Prevalence of Alpha(α)-Thalassemia in Southeast Asia (2010–2020): A Meta-Analysis Involving 83,674 Subjects


Abstract
:1. Introduction
2. Materials and Methods
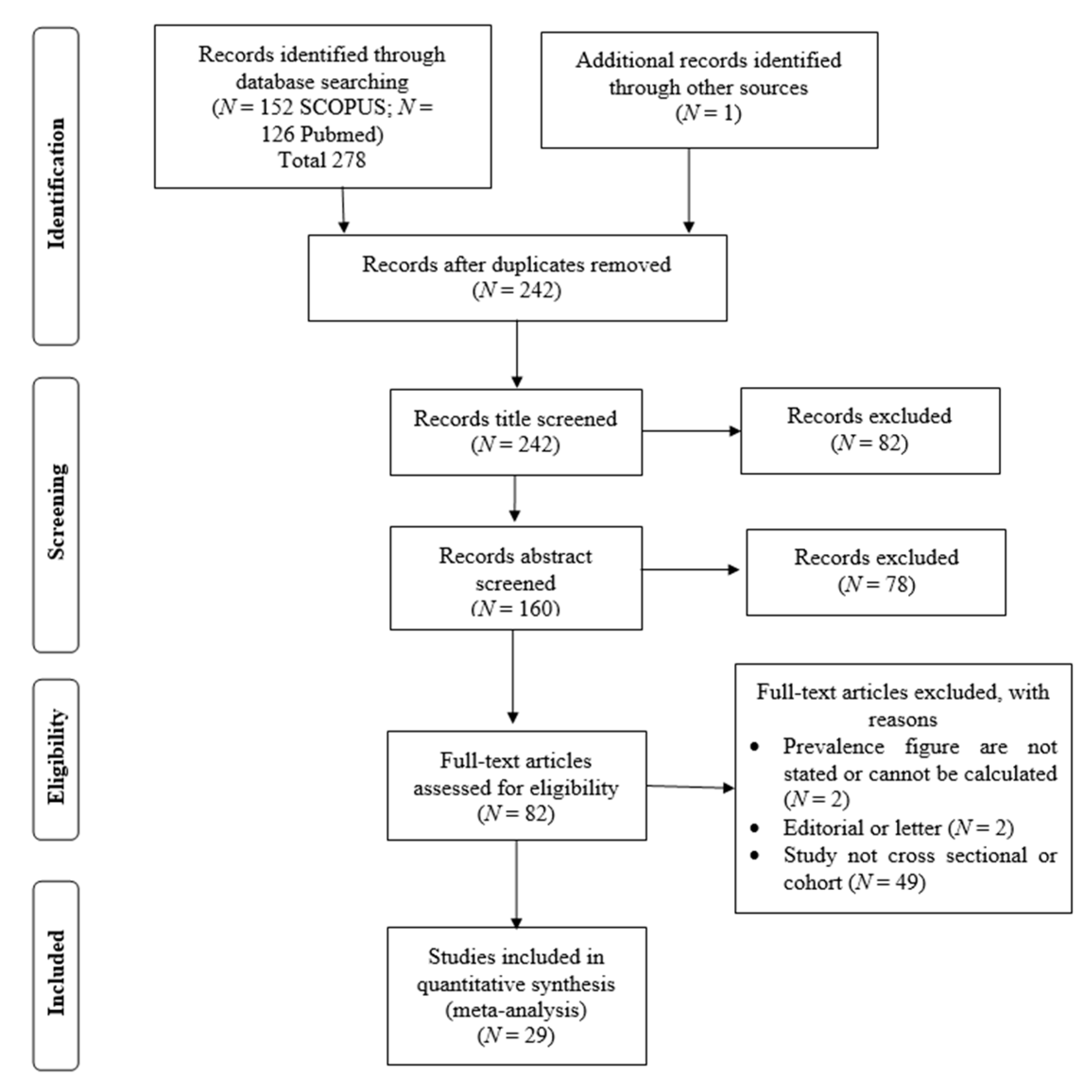
2.1. Study Guidelines and Literature Search
2.2. Selection of Studies and Data Extraction
2.3. Statistical Analyses
3. Results
3.1. Study Characteristics
3.2. Meta-Analysis Outcomes
3.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Higgs, D.R.; Engel, J.D.; Stamatoyannopoulos, G. Thalassemia. Lancet 2012, 379, 73–383. [Google Scholar] [CrossRef]
- Rosnah, B.; Rosline, H.; Zaidah, A.W.; Noor Haslina, M.N.; Marini, R.; Shafini, M.Y.; Nurul Ain, F.A. Detection of common deletional alpha-thalassemia spectrum by molecular technique in Kelantan, Northeastern Malaysia. ISRN Hematol. 2010, 2012, 462969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.I.M.A.; Lee, P.C.; Wee, Y.C.; Tan, K.L.; Mahali, N.F.; George, E.; Chua, K.H. High prevalence of alpha- and beta-thalassemia in the Kadazadusuns in East Malaysia: Challenges in providing effective health care for an indigenous group. J. Biomed. Biotechnol. 2010, 2010, 706872. [Google Scholar] [CrossRef] [PubMed]
- Azma, R.Z.; Ainoon, O.; Hafiza, A.; Azlin, I.; Noor Farisah, A.R.; Nor Hidayati, S.; Noor Hamidah, H. Molecular characteristic of alpha thalassemia among patients diagnosed in UKM medical centre. Malays. J. Pathol. 2014, 36, 27–32. [Google Scholar]
- Kulaphisit, M.; Kampuansai, J.; Leecharoenkiat, K.; Wathikthinnakon, M.; Kangwanpong, D.; Munkongdee, T.; Svasti, S.; Fucharoen, S.; Smith, D.R.; Lithanatudom, P. A comprehensive ethnic-based analysis of alpha thalassemia allele frequency in northern Thailand. Sci. Rep. 2017, 7, 4690. [Google Scholar] [CrossRef]
- Farashi, S.; Harteveld, C.L. Molecular basis of α-thalassemia. Blood Cells Mol. Dis. 2018, 70, 43–53. [Google Scholar] [CrossRef]
- Chui, D.H.K. Alpha-Thalassemia: Hb H disease and Hb Bart’s hydrops fetalis. Ann. N. Y. Acad. Sci. 2005, 1054, 25–32. [Google Scholar] [CrossRef]
- Weatherall, D.J.; Clegg, J.B. The Thalassemia Syndrome, 4th ed.; Blackwell Scientific Publication: Oxford, UK, 2011. [Google Scholar]
- Casale, M.; Meloni, A.; Filosa, A.; Cuccia, L.; Caruso, V.; Palazzi, G.; Rita Gamberini, M.; Pitrolo, L.; Caterina Putti, M.; Giuseppe D’Ascola, D.; et al. Multiparametric Cardiac Magnetic Resonance Survey in Children with Thalassemia Major. Circ. Cardiovasc. Imaging 2015, 8, e003230. [Google Scholar] [CrossRef] [Green Version]
