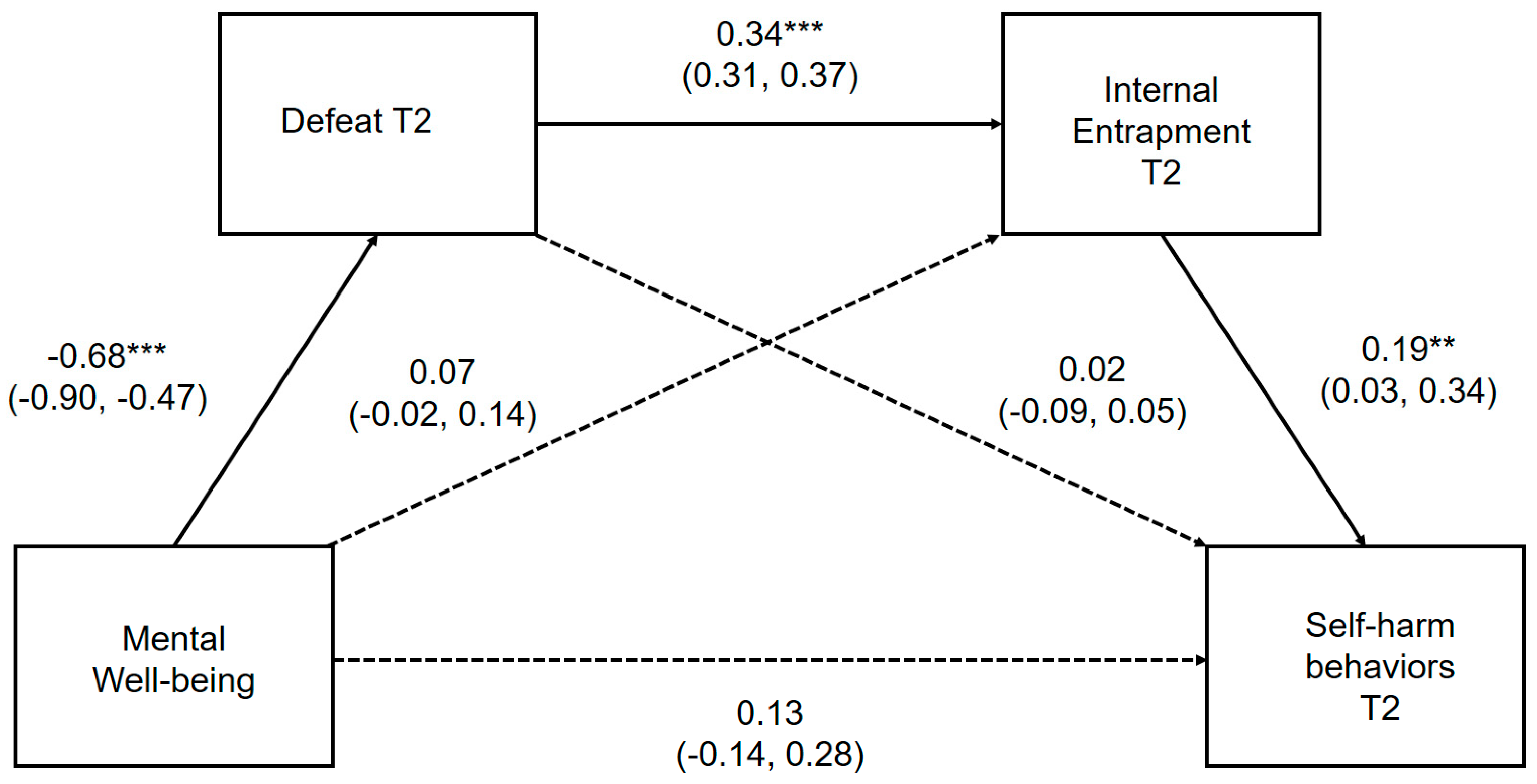
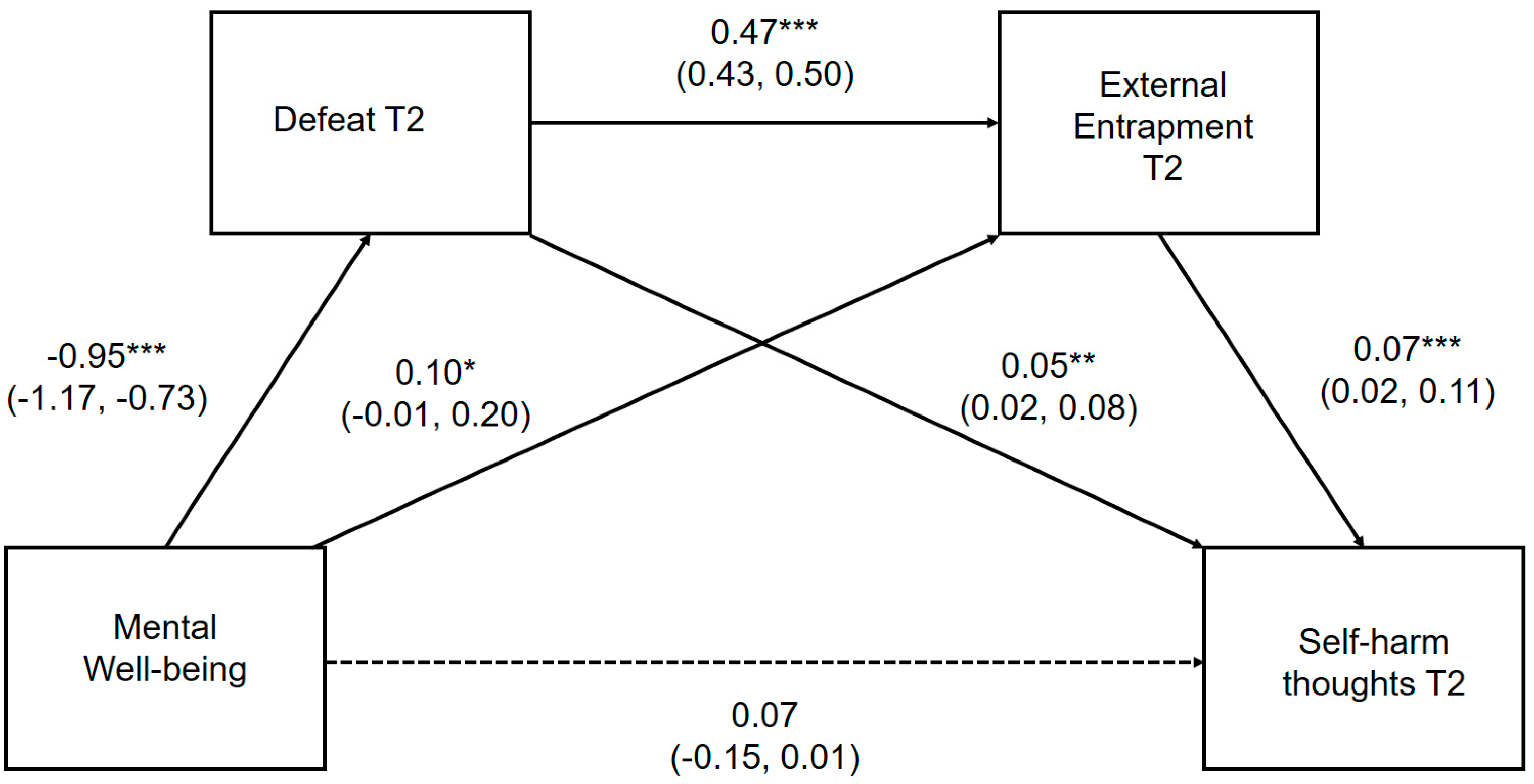
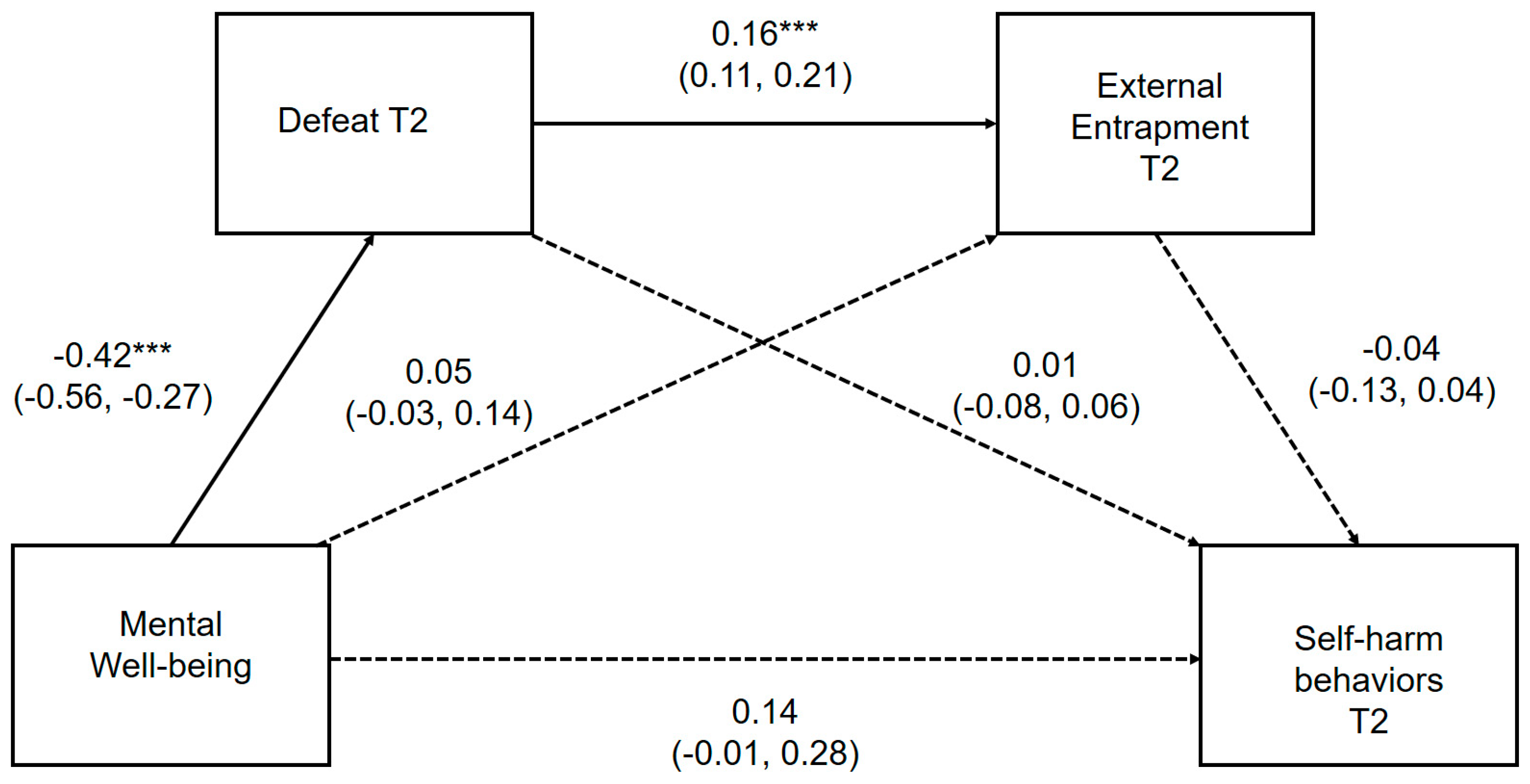
3.4. Do Perceptions of Defeat and Entrapment Mediate the Relationship Between Mental Well-Being and Subsequent Self-Harm Thoughts and Behavior?
3.5. Does Mental Well-Being Moderate the Relationship Between Entrapment and Prospective Self-Harm Thoughts?
4. Discussion
4.1. Mental Well-Being in Relation to Subsequent Self-Harm Thoughts and Behaviors
4.2. Mechanisms Linking Mental Well-Being and Self-Harm Risk: The Role of Defeat and Entrapment
4.3. Establishing the Nature of the Link Between Mental Well-Being and Defeat
4.4. Mental Well-Being as a Moderator of the Relationship Between Entrapment and Self-Harm Thoughts
4.5. Strengths and Limitations
4.6. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- The National Institute for Health and Care Excellence (NICE). Self-Harm in over 8s: Long-Term Management. Clinical Guideline [CG133]. 2011. Available online: https://www.nice.org.uk/guidance/cg133 (accessed on 12 July 2020).
