Impact of Non-Tailored One-Way Automated Short Messaging Service (OASMS) on Glycemic Control in Type 2 Diabetes: A Retrospective Feasibility Study



 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
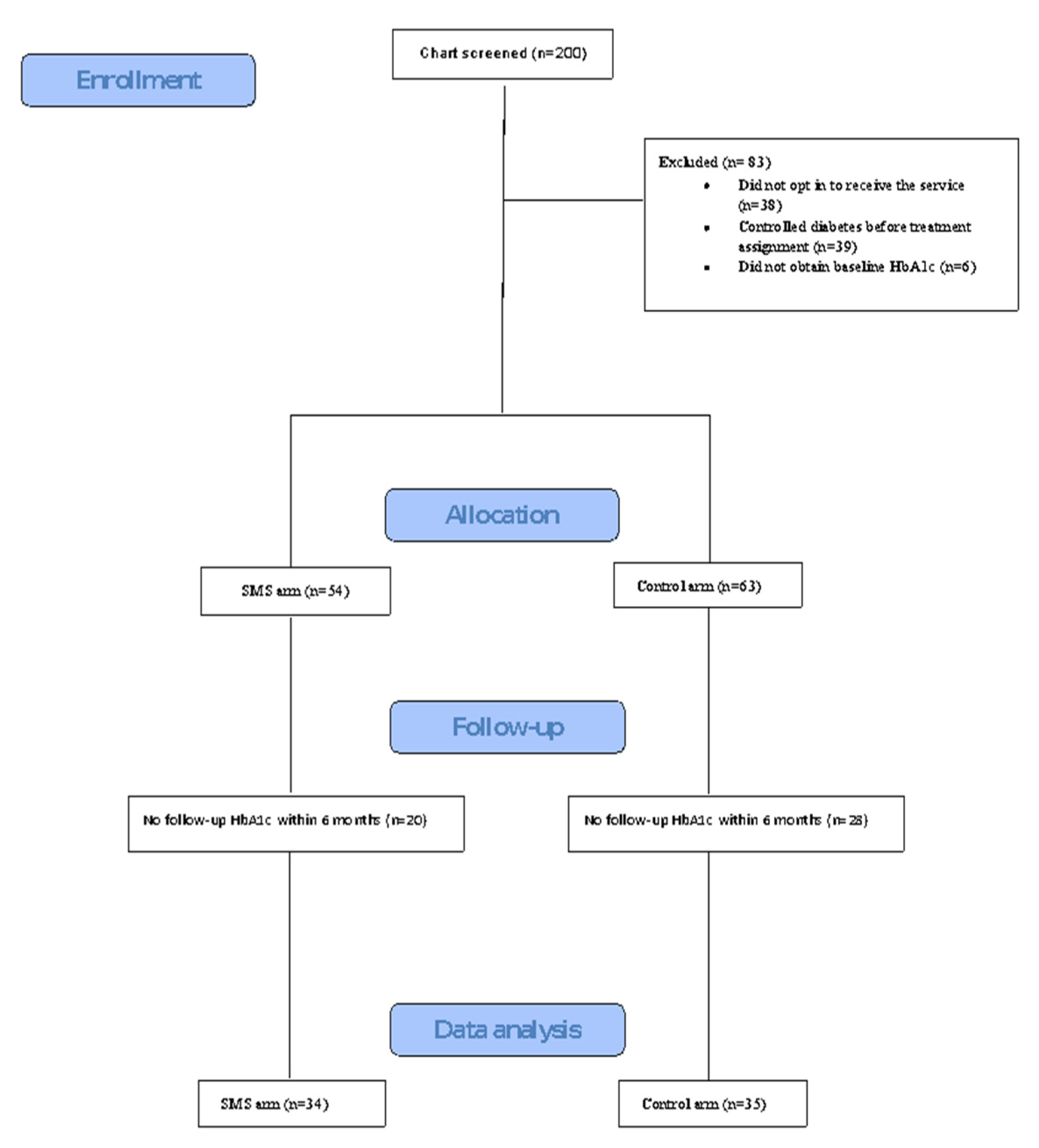
2.2. Sample Selection
2.3. The SMS Intervention
2.4. Data Collection and Variables
2.5. Outcomes
2.6. Statistical Analysis
2.7. Propensity Scores and Inverse Propensity Score Weighting (IPSW)
2.8. Response (HbA1c Reduction) Predictors
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chen, L.M.; Farwell, W.R.; Jha, A.K. Primary care visit duration and quality: Does good care take longer? Arch. Intern. Med. 2009, 169, 1866–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, J.; Greenwood, D.A.; Blanton, L.; Bollinger, S.T.; Butcher, M.K.; Condon, J.E.; Cypress, M.; Faulkner, P.; Fischl, A.H.; Francis, T.; et al. 2017 National Standards for Diabetes Self-Management Education and Support. Diabetes Educ. 2017, 43, 449–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwennesen, N.; Henriksen, J.E.; Willaing, I. Patient explanations for non-attendance at type 2 diabetes self-management education: A qualitative study. Scand. J. Caring Sci. 2016, 30, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Muse, E.D.; Topol, E.J. Can mobile health technologies transform health care? JAMA 2013, 310, 2395–2396. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Topol, E.J. State of Telehealth. N. Engl. J. Med. 2016, 375, 154–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pew Research Center, U.S. Smartphone Use in 2015. In Pew Research Center: Internet, Science & Tech; 2015; Available online: https://www.pewresearch.org/internet/2015/04/01/us-smartphone-use-in-2015/ (accessed on 23 June 2020).
- Greenwood, D.A.; Hankins, A.I.; Parise, C.A.; Spier, V.; Olveda, J.; Buss, K.A. A Comparison of In-person, Telephone, and Secure Messaging for Type 2 Diabetes Self-Management Support. Diabetes Educ. 2014, 40, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Bobrow, K.; Farmer, A.; Cishe, N.; Nwagi, N.; Namane, M.; Brennan, T.P.; Springer, D.; Tarassenko, L.; Levitt, N. Using the Medical Research Council framework for development and evaluation of complex interventions in a low resource setting to develop a theory-based treatment support intervention delivered