Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
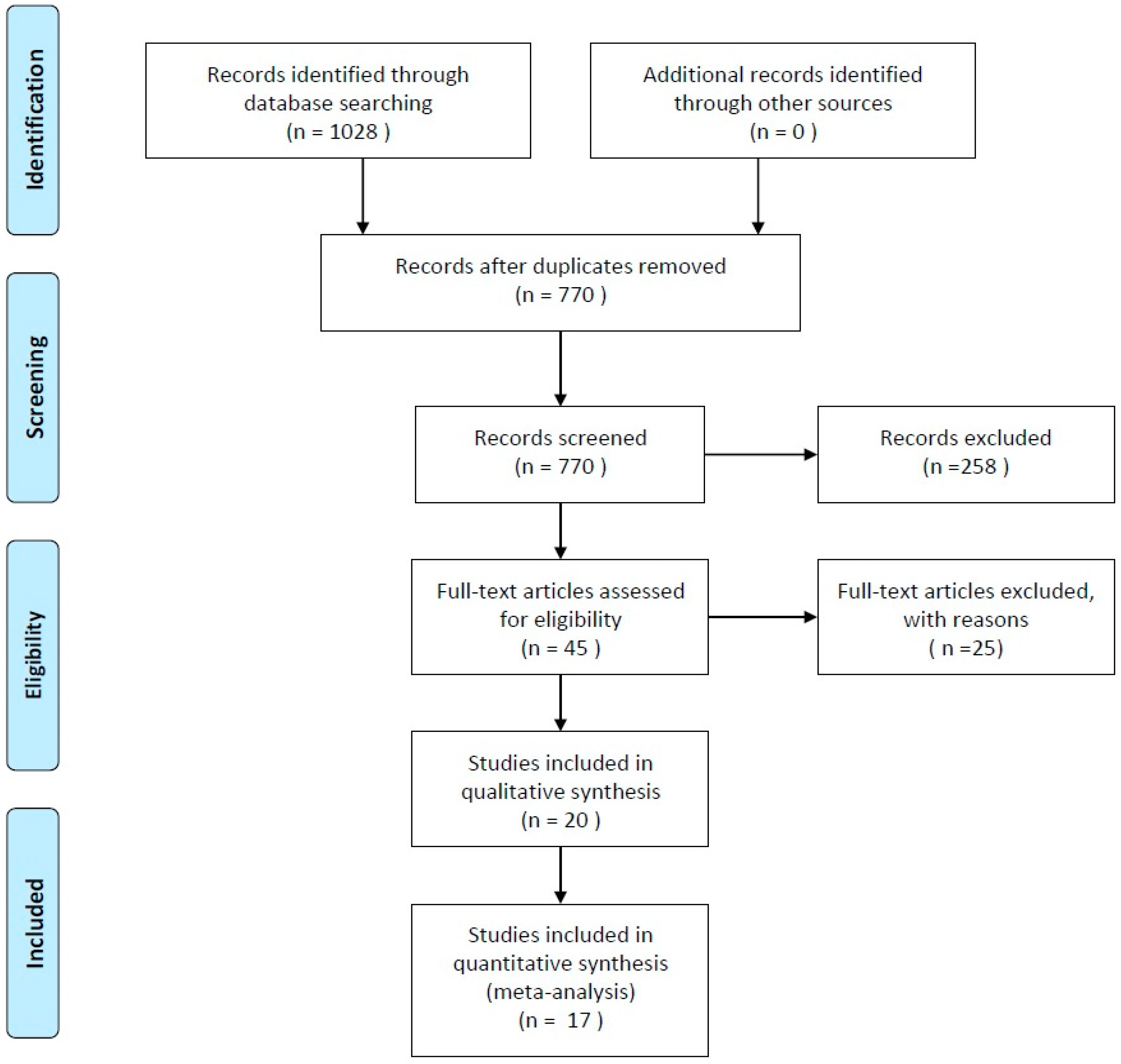
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
- ▪
- Comparison of different neck/shoulder position (One-piece vs. two-pieces or tissue-level or transmucosal vs. bone-level) of dental implants with at least 1-year follow-up after loading;
- ▪
- Patients aged between 18 and 70 years old;
- ▪
- Patients without severe systemic (e.g., recent cardiovascular event or tumoral pathology) or psychiatric disease;
- ▪
- Clinical and radiological parameters measured were at least respectively bleeding on probing (BoP), and marginal bone loss (∆MBL);
- ▪
- Only studies published in English.
- ▪
- Studies included orthodontics patients;
- ▪
- Studies included patients with disabilities;
- ▪
- Studies included patients who are taking bisphosphonates;
- ▪
- Studies comparing two or more different types of implant-abutment connections (e.g., switching platform) not focusing on position related to the bone;
- ▪
- Studies comparing two or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone;
- ▪
- Studies comparing two or more different types of implant or abutment micro design;
- ▪
- Studies comparing two or more different types of micro design of the implant neck or of the abutment;
- ▪
- Final timepoint after less than 1 year after loading;
- ▪
- Studies evaluating short-implants (in literature defined as implant <8.5 mm) [14];
- ▪
- Studies analyzing implants and abutments used to retain removable prosthesis;
- ▪
- Studies published before 1990;
- ▪
- Duplicated studies or studies with different time points were included only one time with the longest duration.
