Effects of an Activity Tracker and App Intervention to Increase Physical Activity in Whole Families—The Step It Up Family Feasibility Study

 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
Objective
2. Methods
2.1. Study Design
2.2. Participants
2.3. The Step It Up Family Intervention
2.4. Procedures
2.5. Measures
2.5.1. Process Measures
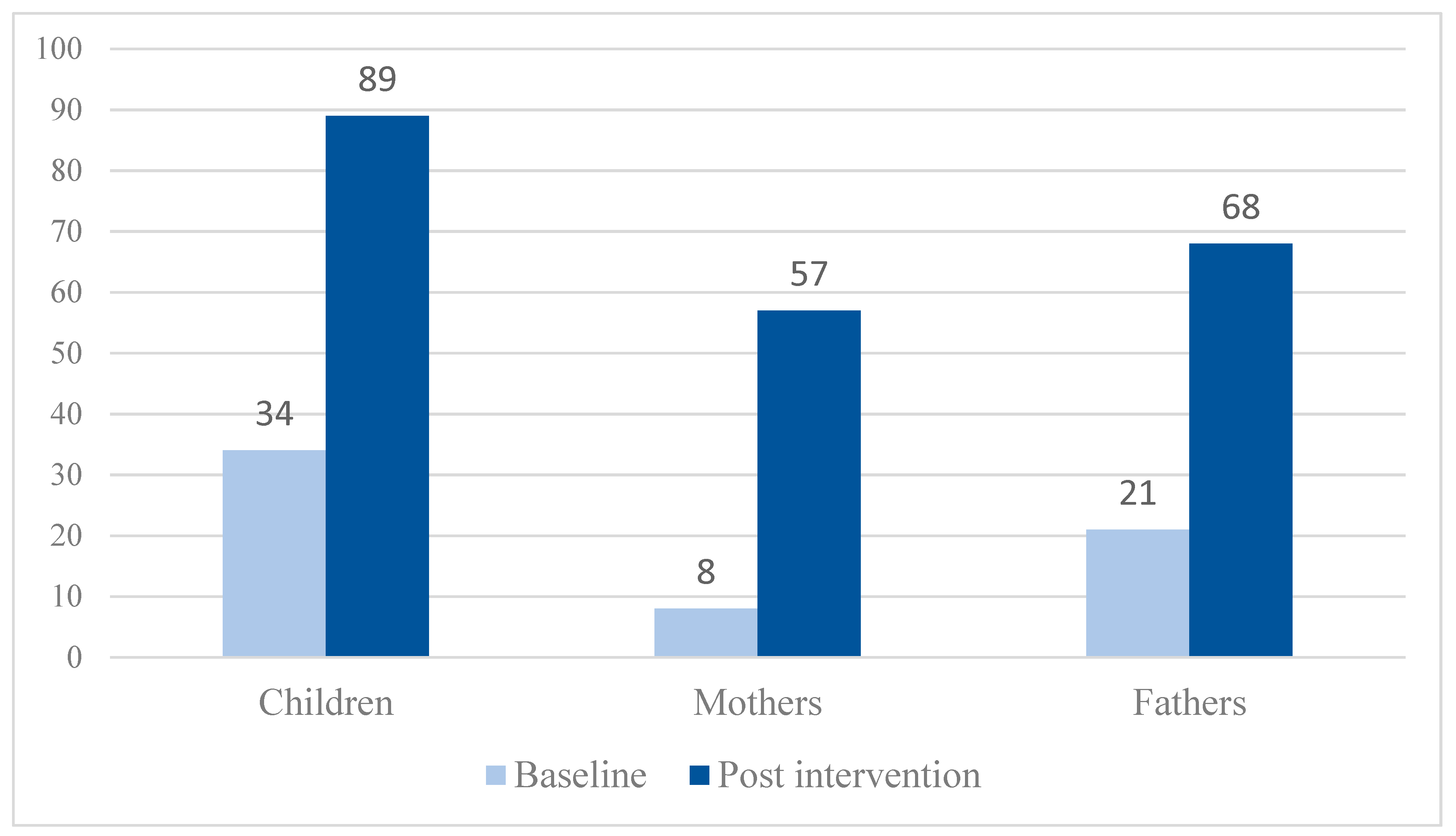
2.5.2. Parent-Reported Physical Activity in Children Pre vs. Post Intervention
2.5.3. Self-Reported Physical Activity in Mothers and Fathers Pre vs. Post Intervention
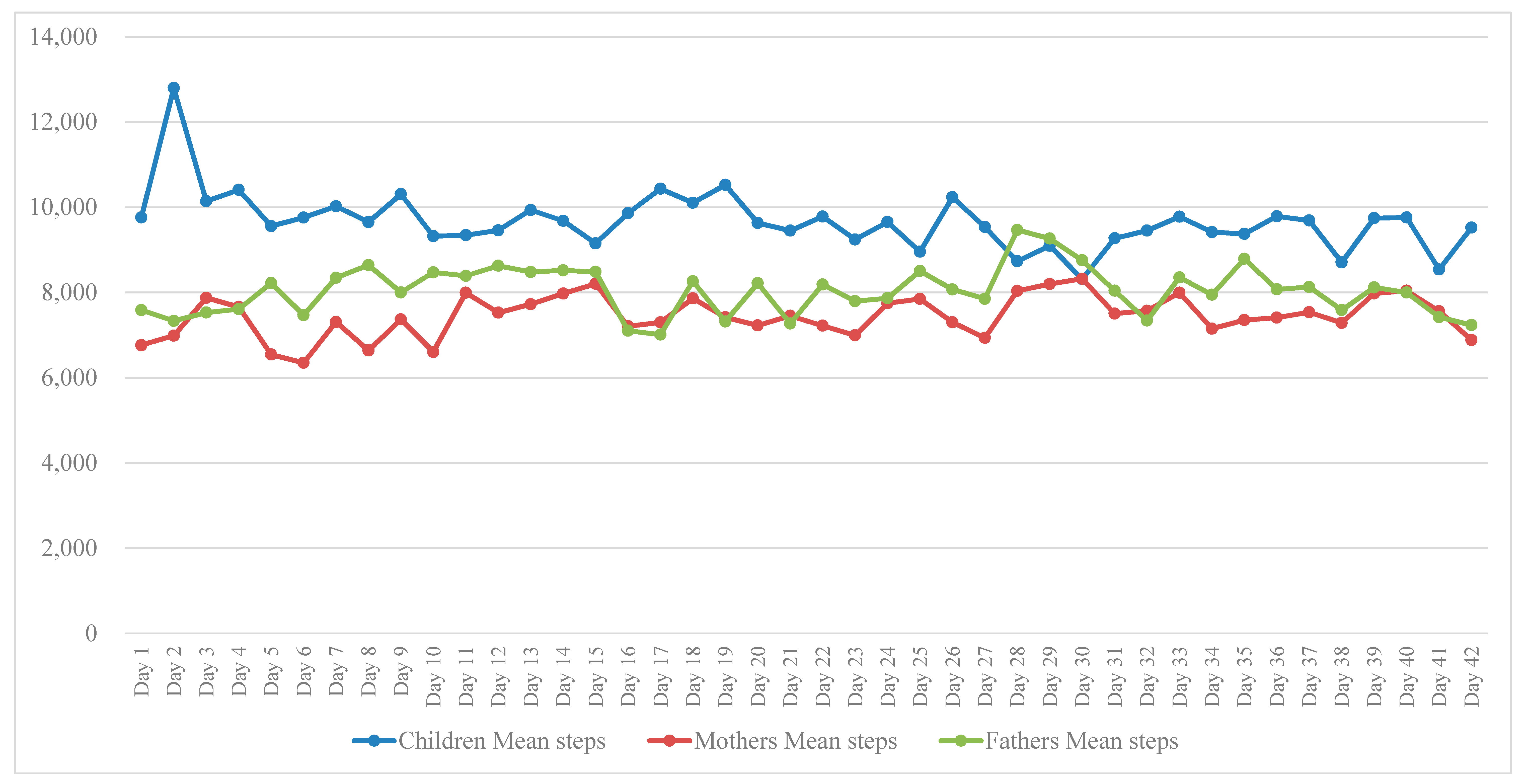
2.5.4. Objective Physical Activity in Children, Mothers and Fathers During the Intervention
2.6. Sample Size
2.7. Statistical Analyses
3. Results
3.1. Recruitment, Participation and Retention
3.2. Baseline Data
3.3. Delivery and Fidelity of the Intervention
3.4. Pre-Post Intervention Effects in Children, Mothers and Fathers
3.5. Pre-Post Intervention Effects at the Family Level
3.6. Physical Activity Levels in Children, Mothers and Fathers during the Intervention
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations for Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Active Healthy Kids Australia. The 2016 Report Card on Physical Activity for Children and Young People. 2016. Available online: https://www.activehealthykidsaustralia.com.au/report-cards/ (accessed on 11 December 2019).
