Social Intelligence and Psychological Distress: Subjective and Psychological Well-Being as Mediators



 and
and
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Procedure
2.3. Instruments
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics and Correlations between Study Variables
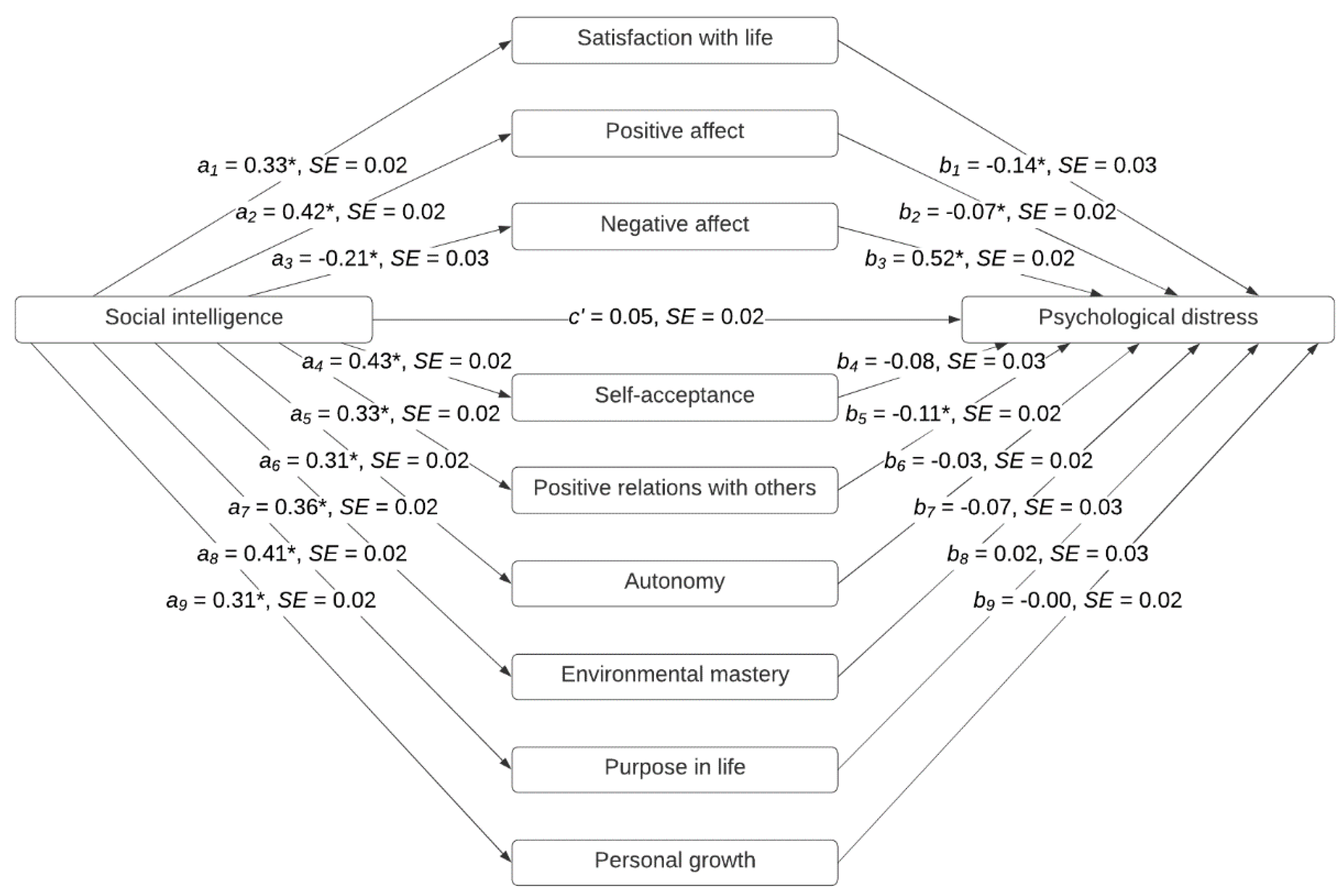
3.2. Multiple Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A


References
- Mayer, J.D.; Caruso, D.R.; Salovey, P. The ability model of emotional intelligence: Principles and updates. Emot. Rev. 2016, 8, 290–300. [Google Scholar] [CrossRef]
- Peterson, C.; Seligman, M.E.P. Character Strengths and Virtues: A Handbook and Classification; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Buschor, C.; Proyer, R.T.; Ruch, W. Self- and peer-rated character strengths: How do they relate to satisfaction with life and orientations to happiness? J. Posit. Psychol. 2013, 8, 116–127. [Google Scholar] [CrossRef] [Green Version]
- Emmons, R.A.; McCullough, M.E. Counting blessings versus burdens: An experimental investigation of gratitude and subjective well-being in daily life. J. Pers. Soc. Psychol. 2003, 84, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Güsewell, A.; Ruch, W. Are only emotional strengths emotional? Character strengths and disposition to positive emotions. Appl. Psychol. Health Well Being 2012, 4, 218–239. [Google Scholar] [CrossRef]
- Park, N.; Peterson, C.; Seligman, M.E.P. Strengths of character and wellbeing. J. Soc. Clin. Psychol. 2004, 23, 603–619. [Google Scholar] [CrossRef] [Green Version]
- Peterson, C.; Ruch, W.; Beermann, U.; Park, N.; Seligman, M.E.P. Strengths of character, orientations to happiness, and life satisfaction. J. Posit. Psychol. 2007, 2, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Gillham, J.; Adams-Deutsch, Z.; Werner, J.; Reivich, K.; Coulter-Heindl, V.; Linkins, M.; Winder, B.; Peterson, C.; Park, N.; Abenavoli, R.; et al. Character strengths predict subjective well-being during adolescence. J. Posit. Psychol. 2011, 6, 31–44. [Google Scholar] [CrossRef]
- Park, N.; Peterson, C. Positive psychology and character strengths: Application to strengths-based school counseling. Prof. Sch. Couns. 2008, 12, 85–92. [Google Scholar] [CrossRef]
- Weber, M.; Ruch, W.; Littman-Ovadia, H.; Lavy, S.; Gai, O. Relationships among higher-order strengths factors, subjective well-being, and general self-efficacy—The case of Israeli adolescents. Pers. Individ. Differ. 2013, 55, 322–327. [Google Scholar] [CrossRef] [Green Version]
- Deci, E.L.; Ryan, R.M. Hedonia, eudaimonia, and well-being: An introduction. J. Happiness Stud. 2008, 9, 1–11. [Google Scholar] [CrossRef]
- Keyes, C.L.M.; Shmotkin, D.; Ryff, C.D. Optimizing well-being: The empirical encounter of two traditions. J. Pers. Soc. Psychol. 2002, 82, 1007–1022. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 42, 141–166. [Google Scholar] [CrossRef]
