The Elaboration of an Intersectoral Partnership to Perform Health Impact Assessment in Urban Planning: The Experience of Quebec City (Canada)


Abstract
:1. Introduction
1.1. Historical Background: The Emergence of Health Impact Assessment
1.2. What Is an Health Impact Assessment (HIA)?
1.3. HIA in Canada
1.4. HIA in the Province of Quebec
1.5. HIA in Urban Planning
1.6. Objectives
2. Methods Undertaken to Create the Partnership
3. Results: The Partnership
3.1. Institutional Arrangements and Challenges for the Implementation of HIA
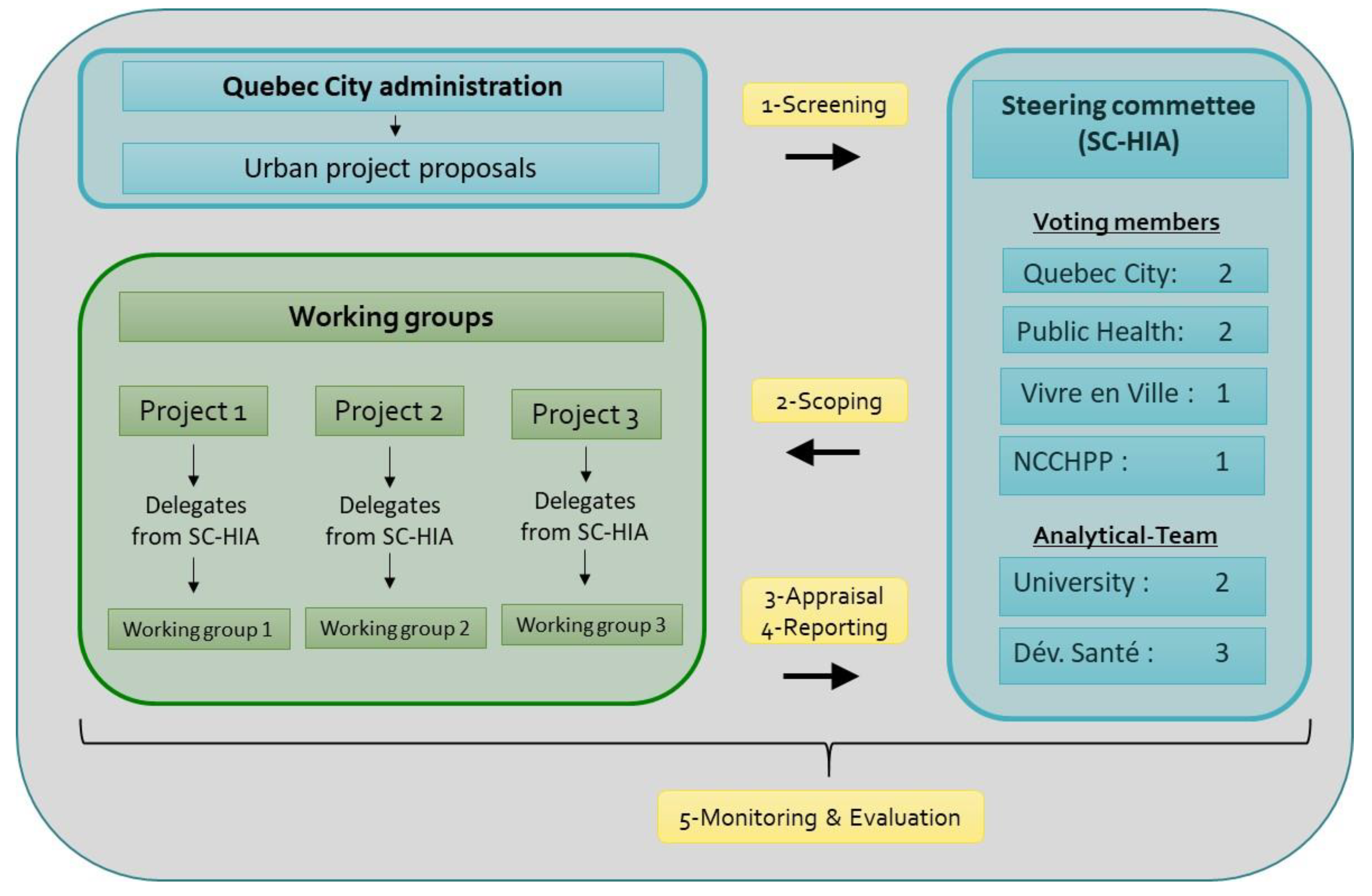
3.2. The Approach Developed to Integrate HIA into Urban Planning in Quebec City
Data Collection and Appraisal
3.3. Emerging Characteristics Perceived by Participants in the HIA Process
4. Discussion
- Promote the conduct of the HIA process in conjunction with an environmental assessment (EA) when the latter is required for the proposal under review. This will allow HIA to benefit from the experience of EA in urban planning processes and will provide an opportunity to exchange data necessary for carrying out both impact assessments.