- Australian Bureau of Statistics. Insufficient Physical Activity, 2017/18; Cat. No. PHE 248; Commonwealth of Australia: Canberra, Australia, 2019.
- Australian Government, Department of Health. Overweight and Obesity. 2019. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/Overweight-and-Obesity (accessed on 11 December 2019).
- Brown, W.J.; Bauman, A.E.; Bull, F.C.; Burton, N.W. Development of Evidence-Based Physical Activity Recommendations for Adults (18–64 Years). 2012. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/content/F01F92328EDADA5BCA257BF0001E720D/$File/DEB-PAR-Adults-18–64years.pdf (accessed on 11 December 2019).
- Medibank. The Cost of Physical Inactivity. 2008. Available online: http://www.medibank.com.au/Client/Documents/Pdfs/pyhsical_inactivity.pdf (accessed on 11 December 2019).
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeppe, S.; Trost, S.G. Maternal and paternal support for physical activity and healthy eating in preschool children: A cross-sectional study. BMC Public Health 2015, 15, 971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeppe, S.; Liersch, S.; Röbl, M.; Krauth, C.; Walter, U. Mothers and fathers both matter: The positive influence of parental physical activity modeling on children’s leisure-time physical activity. Pediatr. Exerc. Sci. 2016, 28, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Vandelanotte, C.; Bere, E.; Lien, N.; Manios, Y.; Bjelland, M.; Vik, F.N.; Van Lippevelde, W.; Verloigne, M.; Kovács, É. The influence of parental modelling on children’s physical activity and screen time: Does it differ by gender? Eur. J. Public Health 2017, 27, 152–157. