How Health Promoters Can Assess Capacity Building Processes in Setting-Based Approaches—Development and Testing of a Monitoring Instrument

Abstract
:1. Introduction
2. Methods
2.1. Research Consortium Capital4Health
2.2. Ethical Considerations
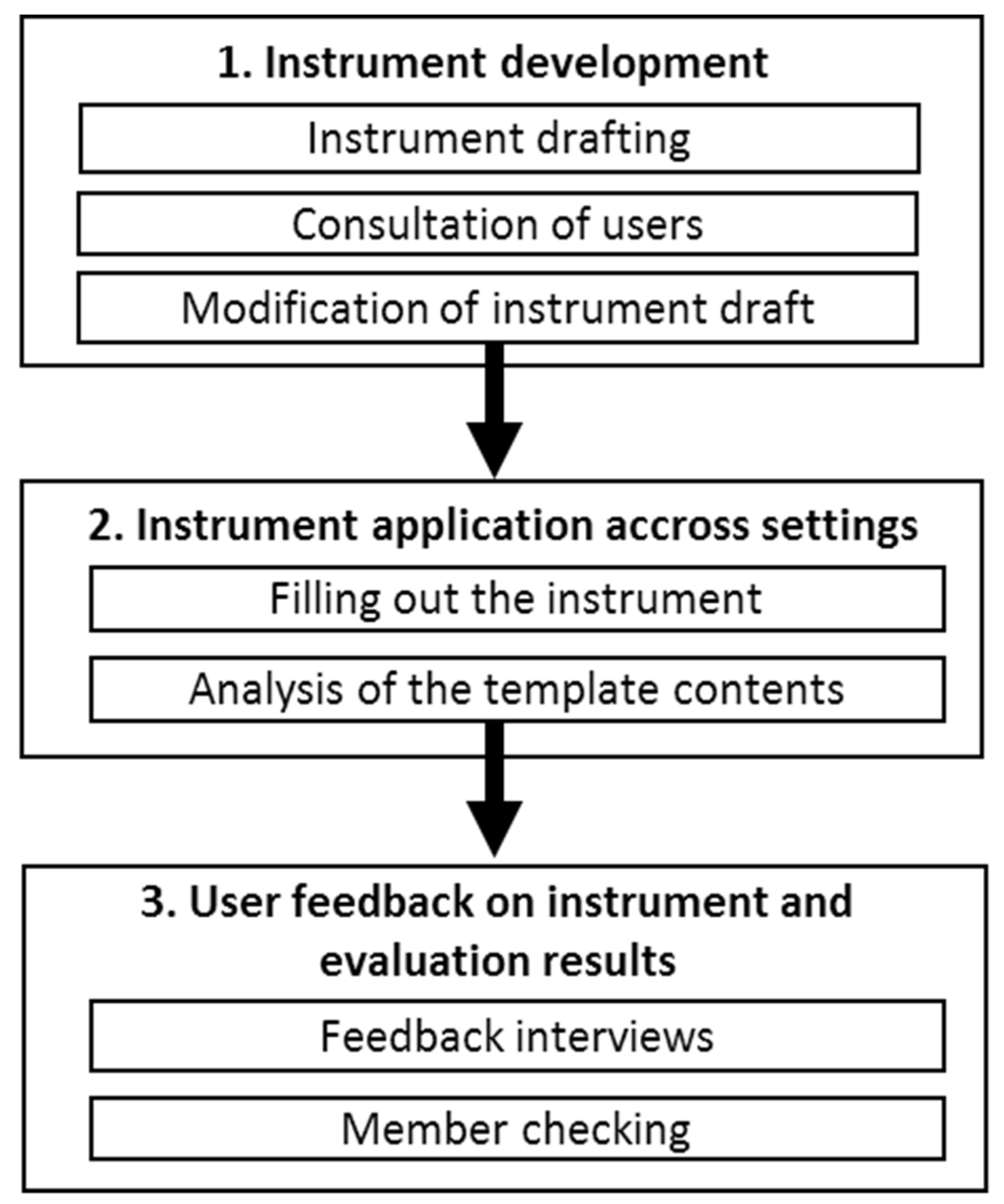
2.3. Instrument Development
2.3.1. Instrument Drafting
2.3.2. Consultation of Users
- (1)
- Is the “EVA-protocol” considered suitable for describing the members of the stakeholder group, their interactions and the development of relevant capacities?