2.3. Screening and Study Selection
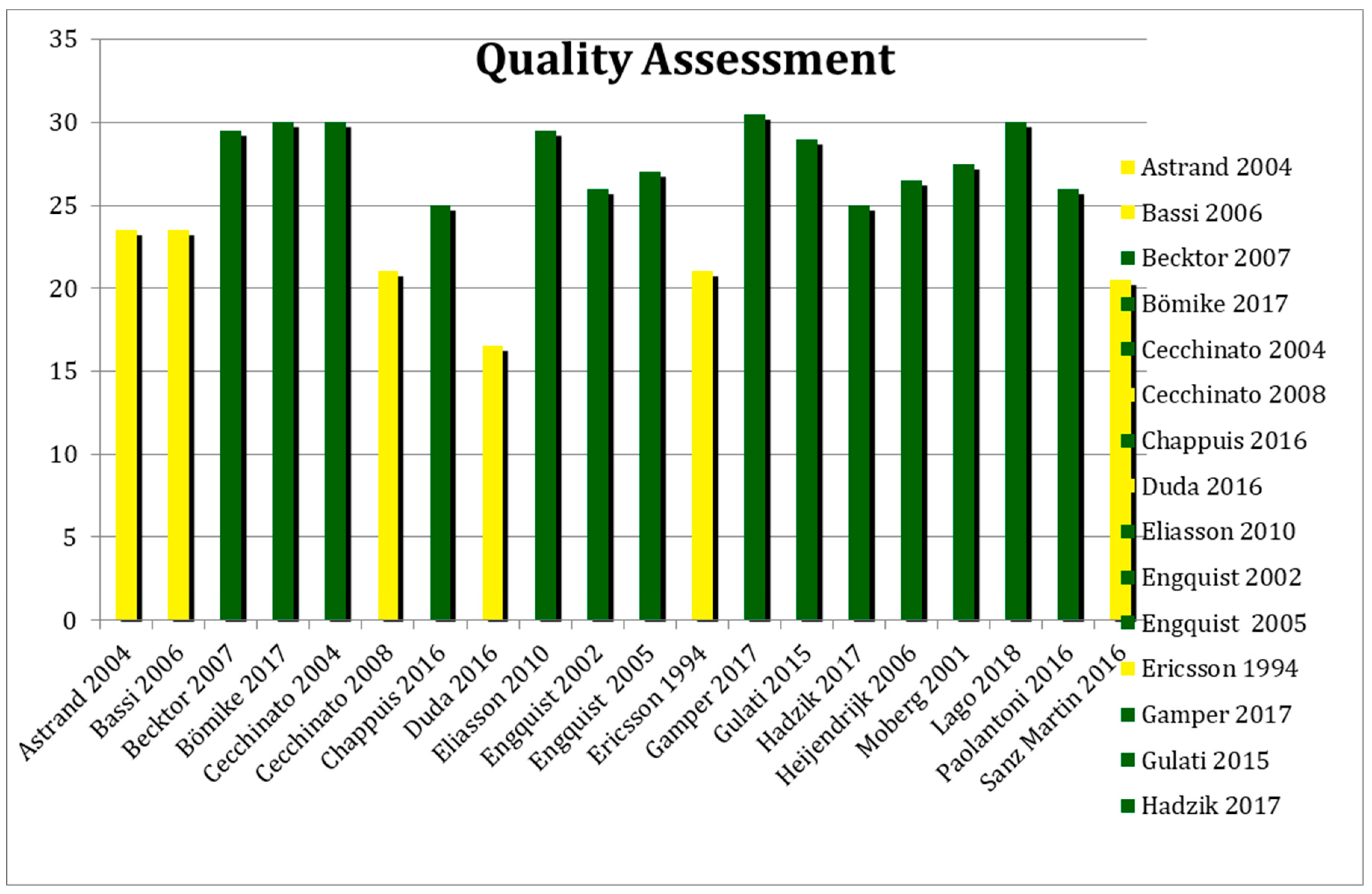
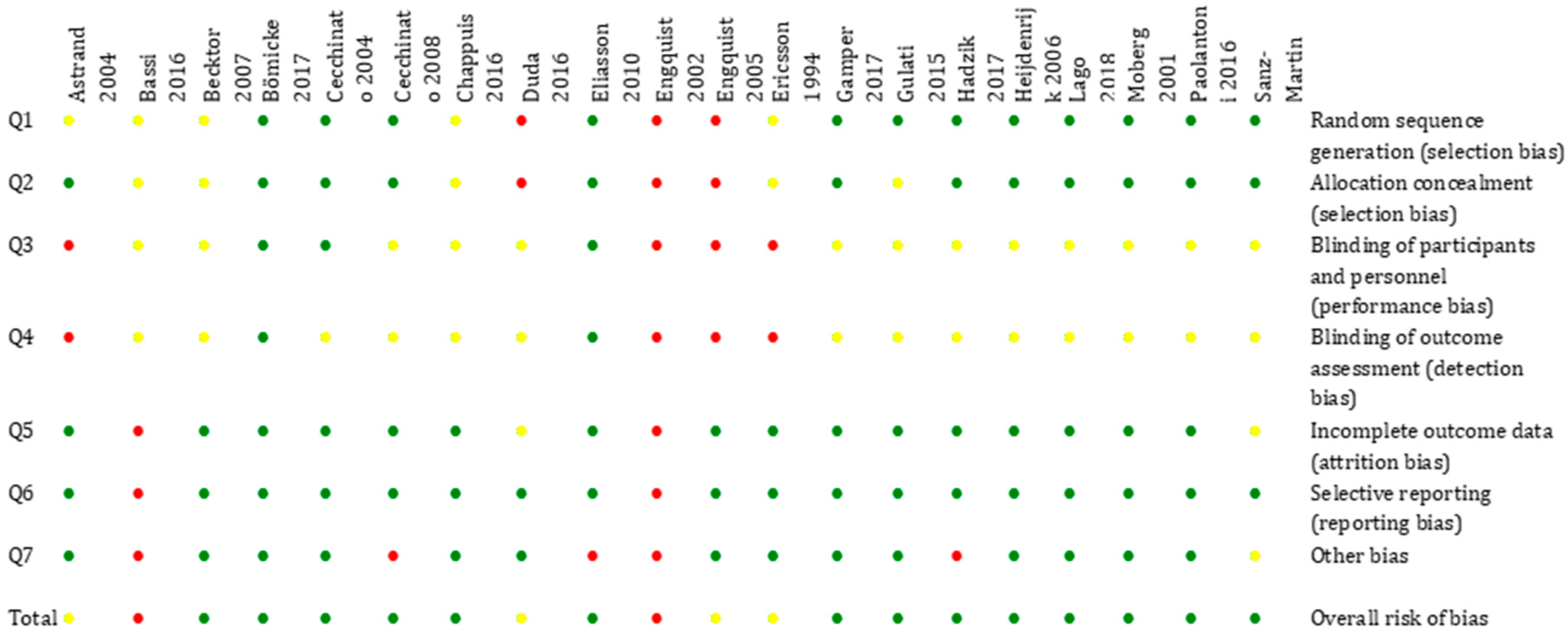
2.4. Quality Assessment (Risk of Bias of Included RCTs)
- Random sequence generation,
- Allocation concealment,
- Blinding of participants, personnel, and outcomes assessors,
- Incomplete outcome data,
- Selective outcome reporting.
