Comparison of the Intrinsic Foot Muscle Activities between Therapeutic and Three-Dimensional Foot-Ankle Exercises in Healthy Adults: An Explanatory Study



Abstract
:1. Introduction
2. Materials and Methods
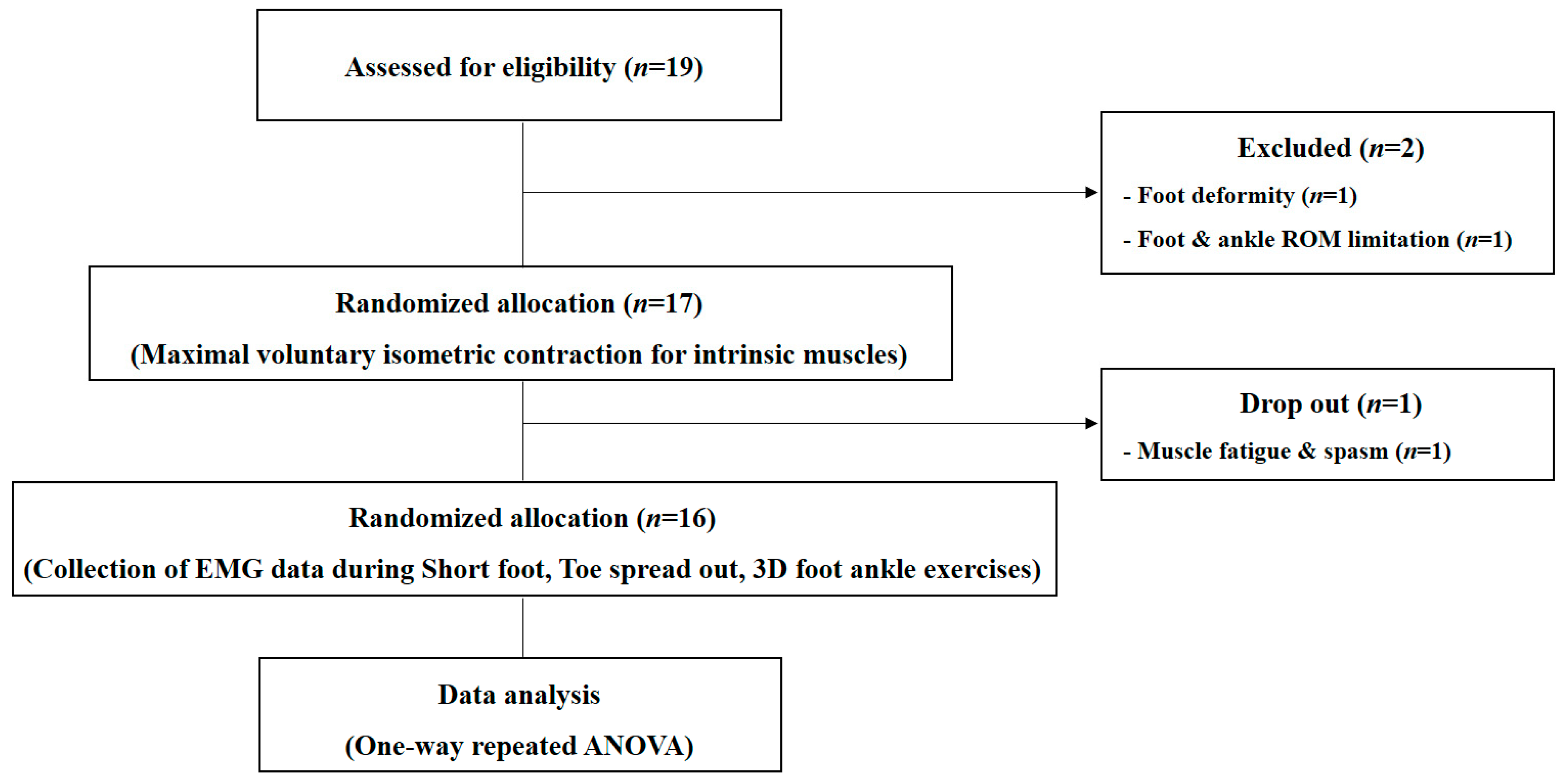
2.1. Participants
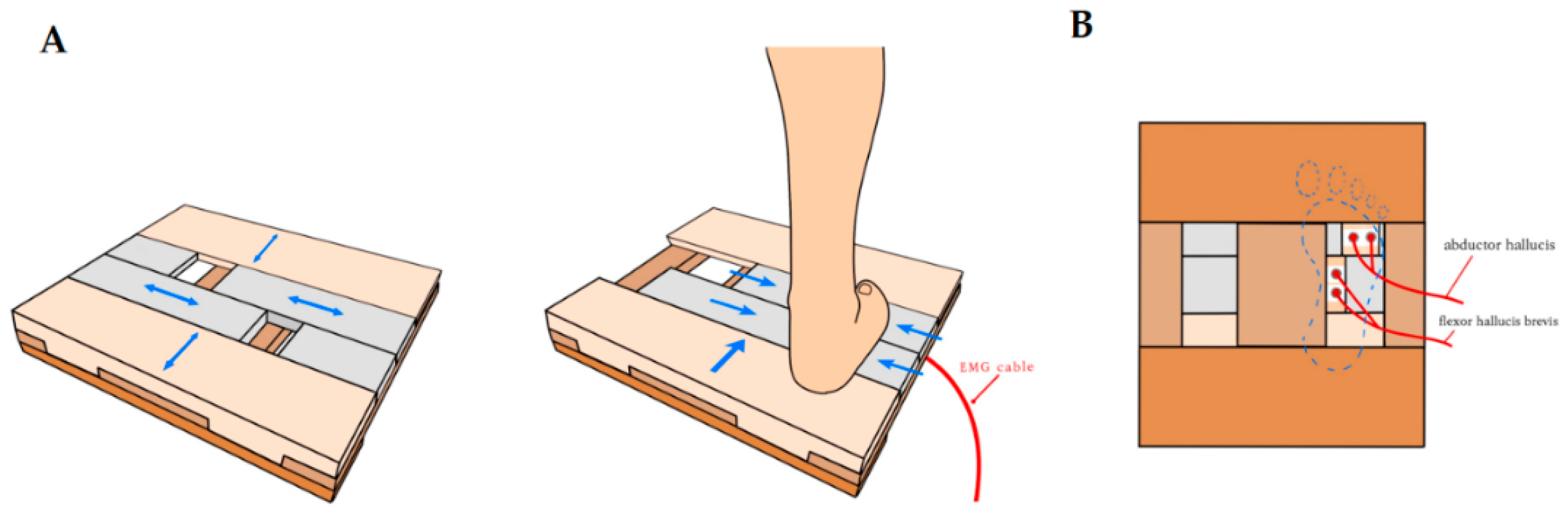
2.2. Measurement of Intrinsic Foot Muscles
2.3. Maximal Voluntary Isometric Contraction (MVIC)
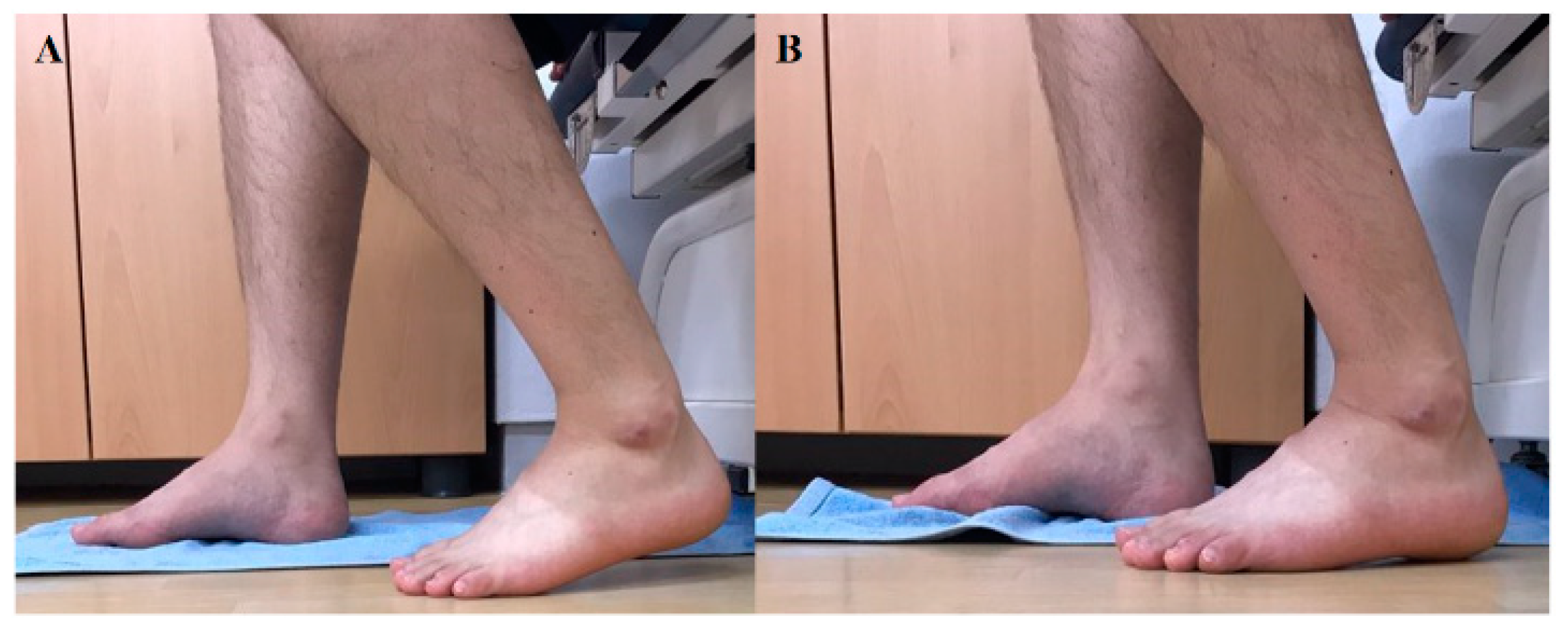
2.4. Foot–ankle Exercise for Strengthening of the Intrinsic Foot Muscles
2.5. AbH/AdH Ratio
2.6. Data Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saltzman, C.L.; Nawoczenski, D.A. Complexities of foot architecture as a base of support. J. Orthop. Sports Phys. Ther. 1995, 21, 354–360. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J.; Bramble, D.; Davis, I. The foot core system: A new paradigm for understanding intrinsic foot muscle function. Br. J. Sports Med. 2015, 49, 290. [Google Scholar] [CrossRef] [Green Version]
- Iaquinto, J.M.; Wayne, J.S. Computational model of the lower leg and foot/ankle complex: Application to arch stability. J. Biomech. Eng. 2010, 132, 021009. [Google Scholar] [CrossRef]
- Snyder, K.R.; Earl, J.E.; O’Connor, K.M.; Ebersole, K.T. Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clin. Biomech. 2009, 24, 26–34. [Google Scholar] [CrossRef]