- (2)
- How can the “EVA-protocol” be improved to better fit the program logic, and to improve usability?
2.3.3. Modification of Instrument Draft
2.4. Instrument Application across Settings
2.4.1. Filling out the Instrument
2.4.2. Analysis of the “EVA-Protocol”
2.5. User Feedback on Instrument Use and Evaluation Results
2.5.1. Feedback Interviews
- (1)
- How understandable were the questions in the protocol? Did you know what kind of information was expected to be given?
- (2)
- How do you rate the order and layout of the questions?
- (3)
- Was the length of the “EVA-protocol” appropriate? How much time did it take to complete the “EVA-protocol”? Did filling out the protocol compromise your daily project work?
- (4)
- To what extent was the information in the “EVA-protocol” relevant to yourself or to your subproject?
- (5)
- Were there any questions that proved redundant for your subproject or the type of stakeholder group you facilitated?
- (6)
- Are there any further comments or suggestions for improvement?
2.5.2. Member Checking
3. Results
3.1. Instrument Application and Analysis
“The pedagogical staff [of the kindergartens] are the stakeholders who are responsible for the implementation of the project actions. They have received support from parents and kindergartens sponsor and have been able to mobilise funds for the purchase of new exercise equipment and for a team training day”.(Subproject 01, protocol number 08)
“The meeting was structured in a directive way by the project team, since a decision on the further course of the stakeholder group was required. Possible work packages for the development of new actions as well as the organisation of an information gathering [for community members] were presented to the group. Nevertheless, it was difficult to name stakeholders responsible for single tasks. [A stakeholder explained]: ‘I personally won’t put much work into it [project] anymore’”.(Subproject 03, protocol number 08)
3.2. Feedback Interviews and Member Checking
3.2.1. Comprehensibility of the Questions
“(...) what indicators do you use to identify whether someone is a leader or not? …If you ask ten people, even experts, you will get different answers. So it would be helpful to spell out the indicators that define a leader [in the “EVA protocol”].”(IP05)
3.2.2. Length and Work Load
“For me, the amount of time necessary to fill out the protocol was all right. Yes, it is additional work, but the scope is okay”.(IP01)
3.2.3. Redundancy, Structure and Answer Format
“We don’t have the option to write down which strategies worked or didn’t work [with the group]. We can only present the results. What’s missing here is an open question: ‘What strategies have been employed by the facilitators to change the respective capacities’”.(IP02)
3.2.4. Usability
“I have filled out the “EVA-protocol” on my own the last few times and have not consulted with X [my colleague]. Which is probably not favorable, because … there’s more subjectivity in it... Last meeting, Y [one specific important stakeholder] wasn’t there, then a certain lack of leadership resulted. And I guess my interpretation is a bit different from X’s [my colleague’s] one. I’m intrigued to learn what X [my colleague] will write down about this topic.”(IP03)
3.2.5. Benefit for Subproject Teams
“[The EVA protocol] would have helped us to answer the question ‘How can we optimize the work in our stakeholder groups’? Is it necessary to address or involve certain people? Is it necessary or relevant to identify a leader? What is it that motivates the people to participate [in the stakeholder groups]? Actually, [we] should have taken a look at the “EVA-protocols” then, because those would have provided good indicators for that”.(IP04)
“I can’t remember a great benefit [of filling out the “EVA-protocols”]. But that was also because of a lack of resources (…) one was always pushed to [prepare the next meeting]”.(IP04)
4. Discussion
4.1. Principle Findings
4.2. Strengths and Limitations
4.3. Comparison with Other Studies
4.4. Implications for Policy and Practice
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cornwall, A.; Jewkes, R. What is participatory research? Soc. Sci. Med. 1995, 41, 1667–1676. [Google Scholar] [CrossRef]