2.5. Quantitative Analysis
3. Results
3.1. Qualitative Analysis
3.2. Quality Assessment
3.3. Quantitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BIC | Bone to Implant Contact |
| BL | Bone-Level (Implants) |
| BoP | Bleeding on Probing |
| PPD | Pocked Probing Depth |
| IAJ | Implant-Abutment Junction |
| ∆MBL | Marginal Bone Loss |
| RCTs | Randomized Clinical Trials |
| TL | Tissue-Level (Implants) |
References
- Buser, D.; Janner, S.F.M.; Wittneben, J.-G.; Bragger, U.; Ramseier, C.A.; Salvi, G. 10-Year Survival and Success Rates of 511 Titanium Implants with a Sandblasted and Acid-Etched Surface: A Retrospective Study in 303 Partially Edentulous Patients. Clin. Implant. Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Nagahisa, K.; Arai, K.; Baba, S. Study on Oral Health–Related Quality of Life in Patients after Dental Implant Treatment with Patient-Reported Outcome. Int. J. Oral Maxillofac. Implant. 2018, 33, 1141–1148. [Google Scholar] [CrossRef]
- Barone, A.; Toti, P.; Marconcini, S.; Derchi, G.; Saverio, M.; Covani, U. Esthetic Outcome of Implants Placed in Fresh Extraction Sockets by Clinicians with or without Experience: A Medium-Term Retrospective Evaluation. Int. J. Oral Maxillofac. Implant. 2016, 31, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Eckert, S.; Hueler, G.; Sandler, N.; Elkattah, R.; McNeil, D. Immediately Loaded Fixed Full-Arch Implant-Retained Prosthesis: Clinical Analysis When Using a Moderate Insertion Torque. Int. J. Oral Maxillofac. Implant. 2019, 34, 737–744. [Google Scholar] [CrossRef]
- Barone, A.; Covani, U. Maxillary alveolar ridge reconstruction with nonvascularized autogenous block bone: clinical results. J. Oral Maxillofac. Surg. 2007, 65, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Grassi, F.R.; Grassi, R.; Vivarelli, L.; Dallari, D.; Nardi, G.M.; Govoni, M.; Kalemaj, Z.; Ballini, A. Design Techniques to Optimize the Scaffold Performance: Freeze-dried Bone Custom-made Allografts for Maxillary Alveolar Horizontal Ridge Augmentation. Materials 2020, 13, 1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermann, F.; Lerner, H.; Palti, A. Factors Influencing the Preservation of the Periimplant Marginal Bone. Implant. Dent. 2007, 16, 165–175. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, A.; Van Der Zypen, E.; Stich, H.; Sutter, F. The reactions of bone, connective tissue, and epithelium to endosteal implants with titanium-sprayed surfaces. J. Maxillofac. Surg. 1981, 9, 15–25. [Google Scholar] [CrossRef]
- Hermann, J.S.; Buser, D.; Schenk, R.K.; Higginbottom, F.L.; Cochran, D.L. Biologic width around titanium implants. A physiologically formed and stable dimension over time. Clin. Oral Implant. Res. 2000, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Iglhaut, G.; Schwarz, F.; Winter, R.R.; Mihatovic, I.; Stimmelmayr, M.; Schliephake, H. Epithelial Attachment and Downgrowth on Dental Implant Abutments-A Comprehensive Review. J. Esthet. Restor. Dent. 2014, 26, 324–331. [Google Scholar] [CrossRef]
- Welch, V.; Petticrew, M.; Tugwell, P.; Moher, D.; O’Neill, J.; Waters, E.; White, H. PRISMA-Equity 2012 Extension: Reporting Guidelines for Systematic Reviews with a Focus on Health Equity. PLoS Med. 2012, 9, e1001333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, C.K.; Thorwarth, M.; Schultze-Mosgau, S. Influence of insertion protocol and implant shoulder design on inflammatory infiltration and gene expression in peri-implant soft tissue during nonsubmerged dental implant healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e11–e19. [Google Scholar] [CrossRef] [PubMed]
- Merickse-Stern, R.; Aerni, D.; Geering, A.H.; Buser, D. Long-term evaluation of non-submerged hollow cylinder implants. Clinical and radiographic results. Clin. Oral Implant. Res. 2001, 12, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Zadeh, H.; Stanford, C.M.; Cooper, L.F. Survival of short dental implants for treatment of posterior partial edentulism: A systematic review. Int. J. Oral Maxillofac. Implant. 2012, 27, 1323–1331. [Google Scholar]
- Becktor, J.P.; Isaksson, S.; Billström, C. A Prospective Multicenter Study Using Two Different Surgical Approaches in the Mandible with Turned Brånemark Implants: Conventional Loading Using Fixed Prostheses. Clin. Implant. Dent. Relat. Res. 2007, 9, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Bratu, E.A.; Tandlich, M.; Shapira, L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: a prospective clinical study [published correction appears in Clin Oral Implants Res. 2009 Oct;20(10):1185]. Clin. Oral Implants Res. 2009, 20, 827–832. [Google Scholar] [CrossRef]
- de Siqueira, R.A.C.; Fontão, F.N.G.K.; Sartori, I.A.M.; Santos, P.G.F.; Bernardes, S.R.; Tiossi, R. Effect of different implant placement depths on crestal bone levels and soft tissue behavior: a randomized clinical trial. Clin. Oral Implants Res. 2017, 28, 1227–1233. [Google Scholar] [CrossRef]
- Chappuis, V.; Bornstein, M.M.; Buser, D.; Belser, U. Influence of implant neck design on facial bone crest dimensions in the esthetic zone analyzed by cone beam CT: A comparative study with a 5-to-9-year follow-up. Clin. Oral Implant. Res. 2016, 27, 1055–1064. [Google Scholar] [CrossRef]
- Chien, H.H.; Schroering, R.L.; Prasad, H.S. Tatakis DN. Effects of a new implant abutment design on peri-implant soft tissues. J. Oral Implantol. 2014, 40, 581–588. [Google Scholar] [CrossRef]
- Cosyn, J.; Sabzevar, M.M.; De Wilde, P.; De Rouck, T. Two-piece implants with turned versus microtextured collars. J. Periodontol. 2007, 78, 1657–1663. [Google Scholar] [CrossRef]
- Ebler, S.; Ioannidis, A.; Jung, R.E.; Hämmerle, C.H.; Thoma, D.S. Prospective randomized controlled clinical study comparing two types of two-piece dental implants supporting fixed reconstructions—Results at 1 year of loading. Clin. Oral Implants Res. 2016, 27, 1169–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, M.; Trullenque-Eriksson, A.; Blasone, R.; Blasone, R.; Malaguti, G.; Gaffuri, C.; Caneva, M.; Minciarelli, A.; Luongo, G. Clinical evaluation of a novel dental implant system as single implants under immediate loading conditions—4-month post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2016, 9, 367–379. [Google Scholar] [PubMed]
