Roma Health: An Overview of Communicable Diseases in Eastern and Central Europe



Abstract
:1. Introduction
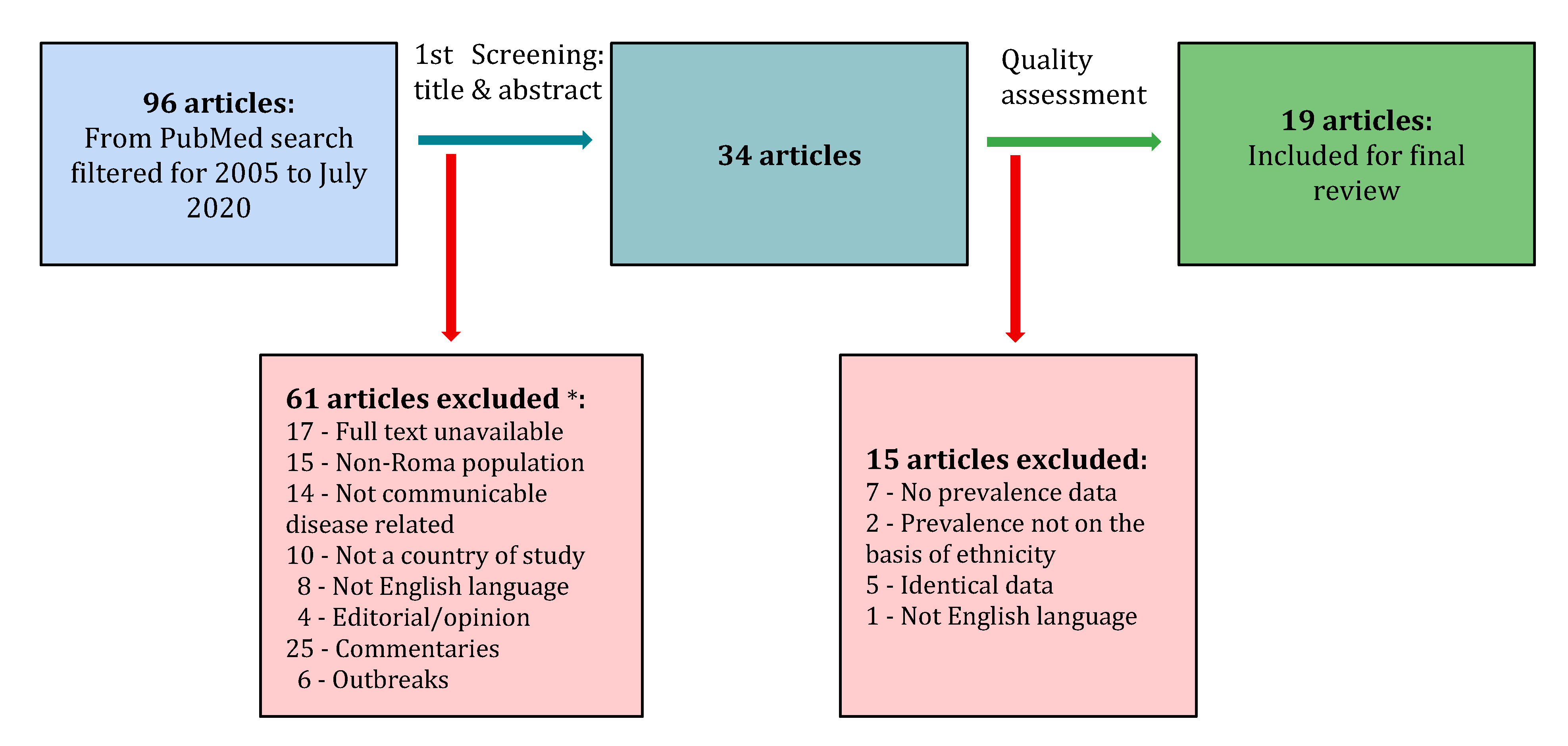
2. Methods
2.1. Sample
2.2. Reporting
3. Results
3.1. Viral Disease
3.2. Parasitic Disease
3.3. Bacterial Disease
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mendizabal, I.; Lao, O.; Marigorta, U.M.; Wollstein, A.; Gusmão, L.; Ferak, V.; Ioana, M.; Jordanova, A.; Kaneva, R.; Kouvatsi, A.; et al. Reconstructing the population history of European Romani from genome-wide data. Curr. Biol. 2012, 22, 2342–2349. [Google Scholar] [CrossRef] [Green Version]
- Font-Porterias, N.; Arauna, L.R.; Poveda, A.; Bianco, E.; Rebato, E.; Prata, M.J.; Calafell, F.; Comas, D. European Roma groups show complex west Eurasian admixture footprints and a common South Asian genetic origin. PLoS Genet. 2019, 15, e1008417. [Google Scholar] [CrossRef]
- Necula, C. The cost of Roma slavery. Perspect. Politice 2012, 5, 33–45. [Google Scholar]
- Cressy, D. Trouble with Gypsies in early modern England. Hist. J. 2015, 59, 45–70. [Google Scholar] [CrossRef] [Green Version]
- Roma Holocaust Remembrance Has Lessons for Europe Today. European Union Agency for Fundamental Rights. 2020. Available online: https://fra.europa.eu/en/news/2020/roma-holocaust-remembrance-has-lessons-europe-today (accessed on 25 July 2020).
