Sex and Gender Interactions on the Use and Impact of Recreational Cannabis


{kind=link}
{kind=link}
Abstract
:1. Introduction
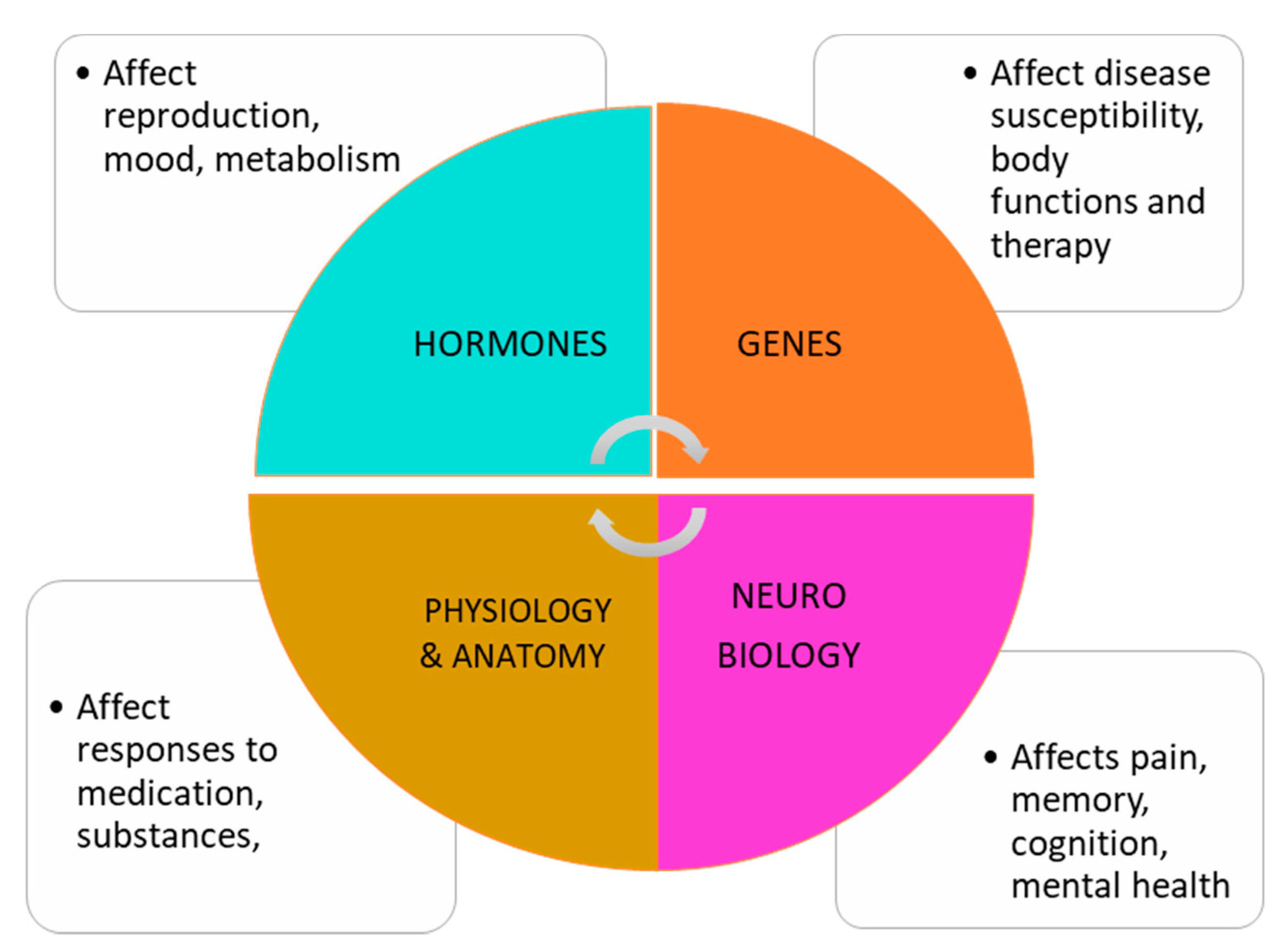
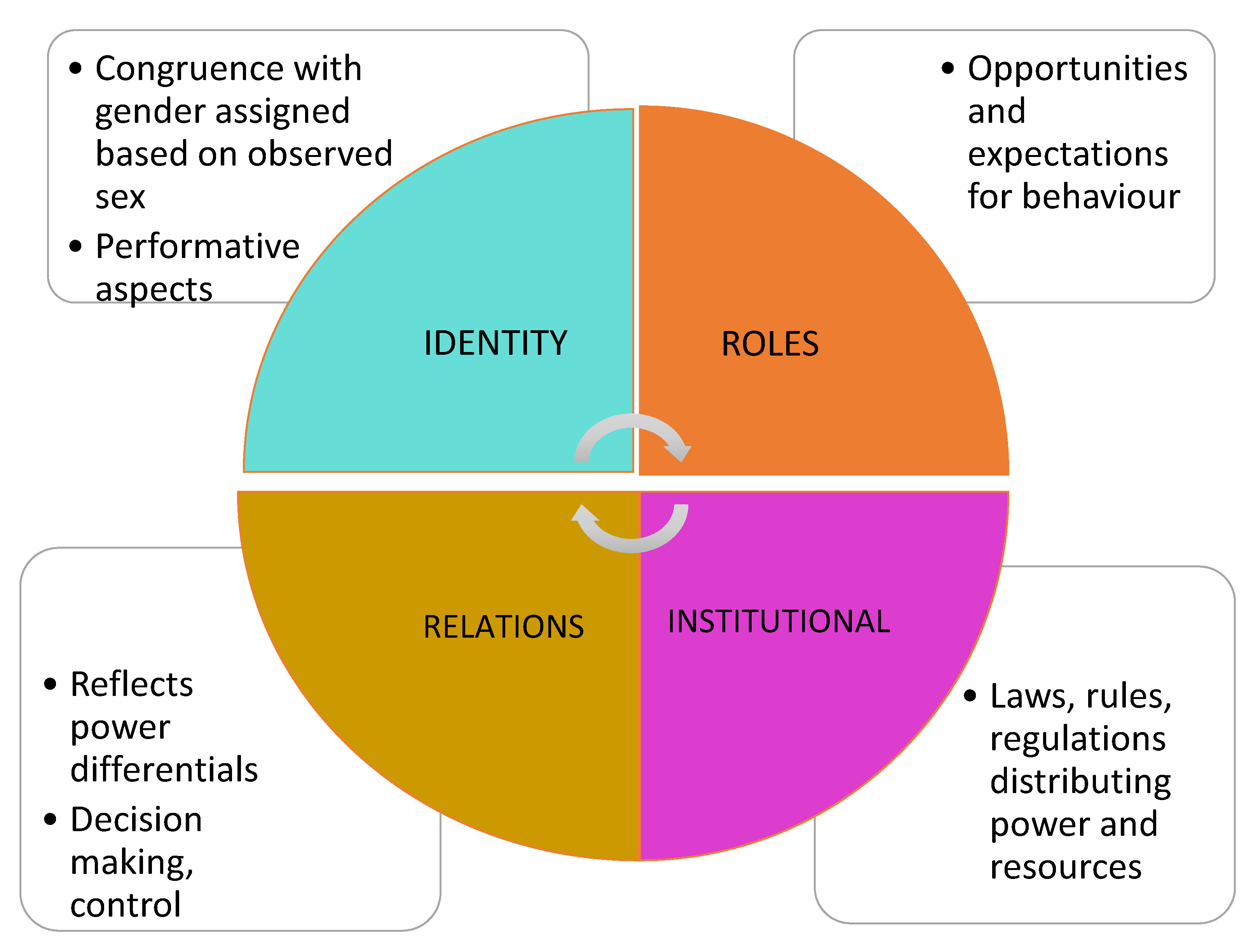
1.1. How Do Sex and Gender Matter in Substance Use?
1.2. Gendered Trends of Use
2. Materials and Methods
Scoping Review on Routes of Administration
- (Q1)
- How do sex and gender related factors impact:
- (a)
- The mode of cannabis or tobacco/nicotine use (ROA)?
