Prenatal Maternal Cortisol Levels and Infant Birth Weight in a Predominately Low-Income Hispanic Cohort


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
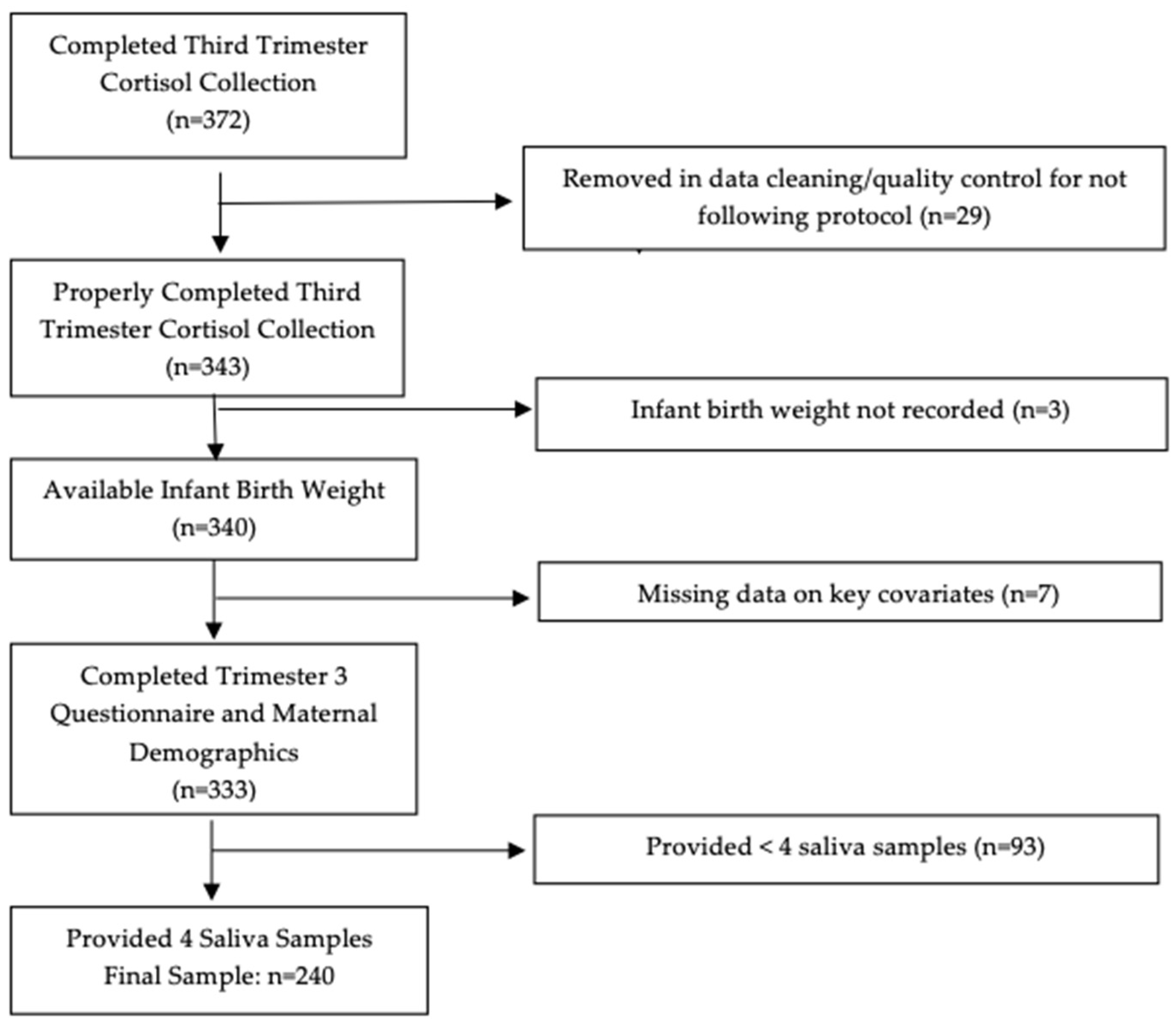
2.1. Sample
2.2. Salivary Cortisol Collection
2.3. Outcome
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Biological Stress Measures
3.3. Biological Stress Measures with Infant Birth Weight
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Individual Biological Stress Metric | β (SE) | p |
|---|---|---|
| Area Under the Curve, grounded (AUCg) *,1 | −7.8 (5.6) | 0.17 |
| Cortisol Awakening Response (CAR) * | −1.7 (16.2) | 0.91 |
| Diurnal Cortisol Slope (DCS) * | 87.1 (27.9) | 0.07 |
References
- Belbasis, L.; Savvidou, M.D.; Kanu, C.; Evangelou, E.; Tzoulaki, I. Birth weight in relation to health and disease in later life: An umbrella review of systematic reviews and meta-analyses. BMC Med. 2016, 14, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camerota, M.; Bollen, K.A. Birth Weight, Birth Length, and Gestational Age as Indicators of Favorable Fetal Growth Conditions in a US Sample. PLoS ONE 2016, 11, e0153800. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Hales, C.N.; Fall, C.H.; Osmond, C.; Phipps, K.; Clark, P.M. Type 2 (non-insulin-dependent) diabetes mellitus, hypertension and hyperlipidaemia (syndrome X): Relation to reduced fetal growth. Diabetologia 1993, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutland, C.L.; Lackritz, E.M.; Mallett-Moore, T.; Bardají, A.; Chandrasekaran, R.; Lahariya, C.; Nisar, M.I.; Tapia, M.D.; Pathirana, J.; Kochhar, S.; et al. Low birth weight: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine 2017, 35, 6492–6500. [Google Scholar] [CrossRef] [PubMed]
- Evensen, E.; Emaus, N.; Kokkvoll, A.; Wilsgaard, T.; Furberg, A.S.; Skeie, G. The relation between birthweight, childhood body mass index, and overweight and obesity in late adolescence: A longitudinal cohort study from Norway, The Tromsø Study, Fit Futures. BMJ Open 2017, 7, e015576. [Google Scholar] [CrossRef]
- Jornayvaz, F.R.; Vollenweider, P.; Bochud, M.; Mooser, V.; Waeber, G.; Marques-Vidal, P. Low birth weight leads to obesity, diabetes and increased leptin levels in adults: The CoLaus study. Cardiovasc. Diabetol. 2016, 15, 73. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.F.; Shu, L.; Sheng, J.; Mu, M.; Wang, S.; Tao, X.Y.; Xu, S.J.; Tao, F.B. Birth weight and risk of coronary heart disease in adults: A meta-analysis of prospective cohort studies. J. Dev. Orig. Health Dis. 2014, 5, 408–419. [Google Scholar] [CrossRef]
