Cultural Adaptation, Validation, and Primary Application of a Questionnaire to Assess Intentions to Eat Low-Glycemic Index Foods among Rural Chinese Women


 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Study Design
2.2. Participant Recruitment and Enrollment
2.3. Data Collection
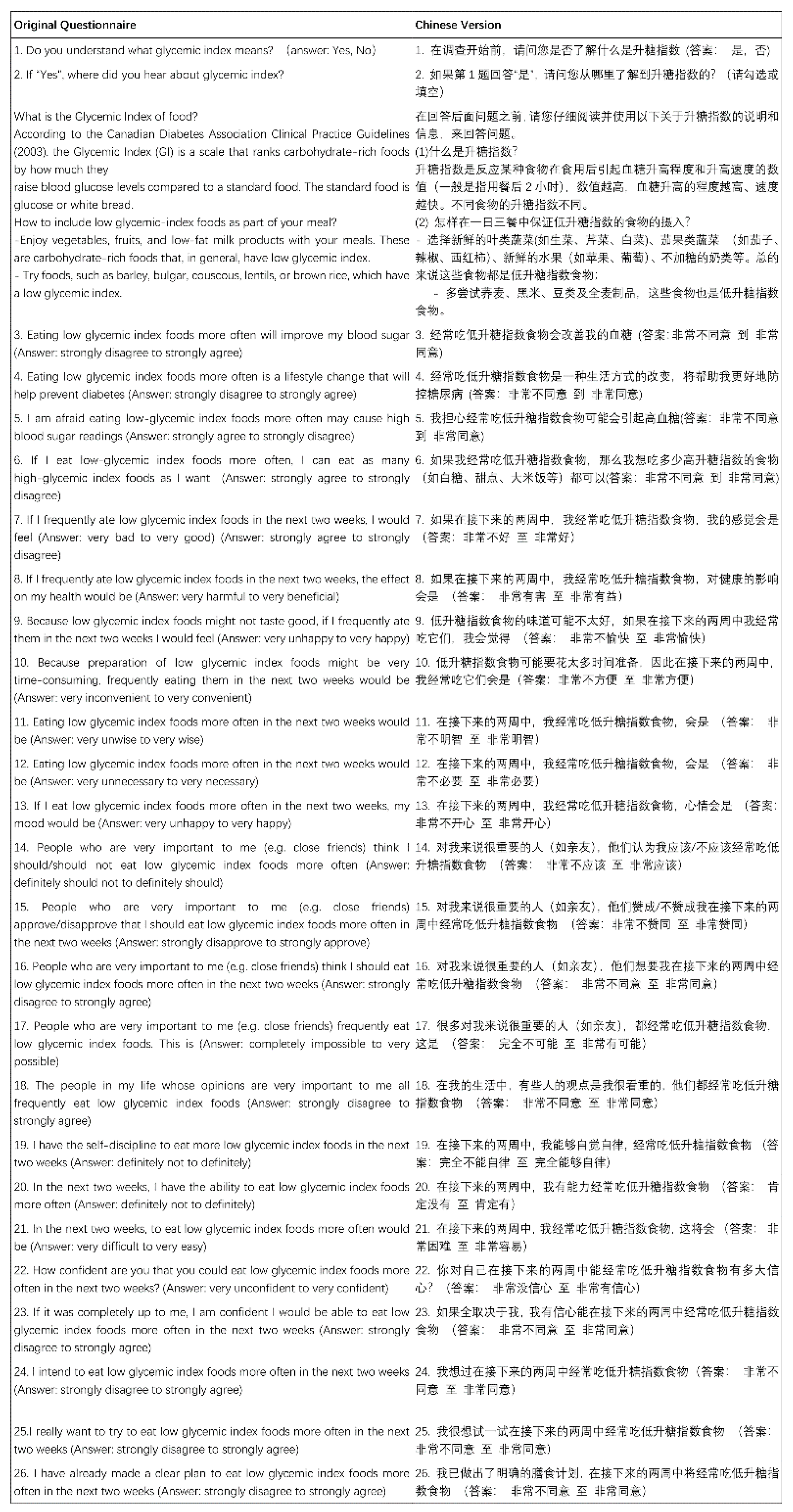
2.3.1. Assessment of the Intention to Eat Low-GI Foods
2.3.2. Assessment of Glycemic Status
2.3.3. Anthropometric Measurements
2.3.4. Dietary Measurements
2.3.5. Physical Activity Measurements
2.3.6. Other Covariates
2.4. Statistical Analysis
3. Results
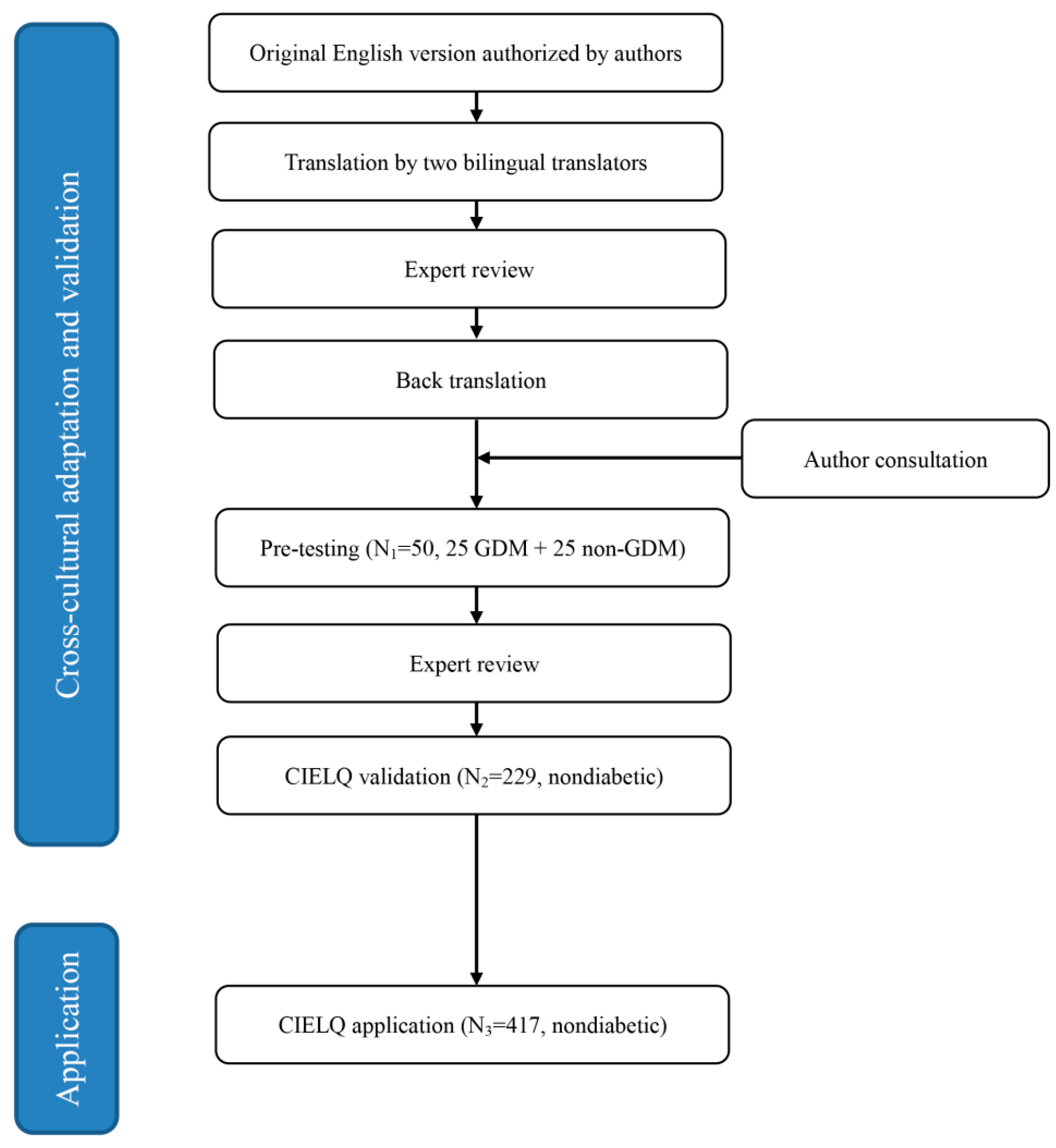
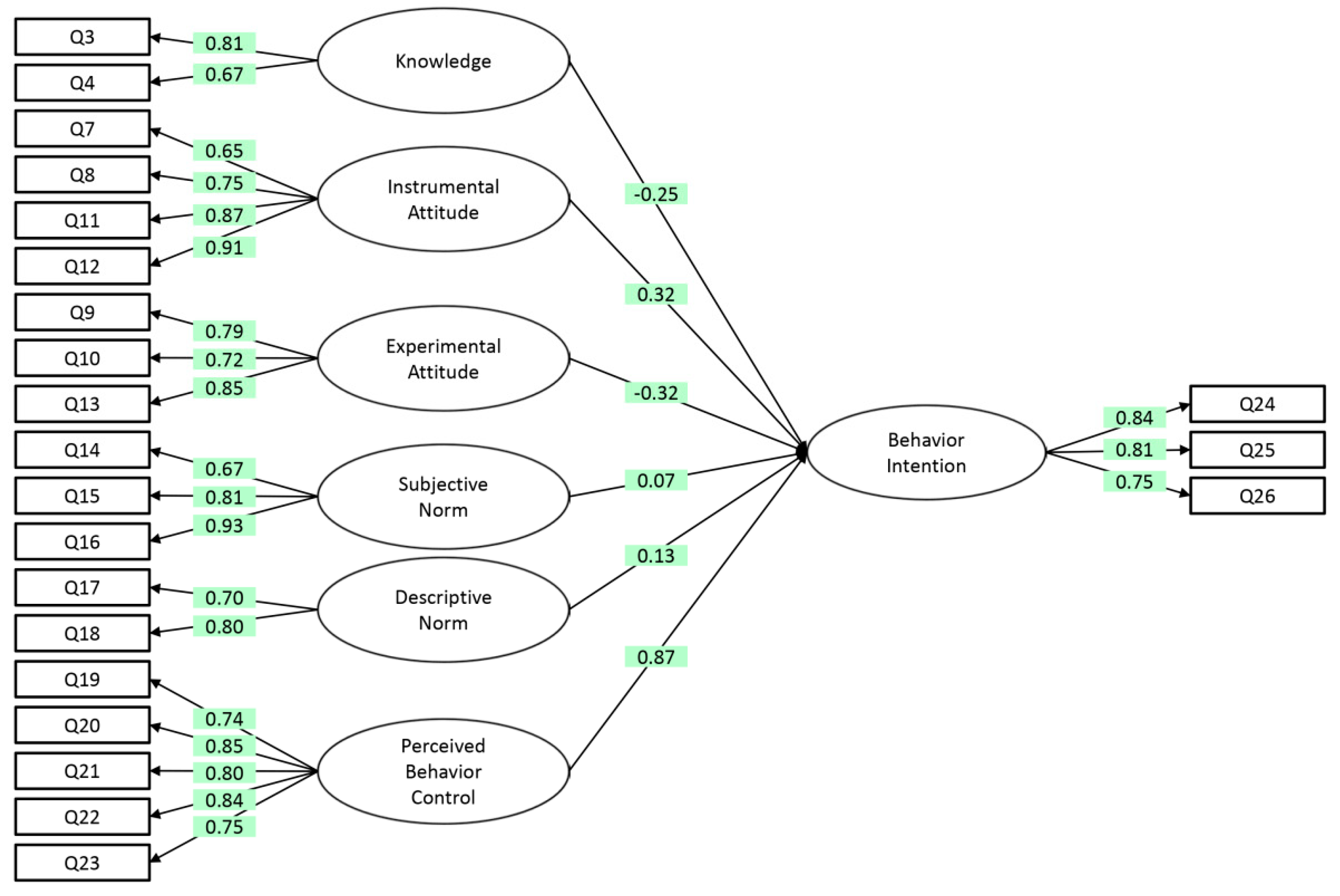
3.1. Cross-Cultural Adaptation and Validation of the CIELQ and Its Application
3.2. Application of the CIELQ
3.2.1. Characteristics of the Participants
3.2.2. CIELQ Score and Its Association with Covariates
3.2.3. CIELQ Score and Its Association with Glycemic Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Cases | % | |||
|---|---|---|---|---|---|
| Age a | |||||
| ≤24 | 11 | 4.8 | |||
| 25–29 | 57 | 24.9 | |||
| 30–34 | 81 | 35.4 | |||
| 35–39 | 49 | 21.4 | |||
| ≥40 | 21 | 9.2 | |||
| Ethnicity | |||||
| Han | 91 | 39.7 | |||
| Minority | 138 | 60.3 | |||
| Education level | |||||
| Primary school and below | 3 | 1.3 | |||
| Primary middle school | 38 | 16.6 | |||
| Senior middle school | 55 | 24.0 | |||
| College | 82 | 35.8 | |||
| Graduate and above | 51 | 22.3 | |||
| Family monthly income (CNY) b | |||||
| ≤999 | 7 | 30.6 | |||
| 1000–3000 | 64 | 27.9 | |||
| ≥3001 | 145 | 63.3% | |||
| BMI (kg/m2) c | |||||
| Underweight | 13 | 5.7 | |||
| Normal | 111 | 48.5 | |||
| Overweight | 70 | 30.6 | |||
| Obese | 29 | 12.7 | |||
| Gravidity d | |||||
| 1 | 67 | 37.0 | |||
| 2 | 50 | 27.6 | |||
| 3 | 27 | 14.9 | |||
| 4 | 19 | 10.5 | |||
| ≥5 | 18 | 9.9 | |||
| Parity e | |||||
| 0 | 4 | 1.7 | |||
