Cardiorespiratory Fitness and Device-Measured Sedentary Behaviour are Associated with Sickness Absence in Office Workers


Abstract
:1. Introduction
2. Materials and Methods
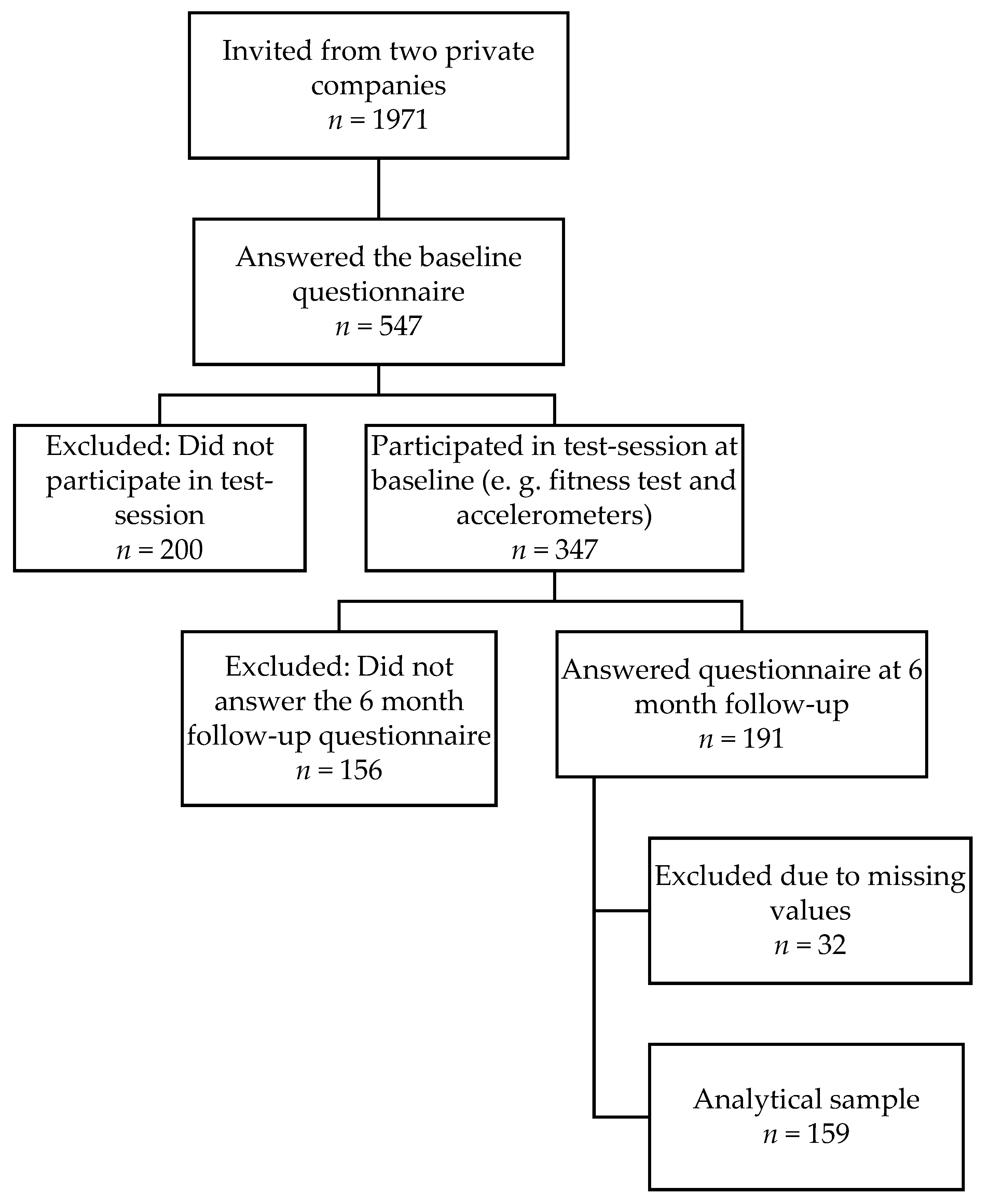
2.1. Study Design and Participants
2.2. Measures
2.3. Data Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nooijen, C.F.J.; Kallings, L.V.; Blom, V.; Ekblom, Ö.; Forsell, Y.; Ekblom, M.M. Common perceived barriers and facilitators for reducing sedentary behaviour among office workers. Int. J. Environ. Res. Public Health 2018, 15, 792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekblom-Bak, E.; Ekblom, Ö.; Andersson, G.; Wallin, P.; Söderling, J.; Hemmingsson, E.; Ekblom, B. Decline in cardiorespiratory fitness in the Swedish working force between 1995 and 2017. Scand. J. Med. Sci. Sports 2019, 29, 232. [Google Scholar] [CrossRef] [PubMed]
- Blair, N.S.; Cheng, N.Y.; Scott Holder, N.J. Is physical activity or physical fitness more important in defining health benefits? Med. Sci. Sports Exerc. 2001, 33, S379–S399. [Google Scholar] [CrossRef] [PubMed]
- Kohler, L.N.; Garcia, D.O.; Harris, R.B.; Oren, E.; Roe, D.J.; Jacobs, E.T. Adherence to diet and physical activity cancer prevention guidelines and cancer outcomes: A systematic review. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1018–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassuk, S.S.; Manson, J.E. Epidemiological evidence for the role of physical activity in reducing risk of type 2 diabetes and cardiovascular disease. J. Appl. Physiol. 2005, 99, 1193. [Google Scholar] [CrossRef] [PubMed]
- Rezende, L.F.M.; Rodrigues Lopes, M.; Rey-Lopez, J.P.; Matsudo, V.K.R.; Luiz, O.D.C. Sedentary behavior and health outcomes: An overview of systematic reviews. PLoS ONE 2014, 9, e105620. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and mental health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef]
- Swedish Social Insurance Agency. Kvinnors Sjukfrånvaro [Women’s Sick Leave]; Social Insurance Report 2014:14; Swedish Social Insurance Agency: Stockholm, Sweden, 2014. [Google Scholar]
- Beemsterboer, W.; Stewart, R.; Groothoff, J.; Nijhuis, F. A literature review on sick leave determinants (1984–2004). Int. J. Occup. Med. Environ. Health 2009, 22, 169. [Google Scholar] [CrossRef] [Green Version]
- Sieurin, L.; Josephson, M.; Vingård, E. Positive and negative consequences of sick leave for the individual, with special focus on part-time sick leave. Scand. J. Public Health 2009, 37, 50–56. [Google Scholar] [CrossRef]
- Bryngelson, A. Long-term sickness absence and social exclusion. Scand. J. Public Health 2009, 37, 839–845. [Google Scholar] [CrossRef]