- Holt, E. Roma women reveal that forced sterilisation remains. Lancet 2005, 365, 927–928. [Google Scholar] [CrossRef]
- Boffey, D. Policing of European Covid-19 Lockdowns Shows Racial Bias–Report. The Guardian. Available online: https://www.theguardian.com/world/2020/jun/24/policing-of-european-covid-19-lockdowns-shows-racial-bias-report (accessed on 25 July 2020).
- The Situation of Roma in 11 EU Member States; Publications Office of the European Union: Luxembourg, 2012.
- Roma Data. UNDP in Europe and Central Asia. 2020. Available online: https://www.eurasia.undp.org/content/rbec/en/home/ourwork/sustainable-development/development-planning-and-inclusive-sustainable-growth/roma-in-central-and-southeast-europe/roma-data.html (accessed on 25 July 2020).
- Duval, L.; Wolff, F.; McKee, M.; Roberts, B. The Roma vaccination gap: Evidence from twelve countries in Central and South-East Europe. Vaccine 2016, 34, 5524–5530. [Google Scholar] [CrossRef]
- Jarcuska, P.; Team, H.-M.; Bobakova, D.; Uhrin, J.; Bobák, L.; Babinska, I.; Kolarcik, P.; Veselska, Z.; Gecková, A.M.; Veselska, Z. Are barriers in accessing health services in the Roma population associated with worse health status among Roma? Int. J. Public Health 2013, 58, 427–434. [Google Scholar] [CrossRef] [Green Version]
- Rechel, B.; Blackburn, C.; Spencer, N.; Rechel, B. Access to health care for Roma children in Central and Eastern Europe: Findings from a qualitative study in Bulgaria. Int. J. Equity Health 2009, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Roma Integration 2020|Roma Decade. Rcc.int. 2020. Available online: https://www.rcc.int/romaintegration2020/romadecade (accessed on 25 July 2020).
- Communicable Diseases. Euro.who.int. 2020. Available online: https://www.euro.who.int/en/health-topics/communicable-diseases (accessed on 3 June 2020).
- Joanna Briggs Institute-Checklist for Prevalence Studies. Joannabriggs.org. 2017. Available online: https://joannabriggs.org/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf (accessed on 18 June 2020).
- Cocu, M.; Thorne, C.; Matuşa, R.; Tica, V.; Florea, C.; Asandi, S.; Giaquinto, C. Mother-to-child transmission of HIV infection in Romania: Results from an education and prevention programme. AIDS Care 2005, 17, 76–84. [Google Scholar] [CrossRef]
- Kabakchieva, E.; Vassileva, S.; Kelly, J.A.; Amirkhanian, Y.A.; DiFranceisco, W.; McAuliffe, T.L.; Antonova, R.; Mihaylova, M.; Vassilev, B.; Khoursine, R.; et al. HIV risk behavior patterns, predictors, and sexually transmitted disease prevalence in the social networks of young Roma (Gypsy) men in Sofia, Bulgaria. Sex. Transm. Dis. 2006, 33, 485–490. [Google Scholar] [CrossRef]
- Gyarmathy, V.; Ujhelyi, E.; Neaigus, A. HIV and selected blood-borne and sexually transmitted infections in a predominantly Roma (Gypsy) neighbourhood in Budapest, Hungary: A rapid assessment. Cent. Eur. J. Public Health 2008, 16, 124–127. [Google Scholar] [CrossRef]
- Gyarmathy, V.; Neaigus, A.; Ujhelyi, E. Vulnerability to drug-related infections and co-infections among injecting drug users in Budapest, Hungary. Eur. J. Public Health 2009, 19, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Amirkhanian, Y.A.; Kelly, J.A.; Kabakchieva, E.; Antonova, R.; Vassileva, S.; DiFranceisco, W.J.; McAuliffe, T.L.; Vassilev, B.; Petrova, E.; Khoursine, R.A. High-risk sexual behavior, HIV/STD prevalence, and risk predictors in the social networks of young Roma (Gypsy) men in Bulgaria. J. Immigr. Minor. Health 2012, 15, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Halánová, M.; Valenčáková, A.; Malcekova, B.; Kváč, M.; Sak, B.; Květoňová, D.; Bálent, P.; Čisláková, L. Occurrence of microsporidia as emerging pathogens in Slovak Roma children and their impact on public health. Ann. Agric. Environ. Med. 2013, 20, 695–698. [Google Scholar]
