Bacterial Profile, Multi-Drug Resistance and Seasonality Following Lower Limb Orthopaedic Surgery in Tropical and Subtropical Australian Hospitals: An Epidemiological Cohort Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hospital and Patient Data
2.2. Microbiological Data
2.3. Meteorological Data
2.4. Statistical Analysis
3. Results
3.1. Meteorological Factors, Patient and Swab Characteristics
3.2. Bacterial Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
List of All Included Orthopaedic Procedures
| Number | ICD Code | Procedure Description |
| 1. | 1488 50393-00 | Bone graft to pelvis |
| 2. | 1488 48200-00 | Bone graft to femur |
| 3. | 1488 48203-00 | Bone graft to femur with internal fixation |
| 4. | 1489 47522-00 | Hemi-arthroplasty of femur (Austin Moore) |
| 5. | 1489 49312-00 | Excision arthroplasty of hip |
| 6. | 1489 49315-00 | Partial arthroplasty of hip |
| 7. | 1489 90607-00 | Resurfacing of hip, unilateral |
| 8. | 1489 90607-01 | Resurfacing of hip, bilateral |
| 9. | 1489 49318-00 | Total arthroplasty of hip, unilateral |
| 10. | 1489 49319-00 | Total arthroplasty of hip, bilateral |
| 11. | 1490 50121-00 | Transplantation of iliopsoas tendon to greater trochanter |
| 12. | 1490 50387-00 | Transfer of iliopsoas tendon to greater trochanter |
| 13. | 1490 50387-01 | Transfer of abdominal musculature to greater trochanter |
| 14. | 1490 50387-02 | Transfer of adductors to ischium |
| 15. | 1491 49300-00 | Arthrodesis of sacro-iliac joint |
| 16. | 1491 49306-00 | Arthrodesis of hip |
| 17. | 1491 48500-00 | Epiphysiodesis of femur |
| 18. | 1491 48506-00 | Epiphysiodesis of femur and tibia and fibula |
| 19. | 1491 50224-09 | En bloc resection of lesion of soft tissue involving penis (prosthesis) |
| 20. | 1491 50224-10 | En bloc resection of lesion of soft tissue involving penis (allograft) |
| 21. | 1491 50224-11 | En bloc resection of lesion of soft tissue involving penis (autograft) |
| 22. | 1491 96225-00 | Arthroscopic repair of hip |
| 23. | 1491 90552-00 | Other repair of hip |
| 24. | 1511 49561-02 | Arthroscopic removal of loose body of knee with debridement/osteoplasty/chondroplasty |
| 25. | 1511 49562-02 | Arthroscopic removal of loose body of knee with chondroplasty/drilling/implant |
| 26. | 1512 49509-01 | Arthrodesis of knee |
| 27. | 1512 49512-00 | Arthrodesis of knee with removal of prosthesis |
| 28. | 1513 48206-00 | Bone graft to tibia |
| 29. | 1513 48209-00 | Bone graft to tibia with internal fixation |
| 30. | 1514 49561-00 | Arthroscopic lateral release of knee with debridement/osteoplasty/chondroplasty |
| 31. | 1514 49562-00 | Arthroscopic lateral release of knee with chondroplasty/drilling/implant |
| 32. | 1515 50411-00 | Resection of distal femur and proximal tibia with knee fusion |
| 33. | 1515 50414-00 | Resection of distal femur and proximal tibia with knee fusion and rotationplasty |
| 34. | 1516 50357-00 | Transfer of rectus femoris hamstring tendon |
| 35. | 1516 50357-01 | Transfer of medial hamstring tendon |
| 36. | 1516 50357-02 | Transfer of lateral hamstring tendon |