- Hof, M.; Pommer, B.; Strbac, G.D.; Vasak, C.; Agis, H.; Zechner, W. Impact of insertion torque and implant neck design on peri-implant bone level: a randomized split-mouth trial. Clin. Implant Dent. Relat. Res. 2014, 16, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Climent, M.; Romero-Ruiz, M.M.; Díaz-Castro, C.M.; Bullón, P.; Ríos-Santos, J.V. Influence of two different machined-collar heights on crestal bone loss. Int. J. Oral Maxillofac. Implants 2014, 29, 1374–1379. [Google Scholar] [CrossRef] [Green Version]
- Judgar, R.; Giro, G.; Zenobio, E.; Coelho, P.G.; Feres, M.; Rodrigues, J.A.; Mangano, C.; Iezzi, G.; Piattelli, A.; Shibli, J.A. Biological width around one- and two-piece implants retrieved from human jaws. BioMed. Res. Int. 2014, 4, 850120. [Google Scholar] [CrossRef]
- Khorsand, A.; Rasouli-Ghahroudi, A.A.; Naddafpour, N.; Shayesteh, Y.S.; Khojasteh, A. Effect of Microthread Design on Marginal Bone Level Around Dental Implants Placed in Fresh Extraction Sockets. Implant Dent. 2016, 25, 90–96. [Google Scholar] [CrossRef]
- Khraisat, A.; Zembic, A.; Jung, R.E.; Hammerle, C.H. Marginal bone levels and soft tissue conditions around single-tooth implants with a scalloped neck design: results of a prospective 3-year study. Int. J. Oral. Maxillofac. Implants 2013, 28, 550–555. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.J.; Lee, D.W.; Kim, C.K.; Park, K.H.; Moon, I.S. Effect of conical configuration of fixture on the maintenance of marginal bone level: preliminary results at 1 year of function. Clin. Oral Implants Res. 2010, 21, 439–444. [Google Scholar] [CrossRef]
- Kütan, E.; Bolukbasi, N.; Yildirim-Ondur, E.; Ozdemir, T. Clinical and Radiographic Evaluation of Marginal Bone Changes around Platform-Switching Implants Placed in Crestal or Subcrestal Positions: A Randomized Controlled Clinical Trial. Clin. Implant Dent. Relat. Res. 2015, 17, e364–e375. [Google Scholar] [CrossRef]
- Marconcini, S.; Giammarinaro, E.; Toti, P.; Alfonsi, F.; Covani, U.; Barone, A. Longitudinal analysis on the effect of insertion torque on delayed single implants: A 3-year randomized clinical study. Clin. Implant Dent. Relat. Res. 2018, 20, 322–332. [Google Scholar] [CrossRef]
- Moberg, L.-E.; Sagulin, G.-B.; Köndell, P.-Å.; Heimdahl, A.; Gynther, G.W.; Bolin, A. Branemark System and ITI Dental Implant System for treatment of mandibular edentulism. A comparative randomized study: 3-year follow-up. Clin. Oral Implant. Res. 2001, 12, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Nóvoa, L.; Batalla, P.; Caneiro, L.; Pico, A.; Liñares, A.; Blanco, J. Influence of Abutment Height on Maintenance of Peri-implant Crestal Bone at Bone-Level Implants: A 3-Year Follow-up Study. Int. J. Periodontics Restorative Dent. 2017, 37, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Ormianer, Z.; Duda, M.; Block, J.; Matalon, S. One- and Two-Piece Implants Placed in the Same Patients: Clinical Outcomes After 5 Years of Function. Int. J. Prosthodont. 2015, 29, 608–610. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Chover, H.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D.; Gomar-Vercher, S.; Agustín-Panadero, R.; Peñarrocha-Diago, M. Impact of crestal and subcrestal implant placement in peri-implant bone: A prospective comparative study. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e103–e110. [Google Scholar] [CrossRef]
- Peñarrocha-Diago, M.A.; Flichy-Fernández, A.J.; Alonso-González, R.; Peñarrocha-Oltra, D.; Balaguer-Martínez, J.; Peñarrocha-Diago, M. Influence of implant neck design and implant-abutment connection type on peri-implant health. Radiological study. Clin. Oral. Implants Res. 2013, 24, 1192–1200. [Google Scholar] [CrossRef]
- Pozzi, A.; Agliardi, E.; Tallarico, M.; Barlattani, A. Clinical and radiological outcomes of two implants with different prosthetic interfaces and neck configurations: randomized, controlled, split-mouth clinical trial. Clin. Implant Dent. Relat. Res. 2014, 16, 96–106. [Google Scholar] [CrossRef]
- Pozzi, A.; Tallarico, M.; Moy, P.K. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with different prosthetic interfaces and design in partially posterior edentulous mandibles. Eur. J. Oral Implantol. 2014, 7, 47–61. [Google Scholar]
- Sanz-Martin, I.; Vignoletti, F.; Nuñez, J.; Permuy, M.; Muñoz, F.; Sanz-Esporrín, J.; Fierravanti, L.; Shapira, L.; Sanz, M. Hard and soft tissue integration of immediate and delayed implants with a modified coronal macrodesign: Histological, micro-CT and volumetric soft tissue changes from a pre-clinical in vivo study. J. Clin. Periodontol. 2017, 44, 842–853. [Google Scholar] [CrossRef]
- Shin, Y.K.; Han, C.H.; Heo, S.J.; Kim, S.; Chun, H.J. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year. Int. J. Oral Maxillofac. Implants 2006, 21, 789–794. [Google Scholar]
- Tan, W.C.; Lang, N.P.; Schmidlin, K.; Zwahlen, M.; Pjetursson, B.E. The effect of different implant neck configurations on soft and hard tissue healing: a randomized-controlled clinical trial. Clin. Oral Implants Res. 2011, 22, 14–19. [Google Scholar] [CrossRef]
- Weinländer, M.; Lekovic, V.; Spadijer-Gostovic, S.; Milicic, B.; Wegscheider, W.A.; Piehslinger, E. Soft tissue development around abutments with a circular macro-groove in healed sites of partially edentulous posterior maxillae and mandibles: a clinical pilot study. Clin. Oral Implants Res. 2011, 22, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Wittneben, J.G.; Gavric, J.; Belser, U.C.; Bornstein, M.M.; Joda, T.; Chappuis, V.; Sailer, I.; Brägger, U. Esthetic and Clinical Performance of Implant-Supported All-Ceramic Crowns Made with Prefabricated or CAD/CAM Zirconia Abutments: A Randomized, Multicenter Clinical Trial. J. Dent. Res. 2017, 96, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Åstrand, P.; Engquist, B.; Anzén, B.; Bergendal, T.; Hallman, M.; Karlsson, U.; Kvint, S.; Lysell, L.; Rundcranz, T. A Three-Year Follow-Up Report of a Comparative Study of ITI Dental Implants® and Brånemark System® Implants in the Treatment of the Partially Edentulous Maxilla. Clin. Implant Dent. Relat. Res. 2004, 6, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Bassi, M.A.; Lopez, M.A.; Confalone, L.; Gaudio, R.M.; Lombardo, L.; Lauritano, D. A prospective evaluation of outcomes of two tapered implant systems. J. Biol. Regul. Homeost. Agents 2016, 30, 1–6. [Google Scholar]