- Formulate, wherever possible, recommendations from the HIA directly on the proposed draft urban plan.
- Develop a plan or a strategy to follow up on the effectiveness of recommendations made during the HIA process. This helps to develop the planners’ understanding of the actions proposed to improve their project in terms of health and to facilitate the consideration of these actions.
- Having a neutral/independent actor with some credibility, such as a university, to coordinate the HIA process may help facilitate intersectoral work and seems to facilitate the acceptance of HIA results by all the actors involved. With a neutral actor, there are no conflicts of interest.
- For the actors in charge of conducting HIAs in urban planning, make sure that everyone knows how to work on urban plans and maps to facilitate interactions with planners.
- Have some flexibility in integrating local community’s concerns into the HIA when the time to complete the impact assessment is very short (for example, three months). This could be considered as a rapid HIA. In this type of HIA, it is often difficult to keep some time open to enable the population affected by the proposal under review to participate in the HIA process. One solution would be to include in the HIA working group a person with an expertise of the local communities’ needs and territory. Another way would be to use the results of public consultations organized by the city on the project under review, when these are available.
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Frank, A.G. The wealth and poverty of nations: Even heretics remain bound by traditional thought. Econ. Political Wkly. 1970, 5, 1177–1184. [Google Scholar]
- Grant, M.; Brown, C.; Caiaffa, W.T.; Capon, A.; Corburn, J.; Coutts, C.; Crespo, C.J.; Ellis, G.; Ferguson, G.; Fudge, C.; et al. Cities and Health: An Evolving Global Conversation; Taylor & Francis: Abingdon, UK, 2017. [Google Scholar]
- Hancock, T. Equity, sustainability and governance: Key challenges facing 21st century cities (Part. 1). In Cities & Health; Taylor & Francis: Oxfordshire, UK, 2017; Volume 1, pp. 95–99. [Google Scholar]
- Vlahov, D.; Freudenberg, N.; Proietti, F.; Ompad, D.; Quinn, A.; Nandi, V.; Galea, S. Urban as a determinant of health. J. Urban Health 2007, 84, 16–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; A Bhutta, Z.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional and national life expectancy, all-cause mortality and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Cerin, E.; Conway, T.L.; A Adams, M.; Frank, L.D.; Pratt, M.; Salvo, D.; Schipperijn, J.; Smith, G.; Cain, K.L.; et al. Physical activity in relation to urban environments in 14 cities worldwide: A cross-sectional study. Lancet 2016, 387, 2207–2217. [Google Scholar] [CrossRef] [Green Version]
- Cummins, S. Ecological approches to public health. In Health Geographies: A Critical Introduction; Sons, J.W., Ed.; Wiley Blackwell: Oxford, UK, 2017; pp. 137–155. [Google Scholar]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behavior. In Health Behavior and Health Education: Theory, Research and Practice; Jossey Bass: San Francisco, CA, USA, 2008; Volume 4, pp. 465–486. [Google Scholar]
- Potvin, L.; Jones, C.M. Twenty-five years after the ottawa charter: The critical role of health promotion for public health. Can. J. Public Health 2011, 102, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Hills, M.; McQueen, D.V. At issue: Two decades of the Ottawa charter. Promot. Educ. 2007, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- United Nations-Habitat and World Health Organization. Integrating Health in Urban and Territorial Planning; World Health Organization: Geneva, Switzerland, 2020; p. 89. [Google Scholar]
- Harris, P.J.; Harris-Roxas, B.F.; Kemp, L. Health impact assessment in urban settings. New South Wales Public Health Bull. 2007, 18, 149–150. [Google Scholar] [CrossRef] [Green Version]
- Harris-Roxas, B.; Harris, E. Differing forms, differing purposes: A typology of health impact assessment. Environ. Impact Assess. Rev. 2011, 31, 396–403. [Google Scholar] [CrossRef]
- World Health Organization. Health Organization. Health impact assessment: Main concepts and suggested approach—The Gothenburg consensus paper. In WHO European Centre for Health Policy; World Health Organization: Brussels, Belgium, 1999; p. 11. [Google Scholar]
- Quigley, R.; den Broeder, L.; Furu, P.; Bond, A.; Cave, B.; Bos, R. Health Impact Assessment International Best Practice Principles: Special Publication Series No 5; International Association for Impact Assessment: Fargo, ND, USA, 2006. [Google Scholar]