- Pan, X.F.; Tang, L.; Lee, A.H.; Binns, C.; Yang, C.X.; Xu, Z.P.; Zhang, J.L.; Yang, Y.; Wang, H.; Sun, X. Association between fetal macrosomia and risk of obesity in children under 3 years in Western China: A cohort study. World J. Pediatrics WJP 2019, 15, 153–160. [Google Scholar] [CrossRef]
- Sparano, S.; Ahrens, W.; De Henauw, S.; Marild, S.; Molnar, D.; Moreno, L.A.; Suling, M.; Tornaritis, M.; Veidebaum, T.; Siani, A.; et al. Being macrosomic at birth is an independent predictor of overweight in children: Results from the IDEFICS study. Matern. Child Health J. 2013, 17, 1373–1381. [Google Scholar] [CrossRef]
- Wang, Y.; Gao, E.; Wu, J.; Zhou, J.; Yang, Q.; Walker, M.C.; Mbikay, M.; Sigal, R.J.; Nair, R.C.; Wen, S.W. Fetal macrosomia and adolescence obesity: Results from a longitudinal cohort study. Int. J. Obes. 2009, 33, 923–928. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.S. The epidemiology of adverse pregnancy outcomes: An overview. J. Nutr. 2003, 133, 1592s–1596s. [Google Scholar] [CrossRef]
- Geronimus, A.T. The weathering hypothesis and the health of African-American women and infants: Eidence and speculations. Ethn. Dis. 1992, 2, 207–221. [Google Scholar] [PubMed]
- Geronimus, A.T. Black/white differences in the relationship of maternal age to birthweight: A population-based test of the weathering hypothesis. Soc. Sci. Med. 1996, 42, 589–597. [Google Scholar] [CrossRef]
- McDonald, S.W.; Kingston, D.; Bayrampour, H.; Dolan, S.M.; Tough, S.C. Cumulative psychosocial stress, coping resources, and preterm birth. Arch. Women’s Ment. Health 2014, 17, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Rondó, P.H.; Ferreira, R.F.; Nogueira, F.; Ribeiro, M.C.; Lobert, H.; Artes, R. Maternal psychological stress and distress as predictors of low birth weight, prematurity and intrauterine growth retardation. Eur. J. Clin. Nutr. 2003, 57, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staneva, A.; Bogossian, F.; Pritchard, M.; Wittkowski, A. The effects of maternal depression, anxiety, and perceived stress during pregnancy on preterm birth: A systematic review. Women Birth J. Aust. Coll. Midwives 2015, 28, 179–193. [Google Scholar] [CrossRef]
