Developing a Family-Centered Care Model in the Neonatal Intensive Care Unit (NICU): A New Vision to Manage Healthcare

 ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
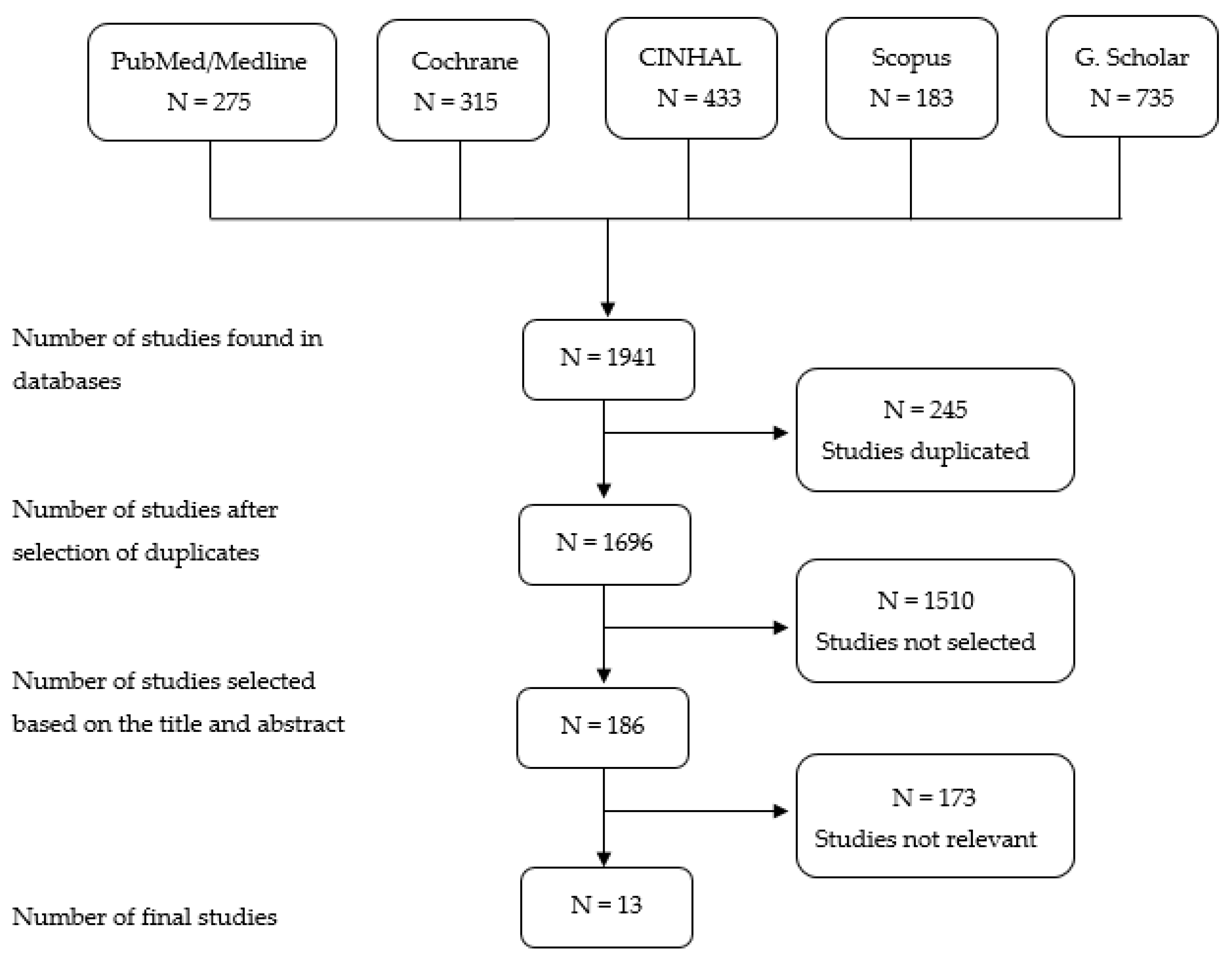
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
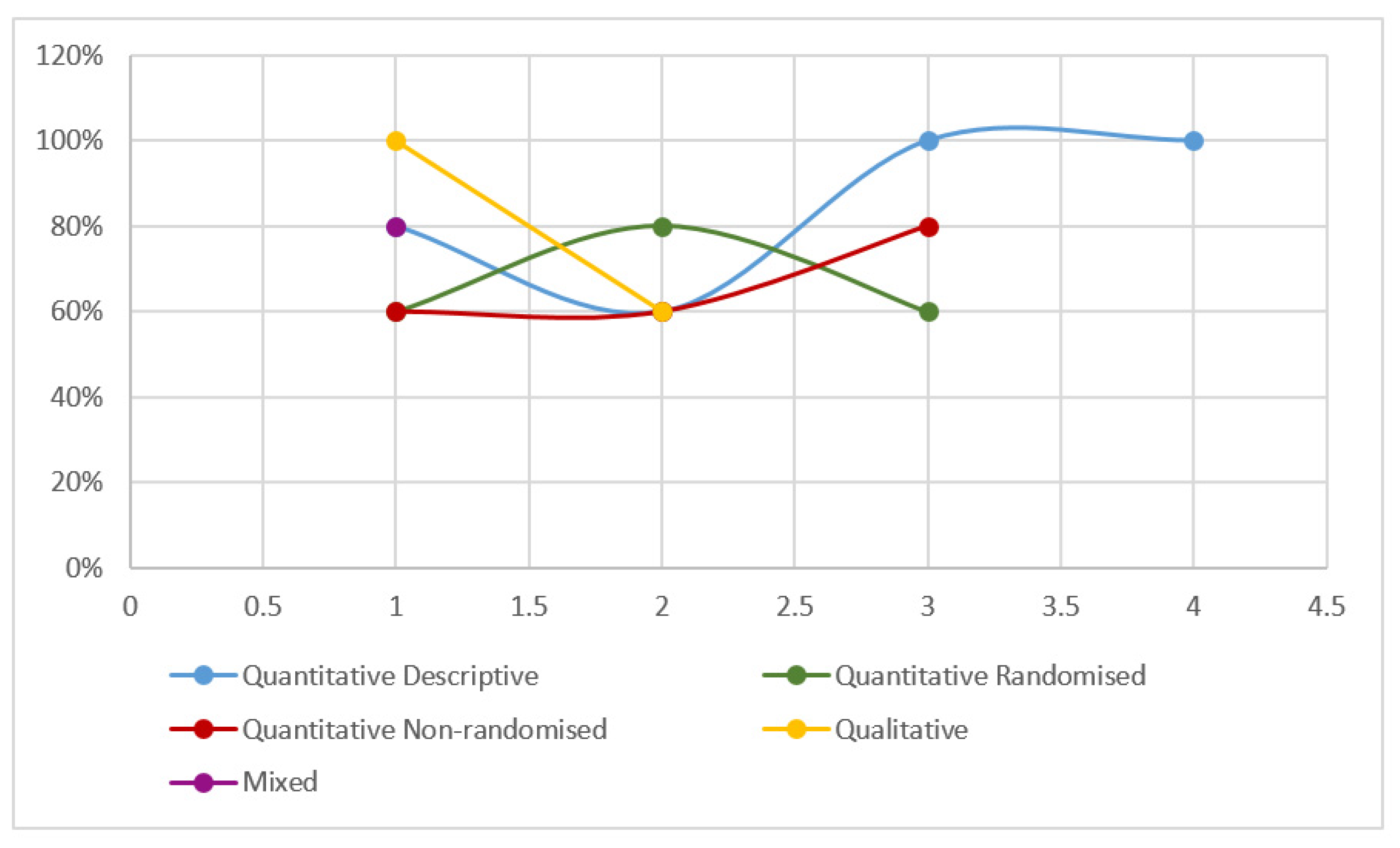
2.3. Quality Review and Evaluation Process
2.4. Data Analysis
3. Results
3.1. Perspective of Parental Involvement in Neonatal Care
3.2. Parental Training through the Health Team
3.3. Benefits of Involving the Family in the Realization of Care
3.4. Humanization NICU Care
4. Discussion
- (1)
- Regarding parental participation within these units, it would be convenient to encourage multidisciplinary clinical sessions, with active participation of both health professionals responsible for formal care and parents;
- (2)
- Likewise, hospital opening hours should be unified during 24 h, and it should even be encouraged that one of the parents spend the night in the NICU with their children;
- (3)
- In order to approach parental training, it would be important to promote learning courses where learning is facilitated from basic to more complex care, delivered by professionals who integrate the team. Such training would bring benefits to the PN, since it would contribute to a joint participation of the health professional and the family, avoiding re-admissions;
- (4)
- The proposal of humanization of the NICU, and the modifications that this entails, must be addressed from the medical and nursing directorates, so that they are heard by the hospital management area.