- (b)
- The health effects of various cannabis routes of administration?
- (Q2)
- What existing health promotion, harm reduction and policy approaches to cannabis ROA are available? Do these approaches include a sex/gender/equity lens?
women; man; women; men; girl; boy; girls; boys; trans; transgender; female; male; sex; gender AND cigar*; e-cigar*; tobacco; nicotine; smoking; vaping; “heat not burn”; marijuana; cannabis; cannabinoid.
3. Results
3.1. Cannabis Use Dependence
3.2. Routes of Administration
3.3. Driving Under the Influence of Cannabis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. The Health and Social Effects of Nonmedical Cannabis Use; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Health Canada. Cannabis Laws and Regulations; Government of Canada: Ottawa, ON, Canada, 2019. [Google Scholar]
- Adinoff, B.; Reiman, A. Implementing social justice in the transition from illicit to legal cannabis. Am. J. Drug Alcohol Abus. 2019, 45, 673–688. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Prevalence of Cannabis Use in the Past Three Months, Self-Reported; Statistics Canada: Ottawa, ON, Canada, 2019. [Google Scholar]
- Schmidt, R.; Poole, N.; Greaves, L.; Hemsing, N. New Terrain: Tools to Integrate Trauma and Gender Informed Responses into Substance Use Practice and Policy; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2018. [Google Scholar]
- Becker, J.B.; McClellan, M.L.; Reed, B.G. Sex differences, gender and addiction. J. Neurosci. Res. 2017, 95, 136–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greaves, L.; Poole, N.; Boyle, E. Transforming Addiction: Gender, Trauma, Transdisciplinarity; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Einstein, G. Bridging the biological and social in neuroscience. In Transforming Addiction: Gender, Trauma, Transdisciplinarity; Greaves, L., Poole, N., Boyle, E., Eds.; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Meyer-Bahlburg, H.F.L. Intersex care development: Current priorities. LGBT Health 2017, 4, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Cranford, J.A.; Eisenberg, D.; Serras, A.M. Substance use behaviors, mental health problems, and use of mental health services in a probability sample of college students. Addict. Behav. 2009, 34, 134–145. [Google Scholar] [CrossRef]
- Carliner, H.; Mauro, P.M.; Brown, Q.L.; Shmulewitz, D.; Rahim-Juwel, R.; Sarvet, A.L.; Wall, M.M.; Martins, S.S.; Carliner, G.; Hasin, D.S. The widening gender gap in marijuana use prevalence in the U.S. During a period of economic change, 2002–2014. Drug Alcohol Depend. 2017, 170, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Felton, J.W.; Collado, A.; Shadur, J.M.; Lejuez, C.W.; MacPherson, L. Sex differences in self-report and behavioral measures of disinhibition predicting marijuana use across adolescence. Exp. Clin. Psychopharmacol. 2015, 23, 265–274. [Google Scholar] [CrossRef]
- Farmer, R.F.; Kosty, D.B.; Seeley, J.R.; Duncan, S.C.; Lynskey, M.T.; Rohde, P.; Klein, D.N.; Lewinsohn, P.M. Natural course of cannabis use disorders. Psychol. Med. 2015, 45, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.M.; Fairman, B.; Gilreath, T.; Xuan, Z.M.; Rothman, E.F.; Parnham, T.; Furr-Holden, C.D.M. Past 15-year trends in adolescent marijuana use: Differences by race/ethnicity and sex. Drug Alcohol Depend. 2015, 155, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Cuttler, C.; Mischley, L.K.; Sexton, M. Sex differences in cannabis use and effects: A cross-sectional survey of cannabis users. Cannabis Cannabinoid Res. 2016, 1, 166–175. [Google Scholar] [CrossRef] [Green Version]