- Riley, W.J. Health disparities: Gaps in access, quality and affordability of medical care. Trans. Am. Clin. Climatol. Assoc. 2012, 123, 167–172. [Google Scholar]
- Nagahawatte, N.T.; Goldenberg, R.L. Poverty, maternal health, and adverse pregnancy outcomes. Ann. N. Y. Acad. Sci. 2008, 1136, 80–85. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Drake, P. Births: Final Data for 2017. Natl. Vital Stat. Rep. Cent. Dis. Control Prev. Natl. Cent. Health Stat. Natl. Vital Stat. Syst. 2018, 67, 1–50. [Google Scholar]
- Arbona, C.; Olvera, N.; Rodriguez, N.; Hagan, J.; Linares, A.; Wiesner, M. Acculturative Stress Among Documented and Undocumented Latino Immigrants in the United States. Hisp. J. Behav. Sci. 2010, 32, 362–384. [Google Scholar] [CrossRef]
- Velasco-Mondragon, E.; Jimenez, A.; Palladino-Davis, A.G.; Davis, D.; Escamilla-Cejudo, J.A. Hispanic health in the USA: A scoping review of the literature. Public Health Rev. 2016, 37, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, E.K.; Kumari, M. Assessing salivary cortisol in large-scale, epidemiological research. Psychoneuroendocrinology 2009, 34. [Google Scholar] [CrossRef] [PubMed]
- Fries, E.; Dettenborn, L.; Kirschbaum, C. The cortisol awakening response (CAR): Facts and future directions. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2009, 72, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, J.C.; Wolf, O.T.; Hellhammer, D.H.; Buske-Kirschbaum, A.; von Auer, K.; Jobst, S.; Kaspers, F.; Kirschbaum, C. Free cortisol levels after awakening: A reliable biological marker for the assessment of adrenocortical activity. Life Sci. 1997, 61, 2539–2549. [Google Scholar] [CrossRef]
- Allolio, B.; Hoffmann, J.; Linton, E.A.; Winkelmann, W.; Kusche, M.; Schulte, H.M. Diurnal salivary cortisol patterns during pregnancy and after delivery: Relationship to plasma corticotrophin-releasing-hormone. Clin. Endocrinol. 1990, 33. [Google Scholar] [CrossRef]
- Jung, C.; Ho, J.T.; Torpy, D.J.; Rogers, A.; Doogue, M.; Lewis, J.G.; Czajko, R.J.; Inder, W.J. A longitudinal study of plasma and urinary cortisol in pregnancy and postpartum. J. Clin. Endocrinol. Metab. 2011, 96, 1533–1540. [Google Scholar] [CrossRef] [Green Version]