- Ryff, C.D. Beyond Ponce de Leon and life satisfaction: New directions in quest of successful aging. Int. J. Behav. Dev. 1989, 12, 35–55. [Google Scholar] [CrossRef]
- Hausler, M.; Strecker, C.; Huber, A.; Brenner, M.; Höge, T.; Höfer, S. Distinguishing relational aspects of character strengths with subjective and psychological well-being. Front. Psychol. 2017, 8, 1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azañedo, C.M.; Fernández-Abascal, E.G.; Barraca, J. Character strengths in Spain: Validation of the Values in Action Inventory of Strengths (VIA-IS) in a Spanish sample. Clin. Salud 2014, 25, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Littman-Ovadia, H.; Lavy, S. Character strengths in Israel: Hebrew adaptation of the VIA Inventory of Strengths. Eur. J. Psychol. Assess. 2012, 28, 41–50. [Google Scholar] [CrossRef]
- Ruch, W.; Proyer, R.T.; Harzer, C.; Park, N.; Peterson, C.; Seligman, M.E.P. Values in Action Inventory of Strengths (VIA-IS): Adaptation and validation of the German version and the development of a peer-rating form. J. Individ. Differ. 2010, 31, 138–149. [Google Scholar] [CrossRef]
- Khumalo, I.P.; Wissing, M.P.; Temane, Q.M. Exploring the validity of the Values-In-Action Inventory of Strengths (VIA-IS) in an African context. J. Psychol. Afr. 2008, 18, 133–142. [Google Scholar] [CrossRef]
- Leontopoulou, S.; Triliva, S. Explorations of subjective wellbeing and character strengths among a Greek University student sample. Int. J. Well Being 2012, 2, 251–270. [Google Scholar] [CrossRef] [Green Version]
- Ryff, C.D. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychother. Psychosom. 2014, 83, 10–28. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L.M. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyes, C.L.M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L.M.; Dhingra, S.S.; Simoes, E.J. Change in level of positive mental health as a predictor of future risk of mental illness. Am. J. Public Health 2010, 100, 2366–2371. [Google Scholar] [CrossRef] [PubMed]
- Valiente, C.; Provencio, M.; Espinosa, R.; Chaves, C.; Fuentenebro, F. Predictors of subjective well-being in patients with paranoid symptoms: Is insight necessarily advantageous? Psychiatry Res. 2011, 189, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Davison, T.E.; McCabe, M.P.; Knight, T.; Mellor, D. Biopsychosocial factors related to depression in aged care residents. J. Affect. Disord. 2012, 142, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Feder, A.; Ahmad, S.; Lee, E.J.; Morgan, J.E.; Singh, R.; Smith, B.W.; Southwick, S.M.; Charney, D.S. Coping and PTSD symptoms in Pakistani earthquake survivors: Purpose in life, religious coping and social support. J. Affect. Disord. 2013, 147, 156–163. [Google Scholar] [CrossRef]