| 37. | 1516 50360-00 | Transfer of combined medial and lateral hamstring tendon |
| 38. | 1516 49503-03 | Transfer of tendon or ligament of knee (not elsewhere defined) |
| 39. | 1516 50423-00 | Transfer of fibula to tibia with external fixation |
| 40. | 1517 49561-01 | Arthroscopic menisectomy of knee with debridement, osteoplasty or chondroplasty |
| 41. | 1517 49562-01 | Arthroscopic menisectomy of knee with chondroplasty/drilling/implant |
| 42. | 1518 49517-00 | Hemi-arthroplasty of knee |
| 43. | 1518 49518-00 | Total arthroplasty of knee, unilateral |
| 44. | 1518 49519-00 | Total arthroplasty of knee, bilateral |
| 45. | 1518 49534-01 | Total replacement arthroplasty of patellofemoral joint of knee |
| 46. | 1519 49521-00 | Total arthroplasty of knee with bone graft to femur, unilateral |
| 47. | 1519 49521-01 | Total arthroplasty of knee with bone graft to femur, bilateral |
| 48. | 1519 49521-02 | Total arthroplasty of knee with bone graft to tibia, unilateral |
| 49. | 1519 49521-03 | Total arthroplasty of knee with bone graft to tibia, bilateral |
| 50. | 1519 49524-00 | Total arthroplasty of knee with bone graft to femur and tibia, unilateral |
| 51. | 1519 49524-01 | Total arthroplasty of knee with bone graft to femur and tibia, bilateral |
| 52. | 1492 49346-00 | Revision of partial arthroplasty of hip |
| 53. | 1492 49324-00 | Revision of total arthroplasty of hip |
| 54. | 1492 49327-00 | Revision of total arthroplasty of hip with bone graft to acetabulum |
| 55. | 1492 49330-00 | Revision of total arthroplasty of hip with bone graft to femur |
| 56. | 1492 49333-00 | Revision of total arthroplasty of hip with bone graft to acetabulum and femur |
| 57. | 1492 49339-00 | Revision of total arthroplasty of hip with anatomic specific allograft to acetabulum |
| 58. | 1492 49342-00 | Revision of total arthroplasty of hip with anatomic specific allograft to femur |
| 59. | 1492 49345-00 | Revision of total arthroplasty of hip with anatomic specific allograft to acetabulum and femur Internal |
| 60. | 1521 47588-00 | Fixation of intra-articular fracture of femoral condyle with repair |
| 61. | 1521 47588-01 | Internal fixation of intra-articular fracture of tibial articular surface of knee with repair |
| 62. | 1521 47591-00 | Internal fixation of intra-articular fracture of femoral condyle and tibial articular surface |
| 63. | 1522 49539-00 | Arthroscopic reconstruction of knee |
| 64. | 1522 49539-01 | Reconstruction of knee |
| 65. | 1522 49542-00 | Arthroscopic reconstruction of cruciate ligament of knee and repair meniscus |
| 66. | 1522 49542-01 | Reconstruction of cruciate ligament of knee with repair of meniscus |
| 67. | 1522 90611-00 | Patellar tendon shortening |
| 68. | 1522 90611-01 | Patellar tendon advancement |
| 69. | 1522 50417-00 | Reconstruction of knee involving transfer of fibula and tibia or repair of quads |
| 70. | 1523 49530-00 | Revision of total arthroplasty of knee with bone graft to femur |
| 71. | 1523 49530-01 | Revision of total arthroplasty of knee with bone graft to tibia |