| 1 | 87 | 38.0 | |||
| 2 | 82 | 35.8 | |||
| ≥3 | 8 | 3.5 | |||
| Dimension of Questionnaire | Cronbach’s Alpha |
|---|---|
| Total questionnaire | 0.945 |
| Knowledge | 0.724 |
| Instrumental attitude | 0.871 |
| Experiential attitude | 0.823 |
| Subjective norm | 0.869 |
| Descriptive norm | 0.715 |
| Perceived behaviour control | 0.901 |
| Behaviour intention | 0.843 |
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beta | p Value | Beta | p Value | Beta | p Value | Beta | p Value | Beta | p Value | Beta | p Value | Beta | p Value | |
| BMI category | 0.007 | 0.875 | 0.018 | 0.617 | 0.039 | 0.322 | 0.089 | 0.022 | 0.009 | 0.841 | −0.039 | 0.272 | 0.045 | 0.158 |
| Age group | 0.033 | 0.505 | −0.007 | 0.866 | 0.081 | 0.054 | −0.081 | 0.053 | 0.093 | 0.051 | −0.013 | 0.724 | 0.052 | 0.130 |
| Ethnicity | −0.01 | 0.835 | −0.040 | 0.259 | −0.009 | 0.815 | −0.012 | 0.751 | −0.012 | 0.779 | 0.042 | 0.231 | −0.004 | 0.907 |
| Education level | 0.071 | 0.165 | 0.119 | 0.003 a | −0.096 | 0.028 a | −0.090 | 0.038 a | 0.039 | 0.432 | −0.019 | 0.637 | −0.089 | 0.013 a |
| Family monthly income level | 0.065 | 0.160 | 0.002 | 0.949 | −0.037 | 0.348 | 0.013 | 0.747 | 0.064 | 0.154 | −0.005 | 0.897 | 0.027 | 0.403 |
| Diabetes history of father | 0.035 | 0.442 | −0.067 | 0.055 | 0.103 | 0.007 a | −0.003 | 0.933 | −0.011 | 0.805 | −0.016 | 0.646 | 0.047 | 0.134 |
| Diabetes history of mother | 0.032 | 0.478 | −0.020 | 0.579 | 0.056 | 0.144 | −0.046 | 0.232 | 0.093 | 0.033 a | −0.073 | 0.036 a | −0.049 | 0.118 |
| Diabetes history of siblings | −0.015 | 0.743 | 0.007 | 0.846 | −0.044 | 0.250 | 0.006 | 0.883 | −0.002 | 0.960 | 0.042 | 0.223 | 0.041 | 0.184 |
| Gravidity | −0.062 | 0.270 | 0.053 | 0.223 | 0.022 | 0.646 | −0.001 | 0.985 | −0.004 | 0.947 | −0.028 | 0.512 | 0.044 | 0.261 |
| Parity | 0.048 | 0.405 | −0.032 | 0.483 | −0.035 | 0.482 | −0.033 | 0.504 | 0.062 | 0.267 | 0.031 | 0.491 | −0.037 | 0.355 |