via SMS text message to improve blood pressure control. BMC Health Serv. Res. 2018, 18, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Q.; Chen, F.; Wang, T. Effectiveness of short message service intervention to improve glycated hemoglobin control and medication adherence in type-2 diabetes: A meta-analysis of prospective studies. Prim. Care Diabetes 2019. [Google Scholar] [CrossRef] [PubMed]
- Saffari, M.; Ghanizadeh, G.; Koenig, H.G. Health education via mobile text messaging for glycemic control in adults with type 2 diabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2014, 8, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Wang, Q.; Yang, X.; Cao, J.; Chen, J.; Mo, X.; Huang, J.; Wang, L.; Gu, D. Effect of mobile phone intervention for diabetes on glycaemic control: A meta-analysis. Diabet. Med. J. Br. Diabet. Assoc. 2011, 28, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Owolabi, E.O.; Goon, D.T. The use of text messaging for improving adherence to anti-diabetic regimen and glycaemic control in low-resource settings of South Africa: A study protocol for a randomised controlled trial. Contemp. Clin. Trials Commun. 2019, 15, 100418. [Google Scholar] [CrossRef] [PubMed]
- Arambepola, C.; Ricci-Cabello, I.; Manikavasagam, P.; Roberts, N.; French, D.P.; Farmer, A. The Impact of Automated Brief Messages Promoting Lifestyle Changes Delivered Via Mobile Devices to People with Type 2 Diabetes: A Systematic Literature Review and Meta-Analysis of Controlled Trials. J. Med. Internet Res. 2016, 18, e86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobson, R.; Whittaker, R.; Pfaeffli Dale, L.; Maddison, R. The effectiveness of text message-based self-management interventions for poorly-controlled diabetes: A systematic review. Digit. Health 2017, 3, 2055207617740315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Clin. Epidemiol. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agency for Healthcare Research and Quality (AHRQ). Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Publication No. 10(14)-EHC063-EF; AHRQ: Rockville, MD, USA, 2014. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis, 2nd ed.; Springer Publishing Company, Incorporated: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Van der Wal, W.M.; Geskus, R.B. ipw: An R Package for Inverse Probability Weighting. J. Stat. Softw. 2011, 1. [Google Scholar] [CrossRef] [Green Version]