| 72. | 1523 49533-00 | Revision of total arthroplasty of knee with bone graft to femur and tibia |
| 73. | 1523 49554-00 | Revision of total arthroplasty of knee with anatomic specific allograft |
| 74. | 1524 49545-00 | Revision of arthrodesis of knee |
| 75. | 1524 49548-00 | Revision of patellofemoral stabilisation of knee |
| 76. | 1524 49551-00 | Revision of reconstructive surgery of knee |
| 77. | 1524 49527-00 | Revision of total arthroplasty of knee |
| 78. | 1524 90562-00 | Patella resurfacing |
Appendix B
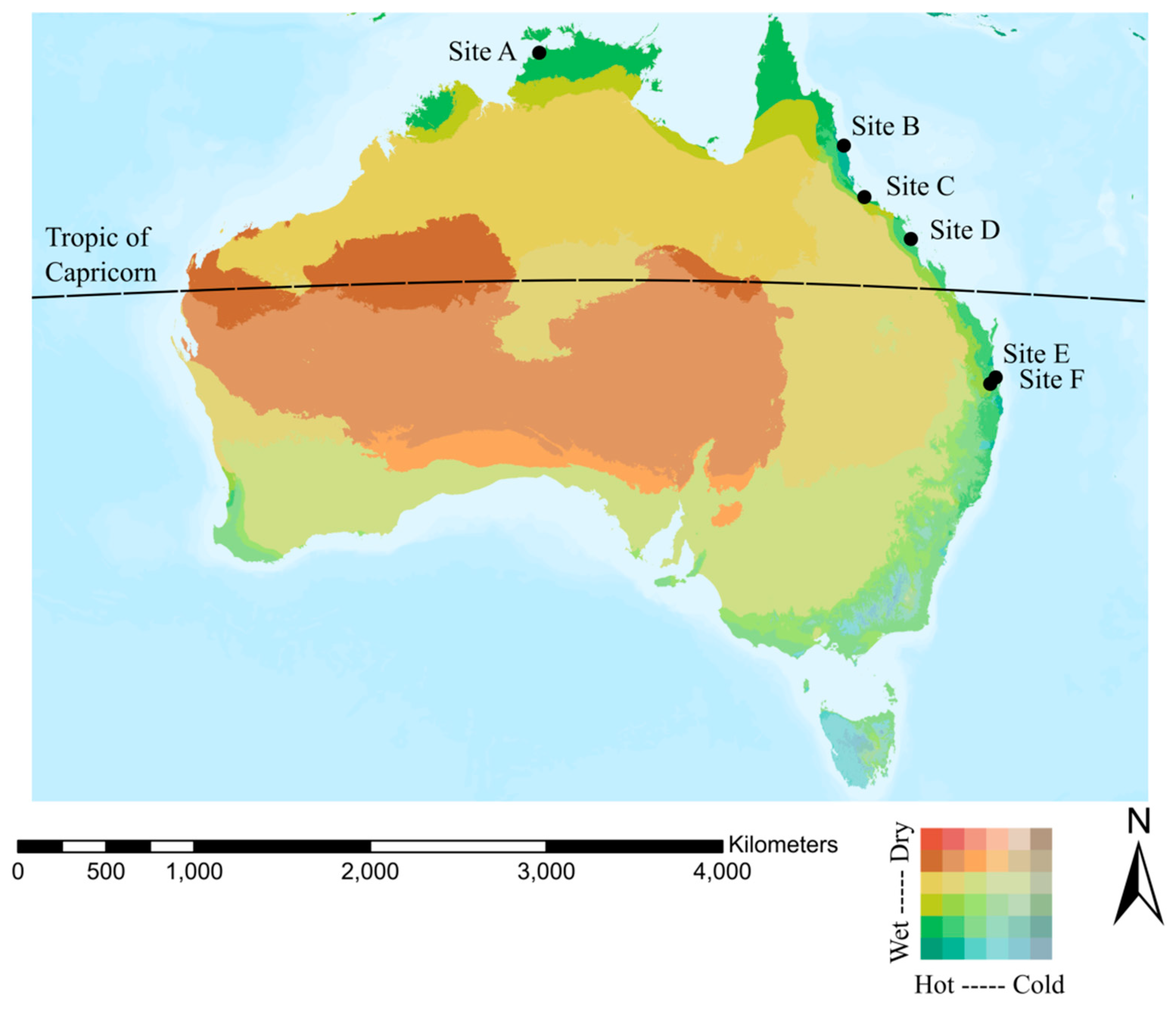
Admission, Swab and Weather Station Data by Hospital Site
| Status | Hospital | Location Latitude and Longitude | Number of Weather Stations Within 25 km Radius | Total Admission Events | Admissions Followed by Positive Swabs | Percentage |
| Tropical | Site A | −12.354860, 130.882845 | 25 | 1107 | 71 | 6.4% |
| Tropical | Site B | −16.912178, 145.768408 | 10 | 2818 | 149 | 5.3% |
| Tropical | Site C | −19.320384, 146.762324 | 3 | 2937 | 202 | 6.9% |
| Tropical | Site D | −21.145531, 149.155603 | 7 | 1767 | 97 | 5.5% |
| Subtropical | Site E | −27.227687, 153.104899 | 13 | 2942 | 84 | 2.9% |
| Subtropical | Site F | −27.389547, 153.022753 | 24 | 7536 | 264 | 3.5% |
Appendix C
Profile of Bacteria Cultured Within 12 Months Following Lower Limb Orthopaedic Procedures in Australian Tropical and Subtropical Hospitals
| Group | Species | Total (n = 867) | Tropical (n = 519) | Sub-tropical (n = 348) | p |
| Staphylococcus | Total | 527 (60.8%) | 320 (61.7%) | 270 (59.5%) | 0.52 |
| S. aureus | 426 (80.8%) | 259 (80.9%) | 167 (80.7%) | 0.94 | |
| MRSA | 101 (19.2%) | 61 (19.1%) | 40 (19.3%) | ||
| MDR S. aureus | 166 (31.5%) | 115 (35.9%) | 51 (24.6%) | 0.006 | |
| CONS | Total | 47 (5.4%) | 24 (4.6%) | 23 (6.6%) | 0.21 |
| S. capitis | 7 (14.9%) | 3 (12.5%) | 4 (17.4%) | 0.49 | |
| S. epidermidis | 32 (68.1%) | 18 (75.0%) | 14 (60.9%) | ||
| S. lugdunensis | 5 (10.6%) | 1 (4.2%) | 4 (17.4%) | ||
| S. haemolyticus | 3 (6.4%) | 2 (8.3%) | 1 (4.3%) | ||
| MDR CONS | 31 (66.0%) | 17 (70.8%) | 14 (60.9%) | 0.47 | |
| Enterococcus | Total | 59 (6.8%) | 32 (6.2%) | 27 (7.8%) | 0.36 |
| E. faecalis | 50 (84.7%) | 30 (93.8%) | 20 (74.1%) | 0.066 | |
| E. faecium | 9 (15.3%) | 2 (6.3%) | 7 (25.9%) | ||
| MDR Enterococcus | 22 (37.3%) | 12 (37.5%) | 10 (37.0%) | 0.97 | |
| Streptococcus | Total | 82 (9.5%) | 57 (11.0%) | 25 (7.2%) | 0.061 |
| Group A | 41 (50.0%) | 32 (56.1%) | 9 (36.0%) | 0.010 | |
| Group B | 13 (15.9%) | 6 (10.5%) | 7 (28.0%) | ||
| Group C | 16 (19.5%) | 14 (24.6%) | 2 (8.0%) | ||
| Group G | 9 (11.0%) | 4 (7.0%) | 5 (20.0%) | ||
| Peptostreptococcus | 1 (1.2%) | 0 | 1 (4.0%) | ||
| Pneumonia Group | 1 (1.2%) | 1 (1.8%) | 0 | ||
| Viridans Group | 1 (1.2%) | 0 | 1 (4.0%) | ||
| MDR Streptococcus | 0 | ||||
| Enterobacteriaceae | Total | 129 (14.9%) | 67 (12.9%) | 62 (17.8%) | 0.047 |
| M. morganii | 11 (8.5%) | 5 (7.5%) | 6 (9.7%) | 0.67 | |
| P. mirabilis | 13 (10.1%) | 7 (10.4%) | 6 (9.7%) | ||
