Visual Status in a Portuguese Population with Intellectual Disability



Abstract
:1. Introduction
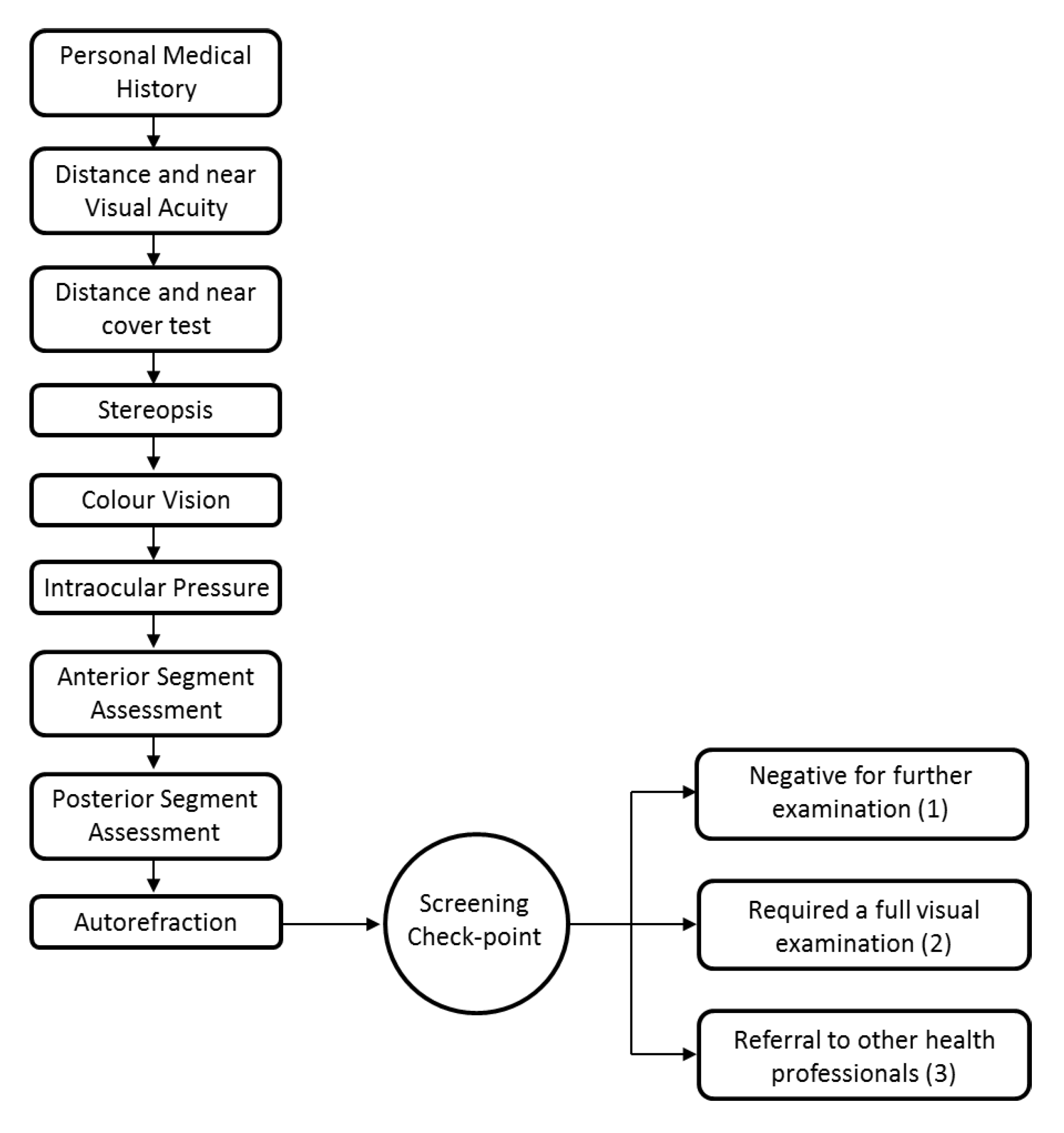
2. Materials and Methods
Data Presentation and Analysis
3. Results
3.1. Number of Athletes
3.2. Demographics
3.3. Success Rate for Testing
3.4. Last Eye Exam and Spectacle Wear
3.5. Symptoms
3.6. Distance and Near Visual Acuity
3.7. Binocular Vision (Cover Test and Stereopsis)
3.8. Colour Vision
3.9. Intraocular Pressure
3.10. Ocular Health
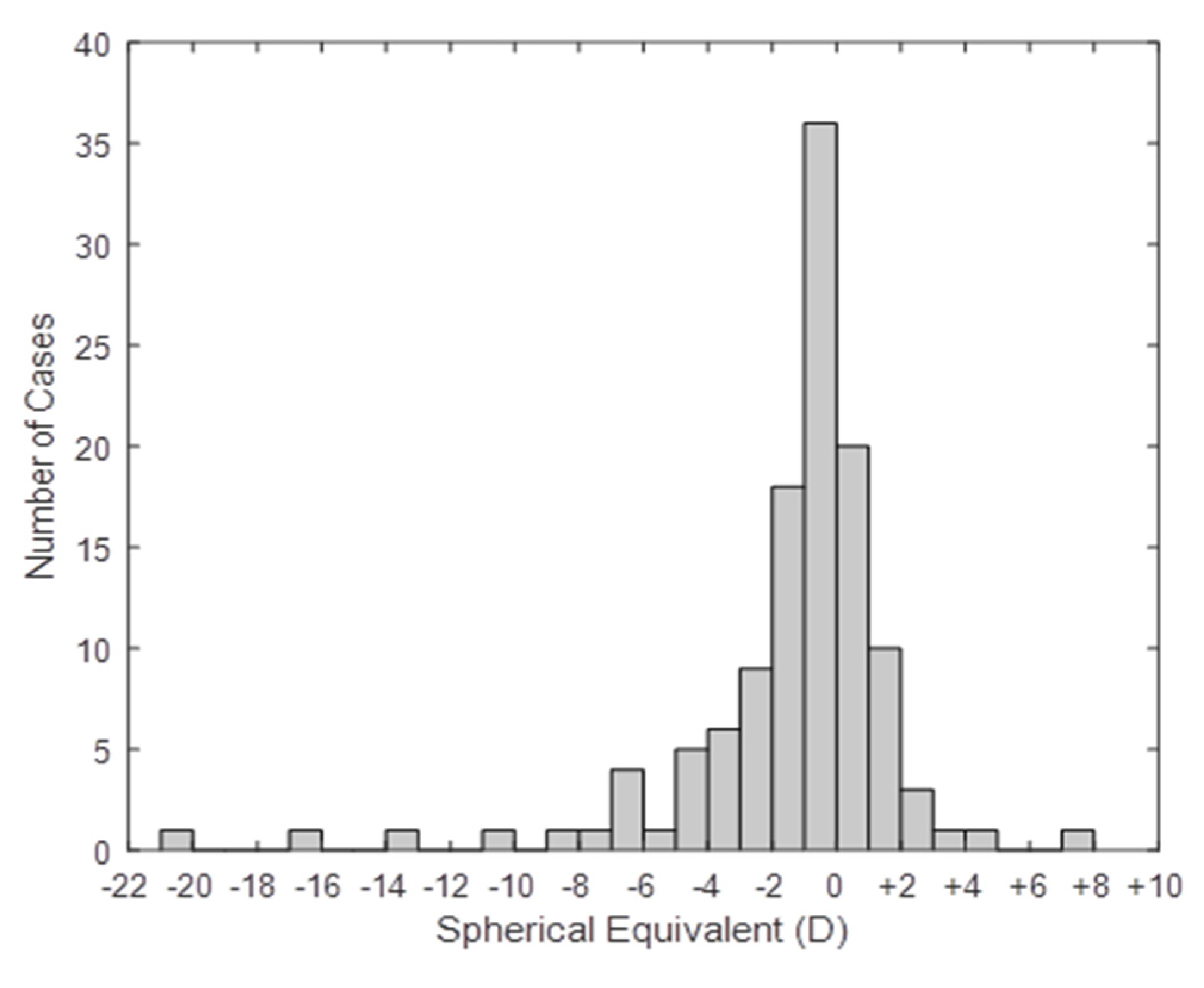
3.11. Autorefraction (Refractive Error)
3.12. Gender
3.13. Full Refraction and Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McKenzie, K.; Milton, M.; Smith, G.; Ouellette-Kuntz, H. Systematic Review of the Prevalence and Incidence of Intellectual Disabilities: Current Trends and Issues. Curr. Dev. Disord. Rep. 2016, 3, 104–115. [Google Scholar] [CrossRef] [Green Version]
- INE. PORDATA—Ambiente de Consulta. XIV Recenseamento Geral da População. 2001. Available online: https://www.pordata.pt/DB/Portugal/Ambiente+de+Consulta/Tabela (accessed on 18 May 2020).