- Pirracchio, R.; Resche-Rigon, M.; Chevret, S. Evaluation of the Propensity score methods for estimating marginal odds ratios in case of small sample size. BMC Med. Res. Methodol. 2012, 12, 70. [Google Scholar] [CrossRef] [PubMed]
- Sahin, C.; Courtney, K.L.; Naylor, P.J.; E Rhodes, R. Tailored mobile text messaging interventions targeting type 2 diabetes self-management: A systematic review and a meta-analysis. Digit. Health 2019, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, S.; Peters, A.L.; Burner, E.; Lam, C.N.; Menchine, M. Trial to examine text message-based mHealth in emergency department patients with diabetes (TExT-MED): A randomized controlled trial. Ann. Emerg. Med. 2014, 63, 745–754.e746. [Google Scholar] [CrossRef] [PubMed]
- Fortmann, A.L.; Gallo, L.C.; Garcia, M.I.; Taleb, M.; Euyoque, J.A.; Clark, T.; Skidmore, J.; Ruiz, M.; Dharkar-Surber, S.; Schultz, J.; et al. Dulce Digital: An mHealth SMS-Based Intervention Improves Glycemic Control in Hispanics with Type 2 Diabetes. Diabetes Care 2017, 40, 1349–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Diabetes Knowledge |
|---|
| Many people need insulin when their blood sugar is high but can stop taking it later–especially if they have lost weight. Diabetes Fact: Glucose, the sugar in your blood, is your main energy source–sort of like the gas in your tank. |
| Motivation |
| Remember, taking care of your diabetes has ups & downs. Don’t focus on one thing. Look at trends over time. Most people sometimes forget to take meds. But taking meds is the MOST important step you can take to stay healthy! |
| Managing Stress Tips |
| Feeling stressed? Sit quietly, close your eyes, breathe deeply, count as you exhale. Do this 10 times & feel the difference! Relax! Take a mini-vacation by sitting quietly, closing your eyes, and just breathing for a minute. |
| Nutritional Facts |
| You can still eat out! Order smaller items from a fast food menu. Even small changes help control diabetes! Shop smart! On a food package nutrition label, look at how many “Servings Per Container” there are. |
| Monitoring Reminders |
| Be a scientist! Check your blood sugar before & after exercise to see how the exercise affects the results. If you check your blood sugar at home, keep a log & show it to your doctor. She will use the info to adjust your medication doses. |