| E. coli | 20 (15.5%) | 11 (16.4%) | 9 (14.5%) | ||
| K. pneumoniae | 22 (17.1%) | 8 (11.9%) | 14 (22.6%) | ||
| S. marcescens | 27 (20.9%) | 16 (23.9%) | 11 (17.7%) | ||
| E. cloacae | 36 (27.9%) | 20 (29.9%) | 16 (25.8%) | ||
| MDR Enterobacteriaceae | 50 (38.8%) | 26 (38.8%) | 24 (38.7%) | 0.99 | |
| Non-fermenters | Total | 224 (25.8%) | 149 (28.7%) | 75 (21.6%) | 0.018 |
| A. baumannii | 12 (5.4%) | 11 (7.4%) | 1 (1.3%) | 0.065 | |
| P. aeruginosa | 212 (94.6%) | 138 (92.6%) | 74 (98.7%) | ||
| MDR Nonfermenters | 18 (8.0%) | 17 (11.4%) | 1 (1.3%) | 0.009 |
Appendix D
Bacterial Species by Season in a Subtropical Location
| Bacterial Species | Overall | Sub-Tropical | Subtropical | ||||
| Spring | Summer | Autumn | Winter | p | |||
| n | n | n (%) | n (%) | n (%) | n (%) | ||
| Staphylococcus | 527 | 207 | 43 (60.6%) | 50 (56.2%) | 62 (60.2%) | 52 (61.2%) | 0.91 |
| MDR S. aureus | 51 | 7 (16.3%) | 12 (24.0%) | 14 (22.6%) | 18 (34.6%) | 0.21 | |
| CONS | 47 | 23 | 5 (7.0%) | 3 (3.4%) | 12 (11.7%) | 3 (3.5%) | 0.069 |
| MDR CONS | 14 | 4 (80.0%) | 2 (66.7%) | 6 (50.0%) | 2 (66.7%) | 0.75 | |
| Enterococcus | 59 | 27 | 6 (8.5%) | 4 (4.5%) | 13 (12.6%) | 4 (4.7%) | 0.12 |
| MDR Enteroccoccus | 10 | 1 (16.7%) | 2 (50.0%) | 5 (38.5%) | 2 (50.0%) | 0.67 | |
| Streptococcus | 82 | 25 | 7 (9.9%) | 4 (4.5%) | 6 (5.8%) | 8 (9.4%) | 0.45 |
| MDR Streptococcus | 0 | n/a | n/a | n/a | n/a | n/a | |
| Enterobacteriaceae | 129 | 62 | 11 (15.5%) | 23 (25.8%) | 12 (11.7%) | 16 (18.8%) | 0.075 |
| MDR Enterobacteriaceae | 24 | 5 (45.5%) | 8 (34.8%) | 8 (66.7%) | 3 (18.3%) | 0.072 | |
| Non-fermenters | 224 | 75 | 12 (16.9%) | 23 (25.8%) | 22 (21.4%) | 18 (21.2%) | 0.60 |
| MDR Non-fermenters | 1 | 1 (8.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.16 | |
Appendix E
Bacterial Species by Season in a Tropical Location
| Bacterial Species | Overall | Tropical | Tropical | ||||
| Spring | Summer | Autumn | Winter | p | |||
| n | n | n (%) | n (%) | n (%) | n (%) | ||
| Staphylococcus | 527 | 320 | 73 (60.3%) | 85 (66.4%) | 96 (63.6%) | 66 (55.5%) | 0.32 |
| MDR S. aureus | 115 | 29 (39.7%) | 26 (30.6%) | 37 (38.5%) | 23 (34.8%) | 0.61 | |
| CONS | 47 | 24 | 7 (5.8%) | 2 (1.6%) | 8 (5.3%) | 7 (5.9%) | 0.30 |
| MDR CONS | 17 | 4 (57.1%) | 1 (50.0%) | 5 (62.5%) | 7 (100.0%) | 0.21 | |
| Enterococcus | 59 | 32 | 10 (8.3%) | 6 (4.7%) | 9 (6.0%) | 7 (5.9%) | 0.70 |
| MDR Enteroccoccus | 12 | 5 (50.0%) | 1 (16.7%) | 2 (22.2%) | 4 (57.1%) | 0.31 | |
| Streptococcus | 82 | 57 | 16 (13.2%) | 11 (8.6%) | 11 (7.3%) | 19 (16.0%) | 0.090 |
| MDR Streptococcus | 0 | n/a | n/a | n/a | n/a | n/a | |
| Enterobacteriaceae | 129 | 67 | 18 (14.9%) | 21 (16.4%) | 11 (7.3%) | 17 (14.3%) | 0.10 |
| MDR Enterobacteriaceae | 26 | 7 (38.9%) | 8 (38.1%) | 4 (36.4%) | 7 (41.2%) | 1.00 | |
| Nonfermenters | 224 | 149 | 39 (32.2%) | 39 (30.5%) | 45 (29.8%) | 26 (21.8%) | 0.29 |
| MDR Nonfermenters | 17 | 5 (12.8%) | 6 (15.4%) | 4 (8.9%) | 2 (7.7%) | 0.73 | |
References