- Emerson, E. Poverty and people with intellectual disabilities. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Porterfield, S.L.; McBride, T.D. The effect of poverty and caregiver education on perceived need and access to health services among children with special health care needs. Am. J. Public Health 2007, 97, 323–329. [Google Scholar] [CrossRef]
- Emerson, E.; Robertson, J.; Wood, J. The Association Between Area-Level Indicators of Social Deprivation and the Emotional and Behavioural Needs of Black and South Asian Children with Intellectual Disabilities in a Deprived Urban Environment. J. Appl. Res. Intellect. Disabil. 2007, 20, 420–429. [Google Scholar] [CrossRef]
- Martínez-Leal, R.; Salvador-Carulla, L.; Linehan, C.; Walsh, P.; Weber, G.; Van Hove, G.; Määttä, T.; Azema, B.; Haveman, M.; Buono, S.; et al. The impact of living arrangements and deinstitutionalisation in the health status of persons with intellectual disability in Europe. J. Intellect. Disabil. Res. 2011, 55, 858–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruddick, L. Health of people with intellectual disabilities: A review of factors influencing access to health care. Br. J. Health Psychol. 2005, 10, 559–570. [Google Scholar] [CrossRef]
- Owens, P.L.; Kerker, B.D.; Zigler, E.; Horwitz, S.M. Vision and oral health needs of individuals with intellectual disability. Ment. Retard. Dev. Disabil. Res. Rev. 2006, 12, 28–40. [Google Scholar] [CrossRef]
- Herer, G.R. Intellectual Disabilities and Hearing Loss. Commun. Disord. Q. 2012, 33, 252–260. [Google Scholar] [CrossRef]
- Evenhuis, H.M.; Sjoukes, L.; Koot, H.M.; Kooijman, A.C. Does visual impairment lead to additional disability in adults with intellectual disabilities? J. Intellect. Disabil. Res. 2009, 53, 19–28. [Google Scholar] [CrossRef]
- Warburg, M. Visual impairment in adult people with intellectual disability: Literature review. J. Intellect. Disabil. Res. 2001, 45, 424–438. [Google Scholar] [CrossRef]
- Akinci, A.; Oner, O.; Bozkurt, O.H.; Guven, A.; Degerliyurt, A.; Munir, K. Refractive errors and ocular findings in children with intellectual disability: A controlled study. J. AAPOS 2008, 12, 477–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Splunder, J.; Stilma, J.S.; Bernsen, R.M.D.; Evenhuis, H.M. Prevalence of visual impairment in adults with intellectual disabilities in the Netherlands: Cross-sectional study. Eye 2006, 20, 1004–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Splunder, J.; Stilma, J.S.; Bernsen, R.M.D.; Evenhuis, H.M. Prevalence of ocular diagnoses found on screening 1539 adults with intellectual disabilities. Ophthalmology 2004, 111, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Evenhuis, H.M.; Theunissen, M.; Denkers, I.; Verschuure, H.; Kemme, H. Prevalence of visual and hearing impairment in a Dutch institutionalized population with intellectual disability. J. Intellect. Disabil. Res. 2001, 45, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Block, S.S.; Beckerman, S.A.; Berman, P.E. Vision profile of the athletes of the 1995 Special Olympics World Summer Games. J. Am. Optom. Assoc. 1997, 68, 699–708. [Google Scholar]