5. Conclusions
6. Strengths and limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
| WHO | World Health Organization |
| PN | Preterm newborn |
| NICU | Neonatal Intensive Care Unit |
| FCC | Family Centered Care |
| NIDCAP | Newborn Individualized Developmental Care and Assessment Program |
| GA | Gestational Age |
| (PCCF-P) Brazilian version | Patient and Family-Parent Focused Care Perception |
| (PCCF-E) Brazilian version | Patient and Family-Team Focused Care Perception |
| PSS: NICU | Parental Stress Scale: Neonatal Intensive Care Unit |
References
- Vogel, J.P.; Chawanpaiboon, S.; Moller, A.B.; Watananirun, K.; Bonet, M.; Lumbiganon, P. The global epidemiology of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Blencowe, H.; Lawn, J. Small babies, big numbers: Global estimates of preterm birth. Lancet 2019, 7, 1–2. [Google Scholar] [CrossRef] [Green Version]
- WHO. Every Newborn Day 2018. Available online: https://www.who.int/maternal_child_adolescent/newborns/every-newborn/en/ (accessed on 6 June 2020).
- Mulkey, S.B.; Du Plessis, A.J. Autonomic nervous system development and its impact on neuropsychiatric outcome. Pediatrics Res. 2019, 85, 120–126. [Google Scholar] [CrossRef]
- Matsufuji, M.; Healthy, N.; Tsuru, H.; Takashima, S. Neuroimaging and neuropathological characteristics of cerebellar injury in extremely low birth weight infants. Brain Dev. 2017, 39, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Gomes, E.; Santos, C.M.D.; Santos, A.; Silva, A.G.D.; Francois, M.A.M.; Romanini, D.S.; Mattos, M.C.V.; Loyal, A.F.; Costa, D. Autonomic responses of premature newborns to body position and environmental noise in the neonatal intensive care unit. Rev. Bras. Ter. Intensive 2019, 31, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Roué, J.M.; Kuhn, P.; Lopez Maestro, M.; Maastrup, R.A.; Mitanchez, D.; Westrup, B.; Sizun, J. Eight principles for patient-centred and family-centred care for newborns in the neonatal intensive care unit. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, 364–368. [Google Scholar] [CrossRef]
- Harillo Acevedo, F.D.; Rico Becerra, J.I.; Martínez, L. The philosophy of care focused on the development of the premature newborn (NIDCAP): A review of the literature. Glob. Sick. 2017, 16, 577–589. [Google Scholar]
- Franck, L.S.; Waddington, C.; O’Brien, K. Family integrated care for preterm infants. Crit. Care Nurs. Clin. 2020, 32, 149–165. [Google Scholar] [CrossRef]
- Franck, L.S.; O’Brien, K. The evolution of family-centered care: From supporting parent-delivered interventions to a model of family integrated care. Birth Defects Res. 2019, 111, 1044–1059. [Google Scholar] [CrossRef]
- Sheldon, R.E. Developmental care for preemies and their families: One neonatologist’s journey towards NIDCAP practice. NeoReviews 2017, 18, 568–575. [Google Scholar] [CrossRef] [Green Version]
- Warren, I. Family and infant neurodevelopmental education: An innovative, educational pathway for neonatal healthcare professionals. Infant 2017, 13, 200–203. [Google Scholar]
- Oude Maatman, S.M.; Bohlin, K.; Lilliesk-ld, S.; Garberg, H.T.; Uitewaal-Poslawky, I.; Kars, M.C.; van den Hoogen, A. Factors influencing implementation of family-centered care in a neonatal intensive care unit. Front. Pediatrics 2020, 8, 222. [Google Scholar] [CrossRef] [PubMed]
- Stefana, A.; Lavelli, M.; Rossi, G.; Beebe, B. Interactive sequences between fathers and preterm infants in the neonatal intensive care unit. Early Hum. Dev. 2020, 140, 1–8. [Google Scholar] [CrossRef] [PubMed]
- NIDCAP Federation International. 2018. Available online: https://nidcap.org/es/ (accessed on 10 June 2020).