- Gudmundsson, A.; Carnes, M. Pulsatile adrenocorticotropic hormone: An overview. Biol. Psychiatry 1997, 41, 342–365. [Google Scholar] [CrossRef]
- Johnson, M.L.; Virostko, A.; Veldhuis, J.D.; Evans, W.S. Deconvolution analysis as a hormone pulse-detection algorithm. Methods Enzymol. 2004, 384, 40–54. [Google Scholar] [CrossRef]
- Bloom, S.L.; Sheffield, J.S.; McIntire, D.D.; Leveno, K.J. Antenatal dexamethasone and decreased birth weight. Obstet. Gynecol. 2001, 97. [Google Scholar] [CrossRef]
- Entringer, S.; Buss, C.; Wadhwa, P.D. Prenatal stress, telomere biology, and fetal programming of health and disease risk. Sci. Signal. 2012, 5, pt12. [Google Scholar] [CrossRef]
- French, N.P.; Hagan, R.; Evans, S.F.; Godfrey, M.; Newnham, J.P. Repeated antenatal corticosteroids: Size at birth and subsequent development. Am. J. Obstet. Gynecol. 1999, 180. [Google Scholar] [CrossRef]
- Reynolds, R.M. Glucocorticoid excess and the developmental origins of disease: Two decades of testing the hypothesis--2012 Curt Richter Award Winner. Psychoneuroendocrinology 2013, 38, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Togher, K.L.; Togher, K.L.; O’Keeffe, M.M.; O’Keeffe, M.M.; Khashan, A.S.; Khashan, A.S.; Gutierrez, H.; Gutierrez, H.; Kenny, L.C.; Kenny, L.C.; et al. Epigenetic regulation of the placental HSD11B2 barrier and its role as a critical regulator of fetal development. Epigenetics 2014, 9, 816–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowther, C.A.; Middleton, P.F.; Voysey, M.; Askie, L.; Zhang, S.; Martlow, T.K.; Aghajafari, F.; Asztalos, E.V.; Brocklehurst, P.; Dutta, S.; et al. Effects of repeat prenatal corticosteroids given to women at risk of preterm birth: An individual participant data meta-analysis. PLoS Med. 2019, 16, e1002771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolten, M.I.; Wurmser, H.; Buske-Kirschbaum, A.; Papoušek, M.; Pirke, K.M.; Hellhammer, D. Cortisol levels in pregnancy as a psychobiological predictor for birth weight. Arch. Women‘s Ment. Health 2011, 14, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, E.C.; Hill, J.; Pickles, A.; Glover, V.; O′Donnell, K.; Sharp, H. Associations between maternal prenatal cortisol and fetal growth are specific to infant sex: Findings from the Wirral Child Health and Development Study. J. Dev. Orig. Health Dis. 2018, 9, 425–431. [Google Scholar] [CrossRef]