- Sumanen, H.; Pietiläinen, O.; Lahelma, E.; Rahkonen, O. Short sickness absence and subsequent sickness absence due to mental disorders—A follow-up study among municipal employees. BMC Public Health 2017, 17, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Björkenstam, E.; Weitoft, G.R.; Lindholm, C.; Björkenstam, C.; Alexanderson, K.; Mittendorfer-Rutz, E. Associations between number of sick-leave days and future all-cause and cause-specific mortality: A population-based cohort study. BMC Public Health 2014, 14, 733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virtanen, M.; Ervasti, J.; Head, J.; Oksanen, T.; Salo, P.; Pentti, J.; Kouvonen, A.; Väänänen, A.; Suominen, S.; Koskenvuo, M.; et al. Lifestyle factors and risk of sickness absence from work: A multicohort study. Lancet Public Health 2018, 3, e545–e554. [Google Scholar] [CrossRef] [Green Version]
- van Amelsvoort, L.G.P.M.; Spigt, M.G.; Swaen, G.M.H.; Kant, I. Leisure time physical activity and sickness absenteeism a prospective study. Occup. Med. 2006, 56, 210–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holstila, A.; Rahkonen, O.; Lahelma, E.; Lahti, J. Changes in leisure-time physical activity and subsequent sickness absence due to any cause, musculoskeletal, and mental causes. J. Phys. Act. Health 2016, 13, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Lahti, J.; Laaksonen, M.; Lahelma, E.; Rahkonen, O. The impact of physical activity on sickness absence. Scand. J. Med. Sci. Sports 2010, 20, 191–199. [Google Scholar] [CrossRef]
- Proper, K.I.; van Den Heuvel, S.G.; De Vroome, E.M.; Hildebrandt, V.H.; Van Der Beek, A.J. Dose-response relation between physical activity and sick leave. Br. J. Sports Med. 2006, 40, 173. [Google Scholar] [CrossRef] [Green Version]
- Lahti, J.; Lahelma, E.; Rahkonen, O. Changes in leisure-time physical activity and subsequent sickness absence: A prospective cohort study among middle-aged employees. Prev. Med. 2012, 55, 618–622. [Google Scholar] [CrossRef]
- Amlani, N.; Munir, F. Does physical activity have an impact on sickness absence? A review. Sports Med. 2014, 44, 887–907. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, P.; Corbett, K.; Mehlum, I.S.; Bjerkedal, T. Impact of aerobic fitness on musculoskeletal sickness absence 5–15 years later: A cohort study of 227,201 male Norwegian employees. Occup. Environ. Med. 2012, 69, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Kyrolainen, H.; Hakkinen, K.; Kautiainen, H.; Santtila, M.; Pihlainen, K.; Hakkinen, A. Physical fitness, BMI and sickness absence in male military personnel. Occup. Med. 2008, 58, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Bernaards, C.M.; Proper, K.I.; Hildebrandt, V.H. Physical activity, cardiorespiratory fitness, and body mass index in