- Baghlani, R.; Hosseini, M.B.; Safaiyan, A.; Alizadeh, M.; Bostanabad, M.A. Neonatal intensive care unit nurses’ perceptions and knowledge of newborn individualized developmental care and assessment program: A multicenter study. Iran. J. Nurs. Midwifery Res. 2019, 24, 113–117. [Google Scholar] [PubMed]
- Hearn, G.; Clarkson, G.; Day, M. The role of the NICU in father involvement, beliefs, and confidence: A follow-up qualitative study. Adv. Neonatal Care 2020, 20, 80–89. [Google Scholar] [CrossRef]
- Hill, C.; Knafl, K.A.; Santacroce, S.J. Family-centered care from the perspective of parents of children cared for in a pediatric intensive care unit: An integrative review. J. Pediatric Nurs. 2017. [Google Scholar] [CrossRef]
- Pineda, R.; Bender, J.; Hall, B.; Shabosky, L.; Annecca, A.; Smith, J. Parent participation in the neonatal intensive care unit: Predictors and relationships to neurobehavior and developmental outcomes. Early Hum. Dev. 2018, 117, 32–38. [Google Scholar] [CrossRef]
- Umberger, E.; Canvasser, J.; Hall, S.L. Enhacing NICU parent engagement and empowerment. Semin. Pediatr. Surg. 2018, 27, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, J.; Aloysius, A.; Platonos, K.; Deierl, A. Family centred care and family delivered care-What are we talking about? J. Neonatal Nurs. 2018, 24, 8–12. [Google Scholar] [CrossRef]
- Govindaswamy, P.; Laing, S.M.; Waters, D.; Walker, K.; Spence, K.; Badawi, N. Father’s needs in a surgical neonatal intensive care unit: Assuring the other parent. PLoS ONE 2020, 15, 1–13. [Google Scholar] [CrossRef]
- Wang, L.; He, J.L.; Fei, S.L. Perceived needs of parents of premature infants in NICU. West. J. Nurs. Res. 2018, 40, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Segers, E.; Ockhuijsen, H.; Baarendse, P.; van Eerden, I.; van den Hoogen, A. The impact of family centred care interventions in a neonatal or pediatric intensive care unit on parents’ satisfaction and length of stay: A systematic review. Intensive Crit. Care Nurs. 2019, 50, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.L.; McGrath, J.N.; Samra, H.A.; Gupta, R. An integrative review of parent satisfaction with care provided in the neonatal intensive care unit. JOGNN 2013, 42, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Crossetti, M.G.O. Integrative review of nursing Research: Scientific rigor required. Rev. Gaúcha Enferm. 2012, 33, 10–11. [Google Scholar] [CrossRef] [Green Version]
- Hong, Q.N.; Pluto, P.; Fábregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Mixed Method Appraisal Tool (MMAT); Mc Gill University (Canada): Montreal, QC, Canada, 2018. [Google Scholar]
- Simphronio Balbino, F.; Ferreira Gomes Balieiro, M.; Aparecida Mandetta, M. Evaluation of the perception of family-centered care and parental stress in a neonatal unit. Rev. Lat. Am. Enferm. 2016, 24, 1–9. [Google Scholar]
- Palma, I.E.; Von Wussow, K.F.; Morales, B.I.; Cifuentes, R.J.; Ambiado, T.S. Stress in parents of hospitalized newborns in a neonatal intensive care unit. Rev. Chil. Pediatr. 2017, 88, 332–339. [Google Scholar]