- D′Anna-Hernandez, K.L.; Hoffman, M.C.; Zerbe, G.O.; Coussons-Read, M.; Ross, R.G.; Laudenslager, M.L. Acculturation, maternal cortisol, and birth outcomes in women of Mexican descent. Psychosom. Med. 2012, 74, 296–304. [Google Scholar] [CrossRef] [Green Version]
- Giesbrecht, G.F.; Campbell, T.; Letourneau, N. Sexually dimorphic adaptations in basal maternal stress physiology during pregnancy and implications for fetal development. Psychoneuroendocrinology 2015, 56, 168–178. [Google Scholar] [CrossRef]
- Gilles, M.; Otto, H.; Wolf, I.A.C.; Scharnholz, B.; Peus, V.; Schredl, M.; Sütterlin, M.W.; Witt, S.H.; Rietschel, M.; Laucht, M.; et al. Maternal hypothalamus-pituitary-adrenal (HPA) system activity and stress during pregnancy: Effects on gestational age and infant’s anthropometric measures at birth. Psychoneuroendocrinology 2018, 94, 152–161. [Google Scholar] [CrossRef]
- Guardino, C.M.; Schetter, C.D.; Saxbe, D.E.; Adam, E.K.; Ramey, S.L.; Shalowitz, M.U. Diurnal salivary cortisol patterns prior to pregnancy predict infant birth weight. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2016, 35, 625–633. [Google Scholar] [CrossRef] [Green Version]
- Hompes, T.; Vrieze, E.; Fieuws, S.; Simons, A.; Jaspers, L.; Van Bussel, J.; Schops, G.; Gellens, E.; Van Bree, R.; Verhaeghe, J.; et al. The influence of maternal cortisol and emotional state during pregnancy on fetal intrauterine growth. Pediatric Res. 2012, 72, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Kivlighan, K.T.; DiPietro, J.A.; Costigan, K.A.; Laudenslager, M.L. Diurnal rhythm of cortisol during late pregnancy: Associations with maternal psychological well-being and fetal growth. Psychoneuroendocrinology 2008, 33, 1225–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spicer, J.; Werner, E.; Zhao, Y.; Choi, C.W.; Lopez-Pintado, S.; Feng, T.; Altemus, M.; Gyamfi, C.; Monk, C. Ambulatory assessments of psychological and peripheral stress-markers predict birth outcomes in teen pregnancy. J. Psychosom. Res. 2013, 75, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bublitz, M.H.; Bourjeily, G.; D’Angelo, C.; Stroud, L.R. Maternal Sleep Quality and Diurnal Cortisol Regulation over Pregnancy. Behav. Sleep Med. 2018, 16, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Bublitz, M.H.; Vergara-Lopez, C.; O’Reilly