- Kurtoglu, A.U.; Kurtoglu, E.; Temizkan, A.K. Effect of iron overload on endocrinopathies in patients with beta-thalassaemia major and intermedia. Endokrynol. Pol. 2012, 63, 260–263. [Google Scholar]
- Suthat, F.; Pranee, W. Haemoglobinopathies in Southeast Asian. Indian J. Med. Res. 2011, 134, 498–506. [Google Scholar]
- Galanello, R.; Cao, A. Alpha-thalassemia. Gen. Med. 2011, 13, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Kuesap, J.; Chaijaroenkul, W.; Rungsihirunrat, K.; Pongjantharasatien, K.; Na-Bangchang, K. Coexistance of Malaria and Thalassemia in malaria endemic areas of Thailand. Korean J. Parasitol. 2015, 53, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Rosanas-Uegell, A.; Senn, N.; Raru, P.; Aponte, J.J.; Reeder, J.C.; Siba, P.M.; Michon, P.; Mueller, I. Lack of associations of α(+)-thalassemia with the risk of Plasmodium falciparum and Plasmodium vivax infection and disease in a cohort of children aged 3-21 months from Papua New Guinea. Int. J. Parasitol. 2012, 42, e1000097. [Google Scholar] [CrossRef]
- Vento, S.; Cainelli, F.; Cesario, F. Infections and thalassemia. Lancet Infect. Dis. 2006, 6, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Ryan, K.; Bain, B.J.; Worthington, D.; James, J.; Plews, D.; Mason, A.; Roper, D.; Rees, D.C.; de la Salle, B.; Streetly, A.; et al. Significant haemoglobinopathies: Guidelines for screening and diagnosis. Br. J. Haematol. 2010, 149, 35–49. [Google Scholar] [CrossRef]
- Lithanatudom, P.; Khampan, P.; Smith, D.R.; Svasti, S.; Fucharoen, S.; Kangwanpong, D.; Kampuansai, J. The prevalence of alpha-thalssemia amongst Tai and Mon-Khmer ethnic groups residing in northern Thailand: A population-based study. Hematology 2016, 21, 480–485. [Google Scholar] [CrossRef] [Green Version]
- O’Riordan, S.; Hien, T.T.; Miles, K.; Allen, A.; Quyen, N.N.; Hung, N.Q.; Anh, D.Q.; Tuyen, L.N.; Khia, D.B.; Thai, C.Q.; et al. Large scale screening for haemoglobin disorders in southern Vietnam: Implications for avoidance and management. Br. J. Haematol. 2010, 150, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Loberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Dersimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Light, R.J.; Pillemer, D.B. Summing up: The Science of Reviewing Research; Harvard University Press: Cambridge, MA, USA, 1984. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H.R. Comprehensive meta-analysis version 2. Englewood 2005, 104, 188–191. [Google Scholar]