| Awareness of GI | −0.027 | 0.561 | 0.035 | 0.336 | −0.069 | 0.078 | −0.023 | 0.556 | −0.089 | 0.044 a | 0.04 | 0.257 | −0.017 | 0.607 |
| Glyceamic testing in 3 months | −0.07 | 0.132 | 0.018 | 0.614 | −0.018 | 0.642 | −0.081 | 0.037 a | 0.067 | 0.130 | −0.019 | 0.598 | 0.016 | 0.619 |
| Score of knowledge | - | - | 0.232 | 0.000 a | −0.093 | 0.046 | 0.109 | 0.017 a | −0.063 | 0.224 | 0.139 | 0.001 a | −0.017 | 0.650 |
| Score of instrumental attitude | 0.384 | 0.000 a | - | - | 0.347 | 0.000 a | 0.410 | 0.000 a | 0.084 | 0.210 | 0.079 | 0.139 | 0.129 | 0.008 a |
| Score of experimental attitude | −0.127 | 0.046 a | 0.287 | 0.000 a | - | - | −0.038 | 0.485 | −0.003 | 0.957 | 0.412 | 0.000 a | −0.133 | 0.003 a |
| Score of subjective norm | 0.152 | 0.017 a | 0.345 | 0.000 a | −0.038 | 0.485 | - | - | 0.238 | 0.000 a | 0.153 | 0.002 a | 0.153 | 0.001 a |
| Score of descriptive norm | −0.069 | 0.224 | 0.055 | 0.210 | −0.003 | 0.957 | 0.185 | 0.000 a | - | - | 0.261 | 0.000 a | 0.116 | 0.003 a |
| Score of PBC | 0.236 | 0.001 a | 0.081 | 0.139 | 0.513 | 0.000 a | 0.187 | 0.002 a | 0.410 | 0.000 a | - | - | 0.636 | 0.000 a |
References
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; di Renzo, G.C.; Cabero, R.L.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. S3), S173–S211. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Zhang, C. Prevalence of Gestational Diabetes and Risk of Progression to Type 2 Diabetes: A Global Perspective. Curr. Diabetes Rep. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Sun, X.; Lu, L.; Liu, F.; Yuan, J. Prevalence of gestational diabetes mellitus in mainland China: A systematic review and meta-analysis. J. Diabetes Investig. 2019, 10, 154–162. [Google Scholar] [CrossRef]