- Israel, B.A.; Schultz, A.J.; Parker, E.A.; Becker, A.B.; Allen, A.J.; Guzman, J.R. Critical issue in developing and following community based participatory research principles. In Community-Based Participatory Research for Health: From Process to Outcomes, 2nd ed.; Minkler, M., Wallerstein, N., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 47–66. [Google Scholar]
- Wallerstein, N.B.; Duran, B. Using community-based participatory research to address health disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Minkler, M. Community-based research partnerships: Challenges and opportunities. J. Urban Health Bull. N. Y. Acad. Med. 2005, 82, ii3–ii12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minkler, M.; Blackwell, A.G.; Thompson, M.; Tamir, H. Community-based participatory research: Implications for public health funding. Am. J. Public Health 2003, 93, 1210–1213. [Google Scholar] [CrossRef] [PubMed]
- Ubert, T.; Forberger, S.; Gansefort, D.; Zeeb, H.; Brand, T. Community capacity building for physical activity promotion among older adults—A literature review. Int. J. Environ. Res. Public Health 2017, 14, 1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Jakarta declaration on leading health promotion into the 21st century. In Proceedings of the Fourth International Conference on Health Promotion: New Players for a New Era—Leading Health Promotion into the 21st Century, Jakarta, Indonesia, 21–25 July 1997. [Google Scholar]
- Crisp, B.R.; Swerrissen, H.; Duckett, S.J. Four approaches to capacity building in health: Consequences for measurement and accountability. Health Promot. Int. 2000, 15, 99–107. [Google Scholar] [CrossRef] [Green Version]
- Hawe, P.; Noort, M.; King, L.; Jordens, C. Multiplying health gains: The critical role of capacity-building within health promotion programs. Health Policy 1997, 39, 29–42. [Google Scholar] [CrossRef]
- McIsaac, J.L.; Hernandez, K.J.; Kirk, S.F.; Curran, J.A. Interventions to support system-level implementation of health promoting schools: A scoping review. Int. J. Environ. Res. Public Health 2016, 13, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Heimburg, D.; Hakkebo, B. Health and equity in all policies in local government: Processes and outcomes in two Norwegian municipalities. Scand. J. Public Health 2017, 45, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawe, P.; King, L.; Noort, M.; Jordens, C.; Llyod, B. Indicators to Help with Capacity Building in Health Promotion; NSW Health Department: Sydney, Australia, 2000. [Google Scholar]
- Liberato, S.C.; Brimblecombe, J.; Ritchie, J.; Ferguson, M.; Coveney, J. Measuring capacity building in communities: A review of the literature. BMC Public Health 2011, 11, 850. [Google Scholar] [CrossRef] [Green Version]
- Gibbon, M.; Labonte, R.; Laverack, G. Evaluating community capacity. Health Soc. Care Community 2002, 10, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Laverack, G.; Labonte, R. A planning framework for community empowerment goalswithin health promotion. Health Policy Plan. 2000, 15, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.M.; Speers, M.A.; McLeroy, K.; Fawcett, S.; Kegler, M.; Parker, E.; Smith, S.R.; Sterling, T.D.; Wallerstein, N. Identifying and defining the dimension of community capacity to provide a basis for measurement. Health Educ. Behav. 1998, 25, 258–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sotomayor, M.; Dominguez, A.; Pawlik, F. Building community capacity for health promotion in a hispanic community. Prev. Chronic. Dis. 2007, 4, 1–8. [Google Scholar]
- Ryan, M.; Erck, L.; McGovern, L.; McCabe, K.; Myers, K.; Nobrega, S.; Li, W.; Lin, W.C.; Punnett, L. “Working on Wellness”: Protocol for a worksite health promotion capacity-building program for employers. BMC Public Health 2019, 19, 111. [Google Scholar] [CrossRef] [PubMed]
- Dressendorfer, R.H.; Raine, K.; Dyck, R.J.; Plotnikoff, R.C.; Collins-Nakai, R.L.; McLaughlin, W.K.; Ness, K. A conceptual model of community capacity development for health promotion in the alberta heart health project. Health Promot. Pract. 2005, 6, 31–36. [Google Scholar] [CrossRef]
- Süß, W.; Nickel, S.; Wolf, K.; Trojan, A. Capacity building for prevention and health promotion for children and parents in a deprived urban quarter: Lenzgesund. Gesundheitswesen 2015, 76, 120–121. [Google Scholar]