- Veselíny, E.; Janičko, M.; Dražilová, S.; Siegfried, L.; Pastvová, L.; Schréter, I.; Kristian, P.; Virág, L.; Jarčuška, P.; Valková, I.; et al. High hepatitis B and low hepatitis C prevalence in Roma population in Eastern Slovakia. Cent. Eur. J. Public Health 2014, 22, S51–S56. [Google Scholar] [CrossRef] [Green Version]
- Halánová, M.; Jarčuška, P.; Kalinová, Z.; Cáriková, K.; Oravcová, J.; Jarčuška, P.; Pella, D.; Mareková, M.; Gecková, A.M.; Čisláková, L. The prevalence of chlamydia trachomatis in the population living in Roma settlements: A comparison with the majority population. Cent. Eur. J. Public Health 2014, 22, S32–S36. [Google Scholar] [CrossRef]
- Djurovic, D.; Prcic, S.; Milojkovic, M.; Konstantinidis, G.; Tamburlini, G. The health status of Roma children-a medical or social issue. Eur. Rev. Med Pharmacol. Sci. 2014, 18, 1218–1223. [Google Scholar]
- Hasajová, A.; Valenčáková, A.; Malčeková, B.; Danišová, O.; Halán, M.; Goldová, M.; Sak, B.; Kvetonova, D.; Kvac, M.; Halánová, M. Significantly higher occurrence of Cryptosporidium infection in Roma children compared with non-Roma children in Slovakia. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1401–1406. [Google Scholar] [CrossRef]
- Antolová, D.; Jarcuska, P.; Janicko, M.; Gecková, A.M.; Halánová, M.; Čisláková, L.; Kalinová, Z.; Reiterová, K.; Škutová, M.; Pella, D.; et al. Seroprevalence of human Toxocara infections in the Roma and non-Roma populations of Eastern Slovakia: A cross-sectional study. Epidemiol. Infect. 2015, 143, 2249–2258. [Google Scholar] [CrossRef] [Green Version]
- Pipiková, J.; Papajová, I.; Šoltys, J.; Schusterová, I. Occurrence of the most common helminth infections among children in the Eastern Slovak Republic. Public Health 2017, 150, 71–76. [Google Scholar] [CrossRef]
- Štrkolcová, G.; Goldová, M.; Bocková, E.; Mojžišová, J. The roundworm Strongyloides stercoralis in children, dogs, and soil inside and outside a segregated settlement in Eastern Slovakia: Frequent but hardly detectable parasite. Parasitol. Res. 2017, 116, 891–900. [Google Scholar] [CrossRef]
- Antolová, D.; Halánová, M.; Janicko, M.; Jarcuska, P.; Reiterová, K.; Jarošová, J.; Gecková, A.M.; Pella, D.; Drazilova, S.; Team, H. A community-based study to estimate the seroprevalence of trichinellosis and echinococcosis in the Roma and non-Roma population of Slovakia. Int. J. Environ. Res. Public Health 2018, 15, 251. [Google Scholar] [CrossRef] [Green Version]
- Antolová, D.; Janicko, M.; Halánová, M.; Jarcuska, P.; Geckova, A.M.; Babinská, I.; Kalinová, Z.; Pella, D.; Mareková, M.; Veselíny, E.; et al. Exposure to toxoplasma gondii in the Roma and non-Roma inhabitants of Slovakia: A cross-sectional seroprevalence study. Int. J. Environ. Res. Public Health 2018, 15, 408. [Google Scholar] [CrossRef] [Green Version]
- Halánová, M.; Veselíny, E.; Kalinová, Z.; Jarcuska, P.; Janicko, M.; Urbančíková, I.; Pella, D.; Drazilova, S.; Babinská, I.; Geckova, A.M. Seroprevalence of hepatitis E virus in Roma settlements: A comparison with the general population in Slovakia. Int. J. Environ. Res. Public Health 2018, 15, 904. [Google Scholar] [CrossRef] [Green Version]