- He, Z.; Xie, H.; Liang, S.; Tang, Y.; Ding, W.; Wu, Y.; Ming, W.K. Influence of different diagnostic criteria on gestational diabetes mellitus incidence and medical expenditures in China. J. Diabetes Investig. 2019, 10, 1347–1357. [Google Scholar] [CrossRef] [PubMed]
- Wendland, E.M.; Torloni, M.R.; Falavigna, M.; Trujillo, J.; Dode, M.A.; Campos, M.A.; Duncan, B.B.; Schmidt, M.I. Gestational diabetes and pregnancy outcomes—A systematic review of the World Health Organization (WHO) and the International Association of Diabetes in Pregnancy Study Groups (IADPSG) diagnostic criteria. BMC Pregnancy Childbirth 2012, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldfield, M.D.; Donley, P.; Walwyn, L.; Scudamore, I.; Gregory, R. Long term prognosis of women with gestational diabetes in a multiethnic population. Postgrad. Med. J. 2007, 83, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Chen, J.L.; Whittemore, R.; Whitaker, E. Postpartum Lifestyle Interventions to Prevent Type 2 Diabetes Among Women with History of Gestational Diabetes: A Systematic Review of Randomized Clinical Trials. J. Womens Health 2016, 25, 38–49. [Google Scholar] [CrossRef]
- Shyam, S.; Arshad, F.; Abdul, G.R.; Wahab, N.A.; Safii, N.S.; Nisak, M.Y.; Chinna, K.; Kamaruddin, N.A. Low glycaemic index diets improve glucose tolerance and body weight in women with previous history of gestational diabetes: A six months randomized trial. Nutr. J. 2013, 12, 68. [Google Scholar] [CrossRef] [Green Version]
- Ghani, R.A.; Shyam, S.; Arshad, F.; Wahab, N.A.; Chinna, K.; Safii, N.S.; Nisak, M.Y.; Kamaruddin, N.A. The influence of fasting insulin level in post-gestational diabetes mellitus women receiving low-glycaemic-index diets. Nutr. Diabetes 2014, 4, e107. [Google Scholar] [CrossRef] [Green Version]
- Wan, C.S.; Nankervis, A.; Teede, H.; Aroni, R. Dietary intervention strategies for ethnic Chinese women with gestational diabetes mellitus: A systematic review and meta-analysis. Nutr. Diet. 2019, 76, 211–232. [Google Scholar] [CrossRef]
