Physical Activity as Part of an Intramural Health Promotion Programme for People with and without Chronic Diseases. A New Tool in Health Care Run by a Public Social Health Insurance

 ,
, 
Abstract
:1. Introduction
1.1. Physical Activity
1.2. Physical Training, Health, and Chronic Diseases
1.3. Social Insurance System in Austria
2. A New Intramural Facility for Health Promotion by a Public Social Insurance
- Promoting physical training
- Optimizing nutritional patterns
- Managing everyday stress
- Increasing social capital
- Improving health literacy
2.1. Target Groups and Basic Concept for the Health Promotion Programme
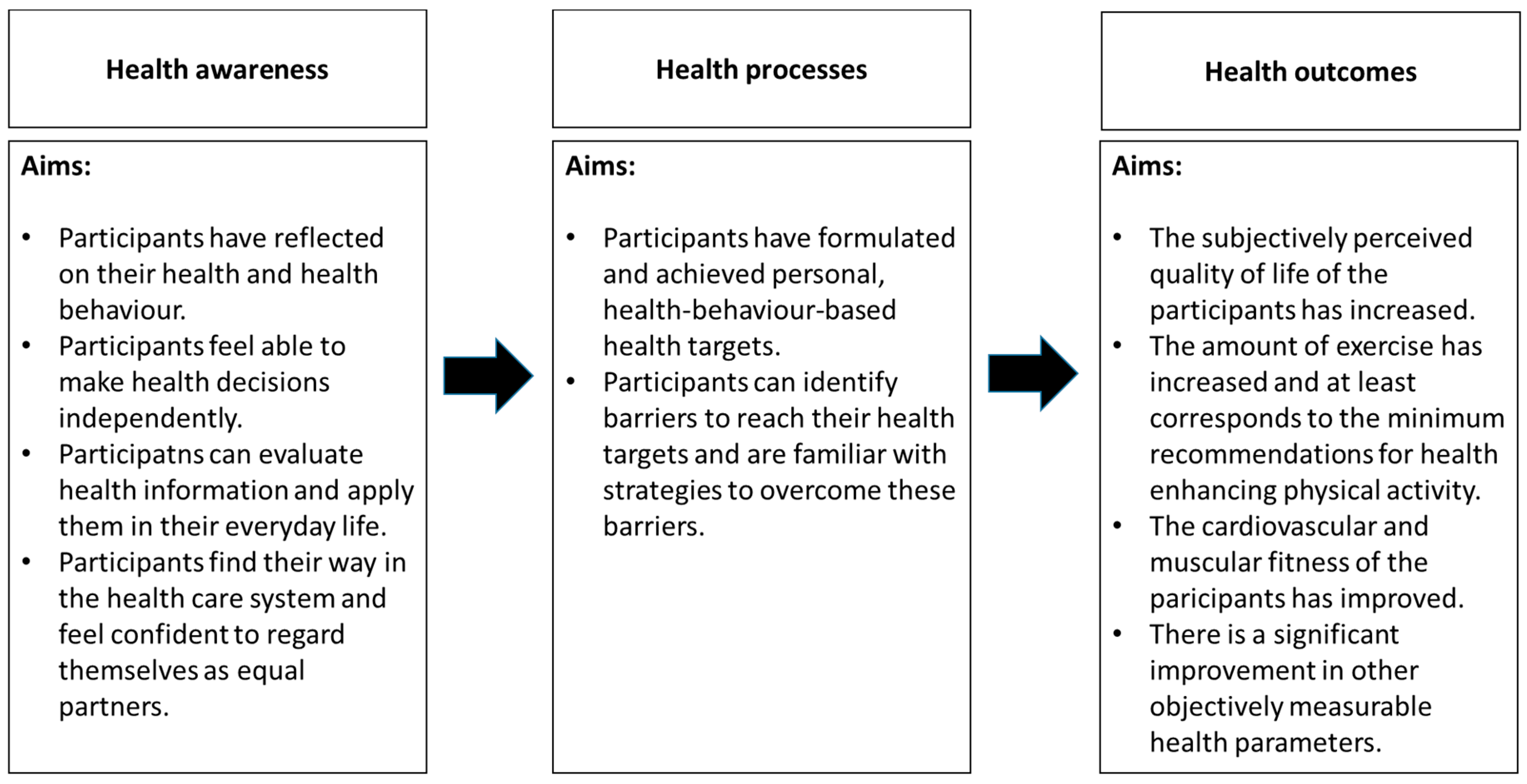
2.2. General Aims and Different Modules in the Intramural Programme
2.3. Diagnostic Tools
2.3.1. Physical Fitness
2.3.2. Physical Activity Behaviour
2.3.3. Other Diagnostic Tools
2.4. Health Promotion Interventions
- “Welcome, introduction, concept” (60 min)
- “Physical exercise and health and basics of training principles” (90 min)
- “Basics of a healthy diet” (90 min)
- “Social capital and health” (90 min)
- “What is health literacy?” (90 min)
- “Dealing with everyday requirements—stress management” (90 min)
- “Methods of resilience—How can I strengthen resilience?” (90 min)
- 8 h of physical training (fitness area, gym, swimming pool, aqua gym, outdoor facilities)
- 6 h teaching kitchen (2 units of three hours each)
- 2 h nutrition seminar
- 5 h of psychology (behaviour change, conversation therapy, time management, stress coping, relaxation techniques, mindfulness exercises, biofeedback) divided into two units of 60 min and two units of 90 min.