- The National Institute for Health and Care Excellence (NICE). Self-Harm in over 8s: Short-Term Management and Prevention of Recurrence. Clinical Guideline [CG16]. 2004. Available online: https://www.nice.org.uk/guidance/cg16 (accessed on 12 July 2020).
- Geulayov, G.; Casey, D.; McDonald, K.C.; Foster, P.; Pritchard, K.; Wells, C.; Clements, C.; Kapur, N.; Ness, J.; Waters, K.; et al. Incidence of suicide, hospital-presenting non-fatal self-harm, and community-occurring non-fatal self-harm in adolescents in England (the iceberg model of self-harm): A retrospective study. Lancet Psychiatry 2018, 5, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Mars, B.; Heron, J.; Klonsky, E.D.; Moran, P.; O’Connor, R.C.; Tilling, K.; Wilkinson, P.; Gunnell, D. Predictors of future suicide attempt among adolescents with suicidal thoughts or non-suicidal self-harm: A population-based birth cohort study. Lancet Psychiatry 2019, 6, 327–337. [Google Scholar] [CrossRef] [Green Version]
- McManus, S.; Gunnell, D.; Cooper, C.; Bebbington, P.E.; Howard, L.M.; Brugha, T.; Jenkins, R.; Hassiotis, A.; Weich, P.; Appleby, L. Prevalence of non-suicidal self-harm and service contact in England, 2000–2014: Repeated cross-sectional surveys of the general population. Lancet Psychiatry 2019, 6, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Hawton, K.; Saunders, K.E.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Olfson, M.; Wall, M.; Wang, S.; Crystal, S.; Bridge, J.A.; Liu, S.M.; Blanco, C. Suicide after deliberate self-harm in adolescents and young adults. Pediatrics 2018, 141, e20173517. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, R.C. The integrated motivational-volitional model of suicidal behavior. Crisis 2011, 32, 295–298. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Nock, M.K. The psychology of suicidal behaviour. Lancet Psychiatry 2014, 1, 73–85. [Google Scholar] [CrossRef]
- Glenn, C.R.; Kleiman, E.M.; Cha, C.B.; Deming, C.A.; Franklin, J.C.; Nock, M.K. Understanding suicide risk within the Research Domain Criteria (RDoC) framework: A meta-analytic review. Depress. Anxiety 2018, 35, 65–88. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Anestis, M.D. Introduction to the special issue: Recent advances in suicide research: Mediators and moderators of risk and resilience. Int. J. Cogn. Ther. 2015, 8, 95–98. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational–volitional model of suicidal behaviour. Philos. Trans. R. Soc. B Biol. Sci. 2018, 373, 20170268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, R.C. Towards and integrated motivational-volitional model of suicidal behaviour. In The International Handbook of Suicide Prevention, 1st ed.; O’Connor, R.C., Pirkis, J.E., Eds.; John Wiley & Sons: Chichester, UK, 2016; Volume 1, pp. 181–198. [Google Scholar]
- Littlewood, D.L.; Gooding, P.; Kyle, S.D.; Pratt, D.; Peters, S. Understanding the role of sleep in suicide risk: Qualitative interview study. BMJ Open 2016, 6, e012113. [Google Scholar] [CrossRef]
- Littlewood, D.L.; Gooding, P.A.; Panagioti, M.; Kyle, S.D. Nightmares and suicide in posttraumatic stress disorder: The mediating role of defeat, entrapment, and hopelessness. J. Clin. Sleep Med. 2016, 12, 393–399. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, R.C. Suicidal behavior as a cry of pain: Test of a psychological model. Arch. Suicide Res. 2003, 7, 297–308. [Google Scholar]
- Rasmussen, S.A.; Fraser, L.; Gotz, M.; MacHale, S.; Mackie, R.; Masterton, G.; McConachie, S.; O’Connor, R.C. Elaborating the cry of pain model of suicidality: Testing a psychological model in a sample of first-time and repeat self-harm patients. Br. J. Clin. Psychol. 2010, 49, 15–30. [Google Scholar] [CrossRef]