- Eils, E.; Nolte, S.; Tewes, M.; Thorwesten, L.; Völker, K.; Rosenbaum, D. Modified pressure distribution patterns in walking following reduction of plantar sensation. J. Biomech. 2002, 35, 1307–1313. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J. Diminished plantar cutaneous sensation and postural control. Perceptual Mot. Skills 2007, 104, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Cresswell, A.G.; Racinais, S.; Whiteley, R.; Lichtwark, G. Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. J. R. Soc. Interface 2014, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulligan, E.P.; Cook, P.G. Effect of plantar intrinsic muscle training on medial longitudinal arch morphology and dynamic function. Man. Ther. 2013, 18, 425–430. [Google Scholar] [CrossRef]
- Chang, R.; Kent-Braun, J.A.; Hamill, J. Use of MRI for volume estimation of tibialis posterior and plantar intrinsic foot muscles in healthy and chronic plantar fasciitis limbs. Clin. Biomech. 2012, 27, 500–505. [Google Scholar] [CrossRef]
- Stewart, S.; Ellis, R.; Heath, M.; Rome, K. Ultrasonic evaluation of the abductor hallucis muscle in hallux valgus: A cross-sectional observational study. BMC Musculoskeletal Disord. 2013, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Angin, S.; Mickle, K.J.; Nester, C.J. Contributions of foot muscles and plantar fascia morphology to foot posture. Gait Posture 2018, 61, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Feger, M.A.; Snell, S.; Handsfield, G.G.; Blemker, S.S.; Wombacher, E.; Fry, R.; Hart, J.M.; Saliba, S.A.; Park, J.S.; Hertel, J. Diminished foot and ankle muscle volumes in young adults with chronic ankle instability. Orthop. J. Sports Med. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickle, K.J.; Munro, B.J.; Lord, S.R.; Menz, H.B.; Steele, J.R. Toe weakness and deformity increase the risk of falls in older people. Clin. Biomech. 2009, 24, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Aiyer, A.; Stewart, S.; Rome, K. The effect of age on muscle characteristics of the abductor hallucis in people with hallux valgus: A cross-sectional observational study. J. Foot Ankle Res. 2015, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Gooding, T.M.; Feger, M.A.; Hart, J.M.; Hertel, J. Intrinsic foot muscle activation during specific exercises: A T2 time magnetic resonance imaging study. J. Athl. Train. 2016, 51, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.H.; Kwon, O.Y.; Kim, S.H.; Jung, D.Y. Comparison of muscle activities of abductor hallucis and adductor hallucis between the short foot and toe-spread-out exercises in subjects with mild hallux valgus. J. Back Musculoskeletal Rehabil. 2013, 26, 163–168. [Google Scholar] [CrossRef]
- Lee, K.S.; Park, D.J. Three-dimensional ankle exercise with combined isotonic technique for an obese subject with plantar fasciitis: A case study. Medicina 2020, 56, 190. [Google Scholar] [CrossRef] [Green Version]
- Arinci Incel, N.; Genç, H.; Erdem, H.R.; Yorgancioglu, Z.R. Muscle imbalance in hallux valgus: An electromyographic study. Am. J. Phys. Med. Rehabil. 2003, 82, 345–349. [Google Scholar] [CrossRef]