- Munkongdee, T.; Tanakulmas, J.; Butthep, P.; Winichagoon, P.; Main, B.; Yiannakis, M.; George, J.; Devenish, R.; Fucharoen, S.; Svasti, S. Molecular epidemiology of hemoglobinpathies in Cambodia. Hemoglobin 2016, 40, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Jomoui, W.; Fucharoen, G.; Sanchaisuriya, K.; Charoenwijitkul, P.; Maneesarn, J.; Xu, X.; Fucharoen, S. Genetic origin of α0-thalassemia (SEA deletion) in Southeast Asian populations and application to accurate prenatal diagnosis of Hb Bart’s hydrops fetalis syndrome. J. Hum. Gen. 2017, 62, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Wongprachum, K.; Sanchaisuriya, K.; Dethvongphanh, M.; Norcharoen, B.; Vidamaly, V.; Sanchaisuriya, P.; Fucharoen, S.; Fucharoen, G.; Schelp, F.P. Molecular heterogeneity of thalassemia among pregnant Laotian women. Acta Hematol. 2016, 135, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Tritipsombut, J.; Sanchaisuriya, K.; Phollarp, P.; Bouakhasith, D.; Sanchaisuriya, P.; Fucharoen, G.; Fucharoen, S.; Schelp, F.P. Micromapping of thalassemia and hemoglobinopathies in different regions of northeast Thailand and Vientaine, Laos people’s democratic republic. Hemoglobin 2012, 36, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Azma, R.Z.; Ainoon, O.; Azlin, I.; Hamenuddin, H.; Hadi, N.A.; Tatt, W.K.; Syazana, I.N.; Asmaliza, A.M.; Das, S.; Hamidah, N.H. Prevalence of iron deficiency anaemia and thalassemia trait among undergraduate medical students. Clin. Ter. 2012, 163, 287–291. [Google Scholar]
- Jameela, S.; Sharifah Sabirah, S.O.; Babam, J.; Phan, C.L.; Visalachy, P.; Chang, K.M.; Salwana, M.A.; Zuridah, A.; Subramanian, Y.; Rahimah, A. Thalassemia screening among students in a secondary school in Ampang, Malaysia. Med. J. Malays. 2011, 66, 522–524. [Google Scholar]
- Mohd Yatim, N.F.; Abd Rahim, M.; Menon, K.; Al-Hassan, F.M.; Ahmad, R.; Manocha, A.B.; Saleem, M.; Yahaya, B.H. Molecular characterization of α and β-thalassaemia among malay patients. Int. J. Mol. Sci. 2014, 15, 8835–8845. [Google Scholar] [CrossRef]