- Ilisiu, M.; Hashim, D.; Andreassen, T.; Støer, N.; Nicula, F.; Weiderpass, E. HPV testing for cervical cancer in Romania: High-Risk hpv prevalence among ethnic subpopulations and regions. Ann. Glob. Health 2019, 85, 89. [Google Scholar] [CrossRef] [Green Version]
- Fecková, M.; Antolová, D.; Janičko, M.; Monika, H.; Štrkolcová, G.; Goldová, M.; Weissová, T.; Lukáč, B.; Nováková, M. The cross-sectional study of Toxoplasma gondii seroprevalence in selected groups of population in Slovakia. Folia Microbiol. 2020, 65, 871–877. [Google Scholar] [CrossRef]
- Fecková, M.; Antolová, D.; Zaleśny, G.; Halánová, M.; Štrkolcová, G.; Goldová, M.; Weissová, T.; Lukáč, B.; Nováková, M. Seroepidemiology of human toxocariasis in selected population groups in Slovakia: A cross-sectional study. J. Infect. Public Health 2020, 13, 1107–1111. [Google Scholar] [CrossRef]
- Simon, P. Collecting ethnic statistics in Europe: A review. Ethn. Racial Stud. 2012, 35, 1366–1391. [Google Scholar] [CrossRef]
- Masseria, C.; Mladovsky, P.; Hernández-Quevedo, C. The socio-economic determinants of the health status of Roma in comparison with non-Roma in Bulgaria, Hungary and Romania. Eur. J. Public Health 2010, 20, 549–554. [Google Scholar] [CrossRef] [Green Version]
- Godefroy, R.; Chaud, P.; Ninove, L.; Dina, J.; Decoppet, A.; Casha, P.; Hraiech, S.; Brouqui, P.; Cassir, N.; Julia, D. Measles outbreak in a French Roma community in the Provence-Alpes-Côte d’Azur region, France, May to July 2017. Int. J. Infect. Dis. 2018, 76, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Georgakopoulou, T.; Horefti, E.; Vernardaki, A.; Pogka, V.; Gkolfinopoulou, K.; Triantafyllou, E.; Tsiodras, S.; Theodoridou, M.; Mentis, A.; Panagiotopoulos, T. Ongoing measles outbreak in Greece related to the recent European-wide epidemic. Epidemiol. Infect. 2018, 146, 1692–1698. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| First Author | Pub. Year | Country of Study | Quality Score 9-Point Scale * | Total Sample Size | No. of Roma within the Sample | Target Group |
|---|---|---|---|---|---|---|
| Cocu M [16] | 2005 | RO | 7 | 11423 | 862 | Pregnant women |
| Kabakchieva E [17] | 2006 | BG | 8 | 296 | 296 | Young Roma men |
| Gyarmathy VA [18] | 2008 | HU | 6 | 64 | 50 | Convenience sample of volunteers |
| Gyarmathy VA [19] | 2009 | HU | 7 | 186 | 42 | Injecting Drug Users |
| Amirkhanian YA [20] | 2013 | BG | 8 | 405 | 405 | Young Roma men |
| Halánová M [21] | 2013 | SK | 5 | 72 | 72 | Roma children 0–14 years |
| Veselíny E [22] | 2014 | SK | 7 | 855 | 441 | HepaMeta subpopulation + |
| Halánová M [23] | 2014 | SK | 6 | 340 | 208 | HepaMeta subpopulation |
| Djurovic D [24] | 2014 | SRB | 3 | 118 | 59 | Hospitalised children 1–2 years |
| Hasajová A [25] | 2014 | SK | 6 | 103 | 53 | Children 0-14 |
| Antolová D [26] | 2015 | SK | 7 | 823 | 429 | HepaMeta subpopulation |
| Pipiková J [27] | 2017 | SK | 6 | 426 | 275 | Children |
| Štrkolcová G [28] | 2017 | SK | 5 | 81 | 60 | Children 0–17 |
| Antolová D [29] | 2018 | SK | 7 | 823 | 429 | HepaMeta subpopulation |
| Antolová D [30] | 2018 | SK | 7 | 806 | 420 | HepaMeta subpopulation |
| Halánová M [31] | 2018 | SK | 7 | 264 | 195 | HepaMeta subpopulation |
| Ilisiu MB [32] | 2019 | RO | 8 | 2060 | 124 | Women 18–68 |
| Fecková M [33] | 2020 | SK | 6 | 1536 | 67 | Children |
| Fecková M [34] | 2020 | SK | 6 | 1489 | 67 | Children |