| Taking Medications |
| Don’t miss out on better health. Take your prescribed meds today! Don’t skip your meds! If you have trouble affording prescriptions, there may be cheaper options. Talk to your doctor. |
| Managing Complications |
| Reminder: Getting your eyes checked every 1 to 2 years can reduce the risk of blindness! Check your feet every day. Let your health care provider know if you develop any sores or ingrown toenails. |
| Characteristic | OASMS Arm n = 34 | Control Arm n = 35 | p-Value |
|---|---|---|---|
| Age, (years), mean (±SD) | 53.3 (11.8) | 61 (13) | 0.012 |
| Male, n (%) | 14 (41.2) | 19 (54.3) | 0.396 |
| Ethnicity, n (%) | 0.007 | ||
| White | 18 (52.9) | 27 (77.1) | |
| African American | 0 (0) | 3 (8.6) | |
| Native American | 1 (2.9) | 0 (0) | |
| Hispanic | 13 (38.2) | 5 (14.3) | |
| Other/unknown | 2 (5.9) | 0 (0) | |
| Employment, n (%) | 0.581 | ||
| Employed | 5 (14.7) | 2 (5.7) | |
| Non-employed | 10 (29.4) | 12 (34.3) | |
| Disabled | 1 (2.9) | 0 (0) | |
| Retired | 5 (14.7) | 8 (22.9) | |
| Unknown | 13 (38.2) | 13 (37.1) | |
| Preferred language, n (%) | |||
| English | 34 (100) | 33 (97.1) | 1.000 |
| Insurance, n (%) | 0.256 | ||
| Medicare | 7 (20.6) | 8 (22.9) | |
| Medicaid | 11 (32.4) | 17 (48.6) | |
| Commercial | 16 (47.1) | 10 (28.6) | |
| Duration of diabetes, years, mean (±SD) | 14.2 (10.8) | 16.3 (12) | 0.445 |
| Diabetes regimen, n (%) | 0.479 | ||
| Insulin only | 6 (17.6) | 7 (20) | |
| Non-insulin therapy | 9 (26.5) | 6 (17.1) | |
| Insulin combined with non-insulin therapy | 18 (52.9) | 17 (48.6) | |
| Insulin pump | 1 (2.9) | 4 (11.4) | |
| No medications | 0 (0) | 5 (2.9) | |
| Charlson comorbidity score, mean (±SD) | 3 (1.7) | 3.8 (2.1) | 0.633 |
| HbA1c %, mean (±SD) | 10.2 (1.9) | 9.9 (1.7) | 0.673 |
| Systolic blood pressure, mm Hg, mean (±SD) | 136.8 (13) | 134.2 (15.5) | 0.454 |
| Diastolic blood pressure, mm Hg, mean (±SD) | 81 (12.4) | 75.6 (11.6) | 0.059 |
| Weight, Kg, mean (±SD) | 102.4 (26.7) | 99.1 (32.9) | 0.673 |
| Body mass index (BMI), kg/m2, mean (±SD) | 38.6 (15.2) | 34.2 (9.8) | 0.162 |
| Variable | OASMS Arm n = 34 | Control Arm n = 35 |
|---|---|---|
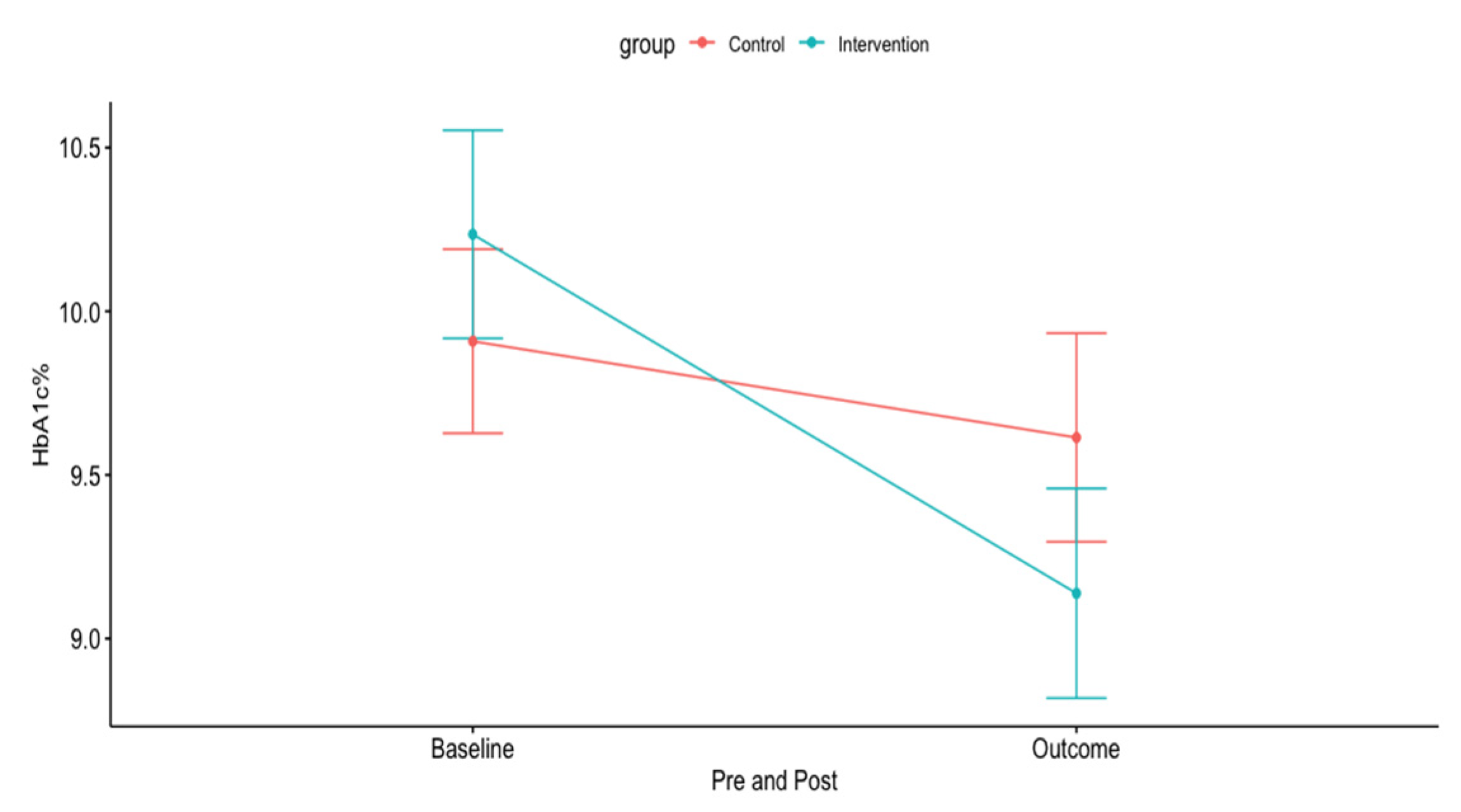