relationship to work productivity and sickness absence in computer workers with preexisting neck and upper limb symptoms. J. Occup. Environ. Med. 2007, 49, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Kaleta, D.; Makowiec-Dabrowska, T.; Jegier, A. Leisure-time physical activity, cardiorespiratory fitness and work ability: A study in randomly selected residents of Lodz. Int. J. Occup. Med. Environ. Health 2004, 17, 457–464. [Google Scholar] [PubMed]
- Reeuwijk, K.G.; Robroek, S.J.; Niessen, M.A.; Kraaijenhagen, R.A.; Vergouwe, Y.; Burdorf, A. The prognostic value of the work ability index for sickness absence among office workers. PLoS ONE 2015, 10, e0126969. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendriksen, J.M.I.; Bernaards, M.C.; Steijn, M.P.W.; Hildebrandt, H.V. Longitudinal relationship between sitting time on a working day and vitality, work performance, presenteeism, and sickness absence. J. Occup. Environ. Med. 2016, 58, 784–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lallukka, T.; Kaila-Kangas, L.; Manty, M.; Koskinen, S.; Haukka, E.; Kausto, J.; Leino-Arjas, P.; Kaikkonen, R.; Halonen, J.I.; Shiri, R. Work-related exposures and sickness absence trajectories: A nationally representative follow-up study among Finnish working-aged people. Int. J. Environ. Res. Public Health 2019, 16, 2099. [Google Scholar] [CrossRef] [Green Version]
- Ekblom-Bak, E.; Björkman, F.; Hellenius, M.L.; Ekblom, B. A new submaximal cycle ergometer test for prediction of VO 2max. Scand. J. Med. Sci. Sports 2014, 24, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Björkman, F.; Ekblom-Bak, E.; Ekblom, Ö.; Ekblom, B. Validity of the revised Ekblom Bak cycle ergometer test in adults. Eur. J. Appl. Physiol. 2016, 116, 1627–1638. [Google Scholar] [CrossRef] [Green Version]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, K.L.; Conway, T.L.; Adams, M.A.; Husak, L.E.; Sallis, J.F. Comparison of older and newer generations of ActiGraph accelerometers with the normal filter and the low frequency extension. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trost, S.G.; Mciver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, S531–S543. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.M.E.E. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2014, 17, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Pfister, T.; Matthews, C.E.; Wang, Q.; Kopciuk, K.A.; Courneya, K.; Friedenreich, C. Comparison of two accelerometers for measuring physical activity and sedentary behaviour. BMJ Open Sport Exerc. Med. 2017, 3, e000227. [Google Scholar] [CrossRef] [Green Version]