- Bergeron, K.; Abdi, S.; DeCorby, K.; Mensah, G.; Rempel, B.; Manson, H. Theories, models and frameworks used in capacity building interventions relevant to public health: A systematic review. BMC Public Health 2017, 17, 914. [Google Scholar] [CrossRef]
- Maclellan-Wright, M.F.; Anderson, D.; Barber, S.; Smith, N.; Cantin, B.; Felix, R.; Raine, K. The development of measures of community capacity for community-based funding programs in Canada. Health Promot. Int. 2007, 22, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Trojan, A.; Nickel, S. Empowerment by capacity building in urban quarters--first results and assessment of a new standardised instrument. Gesundheitswesen 2008, 70, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Gilmore, B.; MCAuliffe, E.; Larkan, F.; Conteh, M.; Dunne, N.; Gaudrault, M.; Mollel, H.; Tumwesigye, N. How do community health committees contribute to capacity buidling for maternal and child health? A realist evaluation protocol. BMJ Open 2016, 6, e011885. [Google Scholar] [CrossRef] [Green Version]
- Curbach, J.; Warrelmann, B.; Brandstetter, S.; Lindacher, V.; Rueter, J.; Loss, J. Empowering senior citizens for healthy nutrition in Germany: A pilot study. Health Soc. Care Community 2018, 26, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Brandstetter, S.; Curbach, J.; Lindacher, V.; Rueter, J.; Warrelmann, B.; Loss, J. Empowerment for healthy nutrition in German communities: A study framework. Health Promot. Int. 2017, 32, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P.; King, L.; Noort, M.; Gifford, S.M.; Lloyd, B. Working invisibly: Health workers talk about capacity-building in health promotion. Health Promot. Int. 1998, 13, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Brandstetter, S.; McCool, M.; Wise, M.; Loss, J. Australian health promotion practitioners’ perceptions on evaluation of empowerment and participation. Health Promot. Int. 2014, 29, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–3. [Google Scholar] [PubMed]
- Rutten, A.; Frahsa, A.; Abel, T.; Bergmann, M.; de Leeuw, E.; Hunter, D.; Jansen, M.; King, A.; Potvin, L. Co-producing active lifestyles as whole-system-approach: Theory, intervention and knowledge-to-action implications. Health Promot. Int. 2017, 34, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Foitzik, E.; Hassel, H. Bewegte Kitas durch Organisationsentwicklung. Prävent. Gesundh. 2019, 1–6. [Google Scholar] [CrossRef]
- Sygusch, R.; Brandl-Bredenbeck, H.P.; Tittlbach, S.; Ptack, K.; Töpfer, C. Gesundheit in Sportunterricht und Sportlehrerbildung. Bestandsaufnahme, Intervention und Evaluation im Projekt ‘Health.edu’; Springer: Wiesbaden, Germany, 2020. [Google Scholar]
- Popp, J.; Grüne, E.; Carl, J.; Pfeifer, K. PArC-AVE-Partizipative Bewegungsförderung in der beruflichen Bildung [PArC-AVE—Participatory physical activity promotion in vocational education]. Bewegungstherapie Gesundheitssport. 2019, 35, 224–225. [Google Scholar]
- Strobl, H.; Brew-Sam, N.; Curbach, J.; Metz, B.; Tittlbach, S.; Loss, J. Action for men: Study protocol of a community capacity building intervention to develop and implement gender-sensitive physical activity programs for men 50 plus. Front. Public Health 2019. (in revision). [Google Scholar]
- Rutten, A.; Gelius, P. Building policy capacities: An interactive approach for linking knowledge to action in health promotion. Health Promot. Int. 2013, 29, 569–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labonte, R.; Laverack, G. Capacity building in health promotion, Part 1: For whom? And for what purpose? Crit. Public Health 2001, 11, 111–127. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Mays, N.; Pope, C. Assessing quality in qualitative research. BMJ 2000, 320, 50–52. [Google Scholar] [CrossRef]
- Mays, N.; Pope, C. Rigour and qualitative research. Br. Med. J. 1995, 311, 109–112. [Google Scholar] [CrossRef]
- Birt, L.; Scott, S.; Cavers, D.; Campbell, C.; Walter, F. Member checking: A tool to enhance trustworthiness or merely a nod to validation? Qual. Health Res. 2016, 26, 1802–1811. [Google Scholar] [CrossRef] [Green Version]
- van Someren, M.; Bernard, Y.; Sandberg, J. The Think Aloud Method: A Practical Approach to Modelling Cognitive; Academic Press: London, UK, 1994. [Google Scholar]
- Nickel, S.; Süß, W.; Lorentz, C.; Trojan, A. Long-term evaluation of community health promotion: Using capacity building as an intermediate outcome measure. Public Health 2018, 162, 9–15. [Google Scholar] [CrossRef]