- Charoenkwan, P.; Taweephol, R.; Sirichotiyakul, S.; Tantiprabha, W.; Sae-Tung, R.; Suanta, S.; Sakdasirisathaporn, P.; Sanguansermsri, T. Cord blood screening for α-thalassemia and hemoglobin variants by isoelectric focusing in northern Thai neonates: Correlation with genotypes and hematologic parameters. Blood Cells Mol. Dis. 2010, 45, 53–57. [Google Scholar] [CrossRef]
- Nillakupt, K.; Nathalang, O.; Arnutti, P.; Jindadamrongwech, S.; Boonsiri, T.; Panichkul, S.; Areekul, W. Prevalence and hematological parameters of thalassemia in the Kradarn subdistrict Chachoengsao province, Thailand. J. Med. Assoc. Thai. 2011, 95, S124–S132. [Google Scholar]
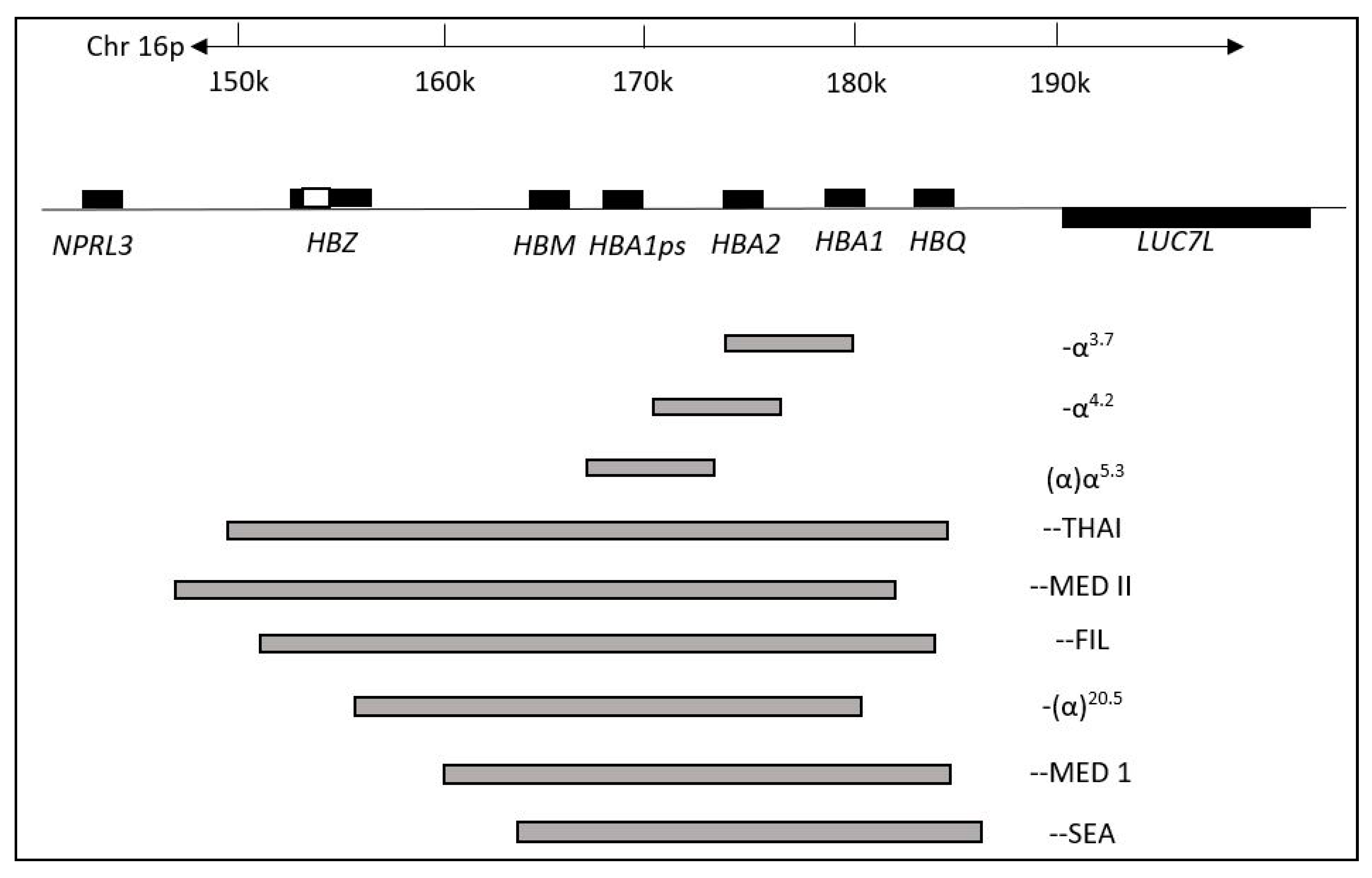
- Pongjantharasatien, K.; Banyatsuppasin, W.; Pounsawat, S.; Jindadamrongwech, S. Occurrence of the --SEA, --THAI, and --FIL α-thalassemia-1 carriers from a 7-year study at Ramathibodi hospital, Bangkok, Thailand. Hemoglobin 2016, 40, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Pichanun, D.; Munkongdee, T.; Klamchuen, S.; Butthep, P.; Winichagoon, P.; Fucharoen, S.; Svasti, S. Molecular screening of the Hbs constant spring (codon 142, TAA>CAA, α2) and paksé (codon 142, TAA>TAT, α2) mutations in Thailand. Hemoglobin 2010, 34, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Pharephan, S.; Sirivatanapa, P.; Makonkawkeyoon, S.; Tuntiwechapikul, W.; Makonkawkeyoon, L. Prevalence of α-thalassemia genotypes in pregnant women in northern Thailand. Indian J. Med. Res. 2016, 143, 315–322. [Google Scholar] [CrossRef]
- Panyasai, S.; Fucharoen, G.; Fucharoen, S. Hemoglobin variants in Northern Thailand: Prevalence, heterogeneity and molecular characteristics. Genet. Test Mol. Biomark. 2016, 20, 37–43. [Google Scholar] [CrossRef]
- Panomai, N.; Sanchaisuriya, K.; Yamsri, S.; Sanchaisuriya, P.; Fucharoen, S.; Schelp, F.P. Thalassemia and iron deficiency in a group of northeast Thai school children: Relationship to the occurrence of anaemia. Eur. J. Pediatr. 2010, 169, 1317–1322. [Google Scholar] [CrossRef]
- Prayalaw, P.; Fuchafoen, G.; Fucharoen, S. Routine screening for α-thalassemia using an immunochromatographic strip assay for haemoglobin Bart’s. J. Med. Screen. 2014, 21, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Seeratanachot, T.; Shimbhu, D.; Charoenkwan, P.; Sanguansermsri, T. Detection of deletion α+-thalassemia mutation [-α (3.7), -α (4.2)] by quantitative PCR assay. Southeast Asian J. Trop. Med. Public Health 2015, 46, 110–115. [Google Scholar]