- Donaldson, L.A.; Karas, M.; O’Brien, D.; Margaret Woodhouse, J. Findings from an opt-in eye examination service in English special schools. Is vision screening effective for this population? PLoS ONE 2019, 14, e0212733. [Google Scholar] [CrossRef]
- Li, J.C.; Wong, K.; Park, A.S.; Fricke, T.R.; Jackson, A.J. The challenges of providing eye care for adults with intellectual disabilities. Clin. Exp. Optom. 2015, 98, 420–429. [Google Scholar] [CrossRef]
- Woodhouse, J.M.; Adler, P.M.; Duignan, A. Ocular and visual defects amongst people with intellectual disabilities participating in Special Olympics. Ophthalmic Physiol. Opt. 2003, 23, 221–232. [Google Scholar] [CrossRef]
- Hyvärinen, L.; Näsänen, R.; Laurinen, P. New Visual Acuity Test for Pre-School Children. Acta Ophthalmol. 1980, 58, 507–511. [Google Scholar] [CrossRef]
- Dobson, V.; Maguire, M.; Orel-Bixler, D.; Quinn, G.; Ying, G. Visual acuity results in school-aged children and adults: Lea Symbols chart versus Bailey-Lovie chart. Optom. Vis. Sci. 2003, 80, 650–654. [Google Scholar]
- Hammond, R.S.; Schmidt, P.P. A Random Dot E Stereogram for the Vision Screening of Children. Arch. Ophthalmol. 1986, 104, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Rosner, J. The effectiveness of the random dot E stereotest as a preschool vision screening instrument. J. Am. Optom. Assoc. 1978, 49, 1121–1124. [Google Scholar] [PubMed]
- Schmidt, P.P. Vision screening with the RDE stereotest in pediatric populations. Optom. Vis. Sci. 1994, 71, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Cotter, S.A.; Lee, D.Y.; French, A.L. Evaluation of a new color vision test: “Color Vision Testing Made Easy”. Optom. Vis. Sci. 1999, 76, 631–636. [Google Scholar] [CrossRef]
- Van Der Jagt, L.H.; Jansonius, N.M. Three portable tonometers, the TGDc-01, the ICARE and the Tonopen XL, compared with each other and with Goldmann applanation tonometry. Ophthalmic Physiol. Opt. 2005, 25, 429–435. [Google Scholar] [CrossRef]
- Martin, X.D. Normal intraocular pressure in man. Ophthalmologica 1992, 205, 57–63. [Google Scholar] [CrossRef]
- Harvey, E.M.; Miller, J.M.; Wagner, L.K.; Dobson, V. Reproducibility and accuracy of measurements with a hand held autorefractor in children. Br. J. Ophthalmol. 1997, 81, 941–948. [Google Scholar] [CrossRef]
- Farook, M.; Venkatramani, J.; Gazzard, G.; Cheng, A.; Tan, D.; Seang-Mei, S. Comparisons of the handheld autorefractor, table-mounted autorefractor, and subjective refraction in Singapore adults. Optom. Vis. Sci. 2005, 82, 1066–1070. [Google Scholar] [CrossRef]
- Thibos, L.N.; Wheeler, W.; Horner, D. Power vectors: An application of fourier analysis to the description and statistical analysis of refractive error. Optom. Vis. Sci. 1997, 74, 367–375. [Google Scholar] [CrossRef]
- Word Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. 2011. Available online: www.who.int (accessed on 19 February 2020).