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D. Parental influences on physical activity behavior in children and adolescents: A brief review. Am. J. Lifestyle Med. 2011, 5, 171–181. [Google Scholar] [CrossRef]
- Davison, K.K.; Kitos, N.; Aftosmes-Tobio, A.; Ash, T.; Agaronov, A.; Sepulveda, M.; Haines, J. The forgotten parent: Fathers’ representation in family interventions to prevent childhood obesity. Prev. Med. 2018, 111, 170–176. [Google Scholar] [CrossRef]
- Klein, D. Electronic activity trackers encourage family fun and fitness. Australas Med. 2015, 8, 216–218. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Barnes, A.T.; Eather, N.; Pollock, E.R.; Lubans, D.R. Engaging fathers to increase physical activity in girls: The “Dads And Daughters Exercising and Empowered” (DADEE) randomized controlled trial. Ann. Behav. Med. 2019, 53, 39–52. [Google Scholar] [CrossRef]
- Salmon, J.; Ridgers, N.; Morgan, P.; Okely, T.; Lubans, D.; Hesketh, K.; Hinkley, T.; Dunstan, D.; Giles-Corti, B. Action area 9: Children and young people. In Blueprint for an Active Australia; National Heart Foundation of Australia, 2014; Available online: heartfoundation.org.au/images/uploads/publications/Blueprint/Blueprint_Children_and_young_people.pdf (accessed on 11 December 2019).
