Hands-On Times, Adherence to Recommendations and Variance in Execution among Three Different CPR Algorithms: A Prospective Randomized Single-Blind Simulator-Based Trial †


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
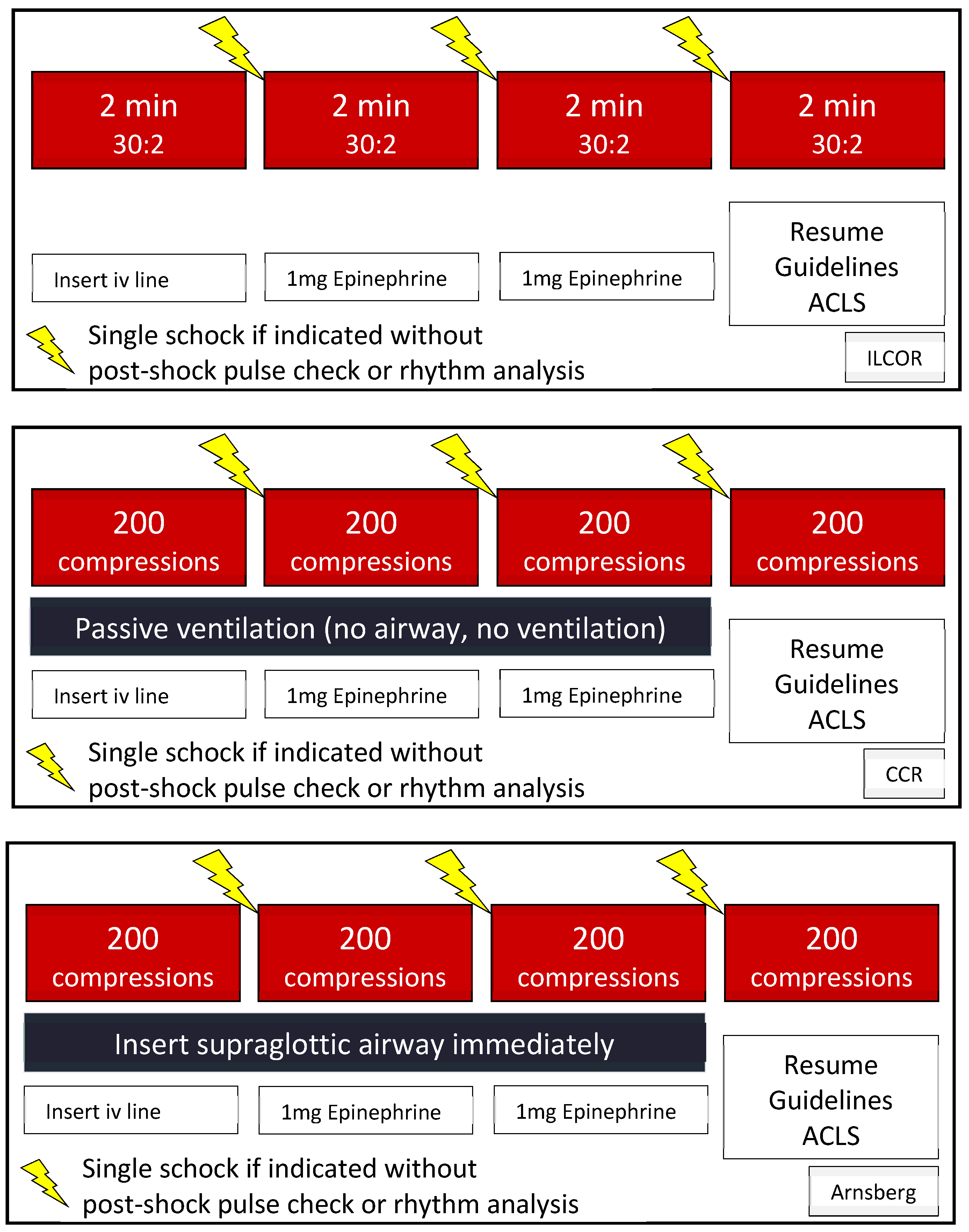
2.3. Interventions
2.4. Outcomes
2.5. Analysis
3. Results
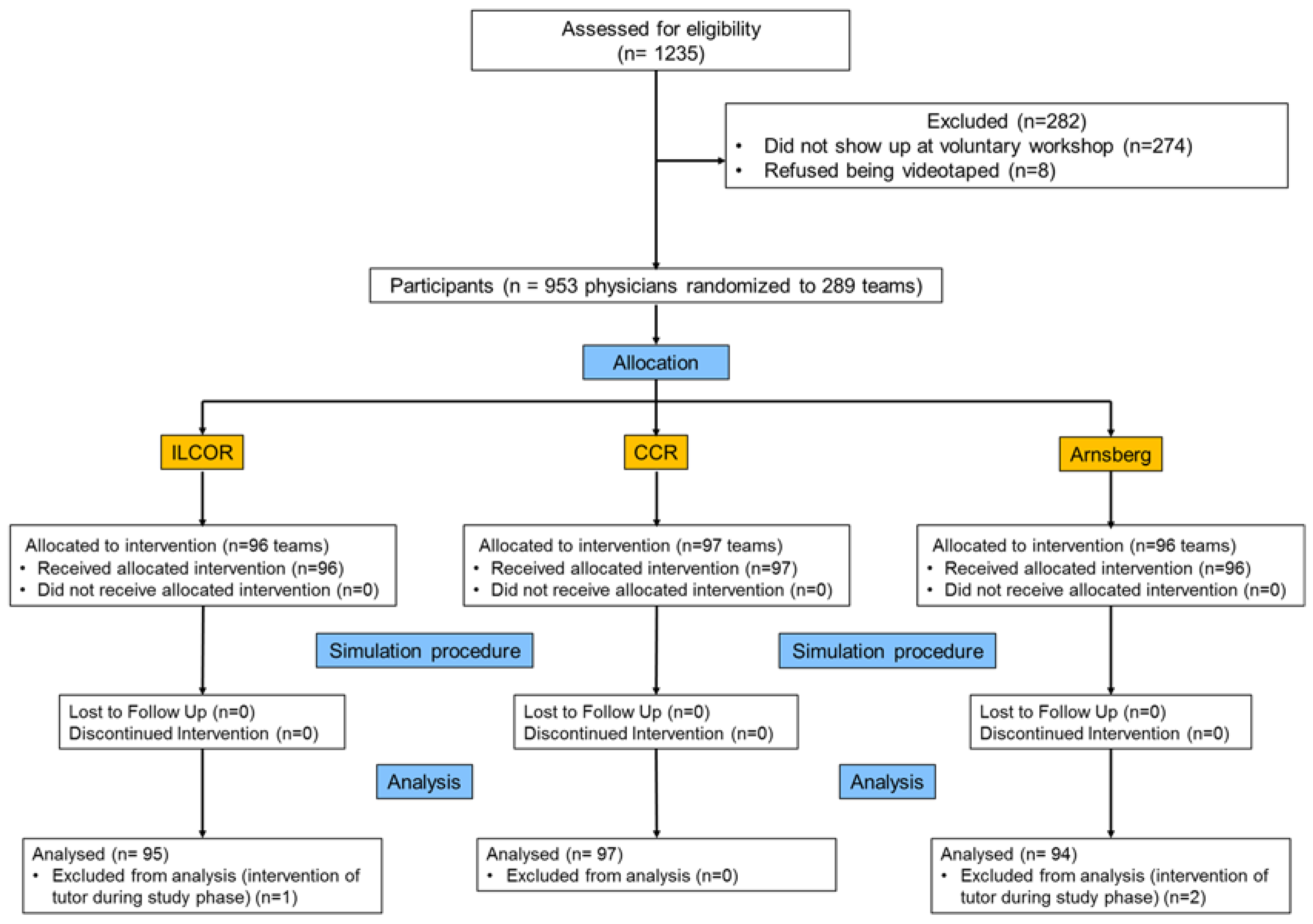
3.1. Participants
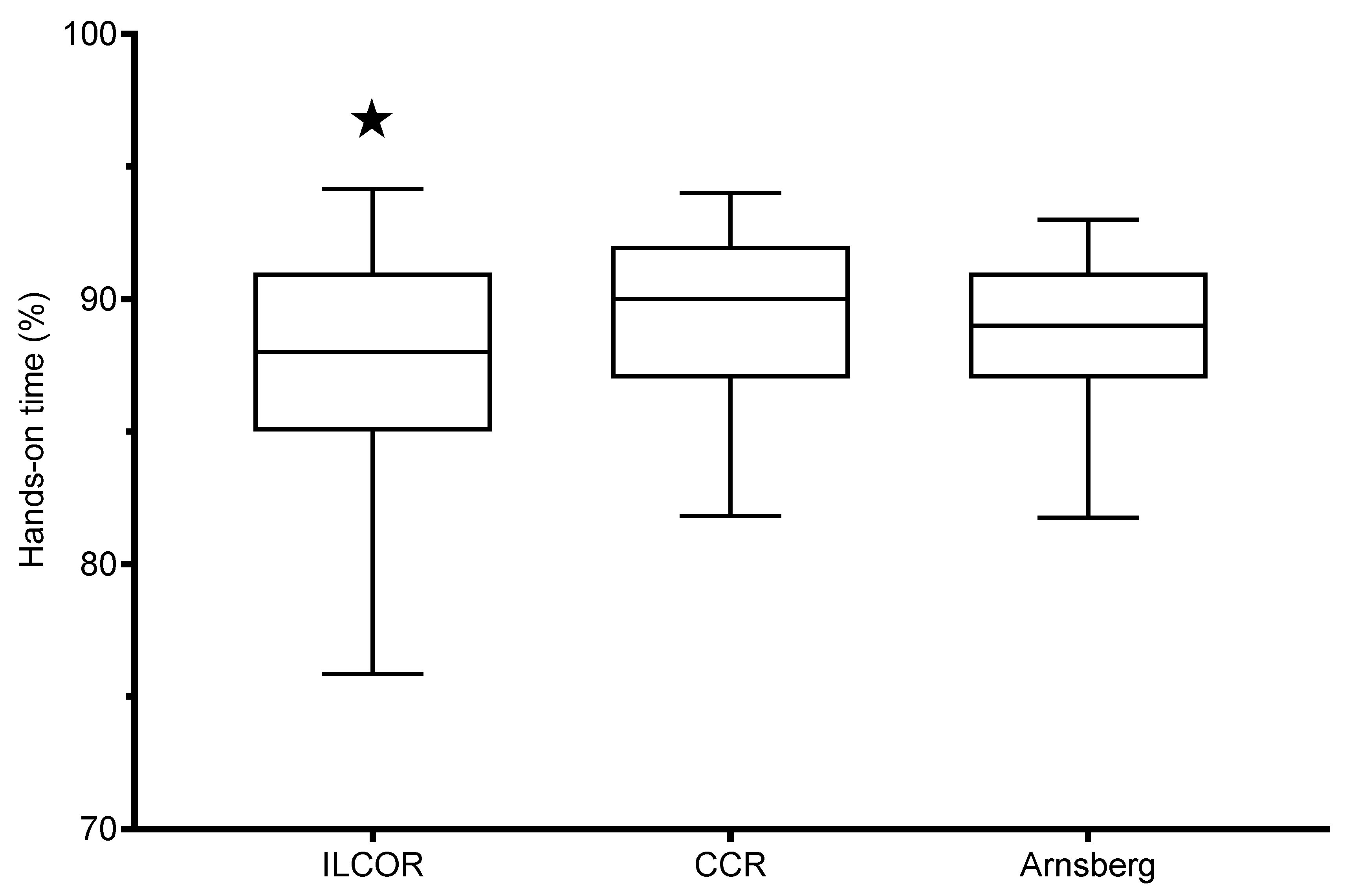
3.2. Primary Outcome
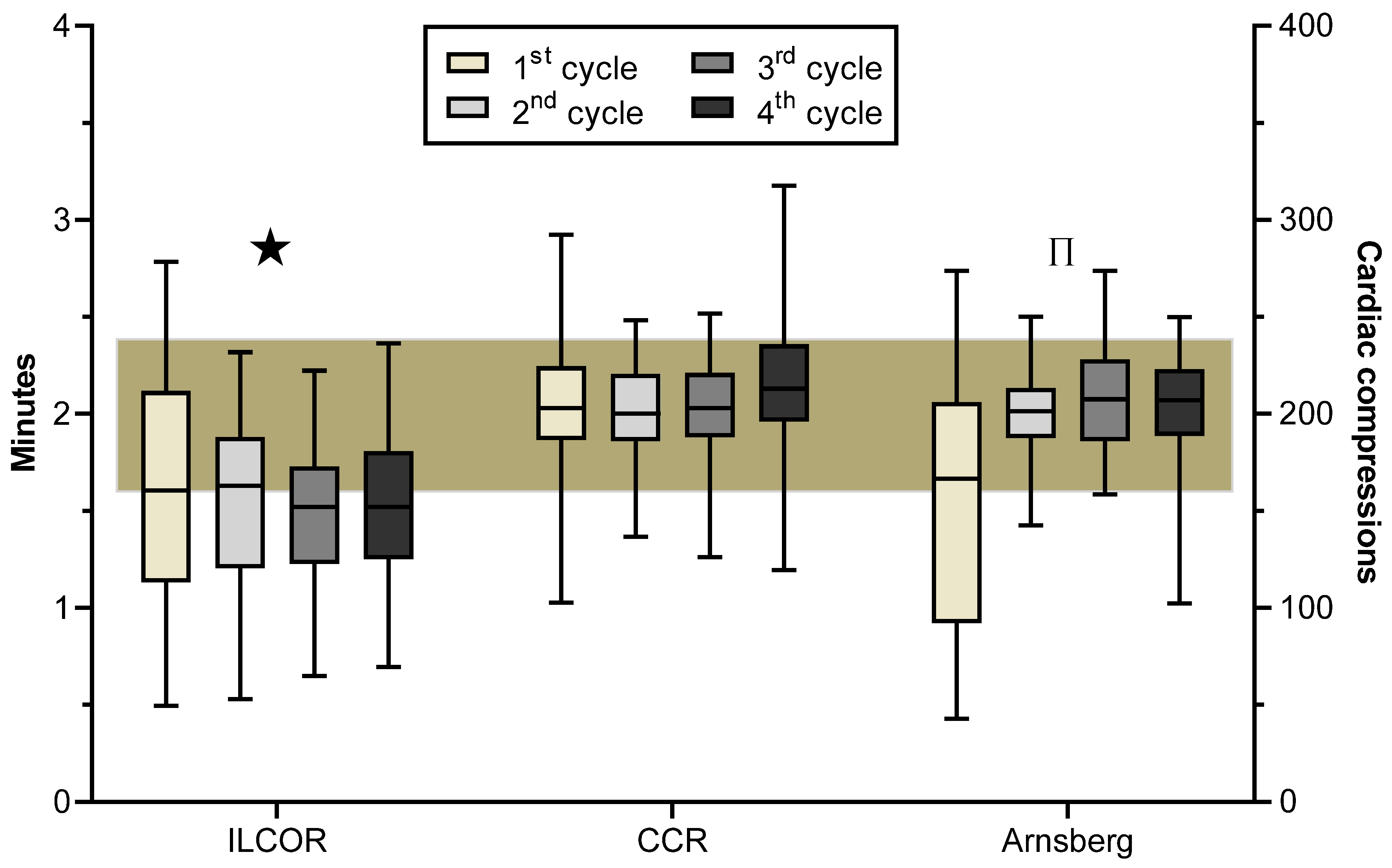
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Link, M.S.; Berkow, L.C.; Kudenchuk, P.J.; Halperin, H.R.; Hess, E.P.; Moitra, V.K.; Neumar, R.W.; O’Neil, B.J.; Paxton, J.H.; Silvers, S.M.; et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S444–S464. [Google Scholar] [CrossRef] [PubMed]