- Uzdrowska, M.; Margaret Woodhouse, J. Visual defects in special olympics participants from Europe. Clin. J. Sport Med. 2016, 26, 133–138. [Google Scholar] [CrossRef]
- Gothwal, V.K.; Sumalini, R.; Narasaiah, A.; Panda, S. Vision Profile and Ocular Characteristics of Special Olympics Athletes: Report from India. Ophthalmic Epidemiol. 2017, 24, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Adoh, T.O.; Woodhouse, J.M. The Cardiff acuity test used for measuring visual acuity development in toddlers. Vis. Res. 1994, 34, 555–560. [Google Scholar] [CrossRef]
- Lowery, J.P.; Hayes, J.R.; Sis, M.; Griffith, A.; Taylor, D. Pacific Acuity Test. Optom. Vis. Sci. 2014, 91, 76–85. [Google Scholar] [CrossRef]
- Mestre, C.; Otero, C.; Díaz-Doutón, F.; Gautier, J.; Pujol, J. An automated and objective cover test to measure heterophoria. PLoS ONE 2018, 13, e0206674. [Google Scholar] [CrossRef] [Green Version]
- McCulloch, D.L.; Sludden, P.A.; McKeown, K.; Kerr, A. Vision care requirements among intellectually disabled adults: A residence-based pilot study. J. Intellect. Disabil. Res. 2007, 40, 140–150. [Google Scholar] [CrossRef]
- Dick, J.; Finlayson, J.; Neil, J.; Mitchell, L.; Robinson, N. Vision awareness training for health and social care professionals working with people with intellectual disabilities: Post-training outcomes. Br. J. Vis. Impair. 2015, 33, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.; Surfraz, M.; Wroldsen, R.; Popa, D.; Grung, R.-M. Improving healthcare access for people with intellectual disabilities in four European countries. Learn Disabil. Pract. 2017, 20, 36–42. [Google Scholar] [CrossRef]
- Karadag, R.; Yagci, R.; Erdurmus, M.; Keskin, U.C.; Aydin, B.; Durmus, M. Ocular findings in individuals with intellectual disability. Can. J. Ophthalmol. 2007, 42, 703–706. [Google Scholar] [CrossRef]
- Hashemi, H.; Rezvan, F.; Yekta, A.A.; Hashemi, M.; Norouzirad, R.; Khabazkhoob, M. The prevalence of astigmatism and its determinants in a rural population of Iran: The “Nooravaran Salamat” mobile eye clinic experience. Middle East Afr. J. Ophthalmol. 2014, 21, 175–181. [Google Scholar]
- Boot, F.H.; Pel, J.J.M.; van der Steen, J.; Evenhuis, H.M. Cerebral visual impairment: Which perceptive visual dysfunctions can be expected in children with brain damage? A systematic review. Res. Dev. Disabil. 2010, 31, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, L.S.; Skov, L.; Jensen, H. Visual dysfunctions and ocular disorders in children with developmental delay. I. Prevalence, diagnoses and aetiology of visual impairment. Acta Ophthalmol. Scand. 2007, 85, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, M. Cortical visual impairment in children—A new challenge for the future? Oman. J. Ophthalmol. 2011, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Hultman, O.; Beth Høeg, T.; Munch, I.C.; Ellervik, C.; la Cour, M.; Andersson Grönlund, M.; Buch Hesgaard, H. The Danish Rural Eye Study: Prevalence of strabismus among 3785 Danish adults—A population-based cross-sectional study. Acta Ophthalmol. 2019, 97, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Erickson, G.B.; Block, S.S. Testability of a color vision screening test in a population with mental retardation. J. Am. Optom. Assoc. 1999, 70, 758–763. [Google Scholar]
- Adler, P.; Cregg, M.; Duignan, A.; Ilett, G.; Woodhouse, J.M. Effect of training on attitudes and expertise of optometrists towards people with intellectual disabilities. Ophthalmic Physiol. Opt. 2005, 25, 105–118. [Google Scholar] [CrossRef] [PubMed]