- Letafatkar, A.; Rajabi, R.; Minoonejad, H.; Rabiei, P. Efficacy of perturbation-enhanced neuromuscular training on hamstring and quadriceps onset time, activation and knee flexion during a tuck-jump task. Int. J. Sports Phys. Ther. 2019, 14, 214–227. [Google Scholar] [CrossRef] [Green Version]
- Hislop, H.; Avers, D.; Brown, M. Daniels and Worthingham’s Muscle Testing, 9th ed.; Saunders Elsevier: St. Louis, MO, USA, 2013. [Google Scholar]
- Adler, S.S.; Beckers, D.; Buck, M. PNF in Practice: An Illustrated Guide, 4th ed.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Tosovic, D.; Ghebremedhin, E.; Glen, C.; Gorelick, M.; Mark Brown, J. The architecture and contraction time of intrinsic foot muscles. J. Electromyogr. Kinesiol. 2012, 22, 930–938. [Google Scholar] [CrossRef]
- Soysa, A.; Hiller, C.; Refshauge, K.; Burns, J. Importance and challenges of measuring intrinsic foot muscle strength. J. Foot Ankle Res. 2012, 5, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Headlee, D.L.; Leonard, J.L.; Hart, J.M.; Ingersoll, C.D.; Hertel, J. Fatigue of the plantar intrinsic foot muscles increases navicular drop. J. Electromyogr. Kinesiol. 2008, 18, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, N.M.; Varacallo, M. Anatomy, Bony Pelvis and Lower Limb, Tibialis Posterior Muscle; StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK539913/ (accessed on 28 September 2020).