- 3 h seminar on social capital (2 units of 90 min each)
- 90 min seminar on health literacy
- 1 h of massage
2.5. Novelty of This Intramural Health Care Facility within the Health Care System
2.6. Considerations Regarding Cost-Effektiveness
3. Outlook and Conclusions
3.1. Further Development
3.2. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Titze, S.; Lackinger, C.; Fessl, C.; Dorner, T.E.; Zeuschner, V. Österreichische Bewegungsempfehlungen für Erwachsene und ältere Erwachsene ohne und mit Körper-, Sinnes-oder Mentalbehinderung sowie für Menschen mit chronischen Erkrankungen. Gesundheitswesen 2020, 82, S170–S176. [Google Scholar] [PubMed]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; HHS: Washington, DC, USA, 2018. [Google Scholar]
- Dorner, T.E.; Haider, S.; Lackinger, C.; Kapan, A.; Titze, S. Bewegungsdeterminanten, Erfüllung der Empfehlungen für ausdauerorientierte Bewegung und Gesundheit: Ergebnisse einer Korrelationsstudie aus den österreichischen Bundesländern. Gesundheitswesen 2020, 82, S207–S216. [Google Scholar] [CrossRef] [PubMed]
- Crevenna, R.; Dorner, T.E. Association between fulfilling the recommendations for health-enhancing physical activity with (instrumental) activities of daily living in older Austrians. Wien. Klin. Wochenschr. 2019, 131, 265–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lackinger, C.; Haider, S.; Kosi, L.; Harreiter, J.; Winhofer, Y.; Kautzky-Willer, A. Potential of a sports club-based exercise program for improving physical activity in type 2 diabetes mellitus. J. Phys. Act. Health 2015, 12, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Lackinger, C.; Strehn, A.; Dorner, T.E.; Niebauer, J.; Titze, S. Health resorts as gateways for regional, standardised, sports club based exercise programmes to increase the weekly time of moderate- to vigorous-intensity physical activity: Study protocol. BMC Public Health 2015, 15, 1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachner, F.; Bobek, J.; Habimana, K.; Ladurner, J.; Lepuschutz, L.; Ostermann, H.; Rainer, L.; Schmidt, A.E.; Zuba, M.; Quentin, W.; et al. Austria: Health system review. Health Syst. Trans. 2018, 20, 1–254. [Google Scholar]
- BVAEB. Kur & Rehabilitation. Eigene Einrichtungen und Vertragseinrichtungen; Versicherungsanstalt öffentlich Bediensteter, Eisenbahnen und Bergbau: Vienna, Austria, 2020. [Google Scholar]
- Blasche, G.; Leibetseder, V.; Marktl, W. Association of spa therapy with improvement of psychological symptoms of occupational burnout: A pilot study. Forsch. Komplementmed. 2010, 17, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Strauss-Blasche, G.; Ekmekcioglu, C.; Vacariu, G.; Melchart, H.; Fialka-Moser, V.; Marktl, W. Contribution of individual spa therapies in the treatment of chronic pain. Clin. J. Pain 2002, 18, 302–309. [Google Scholar] [CrossRef]
- Ekmekcioglu, C.; Strauss-Blasche, G.; Feyertag, J.; Klammer, N.; Marktl, W. The effect of balneotherapy on ambulatory blood pressure. Altern. Ther. Health Med. 2000, 6, 46–53. [Google Scholar]
- Pensionsversicherungsanstalt. Jahresbericht 2019; PVA: Vienna, Austria, 2019. [Google Scholar]
- Allgemeine Unfallversicherungsanstalt. Jahresbericht 2018; AUVA: Vienna, Austria, 2019. [Google Scholar]
- Sozialversicherung der Selbständigen. Gesundheitseinrichtungen. Available online: https://www.svs.at/cdscontent/?contentid=10007.828375&portal=svsportal (accessed on 6 October 2020).