- Legleye, S.; Piontek, D.; Pampel, F.; Goffette, C.; Khlat, M.; Kraus, L. Is there a cannabis epidemic model? Evidence from France, Germany and USA. Int. J. Drug Policy 2014, 25, 1103–1112. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, C.A.; Gallego, J.D.; Bockting, W.O. Demographic characteristics, components of sexuality and gender, and minority stress and their associations to excessive alcohol, cannabis, and illicit (noncannabis) drug use among a large sample of transgender people in the united states. J. Prim. Prev. 2017, 38, 419–445. [Google Scholar] [CrossRef] [PubMed]
- Baggio, S.; Deline, S.; Studer, J.; Mohler-Kuo, M.; Daeppen, J.B.; Gmel, G. Routes of administration of cannabis used for nonmedical purposes and associations with patterns of drug use. J. Adolesc. Health 2014, 54, 235–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, R.J.; Johnson, J.L.; Carter, C.I.; Arora, K. “I couldn’t say, I’m not a girl”—Adolescents talk about gender and marijuana use. Soc. Sci. Med. 2009, 68, 2029–2036. [Google Scholar] [CrossRef] [PubMed]
- Cooper, Z.D.; Craft, R.M. Sex-dependent effects of cannabis and cannabinoids: A translational perspective. Neuropsychopharmacology 2018, 43, 34. [Google Scholar] [CrossRef] [Green Version]
- Nia, A.B.; Mann, C.; Kaur, H.; Ranganathan, M. Cannabis use: Neurobiological, behavioral, and sex/gender considerations. Curr. Behav. Neurosci. Rep. 2018, 5, 271–280. [Google Scholar]
- Greaves, L.; Hemsing, N.; Brabete, A.C.; Poole, N. Sex, Gender and Cannabis; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2019. [Google Scholar]
- Hemsing, N.; Greaves, L. Gender norms, roles and relations and cannabis use patterns: A scoping review. Int. J. Environ. Res. Public Health. [Electronic Resource] in review.
- Jafari, S.; Tang, T. Diagnosis and treatment of marijuana dependence. Br. Columbia Med. J. 2016, 58, 315–317. [Google Scholar]
- Khan, S.S.; Secades-Villa, R.; Okuda, M.; Wang, S.; Perez-Fuentes, G.; Kerridge, B.T.; Blanco, C. Gender differences in cannabis use disorders: Results from the national epidemiologic survey of alcohol and related conditions. Drug Alcohol Depend. 2013, 130, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Kerridge, B.T.; Pickering, R.; Chou, P.; Saha, T.D.; Hasin, D.S. DSM-5 cannabis use disorder in the national epidemiologic survey on alcohol and related conditions-III: Gender-specific profiles. Addict. Behav. 2018, 76, 52–60. [Google Scholar] [CrossRef]
- Fogel, J.S.; Kelly, T.H.; Westgate, P.M.; Lile, J.A. Sex differences in the subjective effects of oral delta-thc in cannabis users. Pharmacol. Biochem. Behav. 2017, 152, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Marusich, J.A.; Lefever, T.W.; Antonazzo, K.R.; Craft, R.M.; Wiley, J.L. Evaluation of sex differences in cannabinoid dependence. Drug Alcohol Depend. 2014, 137, 20–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harte-Hargrove, L.C.; Dow-Edwards, D.L. Withdrawal from thc during adolescence: Sex differences in locomotor activity and anxiety. Behav. Brain Res. 2012, 231, 48–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlienz, N.J.; Budney, A.J.; Lee, D.C.; Vandrey, R. Cannabis withdrawal: A review of neurobiological mechanisms and sex differences. Curr. Addict. Rep. 2017, 4, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lev-Ran, S.; Imtiaz, S.; Taylor, B.J.; Shield, K.D.; Rehm, J.; Le Foll, B. Gender differences in health-related quality of life among cannabis users: Results from the national epidemiologic survey on alcohol and related conditions. Drug Alcohol Depend. 2012, 123, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Sherman, B.J.; McRae-Clark, A.L.; Baker, N.L.; Sonne, S.C.; Killeen, T.K.; Cloud, K.; Gray, K.M. Gender differences among treatment-seeking adults with cannabis use disorder: Clinical profiles of women and men enrolled in the achieving cannabis cessation-evaluating n-acetylcysteine treatment (accent) study. Am. J. Addict. 2017, 26, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, C.E.; Breivogel, C.S.; Gamage, T.F.; Gay, E.A.; Thomas, B.F.; Craft, R.M.; Wiley, J.L. Sex, thc, and hormones: Effects on density and sensitivity of cb1 cannabinoid receptors in rats. Drug Alcohol Depend. 2019, 194, 20–27. [Google Scholar] [CrossRef]