| HbA1c % outcome, crude mean (±SD) | 9.14 (1.87) | 9.61 (1.89) |
| HbA1c %, outcome adjusted means (95% CI) † | 8.89 (8.36 to 9.42) | 9.85 (9.33 to 10.37) |
| HbA1c %, crude mean reduction from baseline (95% CI) | −1.1 (−1.8 to –0.4) | −0.3 (0.7 to 0.1) |
| HbA1c %, adjusted mean reduction from baseline (95% CI) † | −1.17 (−1.71 to −0.64) | −0.21 (−0.73 to 0.31) |
| Characteristic | Estimate (95% CI) | p-Value |
|---|---|---|
| Intercept | 7.411 (4.058–10.763) | <0.001 |
| Age (years) | −0.042 (−0.073 to −0.011) | <0.001 |
| HbA1c at baseline | −0.517 (−0.738 to −0.295) | <0.001 |
| OASMS Intervention | −0.965 (−1.729 to −0.200) | 0.014 |
| Variable | OASMS Arm n = 34 | Control Arm n = 35 | p-Value |
|---|---|---|---|
| Number of clinic visits, median (IQR) | 3 (1–3) | 3 (2.5–4) | 0.011 |
| Text received, median (IQR) | 57.50 (36–78) | - | NA |
| Opted out of service, N (%) | 2 (5.9) | - | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alamer, A.; Palm, C.; Almulhim, A.S.; Te, C.; Pendergrass, M.L.; Fazel, M.T. Impact of Non-Tailored One-Way Automated Short Messaging Service (OASMS) on Glycemic Control in Type 2 Diabetes: A Retrospective Feasibility Study. Int. J. Environ. Res. Public Health 2020, 17, 7590. https://doi.org/10.3390/ijerph17207590
Alamer A, Palm C, Almulhim AS, Te C, Pendergrass ML, Fazel MT. Impact of Non-Tailored One-Way Automated Short Messaging Service (OASMS) on Glycemic Control in Type 2 Diabetes: A Retrospective Feasibility Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7590. https://doi.org/10.3390/ijerph17207590
Chicago/Turabian StyleAlamer, Ahmad, Charles Palm, Abdulaziz S. Almulhim, Charisse Te, Merri L. Pendergrass, and Maryam T. Fazel. 2020. "Impact of Non-Tailored One-Way Automated Short Messaging Service (OASMS) on Glycemic Control in Type 2 Diabetes: A Retrospective Feasibility Study" International Journal of Environmental Research and Public Health 17, no. 20: 7590. https://doi.org/10.3390/ijerph17207590
APA StyleAlamer, A., Palm, C., Almulhim, A. S., Te, C., Pendergrass, M. L., & Fazel, M. T. (2020). Impact of Non-Tailored One-Way Automated Short Messaging Service (OASMS) on Glycemic Control in Type 2 Diabetes: A Retrospective Feasibility Study. International Journal of Environmental Research and Public Health, 17(20), 7590. https://doi.org/10.3390/ijerph17207590