- Österreichische Gesundheitskasse. Standorte. Available online: https://www.gesundheitskasse.at/cdscontent/?contentid=10007.851829&portal=oegkportal (accessed on 6 October 2020).
- Versicherungsanstalt öffentlich Bediensteter. Jahresbericht 2018; BVA: Vienna, Austria, 2018. [Google Scholar]
- Versicherungsanstalt für Eisenbahnen & Bergbau. Jahresbericht 2018; VAEB: Vienna, Austria, 2018. [Google Scholar]
- Cešeiko, R.; Thomsen, S.N.; Tomsone, S.; Eglītis, J.; Vētra, A.; Srebnijs, A.; Timofejevs, M.; Purmalis, E.; Wang, E. Heavy resistance training in breast cancer patients undergoing adjuvant therapy. Med. Sci. Sports Exerc. 2020, 52, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- García-Ramos, A.; Haff, G.G.; Pestaña-Melero, F.L.; Pérez-Castilla, A.; Rojas, F.J.; Balsalobre-Fernández, C.; Jaric, S. Feasibility of the 2-point method for determining the 1-repetition maximum in the bench press exercise. Int. J. Sports Physiol. Perform. 2018, 13, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Uhlemann, M.; Möbius-Winkler, S.; Fikenzer, S.; Adam, J.; Redlich, M.; Möhlenkamp, S.; Hilberg, T.; Schuler, G.C.; Adams, V. Circulating microRNA-126 increases after different forms of endurance exercise in healthy adults. Eur. J. Prev. Cardiol. 2014, 21, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Thiele, D.; Prieske, O.; Chaabene, H.; Granacher, U. Effects of strength training on physical fitness and sport-specific performance in recreational, sub-elite, and elite rowers: A systematic review with meta-analysis. J. Sports Sci. 2020, 38, 1186–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcos-Pardo, P.J.; González-Hernández, J.M.; García-Ramos, A.; López-Vivancos, A.; Jiménez-Reyes, P. Movement velocity can be used to estimate the relative load during the bench press and leg press exercises in older women. PeerJ 2019, 20, e7533. [Google Scholar] [CrossRef] [Green Version]
- Aadahl, M.; Beyer, N.; Linneberg, A.; Thuesen, B.H.; Jørgensen, T. Grip strength and lower limb extension power in 19–72-year-old Danish men and women: The Health2006 study. BMJ Open 2011, 1, 2011-000192. [Google Scholar] [CrossRef] [Green Version]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand grip strength: Age and gender stratified normative data in a population-based study. BMC Res. Notes 2011, 4, 127. [Google Scholar] [CrossRef] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Wonisch, M.; Berent, R.; Klicpera, M.; Laimer, H.; Marko, C.; Pokan, R.; Schmid, P.; Schwann, H. Praxisleitlinien Ergometrie. Austrian J. Cardiol. 2008, 15, 3–17. [Google Scholar]
- Gibbons, R.J.; Balady, G.J.; Bricker, J.T.; Chaitman, B.R.; Fletcher, G.F.; Froelicher, V.F.; Mark, D.B.; McCallister, B.D.; Mooss, A.N.; O’Reilly, M.G.; et al. ACC/AHA 2002 guideline update for exercise testing: Summary article: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation 2002, 106, 1883–1892. [Google Scholar] [PubMed]
- Bruce, R.A.; DeRouen, T.A.; Hossack, K.F. Value of maximal exercise tests in risk assessment of primary coronary heart disease events in healthy men. Five years’ experience of the Seattle heart watch study. Am. J. Cardiol. 1980, 46, 371–378. [Google Scholar] [CrossRef]
- Finger, J.D.; Tafforeau, J.; Gisle, L.; Oja, L.; Ziese, T.; Thelen, J.; Mensink, G.B.; Lange, C. Development of the European Health Interview Survey—Physical Activity Questionnaire (EHIS-PAQ) to monitor physical activity in the European Union. Arch. Public Health 2015, 73, 59. [Google Scholar] [CrossRef] [Green Version]