- Del Carpio, L.; Rasmussen, S.; Paul, S. A theory-based longitudinal investigation examining predictors of self-harm in adolescents with and without bereavement experiences. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Rasmussen, S.; Hawton, K. Distinguishing adolescents who think about self-harm from those who engage in self-harm. Br. J. Psychiatry 2012, 200, 330–335. [Google Scholar]
- Russell, K.; Rasmussen, S.; Hunter, S.C. Insomnia and nightmares as markers of risk for suicidal ideation in young people: Investigating the role of defeat and entrapment. J. Clin. Sleep Med. 2018, 14, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Fliege, H.; Lee, J.R.; Grimm, A.; Klapp, B.F. Risk factors and correlates of deliberate self-harm behavior: A systematic review. J. Psychosom. Res. 2009, 66, 477–493. [Google Scholar] [CrossRef]
- World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice: A Report of the World Health Organization, Department of Mental Health and Substance Abuse in Collaboration with the Victorian Health Promotion Foundation and the University of Melbourne; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Clarke, A.; Friede, T.; Putz, R.; Ashdown, J.; Martin, S.; Blake, A.; Adi, Y.; Parkinson, J.; Flynn, P.; Platt, S.; et al. Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health 2011, 11, 487. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyes, C.L. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [PubMed] [Green Version]
- Stewart-Brown, S.L.; Tennant, R.; Tennant, A.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh MentalWell-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar]
- Linley, P.A.; Joseph, S. Applied positive psychology: A new perspective for professional practice. Posit. Psychol. Pract. 2004, 3–12. [Google Scholar] [CrossRef]
- Zadow, C.; Houghton, S.; Hunter, S.C.; Rosenberg, M.; Wood, L. Associations between positive mental wellbeing and depressive symptoms in Australian adolescents. Educ. Dev. Psychol. 2017, 34, 95–105. [Google Scholar]
- Dolan, P.; Metcalfe, R. Measuring subjective wellbeing: Recommendations on measures for use by national governments. J. Soc. Policy 2012, 41, 409–427. [Google Scholar]
- McAneney, H.; Tully, M.A.; Hunter, R.F.; Kouvonen, A.; Veal, P.; Stevenson, M.; Kee, F. Individual factors and perceived community characteristics in relation to mental health and mental well-being. BMC Public Health 2015, 15, 1237. [Google Scholar]
- Teismann, T.; Forkmann, T.; Glaesmer, H.; Egeri, L.; Margraf, J. Remission of suicidal thoughts: Findings from a longitudinal epidemiological study. J. Affect. Disord 2016, 190, 723–725. [Google Scholar]
- Teismann, T.; Forkmann, T.; Brailovskaia, J.; Siegmann, P.; Glaesmer, H.; Margraf, J. Positive mental health moderates the association between depression and suicide ideation: A longitudinal study. Int. J. Clin. Health Psychol. 2018, 18, 1–7. [Google Scholar]
- Teismann, T.; Brailovskaia, J.; Margraf, J. Positive mental health, positive affect and suicide ideation. Int. J. Clin. Health Psychol. 2019, 19, 165–169. [Google Scholar]
- Morey, Y.; Mellon, D.; Dailami, N.; Verne, J.; Tapp, A. Adolescent self-harm in the community: An update on prevalence using a self-report survey of adolescents aged 13–18 in England. J. Public Health 2017, 39, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Teismann, T.; Brailovskaia, J. Entrapment, positive psychological functioning and suicide ideation: A moderation analysis. Clin. Psychol. Psychother. 2020, 27, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Brailovskaia, J.; Teismann, T.; Margraf, J. Positive mental health, stressful life events, and suicide ideation. Crisis 2020. [Google Scholar] [CrossRef]
- Forkmann, T.; Teismann, T.; Stenzel, J.S.; Glaesmer, H.; De Beurs, D. Defeat and entrapment: More than meets the eye? Applying network analysis to estimate dimensions of highly correlated constructs. BMC Med. Res. Methodol. 2018, 18, 16. [Google Scholar] [CrossRef] [Green Version]