- Amano, Y.; Sugiyama, M.; Lee, J.S.; Kawakubo, K.; Mori, K.; Tang, A.C.; Akabayashi, A. Glycemic index-based nutritional education improves blood glucose control in Japanese adults: A randomized controlled trial. Diabetes Care 2007, 30, 1874–1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, C.K.; Gutschall, M. A randomized trial about glycemic index and glycemic load improves outcomes among adults with type 2 diabetes. Health Educ. Behav. 2009, 36, 615–626. [Google Scholar] [CrossRef]
- Li, Q.; Xiong, R.; Wang, L.; Cui, J.; Shi, L.; Liu, Y.; Luo, B. Associations of dietary habits, physical activity and cognitive views with gestational diabetes mellitus among Chinese women. Public Health Nutr. 2014, 17, 1850–1857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, L.; Wikby, K.; Rask, M. ‘Is gestational diabetes a severe illness?’ exploring beliefs and self-care behaviour among women with gestational diabetes living in a rural area of the south east of China. Aust. J. Rural Health 2016, 24, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Godin, G.; Kok, G. The theory of planned behavior: A review of its applications to health-related behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef]
- Sussman, R.; Gifford, R. Causality in the Theory of Planned Behavior. Pers. Soc. Psychol. Bull. 2019, 45, 920–933. [Google Scholar] [CrossRef] [Green Version]
- Rich, A.; Brandes, K.; Mullan, B.; Hagger, M.S. Theory of planned behavior and adherence in chronic illness: A meta-analysis. J. Behav. Med. 2015, 38, 673–688. [Google Scholar] [CrossRef] [Green Version]