Treter, M.; Stroud, L.R. Association of Lower Socioeconomic Position in Pregnancy with Lower Diurnal Cortisol Production and Lower Birthweight in Male Infants. Clin. Ther. 2016, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smew, A.I.; Hedman, A.M.; Chiesa, F.; Ullemar, V.; Andolf, E.; Pershagen, G.; Almqvist, C. Limited association between markers of stress during pregnancy and fetal growth in ‘Born into Life’, a new prospective birth cohort. Acta Paediatrica 2018, 107, 1003–1010. [Google Scholar] [CrossRef] [Green Version]
- Cherak, S.J.; Giesbrecht, G.F.; Metcalfe, A.; Ronksley, P.E.; Malebranche, M.E. The effect of gestational period on the association between maternal prenatal salivary cortisol and birth weight: A systematic review and meta-analysis. Psychoneuroendocrinology 2018, 94, 49–62. [Google Scholar] [CrossRef]
- Adam, E.K.; Quinn, M.E.; Tavernier, R.; McQuillan, M.T.; Dahlke, K.A.; Gilbert, K.E. Diurnal cortisol slopes and mental and physical health outcomes: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 83, 25–41. [Google Scholar] [CrossRef]
- Stalder, T.; Kirschbaum, C.; Kudielka, B.M.; Adam, E.K.; Pruessner, J.C.; Wüst, S.; Dockray, S.; Smyth, N.; Evans, P.; Hellhammer, D.H.; et al. Assessment of the cortisol awakening response: Expert consensus guidelines. Psychoneuroendocrinology 2016, 63, 414–432. [Google Scholar] [CrossRef]
- Bastain, T.M.; Chavez, T.; Habre, R.; Girguis, M.S.; Grubbs, B.; Toledo-Corral, C.; Amadeus, M.; Farzan, S.F.; Al-Marayati, L.; Lerner, D.; et al. Study Design, Protocol and Profile of the Maternal And Developmental Risks from Environmental and Social Stressors (MADRES) Pregnancy Cohort: A Prospective Cohort Study in Predominantly Low-Income Hispanic Women in Urban Los Angeles. BMC Pregnancy Childbirth 2019, 19, 189. [Google Scholar] [CrossRef] [Green Version]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Clow, A.; Hucklebridge, F.; Stalder, T.; Evans, P.; Thorn, L. The cortisol awakening response: More than a measure of HPA axis function. Neurosci. Biobehav. Rev. 2010, 35, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, S.; McGrath, J.J.; Roy-Gagnon, M.H.; Tu, M.T. Stability of the diurnal cortisol profile in children and adolescents. Psychoneuroendocrinology 2012, 37, 1981–1989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee on Obstetric Practice, American Institute of Ultrasound in Medicine, & Society for Maternal-Fetal Medicine. Committee Opinion No 700: Methods for Estimating the Due Date. Obstet. Gynecol. 2017, 129, e150–e154. [Google Scholar] [CrossRef]