- Cramer, R.J.; Rasmussen, S.; Tucker, R.P. An examination of the Entrapment Scale: Factor structure, correlates, and implications for suicide prevention. Psychiatry Res. 2019, 282, 112550. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Rasmussen, S.; Miles, J.; Hawton, K. Self-harm in adolescents: Self-report survey in schools in Scotland. Br. J. Psychiatry 2009, 194, 68–72. [Google Scholar] [CrossRef]
- Clarke, A.; Putz, R.; Friede, T.; Ashdown, J.; Adi, Y.; Martin, S.; Flynn, P.; Blake, A.; Stewart-Brown, S.; Platt, S. Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) Acceptability and Validation in English and Scottish Secondary School Students (The WAVES Project) Glasgow; NHS Health Scotland: Edinburgh, UK, 2010. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, E.; Sayal, K.; Townsend, E. Correction: Exploring the Relationship between Experiential Avoidance, Coping Functions and the Recency and Frequency of Self-Harm. PLoS ONE 2018, 13, e0192795. [Google Scholar] [CrossRef] [Green Version]
- White, D.; Leach, C.; Sims, R.; Atkinson, M.; Cottrell, D. Validation of the Hospital Anxiety and Depression Scale for use with adolescents. Br. J. Psychiatry 1999, 175, 452–454. [Google Scholar] [CrossRef]
- Hawton, K.; Rodham, K.; Evans, E. By Their Own Young Hand: Deliberate Self-Harm and Suicidal Ideas in Adolescents, 1st ed.; Jessica Kingsley Publishers: London, UK, 2006. [Google Scholar]
- Madge, N.; Hewitt, A.; Hawton, K.; de Wilde, E.J.D.; Corcoran, P.; Fekete, S.; van Heeringen, K.; De Leo, D.; Ystgaard, M. Deliberate self-harm within an international community sample of young people: Comparative findings from the Child & Adolescent Self-harm in Europe (CASE) Study. J. Child. Psychol. Psychiatry 2008, 49, 667–677. [Google Scholar] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2017; pp. 167–180. [Google Scholar]
- Griffiths, A.W.; Wood, A.M.; Maltby, J.; Taylor, P.J.; Tai, S. The prospective role of defeat and entrapment in depression and anxiety: A 12-month longitudinal study. Psychiatry Res. 2014, 216, 52–59. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.C.; Portzky, G. The relationship between entrapment and suicidal behavior through the lens of the integrated motivational–volitional model of suicidal behavior. Curr. Opin. Psychol. 2018, 22, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, R.; Dempsey, R.; Jones, S.; Gooding, P. Defeat and entrapment in bipolar disorder: Exploring the relationship with suicidal ideation from a psychological theoretical perspective. Suicide Life Threat. Behav. 2018, 48, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Siddaway, A.P.; Taylor, P.J.; Wood, A.M.; Schulz, J. A meta-analysis of perceptions of defeat and entrapment in depression, anxiety problems, posttraumatic stress disorder, and suicidality. J. Affect. Disord 2015, 184, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, K. Positive mental health and its relationship with resilience. Ind. Psychiatry J. 2011, 20, 75. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. Research on resilience: Response to commentaries. Child. Dev. 2000, 71, 573–575. [Google Scholar] [CrossRef]
- Richardson, G.E. The metatheory of resilience and resiliency. J. Clin. Psychol. 2002, 58, 307–321. [Google Scholar] [CrossRef]
- Joyce, S.; Shand, F.; Tighe, J.; Laurent, S.J.; Bryant, R.A.; Harvey, S.B. Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- McMahon, E.M.; Keeley, H.; Cannon, M.; Arensman, E.; Perry, I.J.; Clarke, M.; Chambers, D.; Cororan, P. The iceberg of suicide and self-harm in Irish adolescents: A population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1929–1935. [Google Scholar] [CrossRef]
- Hawton, K.; Rodham, K.; Evans, E.; Harriss, L. Adolescents who self harm: A comparison of those who go to hospital and those who do not. Child. Adolesc. Ment. Health 2009, 14, 24–30. [Google Scholar] [CrossRef]