- McDermott, M.S.; Oliver, M.; Simnadis, T.; Beck, E.J.; Coltman, T.; Iverson, D.; Caputi, P.; Sharma, R. The Theory of Planned Behaviour and dietary patterns: A systematic review and meta-analysis. Prev. Med. 2015, 81, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eades, C.E.; France, E.F.; Evans, J. Postnatal experiences, knowledge and perceptions of women with gestational diabetes. Diabet. Med. 2018, 35, 519–529. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Berry, T.R.; Willows, N.D.; Bell, R.C. Assessing Intentions to Eat Low-Glycemic Index Foods by Adults with Diabetes Using a New Questionnaire Based on the Theory of Planned Behaviour. Can. J. Diabetes 2015, 39, 94–100. [Google Scholar] [CrossRef]
- Bujang, M.A.; Sa’At, N.; Sidik, T.; Joo, L.C. Sample Size Guidelines for Logistic Regression from Observational Studies with Large Population: Emphasis on the Accuracy Between Statistics and Parameters Based on Real Life Clinical Data. Malays. J. Med. Sci. 2018, 25, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Tang, Y.; Wiley, J.; Whittemore, R.; Chen, J.L. Effectiveness of a diabetes prevention program for rural women with prior gestational diabetes mellitus: Study protocol of a multi-site randomized clinical trial. BMC Public Health 2018, 18, 809. [Google Scholar] [CrossRef] [PubMed]
- Process of Translation and Adaptation of Instruments. Available online: http://wwwwhoint/substance_abuse/research_tools/translation/en/ (accessed on 4 June 2020).
- Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition). Chin. J. Pract. Intern. Med. 2018, 38, 292–344. [Google Scholar]
- Working Group on Obesity in China. Guidelines on prevention and Control of Overweight and Obesity in Chinese Adults (Excerpts). Acta Nutr. Sin. 2004, 26, 1–4. [Google Scholar]
- Thornton, K.; Villamor, E. Nutritional epidemiology. In Encyclopedia of Food and Health; Caballero, B., Finglas, P.M., Toldrá, F., Eds.; Academic Press: Oxford, UK, 2016; pp. 104–107. [Google Scholar]
- International Physical Activity Questionnaire. Available online: https://sites.google.com/site/theipaq/questionnaire_links (accessed on 4 June 2020).