- Bömicke, W.; Gabbert, O.; Koob, A.; Krisam, J.; Rammelsberg, P. Comparison of immediately loaded flapless-placed one-piece implants and flapped-placed conventionally loaded two-piece implants, both fitted with all-ceramic single crowns, in the posterior mandible: 3-year results from a randomised controlled pilot trial. Eur. J. Oral Implantol. 2017, 10, 179–195. [Google Scholar]
- Cecchinato, D.; Olsson, C.; Lindhe, J. Submerged or non-submerged healing of endosseous implants to be used in the rehabilitation of partially dentate patients. J. Clin. Periodontol. 2004, 31, 299–308. [Google Scholar] [CrossRef]
- Cecchinato, D.; Bengazi, F.; Blasi, G.; Botticelli, D.; Cardarelli, I.; Gualini, F. Bone level alterations at implants placed in the posterior segments of the dentition: Outcome of submerged/non-submerged healing. A 5-year multicenter, randomized, controlled clinical trial. Clin. Oral Implant. Res. 2008, 19, 429–431. [Google Scholar] [CrossRef]
- Duda, M.; Matalon, S.; Lewinstein, I.; Harel, N.; Block, J.; Ormianer, Z. One Piece Immediately Loaded Implants Versus 1 Piece or 2 Pieces Delayed: 3 Years Outcome. Implant Dent. 2016, 25, 109–113. [Google Scholar] [CrossRef]
- Eliasson, A.; Narby, B.; Ekstrand, K.; Hirsch, J.; Johansson, A.; Wennerberg, A. A 5-year prospective clinical study of submerged and nonsubmerged Paragon system implants in the edentulous mandible. Int. J. Prosthodont. 2010, 23, 231–238. [Google Scholar]
- Engquist, B.; Astrand, P.; Anzén, B.; Dahlgren, S.; Engquist, E.; Feldmann, H.; Karlsson, U.; Nord, P.G.; Sahlholm, S.; Svärdström, P. Simplified methods of implant treatment in the edentulous lower jaw. A controlled prospective study. Part I: One-stage versus two-stage surgery. Clin. Implant Dent. Relat. Res. 2002, 4, 93–103. [Google Scholar] [CrossRef]
- Engquist, B.; Astrand, P.; Anzén, B.; Dahlgren, S.; Engquist, E.; Feldmann, H.; Karlsson, U.; Nord Dds, P.; Sahlholm, S.; Svärdström, P. Simplified Methods of Implant Treatment in the Edentulous Lower Jaw: A 3-Year Follow-Up Report of a Controlled Prospective Study of One-Stage versus Two-Stage Surgery and Early Loading. Clin. Implant Dent. Relat. Res. 2005, 7, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I.; Randow, K.; Glantz, P.-O.; Lindhe, J.; Nilner, K. Clinical and radiographical features of submerged and nonsubmerged titanium implants. Clin. Oral Implant. Res. 1994, 5, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Gamper, F.B.; Benic, G.I.; Sanz-Martín, I.; Asgeirsson, A.G.; Hämmerle, C.H.F.; Thoma, D.S. Randomized controlled clinical trial comparing one-piece and two-piece dental implants supporting fixed and removable dental prostheses: 4- to 6-year observations. Clin. Oral Implant. Res. 2017, 28, 1553–1559. [Google Scholar] [CrossRef] [Green Version]
- Gulati, M.; Govila, V.; Verma, S.; Rajkumar, B.; Anand, V.; Aggarwal, A.; Jain, N. In Vivo Evaluation of Two-Piece Implants Placed Following One-Stage and Two-Stage Surgical Protocol in Posterior Mandibular Region. Assessment of Alterations in Crestal Bone Level. Clin. Implant Dent. Relat. Res. 2015, 17, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Hadzik, J.; Botzenhart, U.; Krawiec, M.; Gedrange, T.; Heinemann, F.; Vegh, A.; Dominiak, M. Comparative evaluation of the effectiveness of the implantation in the lateral part of the mandible between short tissue level (TE) and bone level (BL) implant systems. Ann. Anat. 2017, 213, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Heijdenrijk, K.; Raghoebar, G.M.; Meijer, H.J.A.; Stegenga, B.; Van Der Reijden, W.A. Feasibility and Influence of the Microgap of Two Implants Placed in a Non-Submerged Procedure: A Five-Year Follow-Up Clinical Trial. J. Periodontol. 2006, 77, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Lago, L.; Da Silva, L.; Martínez-Silva, I.; Rilo, B. Crestal Bone Level Around Tissue-Level Implants Restored with Platform Matching and Bone-Level Implants Restored with Platform Switching: A 5-Year Randomized Controlled Trial. Int. J. Oral Maxillofac. Implant. 2018, 33, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Paoloantoni, G.; Marenzi, G.; Blasi, A.; Mignogna, J.; Sammartino, G. Findings of a Four-Year Randomized Controlled Clinical Trial Comparing Two-Piece and One-Piece Zirconia Abutments Supporting Single Prosthetic Restorations in Maxillary Anterior Region. BioMed Res. Int. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sanz-Martín, I.; Benic, G.I.; Hämmerle, C.H.; Thoma, D.S. Prospective randomized controlled clinical study comparing two dental implant types: Volumetric soft tissue changes at 1 year of loading. Clin. Oral Implant. Res. 2016, 27, 406–411. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Mallen, C.; Peat, G.; Croft, P. Quality assessment of observational studies is not commonplace in systematic reviews. J. Clin. Epidemiol. 2006, 59, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, U.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Sánchez, I.; Sanz-Martín, I.; De Albornoz, A.C.; Figuero, E.; Sanz, M. Biological effect of the abutment material on the stability of peri-implant marginal bone levels: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 124–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Martín, I.; Sanz-Sánchez, I.; De Albornoz, A.C.; Figuero, E.; Sanz, M. Effects of modified abutment characteristics on peri-implant soft tissue health: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 118–129. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Christensen, A.-E.; Lorenzen, H. Scalloped Implant-Abutment Connection Compared to Conventional Flat Implant-Abutment Connection: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Res. 2017, 8, e2. [Google Scholar] [CrossRef]