- Campo, A.; Mayra, C. Experience and perception of parents with regard to care in children with internation in ICU. Notes Sick 2018, 18, 5–10. [Google Scholar]
- Nyqvist, K.H.; Engvall, G. Parents as their infant’s primary caregivers in a neonatal intesive care unit. J. Pediatr. Nurs. 2009, 24, 153–163. [Google Scholar] [CrossRef]
- Ottosson, C.; Lantz, B. Parental participation in neonatal care. J. Neonatal Nurs. 2017, 23, 112–118. [Google Scholar] [CrossRef]
- O’Brien, K.; Bracht, M.; Macdonell, K.; McBride, T.; Robson, K.; O’Leary, L.; Christie, K.; Galarza, M.; Dicky, T.; Levin, A.; et al. A pilot cohort analytic study of family integrated care in a Canadian neonatal intensive care unit. BMC Pregnancy 2013, 13, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, N.L.; Rubio Grillo, M.H.; Lovers, A. Strategies for neonatal developmental care and family-centered neonatal care. Invest. Educ. Enferm. 2016, 34, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallegos-Martínez, J.; Reyes-Hernández, J.; Silvan-Scochi, C.G. The neonatal unit and the involvement of parents in preterm care. Perinatol. Reprod. Hum. 2010, 24, 98–108. [Google Scholar]
- Verma, A.; María, A.; Pandey, R.M.; Hans, C.; Sherwani, F. Family-centered care to complement care of sick newborns: A randomized controlled trial. Indian Pediatr. 2017, 54, 455–459. [Google Scholar] [CrossRef]
- Sannino, P.; Gianni, M.L.; By Bon, G.; Fontana, C.; Picciolini, O.; Plevani, L.; Fumagalli, M.; Consonni, D.; Fly, F. Support to mothers of premature babies using NIDCAP method: A non-randomized controlled trial. Early Hum. Dev. 2016, 95, 15–20. [Google Scholar] [CrossRef]
- By Bernardo, G.; Svelto, M.; Giordano, M.; Sordino, D.; Riccitelli, M. Supporting parents in taking care of their infants admitted to a neonatal intensive care unit: A prospective cohort pilot study. Ital. J. Pediatr. 2017, 43, 1–11. [Google Scholar] [CrossRef]
- Stelwagen, M.A.; van Kempen, A.; Westmaas, A.; Blees, Y.J.; Scheele, F. Integration of maternity and neonatal care to empower parents. J. Obstet. Gynecol. Neonatal Nurs. 2020, 49, 65–77. [Google Scholar] [CrossRef]
- Kjellsdotter, A.; Lantz, B.; Ottosson, C. Healthcare professionals’ views on parental participation in the neonatal intensive care units. J. Pediatr. Nurs. 2017, 41, 3–8. [Google Scholar] [CrossRef]
- Boztepe, H.; Kerimo-lu Y-ld-z, G. Nurses perceptions of barriers to implementing family-centered care in a pediatric setting: A qualitative study. J. Spec. Pediatr. Nurs. 2017, 22, e12175. [Google Scholar] [CrossRef]
- Fuente González, P. The nursing professional in neonatal units and development-focused care. Sick Goals 2016, 19, 58–64. [Google Scholar]
- Acosta-Romo, M.F.; Cabrera-Bravo, N.; Basante-Castro, Y.; Jury, D. Feelings experienced by parents when their premature children are hospitalized. A contribution to the humanized care. Rev. Univ. Salud 2017, 19, 17–25. [Google Scholar]
- Osuna Guerrero, M.; Pastor-Montero, S.M. Humanization strategies in neonatal units: Bibliographic review. Lascasas Libr. 2018, 14, 15–26. [Google Scholar]



{kind=link}
{kind=link}
| Databases | Combination MeSH Terms |
|---|---|
| PubMed/Medline |
|
| Cochrane CINHAL |
|
| Scopus Google Scholar |