- Moriarty, T.F.; Kuehl, R.; Coenye, T.; Metsemakers, W.J.; Morgenstern, M.; Schwarz, E.M.; Riool, M.; Zaat, S.A.J.; Khana, N.; Kates, S.L.; et al. Orthopaedic device-related infection: Current and future interventions for improved prevention and treatment. EFORT Open Rev. 2016, 1, 89–99. [Google Scholar] [CrossRef]
- Jamei, O.; Gjoni, S.; Zenelaj, B.; Kressmann, B.; Belaieff, W.; Hannouche, D.; Uckay, I. Which Orthopaedic Patients Are Infected with Gram-negative Non-fermenting Rods? J. Bone Joint Infect. 2017, 2, 73–76. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Pastor, J.C.; Munoz-Mahamud, E.; Vilchez, F.; Garcia-Ramiro, S.; Bori, G.; Sierra, J.; Martinez, J.A.; Font, L.; Mensa, J.; Soriano, A. Outcome of acute prosthetic joint infections due to gram-negative bacilli treated with open debridement and retention of the prosthesis. Antimicrob. Agents Chemother. 2009, 53, 4772–4777. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, P.H.; Lee, M.S.; Hsu, K.Y.; Chang, Y.H.; Shih, H.N.; Ueng, S.W. Gram-negative prosthetic joint infections: Risk factors and outcome of treatment. Clin. Infect. Dis. 2009, 49, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Vasso, M.; Schiavone Panni, A.; De Martino, I.; Gasparini, G. Prosthetic knee infection by resistant bacteria: The worst-case scenario. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3140–3146. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Webster, T.J. Bacteria antibiotic resistance: New challenges and opportunities for implant-associated orthopedic infections. J. Orthop. Res. 2018, 36, 22–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, H.K.; Chen, M.C.; Lee, W.C.; Yang, W.E.; Chang, C.H. Seasonal Temperature and Pin Site Care Regimen Affect the Incidence of Pin Site Infection in Pediatric Supracondylar Humeral Fractures. BioMed Res. Int. 2015, 2015, 838913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kane, P.; Chen, C.; Post, Z.; Radcliff, K.; Orozco, F.; Ong, A. Seasonality of infection rates after total joint arthroplasty. Orthopedics 2014, 37, e182–e186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkinson, B.; Armit, D.; McEwen, P.; Lorimer, M.; Harris, I.A. Is Climate Associated With Revision for Prosthetic Joint Infection After Primary TKA? Clin. Orthop. Relat. Res. 2018, 476, 1200–1204. [Google Scholar] [CrossRef]
- Haws, B.E.; Braun, B.M.; Creech, T.B.; Barnard, E.R.; Miller, A.N. Is There a Seasonal Influence on Orthopaedic Surgical Wound Infection Rates? J. Surg. Orthop. Adv. 2017, 25, 172–175. [Google Scholar]
- Anthony, C.A.; Peterson, R.A.; Polgreen, L.A.; Sewell, D.K.; Polgreen, P.M. The Seasonal Variability in Surgical Site Infections and the Association With Warmer Weather: A Population-Based Investigation. Infect. Control Hosp. Epidemiol. 2017, 38, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Durkin, M.J.; Dicks, K.V.; Baker, A.W.; Moehring, R.W.; Chen, L.F.; Sexton, D.J.; Lewis, S.S.; Anderson, D.J. Postoperative infection in spine surgery: Does the month matter? J. Neurosurg. Spine 2015, 23, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leekha, S.; Diekema, D.J.; Perencevich, E.N. Seasonality of staphylococcal infections. Clin. Microbiol. Infect. 