- Koren, G.; Boskovic, R.; Hard, M.; Maltepe, C.; Navioz, Y.; Einarson, A. Motherisk-PUQE (pregnancy-unique quantification of emesis and nausea) scoring system for nausea and vomiting of pregnancy. Am. J. Obstet. Gynecol. 2002, 186, S228–S231. [Google Scholar] [CrossRef]
- Nijm, J.; Kristenson, M.; Olsson, A.G.; Jonasson, L. Impaired cortisol response to acute stressors in patients with coronary disease. Implications for inflammatory activity. J. Intern. Med. 2007, 262, 375–384. [Google Scholar] [CrossRef]
- Saxbe, D. A field (researcher’s) guide to cortisol: Tracking HPA axis functioning in everyday life. Health Psychol. Rev. 2008, 2, 163–190. [Google Scholar] [CrossRef]



| Characteristic | N (%) or Mean (SD) |
|---|---|
| Maternal | |
| Age (years) | 29.1 (5.8) |
| Race | |
| White | 206 (86.2%) |
| Black/African-American | 24 (10.1%) |
| Asian | 2 (0.8%) |
| American Indian/Alaskan Native | 1 (0.4%) |
| >1 race | 6 (2.5%) |
| Ethnicity | |
| Hispanic | 195 (81.3%) |
| Non-Hispanic | 45 (18.7%) |
| Highest Education Level | |
| Less than 12th grade | 57 (23.8%) |
| High School | 76 (31.7%) |
| Some college or technical school | 59 (24.6%) |
| Complete 4 years of college | 32 (13.3%) |
| Some graduate training | 16 (6.6%) |
| Household Annual Income | |
| Less than $15,000 | 48 (20.0%) |
| $15,000–$29,999 | 65 (27.1%) |
| $30,000–$49,999 | 38 (15.8%) |
| $50,000–$99,999 | 13 (5.4%) |
| $100,000 or more | 14 (5.8%) |
| Selected “Don’t Know” | 62 (25.8%) |
| Pre-Pregnancy BMI (kg/m2) | 29.1 (6.9) |
| Infant | |
| Female | 131 (54.6%) |
| Birth weight (g) | 3301.7 (497.3) |
| Low birth weight (<2500 g) | 11 (4.6%) |
| Gestational age at birth (weeks) | 39.0 (1.5) |
| Preterm birth (<37 weeks gestation) | 23 (9.6%) |
| Birth Order | |
| First Born | 85 (35.4%) |
| Second Born | 68 (28.3%) |
| Third Born | 41 (17.1%) |
| Fourth Born or more | 37 (15.4%) |
| Unknown | 9 (3.8%) |
| Type of Delivery | |
| Vaginal | 179 (74.6%) |
| Cesarean section | 61 (25.4%) |
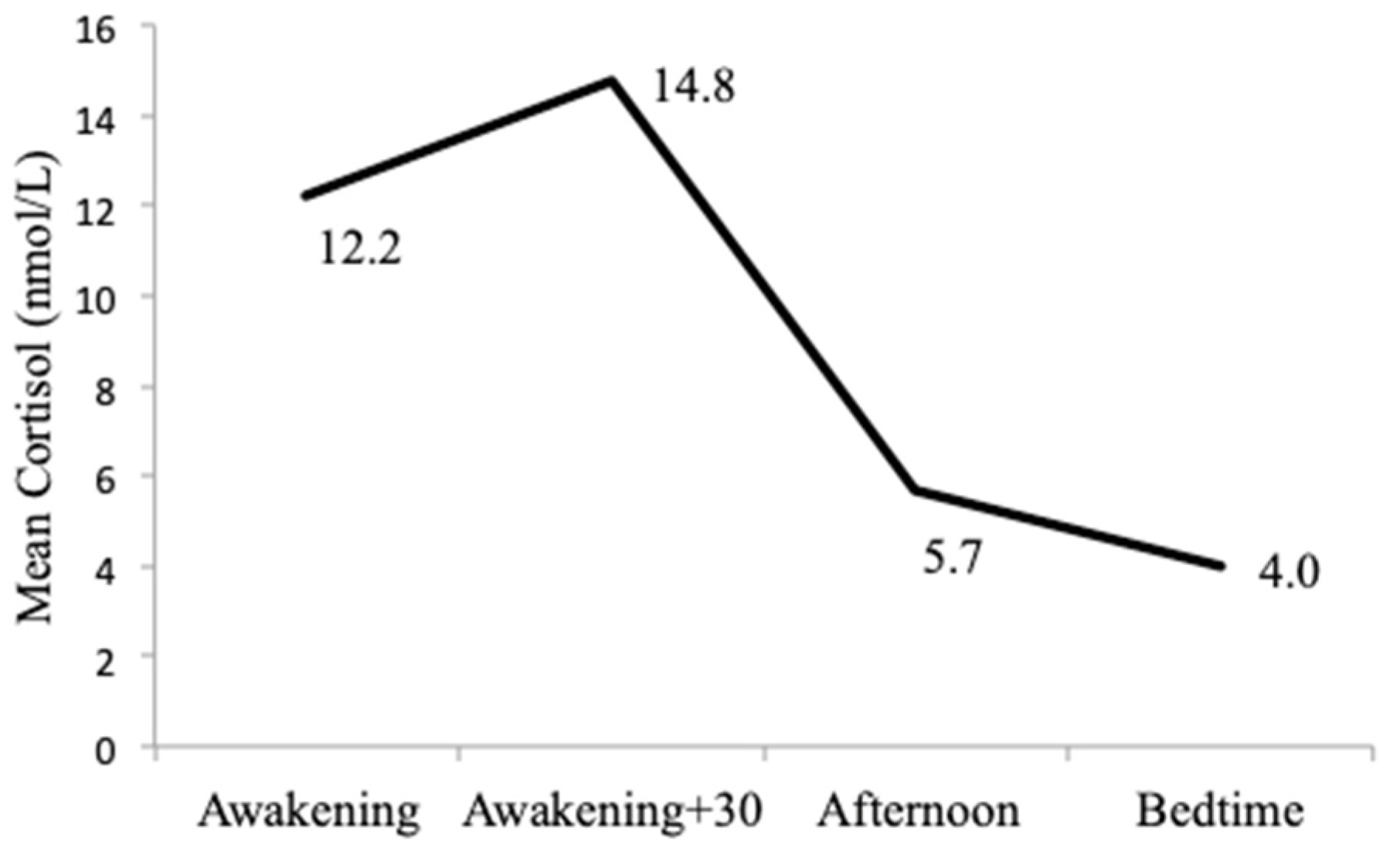
| Stress Metric | Mean (SD) * | Median * | Min-Max |
|---|---|---|---|