- Wisedpanichkij, R.; Jindadamrongwech, S.; Butthep, P. Identification of Hb constant spring (HBA2: c.427T>C) by an automated high performance liquid chromatography method. Hemoglobin 2015, 39, 190–195. [Google Scholar] [CrossRef]
- Uaprasert, N.; Settapiboon, R.; Amomsiriwat, S.; Sarnthammakul, P.; Thanapat, T.; Rojnuckarin, P.; Sutcharitchan, P. Diagnostic utility of isoelectric focusing and high performance liquid chromatography in neonatal cord blood screening for thalassemia and non-sickling hemoglobinopathies. Clin. Chim. Acta. 2013, 427, 23–26. [Google Scholar] [CrossRef]
- Srivorakun, H.; Fucharoen, G.; Changtrakul, Y.; Komwilaisak, P.; Fucharoen, S. Thalassemia and hemoglobinopathies in South East Asia newborns: Diagnostic assessment using capillary electrophoresis system. Clin. Biochem. 2011, 44, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Chaibunruang, A.; Prommetta, S.; Yamsri, S.; Fucharoen, G.; Sae-Ung, N.; Sanchaisuriya, K.; Fucharoen, S. Molecular and hematological studies in a large cohort of α0-thalassemia in northeast Thailand: Data from a single referral centre. Blood Cells Mol. Dis. 2013, 51, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Thanyaornwanya, C.; Singha, K.; Fucharoen, G.; Sanchaisuriya, K.; Thepphitak, P.; Wintachai, P.; Karnpean, R.; Fucharoen, S. Molecular characteristics of α+-thalassemia (3.7 kb deletion) in Southeast Asia: Molecular subtypes, haplotypic heterogeneity, multiple founder effects and laboratory diagnosis. Clin. Biochem. 2019, 71, 31–37. [Google Scholar] [CrossRef]
- Mankhenthong, K.; Phusua, A.; Suantan, S.; Srisittipoj, P.; Charoenkwan, P.; Sanguansermsri, T. Molecular characteristics of thalassemia and haemoglobin variants in prenatal diagnosis program in northern Thailand. Int. J. Hematol. 2019, 110, 474–481. [Google Scholar] [CrossRef]
- Pata, S.; Laopajon, W.; Pongpaiboon, M.; Thongkum, W.; Polpong, N.; Munkongdee, T.; Paiboonsukwong, K.; Fucharoen, S.; Tayapiwatana, C.; Kasinrerk, W. Impact of the detection of ζ-globin chains and haemoglobin Bart’s using immunochromatographic strip test for α0-thalassemia (--SEA) differential diagnosis. PLoS ONE 2019, 14, e0223996. [Google Scholar] [CrossRef]
- Hoa Nguyen, V.; Sanchaisuriya, K.; Wongprachum, K.; Nguyen, M.D.; Phan, T.T.; Vo, V.T.; Sanchaisuriya, P.; Fucharoen, S.; Schelp, F.P. Hemoglobin constant spring is markedly high in women of an ethnic minority group in Vietnam: A community-based survey and hematologic features. Blood Cell Mol. Dis. 2014, 52, 161–165. [Google Scholar] [CrossRef]