- Ridgers, N.D.; Timperio, A.; Brown, H.; Ball, K.; Macfarlane, S.; Lai, S.K.; Richards, K.; Mackintosh, K.A.; McNarry, M.A.; Foster, M.; et al. Wearable activity tracker use among Australian adolescents: Usability and acceptability study. JMIR mHealth uHealth 2018, 6, e86. [Google Scholar] [CrossRef]
- Salmon, J.; Ridgers, N.D. Is wearable technology an activity motivator, or a fad that wears thin? Med. J. Aust. 2017, 206, 119–120. [Google Scholar] [CrossRef]
- Alley, S.; Schoeppe, S.; Guertler, D.; Jennings, C.; Duncan, M.J.; Vandelanotte, C. Interest and preferences for using advanced physical activity tracking devices: Results of a national cross-sectional survey. BMJ Open 2016, 6, e011243. [Google Scholar] [CrossRef] [Green Version]
- Australian Communications and Media Authority. Communications Report 2017–2018. 2019. Available online: https://www.acma.gov.au/sites/default/files/2019-08/Communications%20report%202017-18.pdf (accessed on 11 December 2019).
- Statista. Users of Wearables in Australia. 2019. Available online: https://www.statista.com/outlook/319/107/wearables/australia#market-users (accessed on 11 December 2019).
- Pricewaterhouse Coopers. The Wearable Life 2.0. Connected Living in a Wearable World. 2016. Available online: https://www.pwc.se/sv/pdf-reports/the-wearable-life-2-0.pdf (accessed on 11 December 2019).
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [Green Version]
- Brickwood, K.J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-based wearable activity trackers increase physical activity participation: Systematic review and meta-analysis. JMIR mHealth uHealth 2019, 12, e11819. [Google Scholar] [CrossRef]
- Gal, R.; May, A.M.; van Overmeeren, E.J.; Simons, M.; Monninkhof, E.M. The effect of physical activity interventions comprising wearables and smartphone applications on physical activity: A systematic review and meta-analysis. Sports Med. Open 2018, 4, 42. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Lloyd, A.B.; Wang, M.L.; Eather, N.; Miller, A.; Murtagh, E.M.; Barnes, A.T.; Pagoto, S.L. Involvement of fathers in pediatric obesity treatment and prevention trials: A systematic review. Pediatrics 2017, 139, e20162635. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Charles, J.N.; Khandpur, N.; Nelson, T.J. Fathers’ perceived reasons for their underrepresentation in child health research and strategies to increase their involvement. Matern. Child Health J. 2017, 21, 267–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, P.J.; Young, M.D. The influence of fathers on children’s physical activity and dietary behaviors: Insights, recommendations and future directions. Curr. Obes. Rep. 2017, 6, 324–333. [Google Scholar] [CrossRef]
- Morgan, P.J.; Collins, C.E.; Plotnikoff, R.C.; Callister, R.; Burrows, T.; Fletcher, R.; Okely, A.D.; Young, M.D.; Miller, A.; Lloyd, A.B.; et al. The ‘Healthy Dads, Healthy Kids’ community randomized controlled trial: A community-based healthy lifestyle program for fathers and their children. Prev. Med. 2014, 61, 90–99. [Google Scholar] [CrossRef]
- Neshteruk, C.D.; Nezami, B.T.; Nino-Tapias, G.; Davison, K.K.; Ward, D.S. The influence of fathers on children’s physical activity: A review of the literature from 2009 to 2015. Prev. Med. 2017, 102, 12–19. [Google Scholar] [CrossRef]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.M.; van Sluijs, E.M.F. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis and realist synthesis. Obes. Rev. 2016, 17, 345–360. [Google Scholar] [CrossRef] [Green Version]