- Tallarico, M.; Caneva, M.; Meloni, S.M.; Xhanari, E.; Omori, Y.; Canullo, L. Survival and Success Rates of Different Shoulder Designs: A Systematic Review of the Literature. Int. J. Dent. 2018, 2018, 1–10. [Google Scholar] [CrossRef]
- Palacios-Garzón, N.; Velasco-Ortega, E.; López-López, J. Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials 2019, 12, 154. [Google Scholar] [CrossRef] [Green Version]
- Degidi, M.; Artese, L.; Piattelli, A.; Scarano, A.; Shibli, J.A.; Piccirilli, M.; Perrotti, V.; Iezzi, G. Histological and immunohistochemical evaluation of the peri-implant soft tissues around machined and acid-etched titanium healing abutments: A prospective randomised study. Clin. Oral Investig. 2012, 16, 857–866. [Google Scholar] [CrossRef]
- Coli, P.; Sennerby, L. Is Peri-Implant Probing Causing Over-Diagnosis and Over-Treatment of Dental Implants? J. Clin. Med. 2019, 8, 1123. [Google Scholar] [CrossRef]
- Broggini, N.; McManus, L.; Hermann, J.; Medina, R.; Oates, T.; Schenk, R.; Buser, D.; Mellonig, J.; Cochran, D. Persistent acute inflammation at the implant-abutment interface. J. Dent. Res. 2003, 82, 232–237. [Google Scholar] [CrossRef]
- Buser, D.; Weber, H.P.; Donath, K.; Fiorellini, J.P.; Paquette, D.W.; Williams, R.C. Soft Tissue Reactions to Non-Submerged Unloaded Titanium Implants in Beagle Dogs. J. Periodontol. 1992, 63, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Marcos, G.; Hernández-Herrera, M.; Anitua, E. Marginal Bone Loss around Short Dental Implants Restored at Implant Level and with Transmucosal Abutment: A Retrospective Study. Int. J. Oral Maxillofac. Implant. 2018, 33, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Winitsky, N.; Olgart, K.; Jemt, T.; Smedberg, J.-I. A retro-prospective long-term follow-up of Brånemark single implants in the anterior maxilla in young adults. Part 1: Clinical and radiographic parameters. Clin. Implant Dent. Relat. Res. 2018, 20, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Penarrocha-Oltra, D.; Soldini, C.; Mazzocco, F.; Peñarrocha, M.; Covani, U. Microbiological assessment of the implant-abutment interface in different connections: Cross-sectional study after 5 years of functional loading. Clin. Oral Implant. Res. 2015, 26, 426–434. [Google Scholar] [CrossRef]
- Schwarz, F.; Alcoforado, G.; Nelson, K.; Schaer, A.; Taylor, T.; Beuer, F.; Strietzel, F.P. Impact of implant–abutment connection, positioning of the machined collar/microgap, and platform switching on crestal bone level changes. Camlog Foundation Consensus Report. Clin. Oral Implant. Res. 2014, 25, 1301–1303. [Google Scholar] [CrossRef]
- Fransson, C.; Wennström, J.; Berglundh, T. Clinical characteristics and implant with a history of progressive bone loss. Clin. Oral Implant. Res. 2008, 19, 142–147. [Google Scholar] [CrossRef]
- Hashim, D.; Cionca, N.; Combescure, C.; Mombelli, A. The diagnosis of peri-implantitis: A systematic review on the predictive value of bleeding on probing. Clin. Oral Implant. Res. 2018, 29, 276–293. [Google Scholar] [CrossRef] [Green Version]
- French, D.; Cochran, D.L.; Ofec, R. Retrospective Cohort Study of 4591 Straumann Implants Placed in 2060 Patients in Private Practice with up to 10-Year Follow-up: The Relationship between Crestal Bone Level and Soft Tissue Condition. Int. J. Oral Maxillofac. Implant. 2016, 31, e168–e178. [Google Scholar] [CrossRef] [Green Version]
- Paul, S.; Petsch, M.; Held, U. Modeling of Crestal Bone after Submerged vs. Transmucosal Implant Placement: A Systematic Review with Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2017, 32, 1039–1050. [Google Scholar] [CrossRef]
- Agustín-Panadero, R.; Martínez-Martínez, N.; Fernández-Estevan, L.; Faus-López, J.; Solá-Ruíz, M. Influence of Transmucosal Area Morphology on Peri-implant Bone Loss in Tissue-Level Implants. Int. J. Oral Maxillofac. Implant. 2019, 34, 852–947. [Google Scholar] [CrossRef]
- Candotto, V.; Gabrione, F.; Oberti, L.; Lento, D.; Severino, M. The role of implant-abutment connection in preventing bacterial leakage: A review. J. Biol. Regul. Homeost. Agents 2019, 33, 129–134. [Google Scholar] [PubMed]
- Lutz, R.; Sendlbeck, C.; Wahabzada, H.; Tudor, C.; Prechtl, C.; Schlegel, K.A. Periosteal elevation induces supracortical peri-implant bone formation. J. Cranio-Maxillofac. Surg. 2017, 45, 1170–1178. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | References | Exclusion Motivation |
|---|---|---|
| 1 | Becktor JP, Isaksson S, Billström C. A prospective multicenter study using two different surgical approaches in the mandible with turned Brånemark implants: conventional loading using fixed prostheses [15] | Excluded for the quantitative analysis: The parameter “marginal bone level” was not clearly reported. |
| 2 | Bratu EA, Tandlich M, Shapira L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: a prospective clinical study [16] | Studies comparing 2 or more different types of implant or abutment micro design. |
| 3 | de Siqueira RAC, Fontão FNGK, Sartori IAM, Santos PGF, Bernardes SR, Tiossi R. Effect of different implant placement depths on crestal bone levels and soft tissue behavior: a randomized clinical trial [17] | Studies comparing 2 or more different types of implant or abutment micro design. |
| 4 | Chappuis V, Bornstein MM, Buser D, Belser U. Influence of implant neck design on facial bone crest dimensions in the esthetic zone analyzed by cone beam CT: a comparative study with a 5-to-9-year follow-up [18] | Excluded for the quantitative analysis: excluded because it reports median, not mean value of MBL. |
| 5 | Chien HH, Schroering RL, Prasad HS, Tatakis DN. Effects of a new implant abutment design on peri-implant soft tissues [19] | Studies comparing 2 or more different types of micro design of the implant neck or of the abutment. |
| 6 | Cosyn J, Sabzevar MM, De Wilde P, De Rouck T. Two-piece implants with turned versus microtextured collars [20] | Studies comparing 2 or more different types of implant or abutment micro design. |