- Modell, B.; Darlison, M. Global epidemiology in haemoglobin disorders and derived service indicators. Bull. World Health Organ. 2008, 86, 480–487. [Google Scholar] [CrossRef]
- Nadkarni, A.; Phanasgaonkar, S.; Colah, R.; Mohanty, D.; Ghosh, K. Prevalence and Molecular Characterization of α-Thalassemia Syndromes among Indians. Genet. Test. 2008, 12, 177–180. [Google Scholar] [CrossRef]
- Souza, A.E.S.; Cardoso, G.L.; Takanashi, S.Y.L.; Guerreiro, J.F. α-Thalassemia (3.7 kb deletion) in a population from the Brazilian Amazon region: Santarém, Pará State. Genet. Mol. Res. 2009, 8, 477–481. [Google Scholar] [CrossRef]
- AL-Awamy, B.H. Thalassemia syndromes in Saudi Arabia. Meta-analysis of local studies. Saudi Med. J. 2000, 21, 8–17. [Google Scholar]
- Kee, B.P.; Lian, L.H.; Lee, P.C.; Lai, T.X.; Chua, K.H. Genetic data for 15 STR loci in a Kadazan-Dusun population from East Malaysia. Genet. Mol. Res. 2011, 10, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Forget, B.G.; Bunn, H.F. Classification of the disorders of haemoglobin. Cold Spring Harb. Perspect. Med. 2013, 3, a011684. [Google Scholar] [CrossRef] [Green Version]
- Krause, M.A.; Diakite, S.A.S.; Lopera-Mesa, T.M.; Amaratunga, C.; Arie, T.; Traore, K.; Doumbia, S.; Konate, D.; Keefer, J.R.; Diakite, M.; et al. α-thalassemia impairs the cytoadherence of Plasmodium falciparum-infected erythrocytes. PLoS ONE 2012, e37214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gundula, M.-O.; Gros, P. Erthrocyte variants and the nature of their malaria protective effect. Cell. Microbiol. 2005, 7, 753–763. [Google Scholar] [CrossRef]
- World Health Organization. World Malaria Report 2019; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author [Reference] | α-Thalassemia Genotyping Method | Genotypes Found in the Study | Country | Specific Ethnic 1 | Events 2 | Total 3 |
|---|---|---|---|---|---|---|
| Munkongdee et al., 2016 [25] | Polymerase chain reaction (PCR) | -α3.7, -α4.2, --SEA, αCS, αPs | Cambodia | N/A | 646 | 1631 |
| Jomoui et al., 2017 [26] | PCR | --SEA | Cambodia | N/A | 7 | 21 |
| Wongprachum et al., 2012 [27] | PCR | -α3.7, -α4.2, --SEA, --THAI, αCS, αPs, αQ-Thailand | Laos | N/A | 130 | 411 |
| Jomoui et al., 2017 [26] | PCR | --SEA | Laos | N/A | 28 | 52 |