- Rodham, K.; Hawton, K.; Evans, E. Reasons for deliberate self-harm: Comparison of self-poisoners and self-cutters in a community sample of adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 2004, 43, 80–87. [Google Scholar] [CrossRef]
- Mars, B.; Cornish, R.; Heron, J.; Boyd, A.; Crane, C.; Hawton, K.; Lewis, G.; Tilling, K.; Macleod, J.; Gunnell, D. Using data linkage to investigate inconsistent reporting of self-harm and questionnaire non-response. Arch. Suicide Res. 2016, 20, 113–141. [Google Scholar] [CrossRef] [Green Version]
- Epstein, S.; Roberts, E.; Sedgwick, R.; Polling, C.; Finning, K.; Ford, T.; Dutta, R.; Downs, J. School absenteeism as a risk factor for self-harm and suicidal ideation in children and adolescents: A systematic review and meta-analysis. Eur. Child. Adolesc. Psychiatry 2019, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Winer, E.S.; Cervone, D.; Bryant, J.; McKinney, C.; Liu, R.T.; Nadorff, M.R. Distinguishing mediational models and analyses in clinical psychology: Atemporal associations do not imply causation. J. Clin. Psychol. 2016, 72, 947–955. [Google Scholar] [CrossRef]
- Wells, J.; Barlow, J.; Stewart-Brown, S. A systematic review of universal approaches to mental health promotion in schools. Health Educ. 2003, 103, 197–220. [Google Scholar] [CrossRef]
- Manicavasagar, V.; Horswood, D.; Burckhardt, R.; Lum, A.; Hadzi-Pavlovic, D.; Parker, G. Feasibility and effectiveness of a web-based positive psychology program for youth mental health: Randomized controlled trial. J. Med. Internet Res. 2014, 16, e140. [Google Scholar] [CrossRef]
- Meredith, G.R.; Rakow, D.A.; Eldermine, E.R.B.; Madsen, C.G.; Shelley, S.P.; Sachs, N.A. Minimum Time Dose in Nature to Positively Impact the Mental Health of College-Aged Students, and How to Measure It: A Scoping Review. Front. Psychol. Environ. Psychol. 2020, 11, 2942. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable/Metric | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Mental well-being | |||||||
| 2. Depressive symptoms | −0.51 *** | ||||||
| 3. Defeat | −0.52 *** | 0.41 *** | |||||
| 4. Internal entrapment | −0.42 *** | 0.38 *** | 0.78 *** | ||||
| 5. External entrapment | −0.37 *** | 0.34 *** | 0.76 *** | 0.84 *** | |||
| 6. SHT T2 | −0.27 *** | 0.19 *** | 0.42 *** | 0.45 *** | 0.43 *** | ||
| 7. SHB T2 | −0.16 *** | 0.11 ** | 0.32 *** | 0.35 *** | 0.34 *** | 0.67 *** | |
| Median | 22.85 | 3.00 | 12.00 | 1.50 | 2.00 | - | - |
| Interquartile range | 5.78 | 4.00 | 17.00 | 6.00 | 7.00 | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russell, K.; Rasmussen, S.; Hunter, S.C. Does Mental Well-Being Protect against Self-Harm Thoughts and Behaviors during Adolescence? A Six-Month Prospective Investigation. Int. J. Environ. Res. Public Health 2020, 17, 6771. https://doi.org/10.3390/ijerph17186771
Russell K, Rasmussen S, Hunter SC. Does Mental Well-Being Protect against Self-Harm Thoughts and Behaviors during Adolescence? A Six-Month Prospective Investigation. International Journal of Environmental Research and Public Health. 2020; 17(18):6771. https://doi.org/10.3390/ijerph17186771
Chicago/Turabian StyleRussell, Kirsten, Susan Rasmussen, and Simon C. Hunter. 2020. "Does Mental Well-Being Protect against Self-Harm Thoughts and Behaviors during Adolescence? A Six-Month Prospective Investigation" International Journal of Environmental Research and Public Health 17, no. 18: 6771. https://doi.org/10.3390/ijerph17186771
APA StyleRussell, K., Rasmussen, S., & Hunter, S. C. (2020). Does Mental Well-Being Protect against Self-Harm Thoughts and Behaviors during Adolescence? A Six-Month Prospective Investigation. International Journal of Environmental Research and Public Health, 17(18), 6771. https://doi.org/10.3390/ijerph17186771