| First Author | Pub. Year | Country | No. of Roma | Target Group | HIV | HSV * | Any Hepatitis ** | HAV | HBV | HCV | HEV | HPV |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cocu M | 2005 | RO | 862 | Pregnant women | 0.6 | |||||||
| (0.1) | ||||||||||||
| Gyarmathy VA | 2008 | HU | 50 | Convenience sample of volunteers | 0.0 | 80.0 | 26.0 | 26.0 | ||||
| (0.0) | (42.9) | (28.6) | (14.3) | |||||||||
| Gyarmathy VA | 2009 | HU | 42 | Injecting Drug Users | 0.0 | 100.0 | 71.3 | |||||
| (0.0) | (56.5) | (45.1) | ||||||||||
| Amirkhanian YA | 2013 | BG | 405 | Young Roma men | 0.5 | |||||||
| Veselíny E | 2014 | SK | 441 | HepaMeta subpopulation | 52.8 | 0.7 | ||||||
| Halánová M | 2018 | SK | 195 | HepaMeta subpopulation | 21.5 | |||||||
| (7.2) | ||||||||||||
| Ilisiu MB | 2019 | RO | 124 | Women 18-68 | 6.5 | |||||||
| (15.5) |
| First Author | Pub. Year | Country | No. of Roma | Target Group | Trichomonas | Microsporidia | P. h. Capitis and Scabies | Cryptosporidium | Toxocara | Helminths | T. Gondii |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kabakchieva E | 2006 | BG | 296 | Young Roma men | 8.7 | ||||||
| Halánová M | 2013 | SK | 72 | Roma children 0–14 years | 30.6 | ||||||
| Djurovic D | 2014 | SRB | 59 | Hospitalised children 1–2 years | 10.0 | ||||||
| (0.0) | |||||||||||
| Hasajová A | 2014 | SK | 53 | Children 0–14 | 11.3 | ||||||
| (0.0) | |||||||||||
| Antolová D | 2015 | SK | 429 | HepaMeta subpopulation | 22.1 | ||||||
| (1.0) | |||||||||||
| Pipiková J | 2017 | SK | 275 | Children | 25.8 | ||||||
| (0.7) | |||||||||||
| Štrkolcová G | 2017 | SK | 60 | Children 0–17 | 85.0 | ||||||
| (23.8) | |||||||||||
| Antolová D | 2018 | SK | 429 | HepaMeta subpopulation | * see table footer | ||||||
| Antolová D | 2018 | SK | 420 | HepaMeta subpopulation | 45.0 | ||||||
| (24.1) | |||||||||||
| Fecková M | 2020 | SK | 67 | Children | 20.9 | ||||||
| (7.1) | |||||||||||
| Fecková M | 2020 | SK | 67 | Children | 40.3 | ||||||
| (2.3) |
| First Author | Pub. Year | Country | No. of Roma | Target Group | Chlamydia | Gonorrhoea | Syphilis |
|---|---|---|---|---|---|---|---|
| Kabakchieva E | 2006 | BG | 296 | Young Roma men | 8.0 | 4.5 | 3.5 |
| Gyarmathy VA | 2008 | HU | 50 | Convenience sample of volunteers | 1.8 | ||
| (0.0) | |||||||
| Gyarmathy VA | 2009 | HU | 42 | Injecting Drug Users | * see table footer | 0.0 | * see table footer |
| Amirkhanian YA | 2013 | BG | 405 | Young Roma men | 5.2 | 3.7 | 0.0 |
| Halánová M | 2014 | SK | 208 | HepaMeta subpopulation | 7.2 | ||
| (5.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tombat, K.; van Dijk, J.P. Roma Health: An Overview of Communicable Diseases in Eastern and Central Europe. Int. J. Environ. Res. Public Health 2020, 17, 7632. https://doi.org/10.3390/ijerph17207632
Tombat K, van Dijk JP. Roma Health: An Overview of Communicable Diseases in Eastern and Central Europe. International Journal of Environmental Research and Public Health. 2020; 17(20):7632. https://doi.org/10.3390/ijerph17207632
Chicago/Turabian StyleTombat, Kabir, and Jitse P. van Dijk. 2020. "Roma Health: An Overview of Communicable Diseases in Eastern and Central Europe" International Journal of Environmental Research and Public Health 17, no. 20: 7632. https://doi.org/10.3390/ijerph17207632
APA StyleTombat, K., & van Dijk, J. P. (2020). Roma Health: An Overview of Communicable Diseases in Eastern and Central Europe. International Journal of Environmental Research and Public Health, 17(20), 7632. https://doi.org/10.3390/ijerph17207632