|
| Quantitative Studies | |||||||
|---|---|---|---|---|---|---|---|
| Author(s), Year and Country | Study Design | Study Purpose | Sample Characteristics | Main Variables | Methodological Quality Level | Results | Limitations |
| Hedberg et al. (2009) Sweden | Quantitative dichotomous responses | Explore parents’ views on parental performance of care in the NICU. | N = 29 parents:
10 parents N-II) | Parents:
| 80% | Parents can take care of the PN. Support the role of parents as caregivers. Nurse educators. | The sample should be bigger |
| Martinez et al. (2010) Mexico | Quantitative descriptive | Understand the healthcare environment and the administration of parental care. Parent participation in NICU, at different levels. | N = 9 H:
2 Level II |
| 60% | Encourage parent participation. Implementation of the FCC philosophy. Healthcare training and parent care training. | Enlarge sample size. Evaluate infrastructure, equipment, organization. |
| O’Brien et al. (2013) Canada | Quantitative cohort analysis | Explore the feasibility of implementing the FCC care model. IN NICU promote maternal development: attention to PN. | N = 42 PNs 4 twin PNs were excluded (N =14 PN G. Control) N = 42 mothers (N = 14 mothers G. Control) | Rn:
| 60% | FCC model is feasible and safe. It improves maternal care and PN results. | Use critical incidence reports only to monitor security. Non-representative, non-generalizable parents |
| Sannino et al. (2016) Italy | Quantitative non-randomized control single center | Evaluate NIDCAP effectiveness mother care participation PN. | N = 43 PN (32 GE):
| PN:
| 60% | NIDCAP effective participation of mother in care of PN improves neurofunctional development. Mothers in NIDCAP group more involved. | Small sample size. No group randomization. Bias of the population studied, only one center |
| Simphronio et al. (2016) Brazil | Quantitative quasi-experimental | To evaluate the effects of FCC implementation on perception and parental stress on caring capacity. | N = 132 parents of PN (N = 66 phase prior to intervention, N = 66 after intervention). | Parents:
| 100% | Improved parental perception in FCC in terms of respect, collaboration and support in the post-intervention phase. Greater satisfaction, increased capacity to care for children. Less parental stress and anxiety after intervention | The study investigated two measures (perception and stress). Short-term evaluation. |
| By Bernardo et al. (2017) Italy | Quantitative prospective non-randomized cohort | Compare levels of satisfaction and stress, participation and care: - Parents group FCC. - Non-FCC parents. | G. FCC:
| Parents:
| 60% | FCC Group: higher satisfaction, lower stress level when participating in care. Family integration model advantages, future need for trials. | Small sample size. Selected population of PN disease Qx. Non-randomization. Do not distinguish between procedures that are a source of stress for parents. |
| Ottosson et al. (2017) Sweden | Quantitative multiple regression analysis | Identify process of care components. Vision parents participation care. | N = 141 parents of NICU children.