- Bland, J.M.; Altman, D.G. Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [Green Version]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: London, UK, 2012. [Google Scholar]
- Zhang, F.; Dong, L.; Zhang, C.P.; Li, B.; Wen, J.; Gao, W.; Sun, S.; Lv, F.; Tian, H.; Tuomilehto, J.; et al. Increasing prevalence of gestational diabetes mellitus in Chinese women from 1999 to 2008. Diabetes Med. 2011, 28, 652–657. [Google Scholar] [CrossRef]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef] [Green Version]
- Waller, B.; Tzeng, H.M. Glycaemic index knowledge and use among African Americans with type 2 diabetes. J. Adv. Nurs. 2011, 67, 1102–1108. [Google Scholar] [CrossRef]
- Avedzi, H.M.; Mathe, N.; Storey, K.; Johnson, J.A.; Johnson, S.T. Examining sex differences in glycemic index knowledge and intake among individuals with type 2 diabetes. Prim. Care Diabetes 2018, 12, 71–79. [Google Scholar] [CrossRef]
- Yuan, Y.Q.; Li, F.; Dong, R.H.; Chen, J.S.; He, G.S.; Li, S.G.; Chen, B. The Development of a Chinese Healthy Eating Index and Its Application in the General Population. Nutrients 2017, 9, 977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Y.Q.; Li, F.; Wu, H.; Wang, Y.C.; Chen, J.S.; He, G.S.; Li, S.G.; Chen, B. Evaluation of the Validity and Reliability of the Chinese Healthy Eating Index. Nutrients 2018, 10, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef]
- Zhao, J.V.; Schooling, C.M.; Zhao, J.X. The effects of folate supplementation on glucose metabolism and risk of type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Ann. Epidemiol. 2018, 28, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.Y.; Sim, X.; Wu, Y.; Liang, J.; Tabara, Y.; Hu, C.; Hara, K.; Tam, C.H.; Cai, Q.; Zhao, Q.; et al. Genome-wide association meta-analysis identifies novel variants associated with fasting plasma glucose in East Asians. Diabetes 2015, 64, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fretts, A.M.; Follis, J.L.; Nettleton, J.A.; Lemaitre, R.N.; Ngwa, J.S.; Wojczynski, M.K.; Kalafati, I.P.; Varga, T.V.; Frazier-Wood, A.C.; Houston, D.K.; et al. Consumption of meat is associated with higher fasting glucose and insulin concentrations regardless of glucose and insulin genetic risk scores: A meta-analysis of 50,345 Caucasians. Am. J. Clin. Nutr. 2015, 102, 1266–1278. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Imperatore, G.; Thomas, W.; Cheng, Y.J.; Lobelo, F.; Norris, K.; Devlin, H.M.; Ali, M.K.; Gruss, S.; Bardenheier, B.; et al. Effect of lifestyle interventions on glucose regulation among adults without impaired glucose tolerance or diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2017, 123, 149–164. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.H.; Jung, S.H.; Lee, B.; Choi, D.; Kim, B.Y.; Kim, C.H.; Kang, S.K.; Mok, J.O. Differential Impact of Sleep Duration on Fasting Plasma Glucose Level According to Work Timing. Arch. Med. Res. 2018, 49, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Bélanger, L.J.; Plotnikoff, R.C.; Clark, A.M.; Courneya, K.S. Determinants of physical activity in young adult cancer survivors. Am. J. Health Behav. 2012, 36, 483–494. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Plotnikoff, R.C.; Courneya, K.S. Predicting the physical activity intention-behavior profiles of adopters and maintainers using three social cognition models. Ann. Behav. Med. 2008, 36, 244–252. [Google Scholar] [CrossRef]
- Ajzen, I. Constructing a TPB Questionnaire: Conceptual and Methodological Considerations; Working Paper; University of Massachusetts: Amherst, MA, USA, 2002. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Tabulation on the 2010 Population Census of the People’s Republic of China. Available online: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexce.htm (accessed on 23 August 2020).


| Variables | Cases | % | |
|---|---|---|---|
| Age (years) a | |||
| ≤24 | 25 | 6% | |
| 25–29 | 122 | 29.3% | |
| 30–34 | 145 | 34.8% | |
| 35–39 | 77 | 18.5% | |
| ≥40 | 41 | 9.8% | |
| Ethnicity b | |||
| Han | 233 | 55.9% | |
| Minority | 183 | 43.9% | |