| Tritipsombut et al., 2012 [28] | PCR | -α3.7, -α4.2, --SEA, αCS, αPs | Laos | N/A | 30 | 349 |
| Azma et al., 2012 [29] | PCR | Malaysia | N/A | 14 | 400 | |
| Azma et al., 2014 [4] | PCR | -α3.7, -α4.2, --SEA, αCS, αCD59, αIVS I-1 | Malaysia | Malay, Chinese, Indian, Other | 736 | 1623 |
| Jameela et al., 2011 [30] | PCR | -α3.7, -α4.2, --SEA, --FIL, α125 | Malaysia | Malay, Chinese, Indian, Sikh, Iban | 10 | 310 |
| Mohd Yatim et al., 2014 [31] | PCR | -α3.7, --SEA, αCS, αCD59, | Malaysia | Malay | 28 | 68 |
| Tan et al., 2010 [3] | PCR | -α3.7, -α4.2, --SEA, --THAI, --FIL, αCS, α125, | Malaysia | Kadazandusun | 42 | 125 |
| Charoenkwan et al., 2010 [32] | PCR | -α3.7, -α4.2, --SEA, -αQ-Thailand, αCS | Thailand | N/A | 142 | 566 |
| Lithanatudom et al., 2016 [17] | PCR | -α3.7, -α4.2, --SEA, --THAI, αCS, αPs | Thailand | Yong, Yuan, Lue, Khuen, Blang, Mon, Paluang, Lawa | 33 | 141 |
| Nillakupt et al., 2012 [33] | PCR | -α3.7, --SEA, αCS, αPs | Thailand | N/A | 47 | 266 |
| Pongjantharasatien et al., 2016 [34] | PCR | --SEA, --THAI, --FIL, -αthal-1 | Thailand | N/A | 4555 | 31,632 |
| Pichanun et al., 2010 [35] | PCR | -α3.7, αCS, αPs | Thailand | N/A | 36 | 587 |
| Pharephan et al., 2016 [36] | PCR | -α3.7, -α4.2, --SEA, αCS | Thailand | N/A | 229 | 638 |
| Panyasai et al., 2016 [37] | PCR | -α3.7, -αQT, --SEA, | Thailand | N/A | 51 | 23,914 |
| Panomai et al., 2010 [38] | PCR | -α3.7, -α4.2, --SEA, --THAI, αCS, αPs | Thailand | N/A | 40 | 190 |
| Prayalaw et al., 2014 [39] | PCR | -α3.7, -α4.2, --SEA, αCS, -αQ-Thailand | Thailand | N/A | 75 | 300 |
| Seeratanachot et al., 2015 [40] | Realtime-PCR | -α3.7, -α4.2, --SEA | Thailand | N/A | 62 | 250 |
| Wisedpanichkij et al., 2015 [41] | PCR | -α3.7, -α4.2, --SEA, αCS | Thailand | N/A | 409 | 578 |
| Uaprasert et al., 2013 [42] | PCR | -α3.7, -α4.2, αCS | Thailand | N/A | 67 | 241 |
| Srivorakun et al., 2011 [43] | PCR | -α3.7, --SEA, αCS | Thailand | N/A | 44 | 226 |
| Tritipsombut et al., 2012 [28] | PCR | -α3.7, -α4.2, --SEA, αCS, αPs | Thailand | N/A | 85 | 1460 |
| Chaibunruang et al., 2013 [44] | PCR | --SEA, --THAI | Thailand | N/A | 1874 | 12,525 |
| Kulaphisit et al., 2017 [5] | PCR | -α3.7, -α4.2, --SEA, --THAI, αCS, αPs | Thailand | Yong, Lue, Yuan, Shan, Khuen, Htin, Paluang, Blang, Lawa, Mon, Skaw Karen, Pwo Karen, Padong Karen | 124 | 668 |
| Thanyaornwanya et al., 2019 [45] | PCR | -α3.7, -α4.2, αCS, αPs | Thailand | N/A | 676 | 1192 |