- Strauss, G.P.; Sandt, A.R.; Catalano, L.T.; Allen, D.N. Negative symptoms and depression predict lower psychological well-being in individuals with schizophrenia. Compr. Psychiat. 2012, 53, 1137–1144. [Google Scholar] [CrossRef]
- Valiente, C.; Cantero, D.; Vázquez, C.; Sanchez, A.; Provencio, M.; Espinosa, R. Implicit and explicit self-esteem discrepancies in paranoia and depression. J. Abnorm. Psychol. 2011, 120, 691. [Google Scholar] [CrossRef] [Green Version]
- Fredrickson, B.L. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; King, L.; Diener, E. The benefits of frequent positive affect: Does happiness lead to success? Psychol. Bull. 2005, 131, 803–855. [Google Scholar] [CrossRef] [Green Version]
- Avia, M.D.; Vázquez, C. Optimismo Inteligente [Intelligent Optimism]; Alianza Editorial: Madrid, Spain, 1998. [Google Scholar]
- Fredrickson, B.L. Updated thinking on positivity ratios. Am. Psychol. 2013, 68, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, C.; Hervás, G.; Ho, S. Intervenciones clínicas basadas en la psicología positiva: Fundamentos y aplicaciones. Psicol. Conduct. 2006, 14, 401–432. [Google Scholar]
- Vázquez, C.; Hervás, G.; Rahona, J.J.; Gómez, D. Psychological well-being and health: Contributions of positive psychology. Annu. Clin. Health Psychol. 2009, 5, 15–27. [Google Scholar]
- Fredrickson, B.L. Positivity: Groundbreaking Research Reveals How to Embrace the Hidden Strength of Positive Emotions, Overcome Negativity, and Thrive; Crown Archetype: New York, NY, USA, 2009. [Google Scholar]
- Peterson, C.; Park, N. Classifying and measuring strengths of character. In Oxford Handbook of Positive Psychology, 2nd ed.; López, S.J., Snyder, C.R., Eds.; Oxford University Press: New York, NY, USA, 2009; pp. 25–33. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Atienza, F.L.; Pons, D.; Balaguer, I.; García-Merita, M.L. Propiedades psicométricas de la Escala de Satisfacción con la Vida en adolescentes [Psychometric properties of the Life Satisfaction Scale in adolescents]. Psicothema 2000, 12, 314–319. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Pers. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Díaz, D.; Rodríguez-Carvajal, R.; Blanco, A.; Moreno-Jiménez, B.; Gallardo, I.; Valle, C.; van Dierendonck, D. Adaptación española de las escalas de bienestar psicológico de Ryff [Spanish adaptation of Ryff’s psychological well-being scales]. Psicothema 2006, 18, 572–577. [Google Scholar]
- Derogatis, L.R. Symptom Checklist-90-Revised (SCL-90-R): Administration, Scoring and Procedures Manual; NCS Pearson, Inc.: Bloomington, MN, USA, 1994. [Google Scholar]
- Derogatis, L.R. SCL-90-R. Cuestionario de 90 Síntomas [SCL-90-R. Symptom Checklist-90-Revised]; TEA Ediciones: Madrid, Spain, 2002. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Lamers, S.M.A.; Westerhof, G.J.; Glas, C.A.W.; Bohlmeijer, E.T. The bidirectional relation between positive mental health and psychopathology in a longitudinal representative panel study. J. Posit. Psychol. 2015, 10, 553–560. [Google Scholar] [CrossRef]