- Soar, J.; Nolan, J.P.; Boettiger, B.W.; Perkins, G.D.; Lott, C.; Carli, P.; Pellis, T.; Sandroni, C.; Skrifvars, M.B.; Smith, G.B.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015, 95, 100–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberger, Z.D.; Chan, P.S.; Berg, R.A.; Kronick, S.L.; Cooke, C.R.; Lu, M.; Banerjee, M.; Hayward, R.A.; Krumholz, H.M.; Nallamothu, B.K. Duration of resuscitation efforts and survival after in-hospital cardiac arrest: An observational study. Lancet 2012, 380, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Daya, M.R.; Schmicker, R.H.; Zive, D.M.; Rea, T.D.; Nichol, G.; Buick, J.E.; Brooks, S.; Christenson, J.; MacPhee, R.; Craig, A.; et al. Out-of-hospital cardiac arrest survival improving over time: Results from the Resuscitation Outcomes Consortium (ROC). Resuscitation 2015, 91, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Sasson, C.; Rogers, M.A.; Dahl, J.; Kellermann, A.L. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and meta-analysis. Circ. Cardiovasc Qual. Outcomes 2010, 3, 63–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewy, G.A. Cardiocerebral resuscitation: The new cardiopulmonary resuscitation. Circulation 2005, 111, 2134–2142. [Google Scholar] [CrossRef]
- Ewy, G.A.; Kern, K.B. Recent advances in cardiopulmonary resuscitation: Cardiocerebral resuscitation. J. Am. Coll. Cardiol. 