2012, 18, 927–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBride, M.E.; Duncan, W.C.; Knox, J.M. The environment and the microbial ecology of human skin. Appl. Environ. Microbiol. 1977, 33, 603–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armit, D.; Vickers, M.; Parr, A.; Van Rosendal, S.; Trott, N.; Gunasena, R.; Parkinson, B. Humidity a potential risk factor for prosthetic joint infection in a tropical Australian hospital. ANZ J. Surg. 2018, 88, 1298–1301. [Google Scholar] [CrossRef]
- Fisman, D.N. Seasonality of infectious diseases. Annu. Rev. Public Health 2007, 28, 127–143. [Google Scholar] [CrossRef] [Green Version]
- Australian Government, Bureau of Meteorology, Climate Classification Maps. Available online: http://www.bom.gov.au/jsp/ncc/climate_averages/climate-classifications/index.jsp?maptype=kpngrp#maps (accessed on 24 November 2019).
- Centers for Disease Control and Prevention, Procedure-Associated Module, Surgical Site Infection (SSI) Event. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf (accessed on 24 November 2019).
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Dudareva, M.; Hotchen, A.J.; Ferguson, J.; Hodgson, S.; Scarborough, M.; Atkins, B.L.; McNally, M.A. The microbiology of chronic osteomyelitis: Changes over ten years. J. Infect. 2019, 79, 189–198. [Google Scholar] [CrossRef]
- Tuon, F.F.; Cieslinski, J.; Ono, A.F.M.; Goto, F.L.; Machinski, J.M.; Mantovani, L.K.; Kosop, L.R.; Namba, M.S.; Rocha, J.L. Microbiological profile and susceptibility pattern of surgical site infections related to orthopaedic trauma. Int. Orthop. 2019, 43, 1309–1313. [Google Scholar] [CrossRef]
- Ma, X.; Han, S.; Ma, J.; Chen, X.; Bai, W.; Yan, W.; Wang, K. Epidemiology, microbiology and therapeutic consequences of chronic osteomyelitis in northern China: A retrospective analysis of 255 Patients. Sci. Rep. 2018, 8, 14895. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.D.; Wang, Y.P.; Chen, C.F.; Chen, H.P. The incidence rate, trend and microbiological aetiology of prosthetic joint infection after total knee arthroplasty: A 13 years’ experience from a tertiary medical center in Taiwan. J. Microbiol. Immunol. Infect. 2018, 51, 717–722. [Google Scholar] [CrossRef]
- Norton, T.D.; Skeete, F.; Dubrovskaya, Y.; Phillips, M.S.; Bosco, J.D., 3rd; Mehta, S.A. Orthopedic surgical site infections: Analysis of causative bacteria and implications for antibiotic stewardship. Am. J. Orthop. 2014, 43, E89–E92. [Google Scholar] [PubMed]
- Tucaliuc, D.; Alexa, O.; Tuchilus, C.G.; Ursu, R.G.; Tucaliuc, E.S.; Iancu, L.S. Retrospective study on the etiological spectrum and antibiotic resistance in infections associated with osteosynthesis materials. Revista Medico-Chirurgicala a Societatii de Medici si Naturalisti din Iasi 2014, 118, 147–153. [Google Scholar] [PubMed]
- Rosteius, T.; Jansen, O.; Fehmer, T.; Baecker, H.; Citak, M.; Schildhauer, T.A.; Gessmann, J. Evaluating the microbial pattern of periprosthetic joint infections of the hip and knee. J. Med. Microbiol. 2018, 67, 1608–1613. [Google Scholar] [CrossRef] [PubMed]