- Ferrie, J.E.; Kivimäki, M.; Head, J.; Shipley, M.J.; Vahtera, J.; Marmot, M.G. A comparison of self-reported sickness absence with absences recorded in employers’ registers: Evidence from the Whitehall II study. Occup. Environ. Med. 2005, 62, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Lana, A.T.; de León, A.C.; García, M.T.M.; Jaime, A.A. Smoking and sickness absence among public health workers. Public Health 2005, 119, 144–149. [Google Scholar] [CrossRef]
- Mastekaasa, A. The gender gap in sickness absence: Long-term trends in eight European countries. Eur. J. Public Health 2014, 24, 656–662. [Google Scholar] [CrossRef] [Green Version]
- Sandvik, L.; Erikssen, G.; Thaulow, E. Long term effects of smoking on physical fitness and lung function: A longitudinal study of 1393 middle aged Norwegian men for seven years. BMJ 1995, 311, 715–718. [Google Scholar] [CrossRef] [Green Version]
- Ombrellaro, K.; Perumal, N.; Zeiher, J.; Hoebel, J.; Ittermann, T.; Ewert, R.; Dörr, M.; Keil, T.; Mensink, G.; Finger, J. Socioeconomic correlates and determinants of cardiorespiratory fitness in the general adult population: A systematic review and meta-analysis. Sports Med. 2018, 4, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Salvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question. J. Gen. Intern. Med. 2006, 21, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaikkonen, R.; Härkänen, T.; Rahkonen, O.; Gould, R.; Koskinen, S. Explaining educational differences in sickness absence: A population-based follow-up study. Scand. J. Work Environ. Health 2015, 41, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Ekblom-Bak, E.; Ekblom, Ö.; Fagman, E.; Angerås, O.; Schmidt, C.; Rosengren, A.; Börjesson, M.; Bergström, G. Fitness attenuates the prevalence of increased coronary artery calcium in individuals with metabolic syndrome. Eur. J. Prev. Cardiol. 2018, 25, 309–316. [Google Scholar] [CrossRef] [Green Version]
- Ekblom, Ö.; Ekblom-Bak, E.; Rosengren, A.; Hallsten, M.; Bergström, G.; Börjesson, M. Cardiorespiratory fitness, sedentary behaviour and physical activity are independently associated with the metabolic syndrome, results from the SCAPIS pilot study. PLoS ONE 2015, 10, e0131586. [Google Scholar] [CrossRef] [Green Version]
- Høgsbro, C.; Davidsen, M.; Sørensen, J. Long-term sickness absence from work due to physical inactivity: A registry-based study. Scand. J. Public Health 2018, 46, 306–313. [Google Scholar] [CrossRef]
- Quist, H.G.; Thomsen, B.L.; Christensen, U.; Clausen, T.; Holtermann, A.; Bjorner, J.B.; Andersen, L.L. Influence of lifestyle factors on long-term sickness absence among female healthcare workers: A prospective cohort study. BMC Public Health 2014, 14, 1084. [Google Scholar] [CrossRef] [Green Version]