- Mendonça, G.; Cheng, L.A.; Mélo, E.N.; De Farias Júnior, J.C. Physical activity and social support in adolescents: A systematic review. Health Educ. Res. 2014, 29, 822–839. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.L.; Taylor, N.F.; Shields, N.; Frawley, H.C. Attitudes, barriers and enablers to physical activity in pregnant women: A systematic review. J. Physiother. 2018, 64, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986; ISBN 9780138156145. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. 2008, 49, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Müller, J.; Hoch, A.M.; Zoller, V.; Oberhoffer, R. Feasibility of physical activity assessment with wearable devices in children aged 4–10 years—A pilot study. Front. Pediatr. 2018, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, Y.; Düking, P.; Droszez, A.; Wahl, P.; Mester, J. Criterion-validity of commercially available physical activity tracker to estimate step count, covered distance and energy expenditure during sports conditions. Front. Physiol. 2017, 8, 725. [Google Scholar] [CrossRef] [PubMed]
- Telford, A.; Salmon, J.; Jolley, D.; Crawford, D. Reliability and validity of physical activity questionnaires for children: The children’s leisure activities study survey (CLASS). Pediatr. Exerc. Sci. 2004, 16, 64–78. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. The Active Australia Survey: A Guide for Manual Implimentation, Analysis and Reporting. 2003. Available online: https://www.aihw.gov.au/reports/physical-activity/active-australia-survey/contents/table-of-contents (accessed on 11 December 2019).
- Fjeldsoe, B.S.; Winkler, E.A.H.; Marshall, A.L.; Eakin, E.G.; Reeves, M.M. Active adults recall their physical activity differently to less active adults: Test-retest reliability and validity of a physical activity survey. Health Promot. J. Austr. 2013, 24, 26–31. [Google Scholar] [CrossRef]
- Australian Government, Department of Health. Australia’s Physical Activity and Sedentary Behaviour Guidelines for Adults (18–64 Years). 2014. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/F01F92328EDADA5BCA257BF0001E720D/$File/brochure%20PA%20Guidelines_A5_18-64yrs.pdf (accessed on 11 December 2019).
- Australian Government, Department of Health. Australian 24-Hour Movement Guidelines for Children and Young People (5–17 Years). 2019. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/F01F92328EDADA5BCA257BF0001E720D/$File/brochure-24hr-guidelines-5-17yrs.pdf (accessed on 11 December 2019).
- Sleddens, E.F.C.; Gubbels, J.S.; Kremers, S.P.J.; van der Plas, E.; Thijs, C. Bidirectional associations between activity-related parenting practices, and child physical activity, sedentary screen-based behavior and body mass index: A longitudinal analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 89. [Google Scholar] [CrossRef] [Green Version]
- Van Sluijs, E.M.F.; Kriemler, S.; McMinn, A.M. The effect of community and family interventions on young people’s physical activity levels: A review of reviews and updated systematic review. Br. J. Sports Med. 2011, 45, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Vandelanotte, C.; Stanton, R.; Rebar, A.L.; Van Itallie, A.; Caperchione, C.M.; Duncan, M.J.; Savage, T.N.; Rosenkranz, R.R.; Kolt, G.S. Physical activity screening to recruit inactive randomized controlled trial participants: How much is too much? Trials 2015, 16, 446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, R.A.; Daniels, L.A.; Bell, L.; Magarey, A.M. Facilitators and barriers to the achievement of healthy lifestyle goals: Qualitative findings from Australian parents enrolled in the PEACH child weight management program. J. Nutr. Educ. Behav. 2017, 49, 43–52.e1. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Brown, W.J.; Mummery, W.K.; Vandelanotte, C. 10,000 Steps Australia: A community-wide eHealth physical activity promotion programme. Br. J. Sports Med. 2018, 52, 885–886. [Google Scholar] [CrossRef]
- National Heart Foundation of Australia. Heart Foundation Walking. 2019. Available online: https://walking.heartfoundation.org.au (accessed on 11 December 2019).