| 7 | Ebler S, Ioannidis A, Jung RE, Hämmerle CH, Thoma DS. Prospective randomized controlled clinical study comparing two types of two-piece dental implants supporting fixed reconstructions—results at 1 year of loading [21] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 8 | Esposito M, Trullenque-Eriksson A, Blasone R, et al. Clinical evaluation of a novel dental implant system as single implants under immediate loading conditions—4-month post-loading results from a multicentre randomised controlled trial [22] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 9 | Hof M, Pommer B, Strbac GD, Vasak C, Agis H, Zechner W. Impact of insertion torque and implant neck design on peri-implant bone level: a randomized split-mouth trial [23] | Studies comparing 2 or more different types of implant or abutment micro design. |
| 10 | Herrero-Climent M, Romero Ruiz MM, Díaz-Castro CM, Bullón P, Ríos-Santos JV. Influence of two different machined-collar heights on crestal bone loss [24] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 11 | Judgar R, Giro G, Zenobio E, et al. Biological width around one- and two-piece implants retrieved from human jaws [25] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 12 | Khorsand A, Rasouli-Ghahroudi AA, Naddafpour N, Shayesteh YS, Khojasteh A. Effect of Microthread Design on Marginal Bone Level Around Dental Implants Placed in Fresh Extraction Sockets [26] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 13 | Khraisat A, Zembic A, Jung RE, Hammerle CH. Marginal bone levels and soft tissue conditions around single-tooth implants with a scalloped neck design: results of a prospective 3-year study [27] | Studies comparing 2 or more different types of implant-abutment connections (e.g., Switching platform) not focusing on position related to the bone. |
| 14 | Kim JJ, Lee DW, Kim CK, Park KH, Moon IS. Effect of conical configuration of fixture on the maintenance of marginal bone level: preliminary results at 1 year of function [28] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 15 | Kütan E, Bolukbasi N, Yildirim-Ondur E, Ozdemir T. Clinical and Radiographic Evaluation of Marginal Bone Changes around Platform-Switching Implants Placed in Crestal or Subcrestal Positions: A Randomized Controlled Clinical Trial [29] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 16 | Marconcini S, Giammarinaro E, Toti P, Alfonsi F, Covani U, Barone A. Longitudinal analysis on the effect of insertion torque on delayed single implants: A 3-year randomized clinical study [30] | Studies comparing 2 or more different types of micro design of the implant neck or of the abutment. |
| 17 | Moberg LE, Köndell PA, Sagulin GB, Bolin A, Heimdahl A, Gynther GW. Brånemark System and ITI Dental Implant System for treatment of mandibular edentulism. A comparative randomized study: 3-year follow-up [31] | Excluded for the quantitative analysis:The parameter “marginal bone level” was not clearly reported. |
| 18 | Nóvoa L, Batalla P, Caneiro L, Pico A, Liñares A, Blanco J. Influence of Abutment Height on Maintenance of Peri-implant Crestal Bone at Bone-Level Implants: A 3-Year Follow-up Study [32] | Studies comparing 2 or more different types of micro design of the implant neck or of the abutment. |
| 19 | Ormianer Z, Duda M, Block J, Matalon S. One- and Two-Piece Implants Placed in the Same Patients: Clinical Outcomes After 5 Years of Function [33] | It is the topic of the present review but it is a case series. |
| 20 | Pellicer-Chover H, Peñarrocha-Diago M, Peñarrocha-Oltra D, Gomar-Vercher S, Agustín-Panadero R, Peñarrocha-Diago M. Impact of crestal and subcrestal implant placement in peri-implant bone: A prospective comparative study [34] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 21 | Peñarrocha-Diago MA, Flichy-Fernández AJ, Alonso-González R, Peñarrocha-Oltra D, Balaguer-Martínez J, Peñarrocha-Diago M. Influence of implant neck design and implant-abutment connection type on peri-implant health. Radiological study [35] | Studies comparing 2 or more different types of implant or abutment micro design. |
| 22 | Pozzi A, Agliardi E, Tallarico M, Barlattani A. Clinical and radiological outcomes of two implants with different prosthetic interfaces and neck configurations: randomized, controlled, split-mouth clinical trial [36] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 23 | Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with different prosthetic interfaces and design in partially posterior edentulous mandibles [37] | Studies comparing 2 or more different types of implant-abutment connections (e.g., Switching platform) not focusing on position related to the bone. |
| 24 | Sanz-Martin I, Vignoletti F, Nuñez J, et al. Hard and soft tissue integration of immediate and delayed implants with a modified coronal macrodesign: Histological, micro-CT and volumetric soft tissue changes from a pre-clinical in vivo study [38] | It is a study on animal model (Dog). |
| 25 | Shin YK, Han CH, Heo SJ, Kim S, Chun HJ. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year [39] | Studies comparing 2 or more different types of implant or abutment micro design |
| 26 | Tan WC, Lang NP, Schmidlin K, Zwahlen M, Pjetursson BE. The effect of different implant neck configurations on soft and hard tissue healing: a randomized-controlled clinical trial [40] | Studies comparing 2 or more different types of implant surgical technique with similar implant (e.g., one step surgery or two step) not focusing on position related to the bone. |
| 27 | Weinländer M, Lekovic V, Spadijer-Gostovic S, Milicic B, Wegscheider WA, Piehslinger E. Soft tissue development around abutments with a circular macro-groove in healed sites of partially edentulous posterior maxillae and mandibles: a clinical pilot study [41] | Studies comparing 2 or more different types of micro design of the implant neck or of the abutment. |