- Wood, A.M.; Joseph, S. The absence of positive psychological (eudemonic) well-being as a risk factor for depression: A ten year cohort study. J. Affect. Disord. 2010, 122, 213–217. [Google Scholar] [CrossRef]
- Kobau, R.; Seligman, M.E.; Peterson, C.; Diener, E.; Zack, M.M.; Chapman, D.; Thompson, W. Mental health promotion in public health: Perspectives and strategies from positive psychology. Am. J. Public Health 2011, 101, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, B.H.; Bergen, A.E. Social support concepts and measures. J. Psychosom. Res. 2010, 69, 511–520. [Google Scholar] [CrossRef]
- Henrich, C.C.; Shahar, G. Social support buffers the effects of terrorism on adolescent depression: Findings from Sderot, Israel. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 1073–1076. [Google Scholar] [CrossRef]
- Calvete, E.; Connor-Smith, J.K. Perceived social support, coping, and symptoms of distress in American and Spanish students. Anxiety Stress Coping 2006, 19, 47–65. [Google Scholar] [CrossRef]
- Lakey, B.; Cohen, S. Social support and theory. In Social Support Measurement and Intervention: A Guide for Health and Social Scientists; Cohen, S., Underwood, L.G., Gottlieb, B.H., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 29–52. [Google Scholar]
- Seligman, M.E.P.; Rashid, T.; Parks, A.C. Positive psychotherapy. Am. Psychol. 2006, 61, 774–788. [Google Scholar] [CrossRef] [Green Version]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the rela-tionship between emotional intelligence and health. Pers. Individ. Differ. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Thorsteinsson, N.B.; Rooke, S.E. A meta-analytic investigation of the relationship between emotional intelligence and health. Pers. Individ. Differ. 2007, 42, 921–933. [Google Scholar] [CrossRef]
- Sánchez-Álvarez, N.; Extremera, N.; Fernández-Berrocal, P. The relation between emotional intelligence and subjective well-being: A meta-analytic investigation. J. Posit. Psychol. 2016, 11, 276–285. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Women | Men | Total | |||||
|---|---|---|---|---|---|---|---|
| Fr | % | Fr | % | Fr | % | ||
| Age | 18–24 | 229 | 29.32 | 111 | 17.73 | 340 | 24.16 |
| 25–34 | 224 | 28.68 | 170 | 27.16 | 394 | 28.00 | |
| 35–44 | 206 | 26.38 | 191 | 30.51 | 397 | 28.22 | |
| 45–54 | 106 | 13.57 | 119 | 19.01 | 225 | 15.99 | |
| 55–74 | 16 | 2.05 | 35 | 5.59 | 51 | 3.62 | |
| 781 | 100 | 626 | 100 | 1407 | 100 | ||
| Marital status | Single | 402 | 51.47 | 306 | 48.88 | 708 | 50.32 |
| Married | 207 | 26.50 | 197 | 31.47 | 404 | 28.71 | |
| Living as a couple without being married | 116 | 14.85 | 85 | 13.58 | 201 | 14.29 | |
| Divorced or separated | 53 | 6.79 | 36 | 5.75 | 89 | 6.33 | |