{kind=link}
{kind=link}
| Intervention Component | Description | Incorporated Behavior Change Techniques a | Targeted Behavior Change Theory Mediators b |
|---|---|---|---|
| Introductory session | Child and parent activity trackers were set up and the respective apps downloaded on parents’ smartphone/iPad. All intervention components were explained. Children, mothers and fathers were educated on the importance of physical activity for health, were presented with the Australian physical activity guidelines for children and adults and given examples of how to model and support each other to become more physically active. The introductory session was delivered by a project officer either face-to-face (in 65% of families) at Central Queensland University, a public playground or families’ homes or via telephone in families who lived further way (in 35% of families). | Provide instructions Provide information about behavior-health link Prompt identification as role model Plan social support | Goals (SCT) Outcome expectations (SCT) Social support/relatedness (SCT/SDT) Modelling (SCT) |
| Family resources | Garmin Vivofit activity trackers: Children received the Garmin Vivofit Junior activity tracker. Mothers and fathers received the Garmin Vivofit 3 activity tracker for adults. Garmin apps: The Garmin Vivofit Junior app for children and the Garmin Connect app for adults were installed on mothers’ and fathers’ smartphone/iPad. Family step challenge log poster: During the introductory session, families received a family step challenge log poster in A3 poster format together with magnets to stick on the fridge. Children and parents were encouraged to log their daily and weekly individual and family-level steps in the log poster. Informational resources: Families received leaflets including the Australian Physical Activity Guidelines, information and maps of local walking tracks, 50 tips for family-based physical activities. | Goal-setting Set graded tasks Self-monitoring Performance feedback Provide instructions Provide contingent rewards Provide opportunities for social comparison | Goals (SCT) Autonomy (SDT) Self-efficacy/perceived competence (SCT/ SDT) Outcome expectations (SCT) Social support/relatedness (SCT/SDT) |
| Motivational and educational text messages | Motivational and educational text messages were sent 3 times per week to parents’ smartphone to provide families tips for goal-setting and (co-) physical activities. Emphasis was on how children, mothers and fathers can support and model active behaviors. | Provide instructions Prompt intentions formation Set graded tasks Prompt specific goal-setting Prompt practice Provide general encouragement Prompt identification as role model Plan social support | Goals (SCT) Autonomy (SDT) Social support/relatedness (SCT/SDT) Modelling (SCT) |
| Setting individual and family goals | Setting individual and family goals for being more active daily and weekly. Individual: e.g., 10,000 steps per day, active time per day (60 min children, 30 min adults). Family: e.g., 200,000 steps per week, 60 min of family active recreation on weekend days. | Goal-setting | Goals (SCT) Autonomy (SDT) |