- Saint-Pierre, L.; Lamarre, M.-C.; Simos, J. L’évaluation d’impact sur la santé (EIS): Une démarche intersectorielle pour l’action sur les déterminants sociaux, économiques et environnementaux de la santé. Glob. Health Promot. 2014, 21, 7–14. [Google Scholar] [CrossRef] [Green Version]
- National Collaborating Centre for Healthy Public Policy (NCCHPP); Institut National de Santé Publique du Québec. Introducation to Health Impact Assessment (HIA); National Collaborating Centre for Healthy Public Policy: Montréal, QC, Canada, 2019. [Google Scholar]
- Bourcier, E.; Charbonneau, D.; Cahill, C.; Dannenberg, A.L. An evaluation of health impact assessments in the United States, 2011–2014. Prev. Chronic Dis. 2015, 12, E23. [Google Scholar] [CrossRef] [Green Version]
- Haigh, F.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Harris-Roxas, B.; Keleher, H.; Kemp, L.; Morgan, R.; Chok, H.N.G.; Spickett, J.; et al. The effectiveness of health impact assessment in influencing decision-making in Australia and New Zealand 2005–2009. BMC Public Health 2013, 13, 1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemm, J. Health Impact Assessment: Past Achievement, Current Understanding and Future Progress; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Winkler, M.S. Current global health impact assessment practice. Int. J. Environ. Res. Public Health 2020, 17, 2988. [Google Scholar] [CrossRef]
- De Leeuw, E.; Simos, J. Healthy Cities: The Theory, Policy and Practice of Value-Based Urban Planning; De Leeuw, E., Simos, J., Eds.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Noble, B.F. Environmental impact assessment. Available online: https://www.thecanadianencyclopedia.ca/en/article/environmental-impact-assessment (accessed on 16 October 2020).
- McCallum, L.C.; Ollson, C.A.; Stefanovic, I.L. Advancing the practice of health impact assessment in Canada: Obstacles and opportunities. Environ. Impact Assess. Rev. 2015, 55, 98–109. [Google Scholar] [CrossRef]
- Noble, B.; Bronson, J. Practitioner survey of the state of health integration in environmental assessment: The case of northern Canada. Environ. Impact Assess. Rev. 2006, 26, 410–424. [Google Scholar] [CrossRef]
- Health Canada. The Canadian Handbook on Health Impact Assessment; Health Canada: Ottawa, ON, Canada, 2004; Volume 1–4. [Google Scholar]
- Diallo, T.; Freeman, S. Health impact assessment—Insights from the experience of Québec. Environ. Health Rev. 2020, 63, 6–13. [Google Scholar] [CrossRef]
- Saint-Pierre, L.; Mendell, A. Health impact assessment in Canada. In Health Impact Assessment, Past Achievement, Current Understanding and Future Progress; Kemm, J., Ed.; Oxford University Press: Oxford, UK, 2013; pp. 224–232. [Google Scholar]
- Freeman, S. Health Impact Assessment (HIA) Knowledge and Needs Scan: Findings, Gaps and Recommendations; National Collaborating Centre for Environmental: Vancouver, BC, Canada, 2013. [Google Scholar]
- Government of British Columbia. Public Health Act; Queen‘s Printer: Victoria, BC, Canada, 2008.
- Sharpe, C.; Janzen, C.; Schwandt, M.; Dunn-Pierce, T.; Neudorf, C.; Meili, R. Growing Healthier: A Health Equity Impact Assessment Of Saskatoon’s Growth Plan; Saskatoon Health Region and Upstream: Saskatoon, SK, Canada, 2016. [Google Scholar]
- Molnar, A.; Renahy, E.; O’Campo, P.; Muntaner, C.; Freiler, A.; Shankardass, K. Using win-win strategies to implement health in all policies: A cross-case analysis. PLoS ONE 2016, 11, e0147003. [Google Scholar] [CrossRef] [Green Version]
- Nour, K.; Dutilly-Simard, S.; Brousselle, A.; Smits, P.; Buregeya, J.-M.; Loslier, J.; Denis, J.-L. Evaluation of the effects of health impact assessment practice at the local level in Monteregie. Health Res. Policy Syst. 2016, 14, 7. [Google Scholar] [CrossRef] [Green Version]
- Haigh, F.; Harris, E.; Harris, P.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Keleher, H.; Kemp, L.; Morgan, R.; Chok, H.N.; et al. What makes health impact assessments successful? Factors contributing to effectiveness in Australia and New Zealand. BMC Public Health 2015, 15, 1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nour, K.; Brousselle, A. Évaluation des Effets de la Pratique D’évaluation D’impact sur la Santé (ÉIS) en Montérégie; Centre Intégré de Santé et de Services Sociaux de la Montérégie-Centre: Longueuil, QC, Canada, 2018; p. 47. [Google Scholar]
- Ministère de la Santé et des Services Sociaux du Québec. Politique Gouvernementale de Prévention en Santé; Government of Québec: Québec, QC, Canada, 2016.