| Widowed | 3 | 0.38 | 2 | 0.32 | 5 | 0.36 | |
| 781 | 100 | 626 | 100 | 1407 | 100 | ||
| Educational level | High-school education | 311 | 39.82 | 240 | 38.34 | 551 | 39.16 |
| Postsecondary education | 127 | 16.26 | 97 | 15.50 | 224 | 15.92 | |
| University degree | 336 | 43.02 | 276 | 44.09 | 612 | 43.50 | |
| Ph.D. degree | 7 | 0.90 | 13 | 2.08 | 20 | 1.42 | |
| 781 | 100 | 626 | 100 | 1407 | 100 | ||
| Pearson Correlations | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| 1. Social intelligence | — | ||||||||||
| 2. Satisfaction with life | 0.32 * | — | |||||||||
| 3. Positive affect | 0.41 * | 0.52 * | — | ||||||||
| 4. Negative affect | −0.20 * | −0.45 * | −0.30 * | — | |||||||
| 5. Self-acceptance | 0.43 * | 0.74 * | 0.58 * | −0.47 * | — | ||||||
| 6. Positive relations | 0.32 * | 0.39 * | 0.31 * | −0.27 * | 0.46 * | — | |||||
| 7. Autonomy | 0.30 * | 0.27 * | 0.28 * | −0.34 * | 0.44 * | 0.26 * | — | ||||
| 8. Environmental mastery | 0.36 * | 0.67 * | 0.56 * | −0.47 * | 0.76 * | 0.47 * | 0.42 * | — | |||
| 9. Purpose in life | 0.41 * | 0.65 * | 0.56 * | −0.38 * | 0.79 * | 0.42 * | 0.34 * | 0.76 * | — | ||
| 10. Personal growth | 0.30 * | 0.35 * | 0.38 * | −0.21 * | 0.55 * | 0.34 * | 0.34 * | 0.51 * | 0.54 * | — | |
| 11. Psychological distress | −0.22 * | −0.55 * | −0.43 * | 0.72 * | −0.56 * | −0.36 * | −0.36 * | −0.56 * | −0.47 * | −0.29 * | — |
| Mean | 3.80 | 3.57 | 3.49 | 1.95 | 4.63 | 4.63 | 4.19 | 4.49 | 4.61 | 5.12 | 0.58 |
| Standard Deviation | 0.54 | 0.85 | 0.78 | 0.76 | 0.97 | 1.02 | 0.89 | 0.89 | 0.93 | 0.81 | 0.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azañedo, C.M.; Sastre, S.; Artola, T.; Alvarado, J.M.; Jiménez-Blanco, A. Social Intelligence and Psychological Distress: Subjective and Psychological Well-Being as Mediators. Int. J. Environ. Res. Public Health 2020, 17, 7785. https://doi.org/10.3390/ijerph17217785
Azañedo CM, Sastre S, Artola T, Alvarado JM, Jiménez-Blanco A. Social Intelligence and Psychological Distress: Subjective and Psychological Well-Being as Mediators. International Journal of Environmental Research and Public Health. 2020; 17(21):7785. https://doi.org/10.3390/ijerph17217785
Chicago/Turabian StyleAzañedo, Carolina M., Santiago Sastre, Teresa Artola, Jesús M. Alvarado, and Amelia Jiménez-Blanco. 2020. "Social Intelligence and Psychological Distress: Subjective and Psychological Well-Being as Mediators" International Journal of Environmental Research and Public Health 17, no. 21: 7785. https://doi.org/10.3390/ijerph17217785
APA StyleAzañedo, C. M., Sastre, S., Artola, T., Alvarado, J. M., & Jiménez-Blanco, A. (2020). Social Intelligence and Psychological Distress: Subjective and Psychological Well-Being as Mediators. International Journal of Environmental Research and Public Health, 17(21), 7785. https://doi.org/10.3390/ijerph17217785