| Setting graded achievable goals | Gradually increasing daily and weekly goals for being active. Individual: e.g., 500 more steps/day the next week, increase daily outdoor activity by 5 min. Family: e.g., 20,000 more steps next week, increase weekly family active recreation by 20 min. | Set graded tasks | Goals (SCT) Autonomy (SDT) |
| Self-monitoring | Monitoring step counts and active minutes spent in light, moderate and vigorous physical activity using the activity trackers combined with apps. | Self-monitoring Performance feedback | Autonomy (SDT) Self-efficacy/perceived competence (SCT/ SDT) |
| Family leaderboard | Sharing physical activity levels between children, mother and father via a family leaderboard shown on the app which displayed who had the ‘highest step counts’ and ‘most active minutes.’ | Performance feedback Provide opportunities for social comparison Provide contingent rewards | Social support/relatedness (SCT/SDT) Outcome expectations (SCT) |
| Family step challenges | Families completed daily and weekly family step challenges to energies children, mothers and fathers to support each other and become physical activity role models for each other. Firstly, children, mothers and fathers challenged each other to get the ‘highest step counts’ and ‘most active minutes’ daily and weekly (beat family members’ activity goals). Secondly, families pursued weekly challenges to achieve ‘higher step counts’ and ‘more active minutes’ each week together as a family (reach activity goals together as a family). | Prompt identification as role model Plan social support Model or demonstrate the behavior Provide opportunities for social comparison Provide contingent rewards | Goals (SCT) Autonomy (SDT) Self-efficacy/perceived competence (SCT/ SDT) Outcome expectations (SCT) Social support/relatedness (SCT/SDT) Modelling (SCT) Reinforcement (SCT) |
| Children | All | Girls | Boys | p Value | |
| n (%) | 58 (100.0) | 29 (50.0) | 29 (50.0) | ||
| Age, Mean (SD) | 8.0 (1.5) | 8.1 (1.5) | 7.8 (1.5) | 0.491 | |
| MVPA min/day, Mean (SD) | 56.1 (37.3) | 61.5 (45.6) | 50.6 (25.9) | 0.271 | |
| Meeting physical activity guidelines, n (%) | 19 (33.3) | 10 (34.5) | 9 (32.1) | 0.851 | |
| Parents | All | Mothers | Fathers | p Value | |
| n (%) | 72 | 39 (97.5) | 33 (82.5) | ||
| Age, Mean (SD) | 39.3 (5.4) | 37.8 (4.3) | 41.2 (6.1) | 0.010 | |
| Education, n (%) | 0.217 | ||||
| 13+ years | 30 (76.9) | 51 (70.8) | 21 (63.6) | ||
| 0–12 years | 9 (23.1) | 21 (29.2) | 12 (36.4) | ||
| Work status, n (%) | <0.001 | ||||
| Employed | 29 (74.4) | 59 (81.9) | 30 (90.9) | ||
| Unemployed | 10 (15.6) | 13 (18.1) | 3 (9.1) | ||
| Ethnicity, n (%) | 0.354 | ||||
| Caucasian | 38 (97.4) | 71 (98.6) | 33 (100.0) | ||
| Asian | 1 (2.6) | 1 (1.4) | 0 (0.0) | ||
| MVPA min/day, Mean (SD) | 9.4 (11.7) | 8.6 (9.8) | 10.4 (13.8) | 0.535 | |
| Meeting physical activity guidelines, n (%) | 9 (12.7) | 3 (7.7) | 6 (18.8) | 0.163 | |
| Participants | Participants with Complete Data | Intention-to-Treat | ||||||
|---|---|---|---|---|---|---|---|---|
| n | Pre | Post | Difference a | N | Pre | Post | Difference a | |
| All children | ||||||||
| MVPA min/day, Mean (SD), (95% CI) | 44 | 51.7 (32.8) | 109.5 (56.1) | +57.8 (40.5, 75.0) | 57 b | 56.1 (37.3) | 100.7 (56.3) | +44.6 (29.9, 59.3) |