- Fazio, S.; Stocking, J.; Kuhn, B.; Doroy, A.; Blackmon, E.; Young, H.M.; Adams, J.Y. How much do hospitalized adults move? A systematic review and meta-analysis. Appl. Nurs. Res. 2020, 51, 151189. [Google Scholar] [CrossRef] [PubMed]
- Levenstein, S.; Prantera, C.; Varvo, V.; Scribano, M.L.; Berto, E.; Luzi, C.; Andreoli, A. Development of the Perceived Stress Questionnaire: A new tool for psychosomatic research. J. Psychosom. Res. 1993, 37, 19–32. [Google Scholar] [CrossRef]
- Rutz, W. Rethinking mental health: A European WHO perspective. World Psychiatry 2003, 2, 125–127. [Google Scholar]
- WHO (World Health Organization). WHOQOL-BREF Introduction, Administration, Scoring and Generic Version of the Assessment; WHO: Geneva, Switzerland, 1996. [Google Scholar]
- Park, Y.; Dodd, K.W.; Kipnis, V.; Thompson, F.E.; Potischman, N.; Schoeller, D.A.; Baer, D.J.; Midthune, D.; Troiano, R.P.; Bowles, H.; et al. Comparison of self-reported dietary intakes from the Automated Self-Administered 24-h recall, 4-d food records, and food-frequency questionnaires against recovery biomarkers. Am. J. Clin. Nutr. 2018, 107, 80–93. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, A. Effects of social capital on general health status. Glob. J. Health Sci. 2014, 6, 45–54. [Google Scholar] [CrossRef] [Green Version]
- OECD (Organisation for Economic Co-operation and Development). The OECD Social Capital Questionnaire Databank. Available online: http://www.oecd.org/sdd/social-capital-project-and-question-databank.htm (accessed on 10 September 2020).
- Finbråten, H.S.; Wilde-Larsson, B.; Nordström, G.; Pettersen, K.S.; Trollvik, A.; Guttersrud, Ø. Establishing the HLS-Q12 short version of the European Health Literacy Survey Questionnaire: Latent trait analyses applying Rasch modelling and confirmatory factor analysis. BMC Health Serv. Res. 2018, 18, 506. [Google Scholar] [CrossRef]
- Huber, C.A.; Reich, O.; Früh, M.; Rosemann, T. Effects of integrated care on disease-related hospitalisation and healthcare costs in patients with diabetes, cardiovascular diseases and respiratory illnesses: A propensity-matched cohort study in Switzerland. Int. J. Integr. Care 2016, 16, 11. [Google Scholar] [PubMed] [Green Version]
- Martínez-González, N.A.; Berchtold, P.; Ullman, K.; Busato, A.; Egger, M. Integrated care programmes for adults with chronic conditions: A meta-review. Int. J. Qual. Health Care 2014, 26, 561–570. [Google Scholar] [CrossRef]
- WHO (World Health Organization). WHO Global Strategy on People-Centred and Integrated Health Services: Interim Report; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Sweeney, D.; Rule, J. Sport and community engagement in ageing health: Tackling isolation and scoring better outcomes. NHS Halton CCG and Widnes Vikings. Int. J. Integr. Care 2017, 17, A447. [Google Scholar] [CrossRef]
- Dolan, B.; Gullery, C.; Hamilton, G.; Meates, D. What is integrated care. In Handbook Integrated Care; Amelung, V.E., Stein, K.V., Goodwin, N., Balicer, R., Nolte, E., Suter, E., Eds.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Collins, B. International Whole Health System Redesign. Southcentral Foundation’s ‘Nuka’ System of Care; The King’s Fund: London, UK, 2015. [Google Scholar]
- Groene, O.; Hildebrandt, H. Germany: Evolution and scaling up of the population-based integrated health care system “Healthy Kinzigtal”. In Handbook Integrated Care; Amelung, V.E., Stein, K.V., Goodwin, N., Balicer, R., Nolte, E., Suter, E., Eds.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Nolte, E.; Conklin, A.; Adams, J.L.; Brunn, M.; Cadier, B.; Chevreul, K.; Durand-Zaleski, I.; Elissen, A.; Erler, A.; Flamm, M.; et al. Evaluating Chronic Disease Management. Recommendations for Funders and Users; Rand Corporation: Santa Monica, CA, USA, 2012. [Google Scholar]