- Marusich, J.A.; Craft, R.M.; Lefever, T.W.; Wiley, J.L. The impact of gonadal hormones on cannabinoid dependence. Exp. Clin. Psychopharmacol. 2015, 23, 206–216. [Google Scholar] [CrossRef]
- Struik, D.; Sanna, F.; Fattore, L. The modulating role of sex and anabolic-androgenic steroid hormones in cannabinoid sensitivity. Front. Behav. Neurosci. 2018, 12, 249. [Google Scholar] [CrossRef] [Green Version]
- Craft, R.M.; Marusich, J.A.; Wiley, J.L. Sex differences in cannabinoid pharmacology: A reflection of differences in the endocannabinoid system? Life Sci. 2013, 92, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Wiley, J.L.; Burston, J.J. Sex differences in Δ9-tetrahydrocannabinol metabolism and in vivo pharmacology following acute and repeated dosing in adolescent rats. Neurosci. Lett. 2014, 576, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Britch, S.C.; Wiley, J.L.; Yu, Z.; Clowers, B.H.; Craft, R.M. Cannabidiol-δ9-tetrahydrocannabinol interactions on acute pain and locomotor activity. Drug Alcohol Depend. 2017, 175, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, L.M.; Bonugli, R.J.; McGlothen, K.S. The mothering experiences of women with substance use disorders. Adv. Nurs. Sci. 2016, 39, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.T.; Li, N.; McClure, E.A.; Sonne, S.C.; Gray, K.M. Gender differences in internalizing symptoms and suicide risk among men and women seeking treatment for cannabis use disorder from late adolescence to middle adulthood. J. Subst. Abus. Treat. 2016, 66, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtney, K.E.; Mejia, M.H.; Jacobus, J. Longitudinal studies on the etiology of cannabis use disorder: A review. Curr. Addict. Rep. 2017, 4, 43–52. [Google Scholar] [CrossRef] [PubMed]
- McHugh, R.K.; Votaw, V.R.; Sugarman, D.E.; Greenfield, S.F. Sex and gender differences in substance use disorders. Clin. Psychol. Rev. 2018, 66, 12–23. [Google Scholar] [CrossRef]
- Wilkinson, A.L.; Fleming, P.J.; Halpern, C.T.; Herring, A.H.; Harris, K.M. Adherence to gender-typical behavior and high frequency substance use from adolescence into young adulthood. Psychol. Men Masc. 2018, 19, 145–155. [Google Scholar] [CrossRef]
- Daniulaityte, R.; Zatreh, M.Y.; Lamy, F.R.; Nahhas, R.W.; Martins, S.S.; Sheth, A.; Carlson, R.G. A twitter-based survey on marijuana concentrate use. Drug Alcohol Depend. 2018, 187, 155–159. [Google Scholar] [CrossRef]
- Lee, D.C.; Crosier, B.S.; Borodovsky, J.T.; Sargent, J.D.; Budney, A.J. Online survey characterizing vaporizer use among cannabis users. Drug Alcohol Depend. 2016, 159, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Noack, R.; Hofler, M.; Lueken, U. Cannabis use patterns and their association with DSM-iv cannabis dependence and gender. Eur. Addict. Res. 2011, 17, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Doran, N.; Papadopoulos, A. Cannabis edibles: Behaviours, attitudes, and reasons for use. Environ. Health Rev. 2019, 62, 44–52. [Google Scholar] [CrossRef]