- Park, D.J.; Park, S.Y. Comparison of subjects with and without pes planus during short foot exercises by measuring muscular activities of ankle and navicular drop height. J. Korean Soc. Phys. Med. 2018, 13, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Murley, G.S.; Menz, H.B.; Landorf, K.B. Foot posture influences the electromyographic activity of selected lower limb muscles during gait. J. Foot Ankle Res. 2009, 2, 35. [Google Scholar] [CrossRef] [Green Version]
- Angin, S.; Crofts, G.; Mickle, K.J.; Nester, C.J. Ultrasound evaluation of foot muscles and plantar fascia in pes planus. Gait Posture 2014, 40, 48–52. [Google Scholar] [CrossRef] [Green Version]
- Taş, S.; Ünlüer, N.Ö.; Çetin, A. Thickness, cross-sectional area, and stiffness of intrinsic foot muscles affect performance in single-leg stance balance tests in healthy sedentary young females. J. Biomech. 2020, 99, 109530. [Google Scholar] [CrossRef]
- Moore, K.; Dalley, A. Lower Limb. Clinically Oriented Anatomy; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Natsis, K.; Konstantinidis, G.A.; Symeonidis, P.D.; Totlis, T.; Anastasopoulos, N.; Stavrou, P. The accessory tendon of extensor hallucis longus muscle and its correlation to hallux valgus deformity: A cadaveric study. Surg. Radiol. Anat. 2017, 39, 1343–1347. [Google Scholar] [CrossRef]
- Zhang, F.Q.; Wang, H.J.; Zhang, Q.; Liu, Y.L.; Zhang, Y.Z. Hallux valgus deformity treated with the extensor hallucis longus tendon transfer by dynamic correction. Chin. Med. J. 2010, 123, 3034–3039. [Google Scholar]
- Solomonow, M.; Baratta, R.; Bernardi, M.; Zhou, B.; Lu, Y.; Zhu, M.; Acierno, S. Surface and wire EMG crosstalk in neighbouring muscles. J. Electromyogr. Kinesiol. 1994, 4, 131–142. [Google Scholar] [CrossRef]
- Yang, K.H.; Park, D.J. Reliability of ultrasound in combination with surface electromyogram for evaluating the activity of abdominal muscles in individuals with and without low back pain. J. Exercise Rehabil. 2014, 10, 230–235. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD 1 |
|---|---|
| Age (years) | 27.44 ± 2.58 |
| Height (cm) | 166.19 ± 6.80 |