- Duhl, L.J.; Sanchez, K.A. Healthy Cities and the City Planning Process—A Background Document on Links between Health and Urban Planning; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- Heritage, Z.; Roué-Le Gall, A.; César, C. Urbanisme et aménagements favorables a la santé. Revue Santé Action 2015, 434, 12–13. [Google Scholar]
- Barton, H.; Tsourou, C. Urbanisme et Santé—Un guide de l’OMS pour un Urbanisme Centré sur les Habitants; S2D-Association Internationale Pour La Promotion De La Santé Et Du Développement Durable/OMS-Europe: Rennes, France, 2004. [Google Scholar]
- Simos, J. Paysage, urbanisme et santé. Environnement Risque Santé 2015, 14, 272–276. [Google Scholar]
- Harris, P.; Harris, P.; Wise, M.; Harris, L. Health impact assessment for urban and land-use planning and policy development: Lessons from practice. Plan. Pract. Res. 2010, 25, 531–541. [Google Scholar] [CrossRef]
- Forsyth, A.; Schively Slotterback, C.; Krizek, K. Health impact assessment (HIA) for planners: What tools are useful? J. Plan. Lit. 2010, 24, 231–245. [Google Scholar] [CrossRef]
- Wernham, A. Health impact assessments are needed in decision making about environmental and land-use policy. Health Aff. 2011, 30, 947–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roué-Le Gall, A.; Jabot, F. Health impact assessment on urban development projects in France: Finding pathways to fit practice to context. Glob. Health Promot. 2017, 24, 25–34. [Google Scholar] [CrossRef]
- Morley, M.R.; Lindberg, M.R.; Rogerson, M.B.; Bever, E.; Pollack, K.M. Seven years in the field of health impact assessment: Taking stock and future directions. Chron. Health Impact Assess. 2016, 1, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Signal, L.; Soeberg, M.; Quigley, R. Integrating health impact assessment with the policy process—Lessons and experiences from around the world. In Health Impact Assessment in Local Government: A New Zealand Case Study; O’Mullane, M., Ed.; Oxford University Press: Oxford, UK, 2013; pp. 109–118. [Google Scholar]
- Favre Kruit, C.; Kessler, C. Évaluation d’impact sur la santé. État des lieux au niveau cantonal en Suisse. Berne et Lausanne. Available online: https://promotionsante.ch/assets/public/documents/fr/5-grundlagen/publikationen/diverse-themen/arbeitspapiere/Document_de_travail_033_PSCH_2015-05_-_Evaluation_d_impact_sur_la_sante.pdf (accessed on 16 October 2020).
- Rudolph, L.; Caplan, J.; Mitchell, C.; Ben-Moshe, K.; Dillon, L.; California Department of Public Health; Public Health Institute Health in all policies. Improving health through intersectoral collaboration. NAM Perspect. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Progressing the Sustainable Development Goals through Health in All Policies: Case Studies from around the World; World Health Organisation: Adelaide, Australia, 2014; p. 204. [Google Scholar]
- Freiler, A.; Muntaner, C.; Shankardass, K.; Mah, C.L.; Molnar, A.; Renahy, E.; O’Campo, P. Glossary for the implementation of Health in All Policies (HiAP). J. Epidemiol. Community Health 2013, 67, 1068–1072. [Google Scholar] [CrossRef] [Green Version]
- Molnar, A.; O’Campo, P.; Ng, E.; Mitchell, C.; Muntaner, C.; Renahy, E.; John, A.S.; Shankardass, K. Protocol: Realist synthesis of the impact of unemployment insurance policies on poverty and health. Eval. Program Plan. 2015, 48, 1–9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HIA Projects | Sectoral Representatives | HIA Report | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HIA Project | Scale | QC | RPHA | VEV | NCCHPP | Promotor | DS | University | Student | Start | Completed | # Recommendations |
| Green Neighborhood | site | 2 | 2 | 0 | 1 | 0 | 0 | 1 | 9 | May 2013 | May 2015 | 22 |
| Local urban plan 1 | local | 3 | 6 | 0 | 1 | 0 | 0 | 2 | 5 | Sept. 2015 | May 2016 | 24 |
| Housing project | site | 3 | 2 | 2 | 1 | 1 | 3 | 2 | 0 | April 2017 | June 2017 | 24 |
| Local urban plan 2 | local | 3 | 3 | 2 | 1 | 0 | 3 | 2 | 1 | June 2016 | Jan. 2017 | 42 |
| Housing project | site | 3 | 3 | 2 | 1 | 1 | 3 | 2 | 0 | Sept. 2017 | Jan. 2018 | 41 |