- van Den Heuvel, S.G.; Boshuizen, H.C.; Hildebrandt, V.H.; Blatter, B.M.; Ariëns, G.A.; Bongers, P.M. Effect of sporting activity on absenteeism in a working population. Br. J. Sports Med. 2005, 39, 15. [Google Scholar] [CrossRef] [Green Version]
- Ekblom, O.; Ekblom-Bak, E.; Bolam, K.A.; Ekblom, B.; Schmidt, C.; Soderberg, S.; Bergstrom, G.; Borjesson, M. Concurrent and predictive validity of physical activity measurement items commonly used in clinical settings—Data from SCAPIS pilot study. BMC Public Health 2015, 15, 978. [Google Scholar] [CrossRef] [Green Version]
- Fridolfsson, J.; Borjesson, M.; Arvidsson, D. A biomechanical re-examination of physical activity measurement with accelerometers. Sensors 2018, 18, 3399. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Descriptives | ALL | High Fitness | Low Fitness | High MVPA | Low MVPA | Low SED | High SED |
|---|---|---|---|---|---|---|---|
| n = 159 | n = 80 | n = 79 | n = 79 | n = 80 | n = 79 | n = 80 | |
| Fitness: (m ± SD) (mL/min/kg) | 39.5 ± 8.6 | 46.5 ± 4.7 *** | 32.4 ± 5.2 *** | 40.9 ± 8.4 * | 38.1 ± 8.7 * | 40.2 ± 8.1 | 38.8 ± 9.1 |
| Physical activity: (m ± SD) | |||||||
| % in MVPA | 6.5 ± 2.4 | 6.7 ± 2.5 | 6.2 ± 2.2 | 8.2 ± 2.0 *** | 4.7 ± 0.9 *** | 6.9 ± 2.5 ** | 6.0 ± 2.2 ** |
| % in LIPA | 33.0 ± 6.1 | 33.9 ± 5.8 | 32.2 ± 6.3 | 34.0 ± 5.9 * | 32.0 ± 6.2 * | 35.7 ± 5.5 *** | 30.4 ± 5.5 *** |
| % in MPA | 5.3 ± 1.9 | 5.3 ± 1.9 | 5.4 ± 1.9 | 6.6 ± 1.8 *** | 4.1 ± 0.8 *** | 5.6 ± 2.0 | 5.0 ± 1.6 |
| % in VPA | 1.1 ± 1.2 | 1.4 ± 1.4 *** | 0.8 ±0.8 *** | 1.7 ± 1.4 *** | 0.6 ± 0.6 *** | 1.3 ± 1.1 * | 0.9 ± 1.2 * |
| Sedentary time (m ± SD) % in SED | 60.8 ± 8.4 | 59.7 ± 7.8 | 61.9 ± 9.0 | 59.6 ± 8.0 | 61.9 ± 8.8 | 54.0 ± 5.2 *** | 67.5 ± 5.0 *** |
| Covariates | |||||||
| Age (m ± SD) | 43.0 ± 8.3 | 40.3 ± 6.7 *** | 45.8 ± 8.9 *** | 42.6 ± 8.8 | 43.4 ± 7.9 | 42.3 ± 7.1 | 43.7 ± 9.4 |
| Women (%) | 66.7 | 53.8 *** | 79.7 *** | 69.6 | 63.8 | 70.9 | 62.5 |
| Education (%) | |||||||
| Compulsory education | 2.5 | 1.3 | 3.8 | 2.5 | 2.5 | 0.0 *** | 5.0 *** |
| Upper secondary education | 38.4 | 32.5 | 44.3 | 34.2 | 42.5 | 25.3 *** | 51.3 *** |
| University or equivalent | 54.7 | 58.8 | 50.6 | 60.8 | 48.8 | 70.9 *** | 38.8 *** |
| Higher academic education | 4.4 | 7.5 | 1.3 | 2.5 | 6.3 | 3.8 *** | 5.0 *** |
| Smoking yes/sometimes (%) | 7.5 | 5.0 | 10.1 | 11.4 | 3.8 | 2.5 * | 12.5 * |
| Lower general health (%) a | 17.0 | 8.8 ** | 25.3 ** | 11.4 | 22.5 | 16.5 | 17.5 |
| Sickness absence (%) | |||||||
| Duration ≥ 8 days | 22.0 | 11.3 *** | 32.9 *** | 22.8 | 21.3 | 16.5 | 27.5 |
| Frequency ≥ 2 times | 40.3 | 30.0 ** | 50.6 ** | 40.5 | 40.0 | 32.9 | 47.5 |
| Sickness Absence Duration | |||||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | |
| Odds Ratio (95% Confidence Interval) | |||||