| Awakening Sample (nmol/L) | 12.2 (7.7) | 11.0 | 0.9–75.9 |
| Awakening + 30 min Sample (nmol/L) | 14.8 (9.6) | 13.3 | 1.1–73.5 |
| Afternoon Sample (nmol/L) | 5.7 (4.8) | 4.4 | 0.8–29.7 |
| Bedtime Sample (nmol/L) | 4.0 (4.4) | 2.6 | 0.8–30.0 |
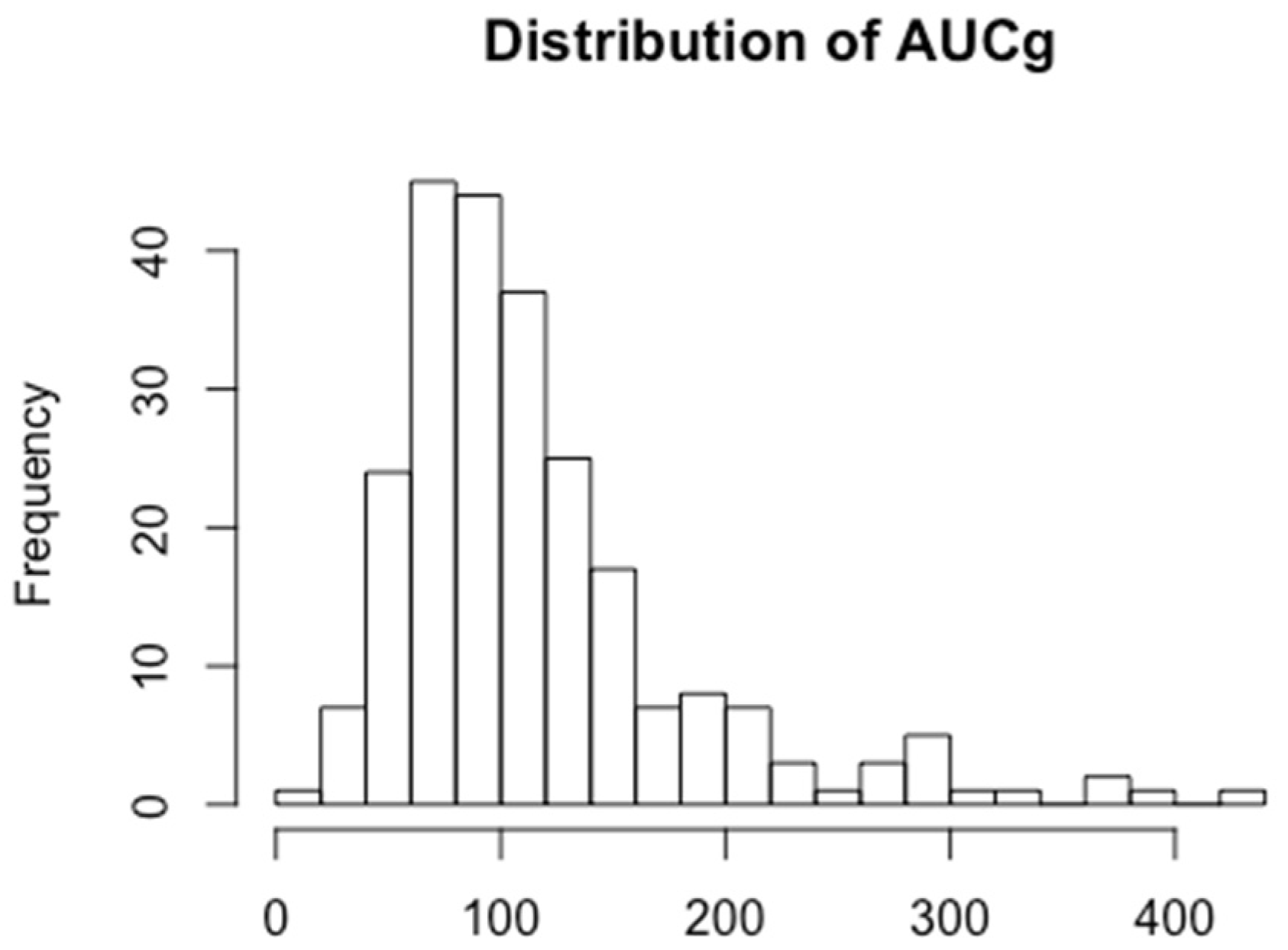
| Area Under the Curve, grounded (AUCg) | 116.7 (67.9) | 99.9 | 13.3–424.9 |
| Cortisol Awakening Response (CAR) | 0.7 (1.8) | 0.4 | −5.7–9.8 |
| Diurnal Cortisol Slope (DCS) | −0.6 (0.6) | −0.6 | −4.7–1.1 |
| Individual Biological Stress Metric | β (SE) | p |
|---|---|---|
| Area Under the Curve, grounded (AUCg) *,1 | −5.6 (5.1) | 0.25 |
| Cortisol Awakening Response (CAR) * | −0.4 (15.3) | 0.98 |
| Diurnal Cortisol Slope (DCS) * | 78.3 (44.9) | 0.08 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peterson, A.K.; Toledo-Corral, C.M.; Chavez, T.A.; Naya, C.H.; Johnson, M.; Eckel, S.P.; Lerner, D.; Grubbs, B.H.; Farzan, S.F.; Dunton, G.F.; et al. Prenatal Maternal Cortisol Levels and Infant Birth Weight in a Predominately Low-Income Hispanic Cohort. Int. J. Environ. Res. Public Health 2020, 17, 6896. https://doi.org/10.3390/ijerph17186896
Peterson AK, Toledo-Corral CM, Chavez TA, Naya CH, Johnson M, Eckel SP, Lerner D, Grubbs BH, Farzan SF, Dunton GF, et al. Prenatal Maternal Cortisol Levels and Infant Birth Weight in a Predominately Low-Income Hispanic Cohort. International Journal of Environmental Research and Public Health. 2020; 17(18):6896. https://doi.org/10.3390/ijerph17186896
Chicago/Turabian StylePeterson, Alicia K., Claudia M. Toledo-Corral, Thomas A. Chavez, Christine H. Naya, Mark Johnson, Sandrah P. Eckel, Deborah Lerner, Brendan H. Grubbs, Shohreh F. Farzan, Genevieve F. Dunton, and et al. 2020. "Prenatal Maternal Cortisol Levels and Infant Birth Weight in a Predominately Low-Income Hispanic Cohort" International Journal of Environmental Research and Public Health 17, no. 18: 6896. https://doi.org/10.3390/ijerph17186896
APA StylePeterson, A. K., Toledo-Corral, C. M., Chavez, T. A., Naya, C. H., Johnson, M., Eckel, S. P., Lerner, D., Grubbs, B. H., Farzan, S. F., Dunton, G. F., Bastain, T. M., & Breton, C. V. (2020). Prenatal Maternal Cortisol Levels and Infant Birth Weight in a Predominately Low-Income Hispanic Cohort. International Journal of Environmental Research and Public Health, 17(18), 6896. https://doi.org/10.3390/ijerph17186896