- Nickel, S.; Süß, W.; Trojan, A. Measuring community capacities with ‘KEQ’: Psychometric tests results for a newly developed instrument for health promotion programs in Germany. In Capacity Building: Planning Programs and Prospects; Brown, D., Ed.; Nova Publishers: New York, NY, USA, 2016; pp. 55–84. [Google Scholar]
- Laverack, G. Evaluating community capacity: Visual representation and interpretation. Community Dev. J. 2006, 41, 266–276. [Google Scholar] [CrossRef]


{kind=link}
| Setting | Target Group | Aim | Stakeholders Involved in Participatory Groups | Number of Stakeholder Groups | Number of Group Meetings | Name, Source |
|---|---|---|---|---|---|---|
| Child care centers | Children | Increase PA levels of children | Educational staff in child care centers | 2 | 3–8 per group | QueB, [31] |
| School, university | Pupils | Develop sport-related health competence in pupils at secondary schools | Physical education teachers, pupils, college students, university lecturers | 6 | 3–7 per group | Health.edu, [32] |
| Workplace | Apprentices | Increase PA of apprentices during workhours | Apprentices and their teachers, company doctor | 3 | 4 per group | PArC-AVE, [33] |
| Rural communities | Older men | Increase motivation and participation in physical activity programs | Local physicians, members of sport associations, mayor, senior citizens representatives | 2 | 10 per group | ACTION4 Men [34] |
| Residential homes | Residents at residential homes | Implement a structured physical activity counseling program | Members of the home management, physicians, nurses, social workers, home residents | 3 | 3 per group | PATEN |
| 1. Description of the Group | |
| |
| 2. Capacity Building—General Skills | |
| Participation |
|
| Leadership |
|
| Problem assessment |
|
| Critical awareness, asking why |
|
| Mobilization of resources |
|
| External linkages, networks, links to others |
|
| Relationship to facilitating researcher |
|
| Project management |
|
| 3. Capacity Building—Specific Skills with Regard to Health Promotion/Physical Activity | |
| |
| Subproject | Setting | Project Team Size | Level of Qualification | Background/Discipline |
|---|---|---|---|---|
| QueB | Child care centers | 4 | 2 Project leaders | Health science, Social and health science for sports |
| 1 senior researcher | ||||
| 1 research assistant | ||||
| Health.edu | School, university | 6 | 1 Project leader | Sport science, Sports pedagogy, Sports education |
| 2 co-project leaders | ||||
| 1 PhD-student | ||||
| 2 research assistants | ||||
| PArC-AVE | Workplace | 3 | 1 Project leader | Sports science and sports |
| 1 senior researcher | ||||
| 1 research assistant | ||||
| ACTION4 men | Rural communities | 4 | 1 Project leader | Medical Sociology, Sports science |
| 1 co-project-leader | ||||
| 1 senior researcher | ||||
| 1 research assistant | ||||
| PATEN | Residential homes | 3 | 1 Project leader | Sports medicine, Sports science |
| 2 research assistants |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sauter, A.; Lindacher, V.; Rueter, J.; Curbach, J.; Loss, J. How Health Promoters Can Assess Capacity Building Processes in Setting-Based Approaches—Development and Testing of a Monitoring Instrument. Int. J. Environ. Res. Public Health 2020, 17, 407. https://doi.org/10.3390/ijerph17020407
Sauter A, Lindacher V, Rueter J, Curbach J, Loss J. How Health Promoters Can Assess Capacity Building Processes in Setting-Based Approaches—Development and Testing of a Monitoring Instrument. International Journal of Environmental Research and Public Health. 2020; 17(2):407. https://doi.org/10.3390/ijerph17020407
Chicago/Turabian StyleSauter, Alexandra, Verena Lindacher, Jana Rueter, Janina Curbach, and Julika Loss. 2020. "How Health Promoters Can Assess Capacity Building Processes in Setting-Based Approaches—Development and Testing of a Monitoring Instrument" International Journal of Environmental Research and Public Health 17, no. 2: 407. https://doi.org/10.3390/ijerph17020407
APA StyleSauter, A., Lindacher, V., Rueter, J., Curbach, J., & Loss, J. (2020). How Health Promoters Can Assess Capacity Building Processes in Setting-Based Approaches—Development and Testing of a Monitoring Instrument. International Journal of Environmental Research and Public Health, 17(2), 407. https://doi.org/10.3390/ijerph17020407