- Lenguerrand, E.; Whitehouse, M.R.; Beswick, A.D.; Kunutsor, S.K.; Foguet, P.; Porter, M.; Blom, A.W.; National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. Risk factors associated with revision for prosthetic joint infection following knee replacement: An observational cohort study from England and Wales. Lancet Infect. Dis. 2019, 19, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Poultsides, L.A.; Triantafyllopoulos, G.K.; Sakellariou, V.I.; Memtsoudis, S.G.; Sculco, T.P. Infection risk assessment in patients undergoing primary total knee arthroplasty. Int. Orthop. 2018, 42, 87–94. [Google Scholar] [CrossRef]
- Kong, L.; Cao, J.; Zhang, Y.; Ding, W.; Shen, Y. Risk factors for periprosthetic joint infection following primary total hip or knee arthroplasty: A meta-analysis. Int. Wound J. 2017, 14, 529–536. [Google Scholar] [CrossRef]
- Springer, B.D.; Cahue, S.; Etkin, C.D.; Lewallen, D.G.; McGrory, B.J. Infection burden in total hip and knee arthroplasties: An international registry-based perspective. Arthroplast. Today 2017, 3, 137–140. [Google Scholar] [CrossRef] [Green Version]
- Gruskay, J.; Smith, J.; Kepler, C.K.; Radcliff, K.; Harrop, J.; Albert, T.; Vaccaro, A. The seasonality of postoperative infection in spine surgery. J. Neurosurg. Spine 2013, 18, 57–62. [Google Scholar] [CrossRef]
- Vickers, M.; Pelecanos, A.; Tran, M.; Eriksson, L.; Assoum, M.; Harris, P.; Jaiprakash, A.; Parkinson, B.; Dulhunty, J.; Crawford, R. Association between higher ambient temperature and orthopaedic infection rates: A systematic review and meta-analysis. ANZ J. Surg. 2019, 89. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Sub-Category | Total (n = 867) | Tropical (n = 519) | Sub-Tropical (n = 348) | p |
|---|---|---|---|---|---|
| Age at procedure | 68.3 (16.0) | 65.9 (16.9) | 72.0 (13.8) | <0.001 | |
| Gender 1 | Female | 389 (46.3%) | 213 (42.3%) | 176 (52.2%) | 0.005 |
| Male | 452 (53.7%) | 291 (57.7%) | 161 (47.8%) | ||
| Surgical site | Hip | 512 (59.1%) | 284 (54.7%) | 228 (65.5%) | 0.002 |
| Knee | 355 (40.9%) | 235 (45.3%) | 120 (34.5%) | ||
| Procedure type | Primary | 695 (80.2%) | 441 (85.0%) | 254 (73.0%) | <0.001 |
| Revision | 172 (19.8%) | 78 (15.0%) | 94 (27.0%) | ||
| Polymicrobial swab | 180 (20.8%) | 119 (22.9%) | 61 (17.5%) | 0.055 | |
| Number of procedures during admission (median (IQR)) | 1 (1 − 1) | 1 (1 − 1) | 1 (1 − 1) | 0.50 | |
| MDR status | MDR S. aureus | 166 (31.5%) | 115 (35.9%) | 54 (24.6%) | 0.006 |
| MDR Nonfermenters (P. aeruginosa and A. baumannii) | 18 (8.0%) | 17 (11.4%) | 1 (1.3%) | 0.009 | |
| Organism count | Enterobacteriaceae | 129 (14.9%) | 67 (12.9%) | 62 (17.8%) | 0.047 |
| Nonfermenters (P. aeruginosa & A. baumannii) | 224 (25.8%) | 149 (28.7%) | 75 (21.6%) | 0.018 | |
| Swab collection for Staphylococcus (n = 527) | Superficial <30 days | 236 (44.8%) | 126 (39.4%) | 110 (53.1%) | 0.004 |
| Deep 30–90 days | 131 (24.9%) | 82 (25.6%) | 49 (23.7%) | ||