- Friese, B.; Slater, M.D.; Battle, R.S. Use of marijuana edibles by adolescents in california. J. Prim. Prev. 2017, 38, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Cooper, Z.D.; Haney, M. Comparison of subjective, pharmacokinetic, and physiological effects of marijuana smoked as joints and blunts. Drug Alcohol Depend. 2009, 103, 107–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spindle, T.R.; Cone, E.J.; Schlienz, N.J.; Mitchell, J.M.; Bigelow, G.E.; Flegel, R.; Hayes, E.; Vandrey, R. Acute pharmacokinetic profile of smoked and vaporized cannabis in human blood and oral fluid. J. Anal. Toxicol. 2019, 43, 233–258. [Google Scholar] [CrossRef] [PubMed]
- Matheson, J.; Sproule, B.; Di Ciano, P.; Fares, A.; Le Foll, B.; Mann, R.E.; Brands, B. Sex differences in the acute effects of smoked cannabis: Evidence from a human laboratory study of young adults. Psychopharmacology 2019, 1–12. [Google Scholar] [CrossRef]
- Dahl, S.L.; Sandberg, S. Female cannabis users and new masculinities: The gendering of cannabis use. Sociology 2015, 49, 696–711. [Google Scholar] [CrossRef] [Green Version]
- Perrine, C.G.; Pickens, C.M.; Boehmer, T.K. Characteristics of a Multistate Outbreak of Lung Injury Associated with E-Cigarette Use, or Vaping—United States; Centre for Disease Control and Prevention: Atlanta, GA, USA, 2019. [Google Scholar]
- Friese, B.; Slater, M.D.; Annechino, R.; Battle, R.S. Teen use of marijuana edibles: A focus group study of an emerging issue. J. Prim. Prev. 2016, 37, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Westfall, R.E.; Janssen, P.A.; Lucas, P.; Capler, R. Survey of medicinal cannabis use among childbearing women: Patterns of its use in pregnancy and retroactive self-assessment of its efficacy against ‘morning sickness’. Complementary Ther. Clin. Pract. 2006, 12, 27–33. [Google Scholar] [CrossRef]
- Banbury, A.; Zask, A.; Carter, S.M.; Van Beurden, E.; Tokley, R.; Passey, M.; Copeland, J. Smoking mull: A grounded theory model on the dynamics of combined tobacco and cannabis use among adult men. Health Promot. J. Aust. 2013, 24, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, L.; Bagot, K. Let’s be blunt: Consumption methods matter among black marijuana smokers. J. Stud. Alcohol Drugs 2016, 77, 451–456. [Google Scholar] [CrossRef] [Green Version]
- Timberlake, D.S. Characterizing blunt smokers by their acquisition of cannabis. Subst. Use Misuse 2018, 53, 1419–1423. [Google Scholar] [CrossRef]
- Schauer, G.L.; Berg, C.J.; Kegler, M.C.; Donovan, D.M.; Windle, M. Assessing the overlap between tobacco and marijuana: Trends in patterns of co-use of tobacco and marijuana in adults from 2003–2012. Addict. Behav. 2015, 49, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Koopman Gonzalez, S.J.; Cofie, L.E.; Trapl, E.S. “I just use it for weed”: The modification of little cigars and cigarillos by young adult African American male users. J. Ethn. Subst. Abus. 2017, 16, 66–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timberlake, D.S. The changing demographic of blunt smokers across birth cohorts. Drug Alcohol Depend. 2013, 130, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Macleod, J.; Robertson, R.; Copeland, L.; McKenzie, J.; Elton, R.; Reid, P. Cannabis, tobacco smoking, and lung function: A cross-sectional observational study in a general practice population. Br. J. Gen. Pract. 2015, 65, e89–e95. [Google Scholar] [CrossRef] [Green Version]
- Health Canada. Drug-Impaired Driving; Health Canada: Ottawa, ON, Canada, 2018. [Google Scholar]
- Jones, A.W.; Holmgren, A.; Kugelberg, F.C. Driving under the influence of cannabis: A 10-year study of age and gender differences in the concentrations of tetrahydrocannabinol in blood. Addiction 2008, 103, 452–461. [Google Scholar] [CrossRef]
- Whitehill, J.M.; Rivara, F.P.; Moreno, M.A. Marijuana-using drivers, alcohol-using drivers, and their passengers: Prevalence and risk factors among underage college students. JAMA Pediatr. 2014, 168, 618–624. [Google Scholar] [CrossRef] [Green Version]