| Jomoui et al., 2017 [26] | PCR | --SEA | Thailand | N/A | 66 | 96 |
| Mankhenthong et al., 2019 [46] | PCR | -α3.7, -α4.2, --SEA, --THAI, αCS | Thailand | N/A | 118 | 1290 |
| Pata et al., 2019 [47] | PCR | -α3.7, -α4.2, --SEA, --THAI, αCS | Thailand | N/A | 82 | 195 |
| O’Riordan et al., 2010 [18] | PCR | -α3.7, -α4.2, --SEA, --THAI, --FIL, αCS | Vietnam | Kinh, Dao, Tay, Nung, S’Tieng, M’Nong, Rac Iay, E De | 996 | 1431 |
| Hoa Nguyen et al., 2014 [48] | PCR | -α3.7, -α4.2, --SEA, --THAI, --SEA, αCS, αPs | Vietnam | Cό-Tu | 98 | 298 |
| Total | 11,580 | 83,674 | ||||
| Heterogeneity | Prevalence Rate (95% CI) | Sample Size (N) | No. of Studies (N) | Subgroups | |
|---|---|---|---|---|---|
| I2 (%) | p-Value | ||||
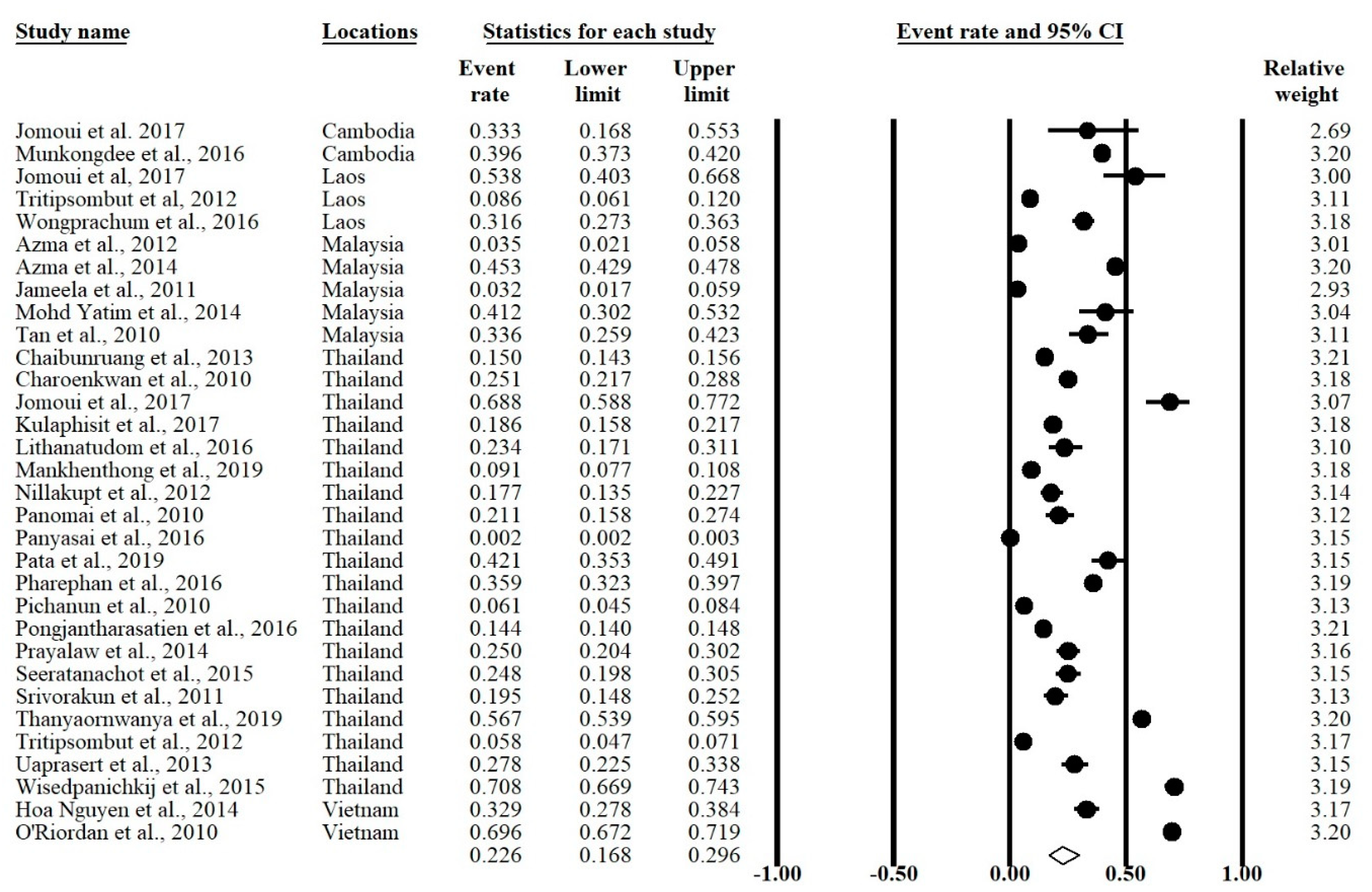
| 99.53 | <0.001 | 0.226 (0.168–0.296) | 83,674 | 32 | Overall |
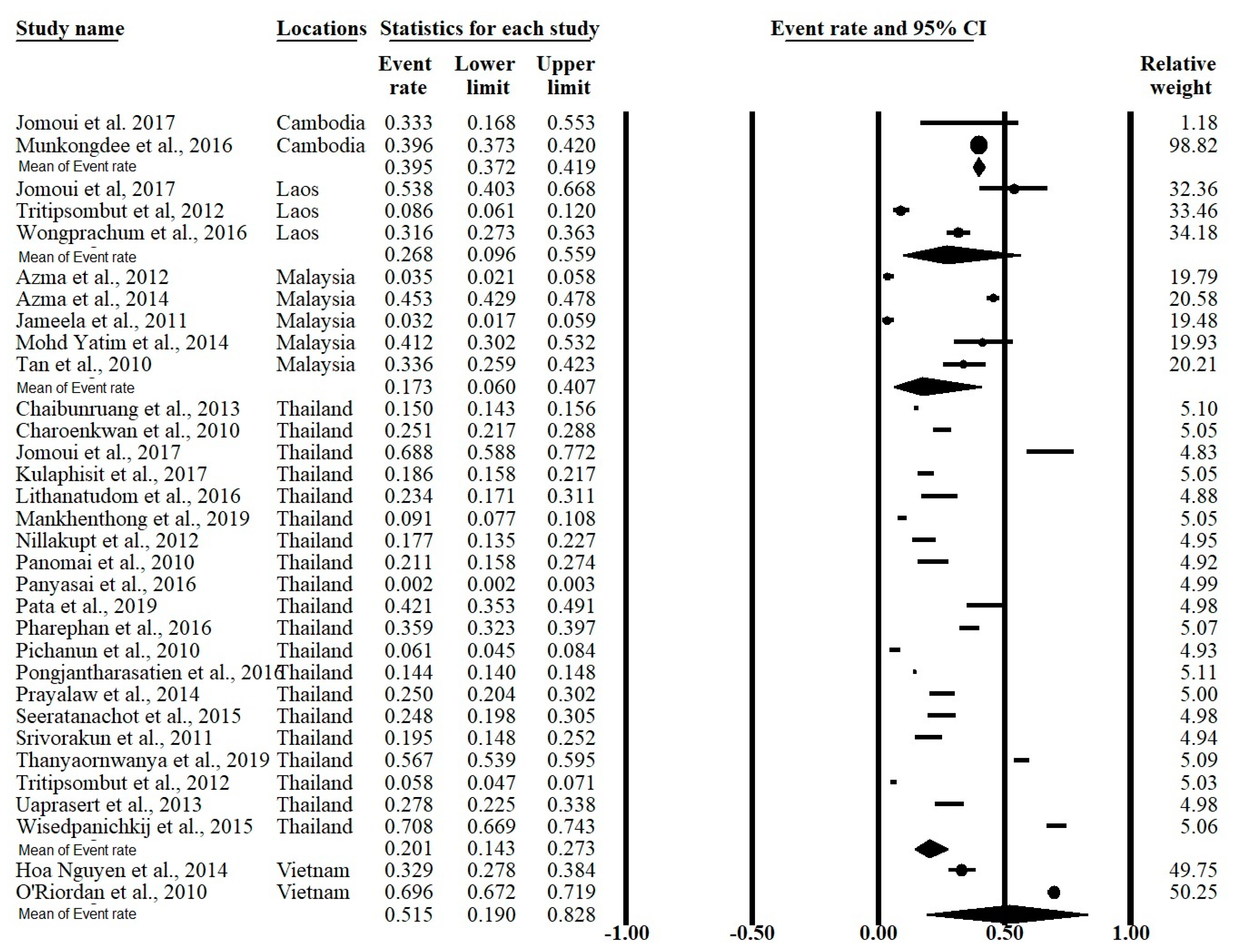
| 0 | 0.560 | 0.395 (0.372–0.419) | 1652 | 2 | Cambodia |
| 97.26 | <0.001 | 0.268 (0.096–0.559) | 812 | 3 | Laos |
| 98.20 | <0.001 | 0.173 (0.060–0.407) | 2526 | 5 | Malaysia |
| 99.47 | <0.001 | 0.201 (0.143–0.273) | 76,955 | 20 | Thailand |
| 99.22 | <0.001 | 0.515 (0.190–0.828) | 1729 | 2 | Vietnam |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goh, L.P.W.; Chong, E.T.J.; Lee, P.-C. Prevalence of Alpha(α)-Thalassemia in Southeast Asia (2010–2020): A Meta-Analysis Involving 83,674 Subjects. Int. J. Environ. Res. Public Health 2020, 17, 7354. https://doi.org/10.3390/ijerph17207354
Goh LPW, Chong ETJ, Lee P-C. Prevalence of Alpha(α)-Thalassemia in Southeast Asia (2010–2020): A Meta-Analysis Involving 83,674 Subjects. International Journal of Environmental Research and Public Health. 2020; 17(20):7354. https://doi.org/10.3390/ijerph17207354
Chicago/Turabian StyleGoh, Lucky Poh Wah, Eric Tzyy Jiann Chong, and Ping-Chin Lee. 2020. "Prevalence of Alpha(α)-Thalassemia in Southeast Asia (2010–2020): A Meta-Analysis Involving 83,674 Subjects" International Journal of Environmental Research and Public Health 17, no. 20: 7354. https://doi.org/10.3390/ijerph17207354
APA StyleGoh, L. P. W., Chong, E. T. J., & Lee, P. -C. (2020). Prevalence of Alpha(α)-Thalassemia in Southeast Asia (2010–2020): A Meta-Analysis Involving 83,674 Subjects. International Journal of Environmental Research and Public Health, 17(20), 7354. https://doi.org/10.3390/ijerph17207354