- David, R.; Zangwill, L.; Stone, D.; Yassur, Y. Epidemiology of intraocular pressure in a population screened for glaucoma. Br. J. Ophthalmol. 1987, 71, 766–771. [Google Scholar] [CrossRef]
- Warburg, M. Visual impairment in adult people with moderate, severe, and profound intellectual disability. Acta Ophthalmol. Scand. 2001, 79, 450–454. [Google Scholar] [CrossRef]
- Resnikoff, S.; Pascolini, D.; Etya’Ale, D.; Kocur, I.; Pararajasegaram, R.; Pokharel, G.P.; Mariotti, S.P. Global data on visual impairment in the year 2002. Bull. World Health Organ. 2004, 82, 844–851. [Google Scholar]
- Rudnicka, A.R.; Mt-Isa, S.; Owen, C.G.; Cook, D.G.; Ashby, D. Variations in primary open-angle glaucoma prevalence by age, gender, and race: A Bayesian meta-analysis. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4254–4261. [Google Scholar] [CrossRef] [Green Version]
- Shen, L.; Melles, R.B.; Metlapally, R.; Barcellos, L.; Schaefer, C.; Risch, N.; Herrinton, L.J.; Wildsoet, C.; Jorgenson, E. The Association of Refractive Error with Glaucoma in a Multiethnic Population. Ophthalmology 2016, 123, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Gogate, P.; Soneji, F.; Kharat, J.; Dulera, H.; Deshpande, M.; Gilbert, C. Ocular disorders in children with learning disabilities in special education schools of Pune, India. Indian J. Ophthalmol. 2011, 59, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.M.-L.; Yeo, A.C.H.; Scheiman, M.; Chen, X. Vergence and Accommodative Dysfunctions in Emmetropic and Myopic Chinese Young Adults. J. Ophthalmol. 2019, 5904903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leone, J.F.; Cornell, E.; Morgan, I.G.; Mitchell, P.; Kifley, A.; Wang, J.J.; Rose, K.A. Prevalence of heterophoria and associations with refractive error, heterotropia and ethnicity in Australian school children. Br. J. Ophthalmol. 2010, 94, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, J.M.; Adler, P.; Duignan, A. Vision in athletes with intellectual disabilities: The need for improved eyecare. J. Intellect. Disabil. Res. 2004, 48, 736–745. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Stations | Number of Athletes n (%) |
|---|---|
| Personal medical history | 134 (100) |
| Distance and near visual acuity | 96 (71.6) |
| Cover test | 111 (82.8) |
| Stereopsis | 105 (78.4) |
| Colour vision | 117 (87.3) |
| Autorefraction | 122 (91.0) |
| Intraocular pressure | 103 (77.9) |
| Slit-lamp biomicroscopy | 134 (100) |
| Ophthalmoscopy | 134 (100) |
| Total number of athletes | 134 (100) |
| Last Eye Exam | Number of Individuals n (%) | Number of Non-Spectacle Wearers n (%) | Number of Spectacle Wearers n (%) |
|---|---|---|---|
| <1 year | 19 (14.2) | 6 (7.3) | 13 (25) |
| >3 years | 14 (10.4) | 9 (11.0) | 5 (9.6) |
| 1 to 3 years | 29 (21.6) | 7 (8.5) | 22 (42.3) |
| Never | 34 (25.4) | 34 (41.5) | 0 (0.0) |
| Not known | 38 (28.4) | 26 (31.7) | 12 (23.1) |
| Total | 134 (100) | 82 (100) | 52 (100) |
| Symptoms | Number of Athletes n (%) |
|---|---|
| Headaches | 32 (23.9) |
| Photosensivity | 24 (17.9) |
| Difficulty seeing at distance | 23 (17.2) |
| Difficulty seeing (distance and near) | 12 (9.0) |
| Difficulty seeing at near | 11 (8.2) |
| Double vision | 8 (5.9) |
| Total number of athletes | 134 (100) |
| Number of athletes | |||
|---|---|---|---|
| All n (%) | Spectacle Wearers n (%) | Non-Spectacle Wearers n (%) | |
| Pass distance and pass near | 47 (49.0) | 12 (32.4) | 35 (59.3) |