| 28 | Wittneben JG, Gavric J, Belser UC, et al. Esthetic and Clinical Performance of Implant-Supported All-Ceramic Crowns Made with Prefabricated or CAD/CAM Zirconia Abutments: A Randomized, Multicenter Clinical Trial [42] | Studies comparing 2 or more different types of micro design of the implant neck or of the abutment. |
| Studies Qualitative Analysis | Study Design | Patients Sample | Number of Implants (BL/TL) | Mean Age Range of the Sample | Type of 6 Implants BL; TL | Type of Prosthetic Restoration | Success Rate BL/TL | Survival Rate BL/TL | Follow-Up | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Astrand P. [43] | Prospective Randomized Comparative Multicenter Study | 28 | 73/77 | 61.7 ± SD range: 36–76 | BL: Branemark TL:ITI | Fixed Partial Bridges | / | 100% | 12 Months; 36 Months; |
| 2 | Bassi M. [44] | Prospective Clinical Study | 133 | 66/67 | 60 ± 11 range: 29–75 | BL: I-Fiz EVO Conical; TL: Shiner EVO Conical; | 52 Single Crown/3 Overdenture/70 Bridges | 88% | 100% | 60 Months; |
| 3 | Becktor. [15] | Prospective Multicenter Study | 80 | 206/198 | TL: 63.5 ± 9.1 Range: 47–89 BL: 65.5 ± 9.4 Range: 44–84 | Branemark System Nobel Biocare AB | Fixed Prosthetic Dentures | 97.6%/91.4% | 6 Months; 12 Months; 36 Months; | |
| 4 | Bömicke W. [45] | Randomized Controlled Trial Study | 38 | 19/19 | TL: 54.37 ± 14.62 BL: 51.51 ± 13.96 | Nobel Biocare AB | Single Zirconia Crown | / | 100%/94.7% | 12 Months; 36 Months; |
| 5 | Cecchinato D. [46] | Multicenter Randomized Controlled Crinical Trial | 84 | 171/153 | 51.6 | Astra Tech | Fixed Prosthetic dentures | / | >98% | 12 Months; 24 Months; |
| 6 | Cecchinato D. [46] | Multicenter Randomized Controlled Crinical Trial | 84 | 171/153 | 51.6 | Astra Tech | Fixed Prosthetic Dentures | / | >98% | 24 Months; 60 Months; |
| 7 | Chappuis V. [18] | Comparative Study | 61 | 20/41 | TL: 38.8 Range: 24–72 BL: 41.7 Range: 24–60 | Straumann | Single Crown | / | / | 60 Months; |
| 8 | Duda M. [48] | Non Randomized Retrospective Study | 33 | 29/24 | TL: 42.5 BL: 53.6 | Q Implants Trinon Titanium GmbH | / | 100%/91.7% | 6, 12, 36 Months; 60 Months; | |
| 9 | Eliasson A. [49] | prospective clinical study | 29 | 84/84 | 65 | DBA Paragon | Full arch ISFP | 86.2% | 99.4% | 12 Months; 60 Months; |
| 10 | Engquist B. [50] | Controlled Prospective Study | 82 | 113/80 | TL: 65 BL: 64 | Branemark System Noble BIocare AB | Fixed Prosthetic bridges | / | 97.5%/93.2% | 12 Months; |
| 11 | Engquist B. [51] | Controlled Prospective Study | 108 | 110/106 | 64.9 | Branemark System Nobel Biocare AB | Fixed Prosthetic Bridges with Cantilever | / | 100%/100% | 12 Months; 36 Months; |
| 12 | Ericsson I. [52] | Longitudinal Study | 11 | 33/30 | 61 Range: 42–72 | Branemark System | Fixed Prosthetic Bridges | / | / | 12 Months; 18 Months; |
| 13 | Gamper F.A. [53] | Randomized Controlled Clinical Trial Study | 60 | 86/65 | TL: 47.5 ± 15 BL: 55.8 ± 14 | BL: Branemark system Nobel Biocare AB TL: Straumann | Removable Prosthetic Prostheses/Screw Retained prostheses/cemented prostheses | / | 98.9%/96.6% | 60 Months; |
| 14 | Gulati M. [54] | Prospective Randomized Comparative Study | 19 | 10/10 | TL: 28.22 ± 3.27 BL: 27.20 ± 2.78 Range: 23–33 | Adin Dental Implant System | Screw-Retained Porcelain Fused to Metal Prosthesis | / | / | 3 and 6 Months; |
| 15 | Hadzik J. [55] | Clinical Study | 13 | 16/16 | TL: 46.3 BL: 45.9 Range: 20–63 | BL: Osseospeed TX, Astra tech TL: RN SLActive®, Straumann | Cemented Crowns | / | 100% | 6 Months; |
| 16 | Heijdenrijk K. [56] | Prospective Randomized Study | 60 | 38/38 | 58 ± 11 | Unknown | Overdenture with Clip Attachment | / | / | 12, 24, 36, 48, and 60 Months; |
| 17 | Lago L. [57] | Randomized Clinical Trial | 100 | 102/100 | 50.5 Range: 25–70 | Straumann | Single Crowns | 96.1%/98% | 12 and 60 Months; | |
| 18 | Moberg [31] | Randomized Prospective Study | 40 | 103/106 | BL: 62.6 ± 7.0 Range: 44.2–75.2 TL: 64.0 ± 6.8 Range: 40.2–77.2 | BL: Branemark System Nobel Biocare AB TL: ITI system | Screw Prosthetic Bridges | 97.9%/96.8% | / | 6 Months; 12 Months; 36 Months; |
| 19 | Paolantoni G. [58] | Randomized Controlled Clinical Trial Study | 65 | 29/45 | 53 ± 4 | Thommen Medical AG | Single Crowns | 100% | 60 Months; | |
| 20 | Sanz-Martin I. [59] | Prospective Randomized Controlled Clinical Study | 33 | 18/15 | Unknown | BL: Branemark System Nobel Biocare AB TL: Strumann | Group 2 Piece: SCs-4FDPs Group 1 Piece: SCs–4FDPs | / | / | 12 Months; |
| Total | 1161 | 2933 | 3–60 Months; |
| Mean Value Marginal Bone Changes # | Bone Level Implant | Tissue Level | Significance (p < 0.05) |
|---|---|---|---|
| 3 Months | 0.19 | 0.28 | /(Only Gulati 2013) |
| 6 Months | 0.33 | 0.42 | 0.0169 * (3 studies) |
| n = 115 | n = 65 | n = 50 | |
| 12 Months | 0.25 | 0.18 | 0.0000 * (12 studies) |
| n = 1850 | n = 971 | n = 879 | |
| 18 Months | 0.05 | 0.04 | /(Only Ericsson 1994) |
| 24 Months | 0.18 | 0.24 | 0.1907 (2 studies) |
| 36 Months | 0.45 | 0.48 | 0.5031 (5 studies) |
| 48 Months | 1.4 | 1.6 | /(Only Heijdenrijk 2006) |
| 60 Months | 0.29 | 0.38 | 0.0050 * (7 studies) |
| n = 1069 | n = 576 | n = 493 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosola, S.; Marconcini, S.; Boccuzzi, M.; Menchini Fabris, G.B.; Covani, U.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6920. https://doi.org/10.3390/ijerph17186920
Cosola S, Marconcini S, Boccuzzi M, Menchini Fabris GB, Covani U, Peñarrocha-Diago M, Peñarrocha-Oltra D. Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(18):6920. https://doi.org/10.3390/ijerph17186920
Chicago/Turabian StyleCosola, Saverio, Simone Marconcini, Michela Boccuzzi, Giovanni Battista Menchini Fabris, Ugo Covani, Miguel Peñarrocha-Diago, and David Peñarrocha-Oltra. 2020. "Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review" International Journal of Environmental Research and Public Health 17, no. 18: 6920. https://doi.org/10.3390/ijerph17186920
APA StyleCosola, S., Marconcini, S., Boccuzzi, M., Menchini Fabris, G. B., Covani, U., Peñarrocha-Diago, M., & Peñarrocha-Oltra, D. (2020). Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review. International Journal of Environmental Research and Public Health, 17(18), 6920. https://doi.org/10.3390/ijerph17186920