- Goodwin, N. Understanding and evaluating the implementation of integrated care: A ‘Three Pipe’ problem. Int. J. Integr. Care 2016, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Roux, L.; Pratt, M.; Tengs, T.O.; Yore, M.M.; Yanagawa, T.L.; Van Den Bos, J.; Rutt, C.; Brownson, R.C.; Powell, K.E.; Heath, G.; et al. Cost effectiveness of community-based physical activity interventions. Am. J. Prev. Med. 2008, 35, 578–588. [Google Scholar] [CrossRef]
- Alt, R.; Binder, A.; Helmenstein, C.; Kleissner, A.; Krabb, P. Der volkswirtschaftliche Nutzen von Bewegung. Volkswirtschaftlicher Nutzen von Bewegung, volkswirtschaftliche Kosten von Inaktivität und Potenziale von mehr Bewegung. Studie im Auftrag der Österreichischen Bundes-Sportorganisation (BSO) und FitSportAustria; SportsEconAustria: Vienna, Austria, 2015. [Google Scholar]
- Hauptverband der österr. Sozialversicherungsträger. Statistisches Handbuch der österreichischen Sozialversicherung 2019; Hauptverband der österr. Sozialversicherungsträger: Vienna, Austria, 2019. [Google Scholar]
- Woolley, A.K.; Hadjiconstantinou, M.; Davies, M.; Khunti, K.; Seidu, S. Online patient education interventions in type 2 diabetes or cardiovascular disease: A systematic review of systematic reviews. Prim. Care Diabetes 2019, 13, 16–27. [Google Scholar] [CrossRef]
- Lipari, M.; Berlie, H.; Saleh, Y.; Hang, P.; Moser, L. Understandability, actionability, and readability of online patient education materials about diabetes mellitus. Am. J. Health Syst. Pharm. 2019, 76, 182–186. [Google Scholar] [CrossRef]
- Powell, H.S.; Greenberg, D.L. Screening for unhealthy diet and exercise habits: The electronic health record and a healthier population. Prev. Med. Rep. 2019, 14, 100816. [Google Scholar] [CrossRef]
- AuYoung, M.; Linke, S.E.; Pagoto, S.; Buman, M.P.; Craft, L.L.; Richardson, C.R.; Hutber, A.; Marcus, B.H.; Estabrooks, P.; Sheinfeld Gorin, S. Integrating physical activity in primary care practice. Am. J. Med. 2016, 129, 1022–1029. [Google Scholar] [CrossRef] [Green Version]
- Dorner, T.E.; Wilfinger, J.; Hoffman, K.; Lackinger, C. Association between physical activity and the utilization of general practitioners in different age groups. Wien. Klin. Wochenschr. 2019, 131, 278–287. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Types of Intramural Facilities (Horizontal)Characteristics (Vertical) | Rehabilitation | Traditional in-Patient Spa Therapy | New Intramural Health Promotion Facility |
|---|---|---|---|
| Financial coverage | Public social insurance | Public social insurance | Public social insurance |
| Duration | 3–6 weeks | 3 weeks | 3 weeks, split in 2 + 1 week |
| Focus | Indication-centred | Indication-centred | Person-centred |
| Time in the course of disease | After acute disease treatment | After acute disease treatment | Independent from existence of diseases |
| Health model | Bio-psycho-social (with emphasis on medical health) | Bio-psycho-social (with emphasis on medical health) | Bio-psycho-social (all dimensions equal) |
| Aims | Return-to-work; occupational and social rehabilitation; prevention of early exit from the labour market; prevention of reoccurrence or exacerbation of the disease | Prevention of reoccurrence or exacerbation of the disease; maintenance of ability to work | Gain in health in all dimensions; higher quality of life; improvement of ability to work |
| Orientation of measures | Active and passive | Mainly passive | Mainly active |