| Fitness (mL/min/kg) | 0.92 (0.87–0.96) | 0.92 (0.87–0.98) | 0.91 (0.86–0.97) | 0.92 (0.86–0.98) | 0.92 (0.86–0.98) |
| % in LIPA | 0.98 (0.92–1.04) | 0.98 (0.92–1.04) | 0.98 (0.91–1.04) | 0.97 (0.91–1.04) | 1.00 (0.92–1.09) |
| % in MPA | 0.97 (0.79–1.19) | 0.96 (0.78–1.18) | 0.93 (0.75–1.16) | 0.94 (0.75–1.17) | 0.96 (0.76–1.21) |
| % in VPA | 0.80 (0.54–1.17) | 0.82 (0.55–1.23) | 0.83 (0.55–1.25) | 0.87 (0.57–1.31) | 1.04 (0.67–1.61) |
| % in MVPA | 0.93 (0.79–1.10) | 0.93 (0.79–1.11) | 0.92 (0.77–1.10) | 0.93 (0.78–1.12) | 0.98 (0.81–1.19) |
| % in SED | 1.03 (0.98–1.07) | 1.03 (0.98–1.08) | 1.02 (0.97–1.07) | 1.02 (0.97–1.07) | 1.00 (0.95–1.06) |
| Sickness Absence Frequency | |||||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | |
| Odds Ratio (95% Confidence Interval) | |||||
| Fitness (mL/min/kg) | 0.93 (0.90–0.97) | 0.93 (0.89–0.98) | 0.94 (0.89–0.98) | 0.94 (0.89–0.99) | 0.94 (0.89–0.99) |
| % in LIPA | 0.97 (0.92–1.02) | 0.96 (0.91–1.02) | 0.96 (0.91–1.01) | 0.96 (0.91–1.01) | 0.99 (0.92–1.06) |
| % in MPA | 0.96 (0.81–1.15) | 0.95 (0.80–1.14) | 0.94 (0.78–1.12) | 0.94 (0.79–1.13) | 0.98 (0.81–1.18) |
| % in VPA | 0.89 (0.67–1.18) | 0.89 (0.66–1.19) | 0.90 (0.67–1.21) | 0.92 (0.68–1.25) | 1.07 (0.78–1.46) |
| % in MVPA | 0.95 (0.83–1.09) | 0.94 (0.82–1.09) | 0.94 (0.81–1.08) | 0.94 (0.82–1.09) | 1.00 (0.86–1.16) |
| % in SED | 1.03 (0.99–1.08) | 1.04 (1.00–1.09) | 1.04 (1.00–1.08) | 1.04 (1.00–1.08) | 1.03 (0.99–1.08) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drake, E.; Ekblom, M.M.; Ekblom, Ö.; Kallings, L.V.; Blom, V. Cardiorespiratory Fitness and Device-Measured Sedentary Behaviour are Associated with Sickness Absence in Office Workers. Int. J. Environ. Res. Public Health 2020, 17, 628. https://doi.org/10.3390/ijerph17020628
Drake E, Ekblom MM, Ekblom Ö, Kallings LV, Blom V. Cardiorespiratory Fitness and Device-Measured Sedentary Behaviour are Associated with Sickness Absence in Office Workers. International Journal of Environmental Research and Public Health. 2020; 17(2):628. https://doi.org/10.3390/ijerph17020628
Chicago/Turabian StyleDrake, Emma, Maria M. Ekblom, Örjan Ekblom, Lena V. Kallings, and Victoria Blom. 2020. "Cardiorespiratory Fitness and Device-Measured Sedentary Behaviour are Associated with Sickness Absence in Office Workers" International Journal of Environmental Research and Public Health 17, no. 2: 628. https://doi.org/10.3390/ijerph17020628
APA StyleDrake, E., Ekblom, M. M., Ekblom, Ö., Kallings, L. V., & Blom, V. (2020). Cardiorespiratory Fitness and Device-Measured Sedentary Behaviour are Associated with Sickness Absence in Office Workers. International Journal of Environmental Research and Public Health, 17(2), 628. https://doi.org/10.3390/ijerph17020628