| Late 90–365 days | 160 (30.4%) | 112 (35.0%) | 48 (23.3%) | ||
| Enterobacteriaceae swab site (n = 129) | Hip | 61 (47.3%) | 25 (37.3%) | 36 (58.1%) | 0.038 |
| Knee | 41 (31.8%) | 26 (38.8%) | 15 (24.2%) | ||
| Other body site | 10 (7.8%) | 8 (11.9%) | 2 (3.2%) | ||
| Not specified | 17 (13.2%) | 8 (11.9%) | 9 (14.5%) | ||
| Organism/Organism Group | Antibiotic 1 | Percentage of MDR Isolates Susceptible |
|---|---|---|
| MDR S. aureus 2 (n = 166) | Flucloxacillin or Cephazolin | 30% |
| Erythromycin or Clindamycin | 50% | |
| Trimethoprim-Sulphamethoxazole | 79% | |
| Vancomycin | 99% | |
| MDR CONS (n = 31) | Flucloxacillin or Cephazolin | 10% |
| Erythromycin or Clindamycin | 16% | |
| Trimethoprim-Sulphamethoxazole | 48% | |
| Vancomycin | 100% | |
| MDR Enterococci (n = 22) | Ampicillin | 73% |
| Vancomycin | 77% | |
| Teicoplanin | 95% | |
| MDR Enterobacteriaceae (n = 50) | Ampicillin | 0% |
| Amoxicillin-Clavulanic Acid | 4% | |
| Cephazolin | 4% | |
| Trimethoprim-Sulphamethoxazole | 82% | |
| Ceftriaxone | 86% | |
| Piperacillin-Tazobactam | 88% | |
| Gentamicin | 90% | |
| Ciprofloxacin | 90% | |
| Meropenem | 100% | |
| MDR P. aeruginosa and A. baumannii (n = 18) | Ceftazidime | 44% |
| Ciprofloxacin | 50% | |
| Piperacillin-Tazobactam | 61% | |
| Gentamicin | 67% | |
| Meropenem | 67% | |
| Streptococci (n = 0) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vickers, M.L.; Ballard, E.L.; Harris, P.N.A.; Knibbs, L.D.; Jaiprakash, A.; Dulhunty, J.M.; Crawford, R.W.; Parkinson, B. Bacterial Profile, Multi-Drug Resistance and Seasonality Following Lower Limb Orthopaedic Surgery in Tropical and Subtropical Australian Hospitals: An Epidemiological Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 657. https://doi.org/10.3390/ijerph17020657
Vickers ML, Ballard EL, Harris PNA, Knibbs LD, Jaiprakash A, Dulhunty JM, Crawford RW, Parkinson B. Bacterial Profile, Multi-Drug Resistance and Seasonality Following Lower Limb Orthopaedic Surgery in Tropical and Subtropical Australian Hospitals: An Epidemiological Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(2):657. https://doi.org/10.3390/ijerph17020657
Chicago/Turabian StyleVickers, Mark L., Emma L. Ballard, Patrick N. A. Harris, Luke D. Knibbs, Anjali Jaiprakash, Joel M. Dulhunty, Ross W. Crawford, and Benjamin Parkinson. 2020. "Bacterial Profile, Multi-Drug Resistance and Seasonality Following Lower Limb Orthopaedic Surgery in Tropical and Subtropical Australian Hospitals: An Epidemiological Cohort Study" International Journal of Environmental Research and Public Health 17, no. 2: 657. https://doi.org/10.3390/ijerph17020657
APA StyleVickers, M. L., Ballard, E. L., Harris, P. N. A., Knibbs, L. D., Jaiprakash, A., Dulhunty, J. M., Crawford, R. W., & Parkinson, B. (2020). Bacterial Profile, Multi-Drug Resistance and Seasonality Following Lower Limb Orthopaedic Surgery in Tropical and Subtropical Australian Hospitals: An Epidemiological Cohort Study. International Journal of Environmental Research and Public Health, 17(2), 657. https://doi.org/10.3390/ijerph17020657