| Industrial and high technology development plan | site | 3 | 3 | 1 | 0 | 0 | 3 | 2 | 0 | March 2018 | Sept. 2018 | 39 |
| Local street | local | 3 | 2 | 1 | 0 | 0 | 4 | 2 | 0 | July 2018 | Dec. 2018 | 23 |
| Public transport | site | 1 | 4 | 1 | 0 | 2 | 0 | 2 | 4 | Sept. 2018 | May 2019 | 59 |
| Public space | local | 2 | 1 | 1 | 0 | 0 | 3 | 2 | 1 | Jan 2019 | May 2019 | 21 |
| Park | local | 3 | 2 | 1 | 0 | 0 | 3 | 2 | 0 | Sept. 2019 | April 2020 | 21 |
| Recommendation | Application |
|---|---|
| Separate the dog park in two with an opaque barrier, one part for small dogs and the other for big dogs, which should discourage barking. | The municipality used this recommendation and all related explanations when residents asked which improvements would be made to reduce the noise level related to the dog park. |
| Universal accessibility: favor mobility using a wheelchair and improve the comfort of pedestrian infrastructure by installing 2.4m-sidewalks on each side of the road. | The concept was presented to a committee. Modifications have thus been applied to allow for living spaces for vulnerable populations in the project. |
| Pedestrian safety: adjust the speed limit according to the ambient characteristics to be coherent with the environment (30 km/h for the residential neighborhood). | This was a major preoccupation for the municipality. This recommendation allowed for an insistence on the application of measures for the safety of pedestrians. All parties involved in the project were asked to consider pedestrians. |
| Lighting: there should be 5 m between lamp posts. Blue/white light should be diminished, and yellow light should be favored to reduce the impact on the circadian rhythm of the residents. 6 lux for pedestrian and cyclists’ areas and 8 lux for residential streets. | This allowed the reconsideration of norms regarding lighting in residential zones for better lighting and not more lighting. |
| Favor urban agriculture: create gardens on the roofs to favor access to fresh fruits and vegetables for disadvantaged populations. | Community gardens were integrated in the project since the HIA provided a space to debate this with stakeholders, promoters and municipal officials. |
| Social diversity: ensure a certain level of social diversity by adding nine social housing units to represent 10% of the total number of units. | It was decided that within the 700 units that would be developed, 70 would be for social housing (10%) which was recommended in the HIA. |
| Air quality: increase the green area of the neighborhood to increase the air filtration capacity of the neighborhood. | Greening and adding to green areas have been considered to reduce the bad air quality. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamache, S.; Diallo, T.A.; Shankardass, K.; Lebel, A. The Elaboration of an Intersectoral Partnership to Perform Health Impact Assessment in Urban Planning: The Experience of Quebec City (Canada). Int. J. Environ. Res. Public Health 2020, 17, 7556. https://doi.org/10.3390/ijerph17207556
Gamache S, Diallo TA, Shankardass K, Lebel A. The Elaboration of an Intersectoral Partnership to Perform Health Impact Assessment in Urban Planning: The Experience of Quebec City (Canada). International Journal of Environmental Research and Public Health. 2020; 17(20):7556. https://doi.org/10.3390/ijerph17207556
Chicago/Turabian StyleGamache, Stéphanie, Thierno Amadou Diallo, Ketan Shankardass, and Alexandre Lebel. 2020. "The Elaboration of an Intersectoral Partnership to Perform Health Impact Assessment in Urban Planning: The Experience of Quebec City (Canada)" International Journal of Environmental Research and Public Health 17, no. 20: 7556. https://doi.org/10.3390/ijerph17207556
APA StyleGamache, S., Diallo, T. A., Shankardass, K., & Lebel, A. (2020). The Elaboration of an Intersectoral Partnership to Perform Health Impact Assessment in Urban Planning: The Experience of Quebec City (Canada). International Journal of Environmental Research and Public Health, 17(20), 7556. https://doi.org/10.3390/ijerph17207556