| Extent of measures | Variable | 1400 min | 2700 min |
| Screening before the stay | No | No | Yes |
| Diagnostics | Sufficient in connection with the disease | Basic | Comprehensive |
| Orientation on individual health goals | Partly | No | Yes |
| Area | Measurement | Time of Measurement | ||
|---|---|---|---|---|
| Before the Initial Stay | Initial Stay | Follow Up Week | ||
| General medical and physical examination | Medical history | √ | ||
| Medical anamnesis | √ | √ | ||
| Lifestyle anamnesis | √ | √ | ||
| Anthropometric parameters | √ | √ | ||
| Bioimpedance analysis | √ | √ | ||
| Resting ECG | √ | √ | ||
| Laboratory parameters | √ | √ | ||
| Sleep quality | √ | √ | ||
| Physical activity | Physical activity behaviour | √ | ||
| Activity tracking | √ | √ | ||
| Physical fitness | Maximum muscle strength (1-RPM) | √ | √ | |
| Exercise stress test | √ | √ | ||
| Submaximal muscle strength (70% of 1-RPM) | √ | √ | ||
| Handgrip strength | √ | √ | ||
| Strength endurance | √ | √ | ||
| Additional diagnostic tools for: | Nutrition | √ | √ | |
| Perceived stress | √ | √ | ||
| Social capital | √ | √ | ||
| Health literacy | √ | √ | ||
| Sleep quality | √ | √ | ||
| Health resources | √ | √ | ||
| Quality of life | √ | √ | ||
| Adherence | Adherence to tailored health goals | √ | ||
| Module | Content | Duration (h) |
|---|---|---|
| Basic modules | Welcome | 1 |
| Physical exercise | 1.5 | |
| Healthy diet | 1.5 | |
| Social capital | 1.5 | |
| Health literacy | 1.5 | |
| Stress management | 1.5 | |
| Resilience | 1.5 | |
| →Total duration basic module | 10 | |
| Core modules | Physical training | 8 |
| Teaching kitchen | 6 | |
| Nutrition seminar | 2 | |
| Psychological support | 5 | |
| Social capital | 3 | |
| Health literacy | 1.5 | |
| Massage | 1 | |
| →Total duration core module | 26.5 | |
| Elective modules | Creative workshop | 3 |
| Individually agreed | 6 | |
| →Total duration elective modules | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dorner, T.E.; Wolner-Strohmeyer, G.; Katzenbeisser, C.; Lackinger, C.; Stein, K.V. Physical Activity as Part of an Intramural Health Promotion Programme for People with and without Chronic Diseases. A New Tool in Health Care Run by a Public Social Health Insurance. Int. J. Environ. Res. Public Health 2020, 17, 7491. https://doi.org/10.3390/ijerph17207491
Dorner TE, Wolner-Strohmeyer G, Katzenbeisser C, Lackinger C, Stein KV. Physical Activity as Part of an Intramural Health Promotion Programme for People with and without Chronic Diseases. A New Tool in Health Care Run by a Public Social Health Insurance. International Journal of Environmental Research and Public Health. 2020; 17(20):7491. https://doi.org/10.3390/ijerph17207491
Chicago/Turabian StyleDorner, Thomas E., Gudrun Wolner-Strohmeyer, Christian Katzenbeisser, Christian Lackinger, and K. Viktoria Stein. 2020. "Physical Activity as Part of an Intramural Health Promotion Programme for People with and without Chronic Diseases. A New Tool in Health Care Run by a Public Social Health Insurance" International Journal of Environmental Research and Public Health 17, no. 20: 7491. https://doi.org/10.3390/ijerph17207491
APA StyleDorner, T. E., Wolner-Strohmeyer, G., Katzenbeisser, C., Lackinger, C., & Stein, K. V. (2020). Physical Activity as Part of an Intramural Health Promotion Programme for People with and without Chronic Diseases. A New Tool in Health Care Run by a Public Social Health Insurance. International Journal of Environmental Research and Public Health, 17(20), 7491. https://doi.org/10.3390/ijerph17207491