- O’Malley, P.M.; Johnston, L.D. Driving after drug or alcohol use by U.S. High school seniors, 2001–2011. Am. J. Public Health 2013, 103, 2027–2034. [Google Scholar]
- Jones, C.B.; Hill, M.L.; Pardini, D.A.; Meier, M.H. Prevalence and correlates of vaping cannabis in a sample of young adults. Psychol. Addict. Behav. 2016, 30, 915. [Google Scholar] [CrossRef]
- Dubois, S.; Mullen, N.; Weaver, B.; Bédard, M. The combined effects of alcohol and cannabis on driving: Impact on crash risk. Forensic Sci. Int. 2015, 248, 94–100. [Google Scholar] [CrossRef]
- Earle, A.M.; Napper, L.E.; LaBrie, J.W.; Brooks-Russell, A.; Smith, D.J.; de Rutte, J. Examining interactions within the theory of planned behavior in the prediction of intentions to engage in cannabis-related driving behaviors. J. Am. Coll. Health 2019, 1–7. [Google Scholar] [CrossRef]
- Anderson, B.M.; Rizzo, M.; Block, R.I.; Pearlson, G.D.; O’Leary, D.S. Sex differences in the effects of marijuana on simulated driving performance. J. Psychoact. Drugs 2010, 42, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.M.; Rizzo, M.; Block, R.I.; Pearlson, G.D.; O’Leary, D.S. Sex, drugs, and cognition: Effects of marijuana. J. Psychoact. Drugs 2010, 42, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Bauer, G.R. Incorporating intersectionality theory into population health research methodology: Challenges and the potential to advance health equity. Soc. Sci. Med. 2014, 110, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Hankivsky, O.; Doyal, L.; Einstein, G.; Kelly, U.; Shim, J.; Weber, L.; Repta, R. The odd couple: Using biomedical and intersectional approaches to address health inequities. Glob. Health Action 2017, 10, 1326686. [Google Scholar] [CrossRef]
- Van Anders, S.M.; Steiger, J.; Goldey, K.L. Effects of gendered behavior on testosterone in women and men. Proc. Natl. Acad. Sci. USA 2015, 112, 13805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Centre on Substance Use and Addiction. Canada’s Low-Risk Alcohol Drinking Guidelines; CCSA: Ottawa, ON, Canada, 2018. [Google Scholar]
- Greaves, L. Raising the bar on women’s health promotion. In Making It Better: Gender Transformative Health Promotion; Greaves, L., Pederson, A., Poole, N., Eds.; CSPI: Toronto, ON, Canada, 2014; pp. 1–16. [Google Scholar]
- Pederson, A.; Poole, N.; Greaves, L.; Gerbrandt, J.; Fang, M.L. Envisioning gender-transformative health promotion. In Making It Better: Gender Transformative Health Promotion; Greaves, L., Pederson, A., Poole, N., Eds.; CSPI: Toronto, ON, Canada, 2014; pp. 17–41. [Google Scholar]
- Hakkarainen, P. Vaporizing the pot world—Easy, healthy, and cool. Drugs Alcohol Today 2016, 16, 185–193. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greaves, L.; Hemsing, N. Sex and Gender Interactions on the Use and Impact of Recreational Cannabis. Int. J. Environ. Res. Public Health 2020, 17, 509. https://doi.org/10.3390/ijerph17020509
Greaves L, Hemsing N. Sex and Gender Interactions on the Use and Impact of Recreational Cannabis. International Journal of Environmental Research and Public Health. 2020; 17(2):509. https://doi.org/10.3390/ijerph17020509
Chicago/Turabian StyleGreaves, Lorraine, and Natalie Hemsing. 2020. "Sex and Gender Interactions on the Use and Impact of Recreational Cannabis" International Journal of Environmental Research and Public Health 17, no. 2: 509. https://doi.org/10.3390/ijerph17020509
APA StyleGreaves, L., & Hemsing, N. (2020). Sex and Gender Interactions on the Use and Impact of Recreational Cannabis. International Journal of Environmental Research and Public Health, 17(2), 509. https://doi.org/10.3390/ijerph17020509