| Pass distance and fail near | 7 (7.3) | 2 (5.4) | 8 (13.6) |
| Fail distance and pass near | 20 (20.8) | 12 (32.4) | 8 (13.6) |
| Fail distance and fail near | 22 (22.9) | 11 (29.7) | 11 (18.6) |
| Total | 96 (100) | 37 (100) | 59 (100) |
| Type of Deviation | Number of Athletes n (%) | |
|---|---|---|
| Distance | Near | |
| Exotropia | 15 (13.5) | 15 (13.5) |
| Esotropia | 6 (5.4) | 7 (6.3) |
| Hypertropia | 7 (6.3) | 6 (5.4) |
| Orthophoria | 76 (68.5) | 59 (53.2) |
| Exophoria | 7 (6.3) | 20 (18.0) |
| Esophoria | 0 (0) | 4 (3.6) |
| Total | 111 (100) | 111 (100) |
| Eye Health | Number of Athletes n (%) |
|---|---|
| Absence of eyelids | 1 (0.7) |
| Blepharitis | 3 (2.2) |
| Cataract or lens opacities | 11 (8.2) |
| Conjunctival follicles | 4 (3.0) |
| Conjunctival hyperaemia | 15 (11.2) |
| Conjunctivitis | 2 (1.5) |
| Corneal opacity | 1 (0.7) |
| Disc abnormalities | 2 (1.5) |
| Glaucoma suspect † | 5 (3.7) |
| Intraocular lenses | 2 (1.5) |
| Lachrymal duct obstruction | 1 (0.7) |
| Madarosis | 1 (0.7) |
| Meibomian gland dysfunction | 8 (6.0) |
| Normal Exam | 54 (54.5) |
| Pterygium/Pinguecula | 5 (3.7) |
| Keratoconus | 1(0.7) |
| Retina abnormalities | 1 (0.7) |
| Total | 134 (100) |
| Spherical Equivalent (DS) | Number of athletes | ||||
|---|---|---|---|---|---|
| All n (%) | Spectacle Wearers n (%) | Non-Spectacle Wearers n (%) | Males n (%) | Females n (%) | |
| High myopia (≤−6.00) | 10 (8.2) | 9 (19.1) | 1 (1.3) | 8 (8.8) | 2 (6.5) |
| Moderate myopia (−3.00; −6.00) | 12 (9.8) | 7 (14.9) | 5 (6.7) | 10 (11.0) | 2 (6.5) |
| Low myopia (−1.00; −3.00) | 27 (22.1) | 8 (17.0) | 19 (25.3) | 19 (20.9) | 8 (25.8) |
| Emmetropia (−1.00; +1.00) | 57 (46.7) | 15 (31.9) | 42 (56.0) | 44 (48.4) | 13 (41.9) |
| Low hyperopia (+1.00; +3.00) | 13 (10.7) | 5 (10.6) | 8 (10.7) | 7 (7.7) | 6 (19.4) |
| Moderate hyperopia (+3.00; +6.00) | 2 (1.6) | 2 (4.3) | 0 (0) | 2 (2.2) | 0 (0) |
| High hyperopia (>+6.00) | 1 (0.8) | 1 (2.1) | 0 (0) | 1 (1.1) | 0 (0) |
| Total | 122 (100) | 47 (100) | 75 (100) | 91 (100) | 31 (100) |
| U= 1378, p = 0.064 | U = 1387, p = 0.897 | ||||
| Cylinder (DC) | |||||
| No significant cylinder (0.00; 1.00) | 81 (66.4) | 20 (42.6) | 61 (81.3) | 59 (64.8) | 22 (70.7) |
| Low cylinder (1.00; 3.00) | 30 (24.6) | 19 (40.4) | 11 (14.7) | 24 (26.4) | 6 (19.4 |
| High cylinder (>3.00) | 11 (9.0) | 8 (17) | 3 (4.0) | 8 (8.7) | 3 (9.7) |
| Total | 122 (100) | 47 (100) | 75 (100) | 91 (100) | 31 (100) |
| U = 1060.5, p < 0.001 | U = 1414.5, p = 0.949 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serra, P.; Costa, R.; Almeida, N.; Baptista, A. Visual Status in a Portuguese Population with Intellectual Disability. Int. J. Environ. Res. Public Health 2020, 17, 7715. https://doi.org/10.3390/ijerph17217715
Serra P, Costa R, Almeida N, Baptista A. Visual Status in a Portuguese Population with Intellectual Disability. International Journal of Environmental Research and Public Health. 2020; 17(21):7715. https://doi.org/10.3390/ijerph17217715
Chicago/Turabian StyleSerra, Pedro, Regina Costa, Nuno Almeida, and António Baptista. 2020. "Visual Status in a Portuguese Population with Intellectual Disability" International Journal of Environmental Research and Public Health 17, no. 21: 7715. https://doi.org/10.3390/ijerph17217715
APA StyleSerra, P., Costa, R., Almeida, N., & Baptista, A. (2020). Visual Status in a Portuguese Population with Intellectual Disability. International Journal of Environmental Research and Public Health, 17(21), 7715. https://doi.org/10.3390/ijerph17217715