| Meeting physical activity guidelines, n (%) | 44 | 15 (34.1) | 39 (88.6) | +24 (54.5) | 57 | 19 (33.3) | 43 (75.4) | +24 (42.1) |
| Boys | ||||||||
| MVPA min/day, Mean (SD), (95% CI) | 23 | 49.9 (28.5) | 104.0 (46.8) | +54.0 (33.9, 74.2) | 28 b | 50.6 (25.9) | 95.0 (46.6) | +44.4 (26.2, 62.6) |
| Meeting physical activity guidelines, n (%) | 23 | 8 (34.8) | 21 (91.3) | +13 (56.5) | 28 b | 9 (32.1) | 22 (78.6) | +13 (46.5) |
| Girls | ||||||||
| MVPA min/day, Mean (SD), (95% CI) | 21 | 53.7 (37.6) | 115.5 (65.4) | +61.8 (31.2, 92.5) | 29 | 61.5 (45.6) | 106.3 (64.7) | +44.8 (20.6, 68.9) |
| Meeting physical activity guidelines, n (%) | 21 | 7 (33.3) | 18 (85.7) | +11 (52.4) | 29 | 10 (34.5) | 21 (72.4) | +11 (37.9) |
| All parents | ||||||||
| MVPA min/day, Mean (SD), (95% CI) | 65 | 9.6 (12.1) | 38.3 (33.6) | +28.7 (20.4, 37.1) | 71b | 9.4 (11.7) | 35.7 (33.3) | +26.3 (18.4, 34.1) |
| Meeting physical activity guidelines, n (%) | 65 | 9 (13.8) | 40 (61.5) | +31 (47.7) | 71b | 9 (12.7) | 40 (56.3) | +31 (43.6) |
| Mothers | ||||||||
| MVPA min/day, Mean (SD), (95% CI) | 37 | 8.5 (10.0) | 35.8 (35.6) | +27.3 (15.6, 39.0) | 39 | 8.6 (9.8) | 34.6 (35.1) | +25.9 (14.7, 37.2) |
| Meeting physical activity guidelines, n (%) | 37 | 3 (8.1) | 21 (56.8) | +18 (48.7) | 39 | 3 (7.7) | 21 (53.8) | +18 (46.1) |
| Fathers | ||||||||
| MVPA min/day, Mean (SD), (95% CI) | 28 | 11.0 (14.5) | 41.6 (31.1) | +30.5 (18.0, 43.0) | 32 b | 10.4 (13.8) | 37.1 (31.5) | +26.7 (15.3, 38.2) |
| Meeting physical activity guidelines, n (%) | 28 | 6 (21.4) | 19 (67.9) | +13 (46.5) | 32 b | 6 (18.8) | 19 (59.4) | +13 (40.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoeppe, S.; Salmon, J.; Williams, S.L.; Power, D.; Alley, S.; Rebar, A.L.; Hayman, M.; Duncan, M.J.; Vandelanotte, C. Effects of an Activity Tracker and App Intervention to Increase Physical Activity in Whole Families—The Step It Up Family Feasibility Study. Int. J. Environ. Res. Public Health 2020, 17, 7655. https://doi.org/10.3390/ijerph17207655
Schoeppe S, Salmon J, Williams SL, Power D, Alley S, Rebar AL, Hayman M, Duncan MJ, Vandelanotte C. Effects of an Activity Tracker and App Intervention to Increase Physical Activity in Whole Families—The Step It Up Family Feasibility Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7655. https://doi.org/10.3390/ijerph17207655
Chicago/Turabian StyleSchoeppe, Stephanie, Jo Salmon, Susan L. Williams, Deborah Power, Stephanie Alley, Amanda L. Rebar, Melanie Hayman, Mitch J. Duncan, and Corneel Vandelanotte. 2020. "Effects of an Activity Tracker and App Intervention to Increase Physical Activity in Whole Families—The Step It Up Family Feasibility Study" International Journal of Environmental Research and Public Health 17, no. 20: 7655. https://doi.org/10.3390/ijerph17207655
APA StyleSchoeppe, S., Salmon, J., Williams, S. L., Power, D., Alley, S., Rebar, A. L., Hayman, M., Duncan, M. J., & Vandelanotte, C. (2020). Effects of an Activity Tracker and App Intervention to Increase Physical Activity in Whole Families—The Step It Up Family Feasibility Study. International Journal of Environmental Research and Public Health, 17(20), 7655. https://doi.org/10.3390/ijerph17207655