| Weight (kg) | 59.75 ± 9.54 |
| BMI 2 (kg/m2) | 21.57 ± 2.62 |
| Sex | Male 8 (50%), female 8 (50%) |
| Dominant foot | Right = 13 (81.2%), left = 3 (18.8%) |
| Variable | SF 5 | TSO 6 | D1F 7 | D1E 8 | D2F 9 | D2E 10 |
|---|---|---|---|---|---|---|
| AbH 1 (%MVIC) * | 65.06 ± 28.01 | 80.84 ± 26.33 | 61.41 ± 21.33 | 76.48 ± 30.40 | 51.00 ± 17.20 | 78.97 ± 22.00 |
| AdH 2 (%MVIC) | 92.36 ± 8.16 | 88.10 ± 7.66 | 86.18 ± 7.40 | 93.37 ± 10.49 | 88.95 ± 5.84 | 92.96 ± 8.17 |
| EHL 3 (%MVIC) * | 49.16 ± 16.44 | 52.92 ± 19.37 | 68.14 ± 19.37 | 53.75 ± 14.22 | 73.19 ± 22.83 | 49.35 ± 11.56 |
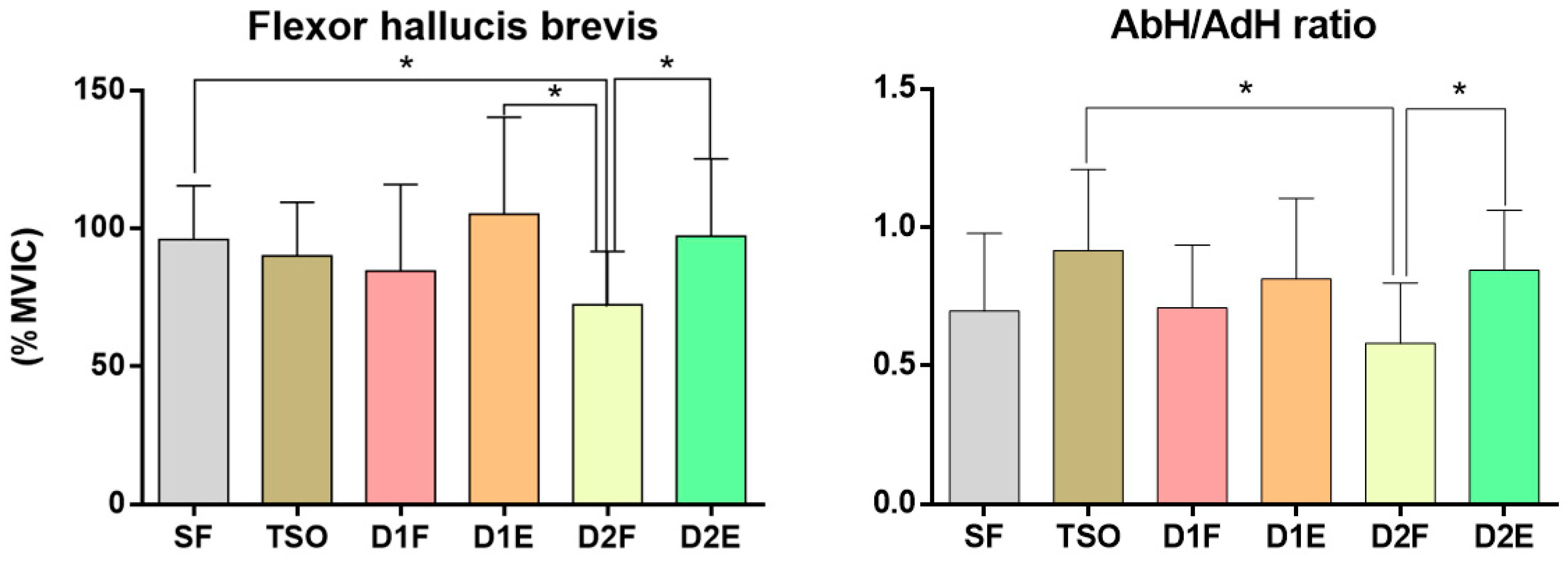
| FHB 4 (%MVIC) * | 95.96 ± 19.54 | 90.09 ± 19.40 | 84.58 ± 31.35 | 105.14 ± 35.15 | 72.28 ± 19.35 | 97.23 ± 27.97 |
| AbH/AdH ratio * | 0.70 ± 0.28 | 0.92 ± 0.29 | 0.71 ± 0.23 | 0.81 ± 0.29 | 0.58 ± 0.22 | 0.85 ± 0.22 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.-J.; Hwang, Y.-I. Comparison of the Intrinsic Foot Muscle Activities between Therapeutic and Three-Dimensional Foot-Ankle Exercises in Healthy Adults: An Explanatory Study. Int. J. Environ. Res. Public Health 2020, 17, 7189. https://doi.org/10.3390/ijerph17197189
Park D-J, Hwang Y-I. Comparison of the Intrinsic Foot Muscle Activities between Therapeutic and Three-Dimensional Foot-Ankle Exercises in Healthy Adults: An Explanatory Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7189. https://doi.org/10.3390/ijerph17197189
Chicago/Turabian StylePark, Du-Jin, and Young-In Hwang. 2020. "Comparison of the Intrinsic Foot Muscle Activities between Therapeutic and Three-Dimensional Foot-Ankle Exercises in Healthy Adults: An Explanatory Study" International Journal of Environmental Research and Public Health 17, no. 19: 7189. https://doi.org/10.3390/ijerph17197189
APA StylePark, D. -J., & Hwang, Y. -I. (2020). Comparison of the Intrinsic Foot Muscle Activities between Therapeutic and Three-Dimensional Foot-Ankle Exercises in Healthy Adults: An Explanatory Study. International Journal of Environmental Research and Public Health, 17(19), 7189. https://doi.org/10.3390/ijerph17197189