| Characteristics of parents:
EMPATHIC-N):
| 80% | Strong points of PN: better interaction with breastfeeding and caring. Professional hands-on involvement: facilitates parent participation. Important contact nurse continuity. | No random sample: generalization of results questioned. |
| Palma et al. (2017) Chile | Quantitative cross-sectional description | Knowing stress levels and parental perceptions of participating PN in NICU care. | N = 100 parents (N = 43 men, N = 57 women) N = 59 RN. | Parents:
| 100% | Support and parent education, allows them to cope with stress. Encourage care and practices that promote parent–PN bonding. | Not analyze other factors that can influence stress, such as mental health, social network, personality. |
| Verma et al. (2017) India | Quantitative randomized controlled trial | Evaluate impact of parent involvement in care of PN. | N = 295 PN NICU: G.Control=147 G.Interven=148 Family:
|
| 80% | G. Intervention, better preparation good home transition. Decreases hospital stay. Parent empowerment: cornerstone of the continuum of care | Study low power to detect differences. No evaluation of long-term results. |
| Govindaswamy et al. (2020) Australia | Quantitative prospective cohort | Identify needs for parental involvement in NICU care | N = 48 parents of PN (N = 23 G. Intervention N = 25 G. Control) N = 48 PN. | Characteristics of parents:
or 36–40 (11) or 40 (7)
o No (20)
o No (46) Characteristics PN:
or 34–37 (13) or 37(33)
or 1501–2500 (10) or 2501 (37) | 60% | Parents G. Intervention need to actively participate in PN care, recognize caregiving role. FCC Model meeting parent needs. | Difficult to evaluate sample representativeness and generalization of results. Includes only parents who can read and write in English. Limited sampling method. |
| Qualitative Studies | |||||||
| Campo et al. (2018) Argentina | Qualitative phenomenological paradigm | Identify parenting needs. Pick up parental care granted to PN upon discharge. | N = 8 parents children admitted to NICU. |
| 100% | Parents argue nursing: teaches care, family empowerment Communication improves bonding. Open NICU guides and trains parents in care. | Data are collected until they provide information relevant to the study. |
| Stelwagen et al. (2019) Holland | Qualitative descriptive | Describes transition from traditional NICU design to new infrastructure that enables parent empowerment | N = 53 families | Room design:
| 60% | Implementation of infrastructure for neonatal care, facilitates parent empowerment. Requires willingness to change. | Minimum description of the implementation mechanism and its cost. |
| Mixed Studies | |||||||
| Hernandez et al. (2016) Colombia | Quantitative descriptive and qualitative analysis | Evaluate strategies for developing PN and FCC in NICU | N = 7 mothers |
| 80% | Healthcare workers: Encourages humanized care in NICUs. Educates the family in PN care, with mutual communication and training. Parents need more communication, participation, and increased visiting hours. The changes to promote FCC obtained positive results in the short term. | Personal change during study, obstacle to continuous reflection. Changes in care practice occurred over a short period of time. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Cantarino, S.; García-Valdivieso, I.; Moncunill-Martínez, E.; Yáñez-Araque, B.; Ugarte Gurrutxaga, M.I. Developing a Family-Centered Care Model in the Neonatal Intensive Care Unit (NICU): A New Vision to Manage Healthcare. Int. J. Environ. Res. Public Health 2020, 17, 7197. https://doi.org/10.3390/ijerph17197197
Gómez-Cantarino S, García-Valdivieso I, Moncunill-Martínez E, Yáñez-Araque B, Ugarte Gurrutxaga MI. Developing a Family-Centered Care Model in the Neonatal Intensive Care Unit (NICU): A New Vision to Manage Healthcare. International Journal of Environmental Research and Public Health. 2020; 17(19):7197. https://doi.org/10.3390/ijerph17197197
Chicago/Turabian StyleGómez-Cantarino, Sagrario, Inmaculada García-Valdivieso, Eva Moncunill-Martínez, Benito Yáñez-Araque, and M. Idoia Ugarte Gurrutxaga. 2020. "Developing a Family-Centered Care Model in the Neonatal Intensive Care Unit (NICU): A New Vision to Manage Healthcare" International Journal of Environmental Research and Public Health 17, no. 19: 7197. https://doi.org/10.3390/ijerph17197197
APA StyleGómez-Cantarino, S., García-Valdivieso, I., Moncunill-Martínez, E., Yáñez-Araque, B., & Ugarte Gurrutxaga, M. I. (2020). Developing a Family-Centered Care Model in the Neonatal Intensive Care Unit (NICU): A New Vision to Manage Healthcare. International Journal of Environmental Research and Public Health, 17(19), 7197. https://doi.org/10.3390/ijerph17197197