| Education level | |||
| Primary school and below | 4 | 1% | |
| Primary middle school | 89 | 21.3% | |
| Senior middle school | 120 | 28.8% | |
| College | 114 | 27.3% | |
| Graduate and above | 90 | 21.6% | |
| Family monthly income (CNY) c | |||
| ≤999 | 9 | 2.2% | |
| 1000–3000 | 98 | 23.5% | |
| ≥3001 | 294 | 70.5% | |
| BMI (kg/m2) d | |||
| Underweight | 17 | 4.1% | |
| Normal | 209 | 50.1% | |
| Overweight | 127 | 30.5% | |
| Obese | 58 | 13.9% | |
| Gravidity e | |||
| 1 | 108 | 25.9% | |
| 2 | 96 | 23% | |
| 3 | 96 | 23% | |
| 4 | 67 | 16.1% | |
| ≥5 | 49 | 11.8% | |
| Parity f | |||
| 0 | 1 | 0.2% | |
| 1 | 155 | 37.2% | |
| 2 | 249 | 59.7% | |
| ≥3 | 11 | 2.6% | |
| Factors | N | Median (95% CI) |
|---|---|---|
| Knowledge (Q3,Q4) | 412 | 12 (11.00–12.00) |
| Instrumental attitude (Q7, Q8, Q11 and Q12) | 415 | 20 (20.00–21.00) |
| Experimental attitude (Q9, Q10 and Q13) | 415 | 12 (12.00–13.00) |
| Subjective norm (Q14 to Q16) | 414 | 16 (15.00–16.49) |
| Descriptive norm (Q17 and Q18) | 415 | 9 (8.00–9.00) |
| Perceived behavioral control (Q19 to Q23) | 413 | 24 (23.00–25.00) |
| Intention (Q24 to Q26) | 414 | 15 (15.00–16.00) |
| Total score | 398 | 106 (103.00–110.00) |
| Dependent | Independent | Crude OR(95% CI) | p-Value | Adjusted OR(95% CI) | p-Value |
|---|---|---|---|---|---|
| FPG | Score of knowledge | 0.988 (0.821–1.191) | 0.903 | - | - |
| Score of instrumental attitude | 1.023 (0.931–1.124) | 0.634 | - | - | |
| Score of experimental attitude | 0.976 (0.870–1.096) | 0.684 | - | - | |
| Score of subjective norm | 0.996 (0.891–1.113) | 0.942 | 0.848 (0.640–1.043) a | 0.118 | |
| Score of descriptive norm | 0.801 (0.683–0.938) | 0.006 | - | - | |
| Score of PBC | 0.960 (0.897–1.027) | 0.236 | - | - | |
| Score of behavior intention | 0.968 (0.858–1.091) | 0.591 | - | - | |
| Score of total score | 0.991 (0.970–1.012) | 0.392 | - | - | |
| 2h-OGTT | Score of knowledge | 1.016 (0.893–1.156) | 0.813 | - | - |
| Score of instrumental attitude | 0.963 (0.901–1.029) | 0.265 | 1.330 (1.036–1.708) b | 0.025 | |
| Score of experimental attitude | 1.047 (0.966–1.135) | 0.260 | 0.837 (0.640–1.093) b | 0.191 | |
| Score of subjective norm | 0.965 (0.890–1.045) | 0.381 | - | - | |
| Score of descriptive norm | 1.041 (0.931–1.164) | 0.480 | - | - | |
| Score of PBC | 1.012 (0.964–1.062) | 0.625 | 0.793 (0.640–0.983) b | 0.035 | |
| Score of behavior intention | 0.965 (0.883–1.054) | 0.425 | - | - | |
| Score of total score | 1.000 (0.985–1.014) | 0.974 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Li, F.; Lin, Q.; Shi, J.; Luo, J.; Long, Q.; Yang, Q.; Ouyang, Y.; Liu, H.; Bell, R.C.; et al. Cultural Adaptation, Validation, and Primary Application of a Questionnaire to Assess Intentions to Eat Low-Glycemic Index Foods among Rural Chinese Women. Int. J. Environ. Res. Public Health 2020, 17, 7577. https://doi.org/10.3390/ijerph17207577
Li M, Li F, Lin Q, Shi J, Luo J, Long Q, Yang Q, Ouyang Y, Liu H, Bell RC, et al. Cultural Adaptation, Validation, and Primary Application of a Questionnaire to Assess Intentions to Eat Low-Glycemic Index Foods among Rural Chinese Women. International Journal of Environmental Research and Public Health. 2020; 17(20):7577. https://doi.org/10.3390/ijerph17207577
Chicago/Turabian StyleLi, Mingshu, Fang Li, Qian Lin, Jingzheng Shi, Jing Luo, Qing Long, Qiping Yang, Yufeng Ouyang, Hanmei Liu, Rhonda C. Bell, and et al. 2020. "Cultural Adaptation, Validation, and Primary Application of a Questionnaire to Assess Intentions to Eat Low-Glycemic Index Foods among Rural Chinese Women" International Journal of Environmental Research and Public Health 17, no. 20: 7577. https://doi.org/10.3390/ijerph17207577
APA StyleLi, M., Li, F., Lin, Q., Shi, J., Luo, J., Long, Q., Yang, Q., Ouyang, Y., Liu, H., Bell, R. C., & Guo, J. (2020). Cultural Adaptation, Validation, and Primary Application of a Questionnaire to Assess Intentions to Eat Low-Glycemic Index Foods among Rural Chinese Women. International Journal of Environmental Research and Public Health, 17(20), 7577. https://doi.org/10.3390/ijerph17207577