2009, 53, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewy, G.A. The cardiocerebral resuscitation protocol for treatment of out-of-hospital primary cardiac arrest. Scand. J. Trauma Resusc Emerg. Med. 2012, 20, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewy, G.A.; Sanders, A.B. Alternative Approach to Improving Survival of Patients With Out-of-Hospital Primary Cardiac Arrest. J. Am. Coll. Cardiol. 2013, 61, 113–118. [Google Scholar] [CrossRef] [Green Version]
- Ewy, G.A. Cardiocerebral and cardiopulmonary resuscitation—2017 update. Acute Med. Surg. 2017, 4, 227–234. [Google Scholar] [CrossRef]
- Russi, C.S.; Miller, L.; Hartley, M.J. A comparison of the King-LT to endotracheal intubation and Combitube in a simulated difficult airway. Prehosp. Emerg. Care 2008, 12, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Abella, B.S.; Sandbo, N.; Vassilatos, P.; Alvarado, J.P.; O’Hearn, N.; Wigder, H.N.; Hoffman, P.; Tynus, K.; Vanden Hoek, T.L.; Becker, L.B. Chest compression rates during cardiopulmonary resuscitation are suboptimal: A prospective study during in-hospital cardiac arrest. Circulation 2005, 111, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Abella, B.S.; Alvarado, J.P.; Myklebust, H.; Edelson, D.P.; Barry, A.; O’Hearn, N.; Vanden Hoek, T.L.; Becker, L.B. Quality of Cardiopulmonary Resuscitation During In-Hospital Cardiac Arrest. JAMA 2005, 293, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Wik, L.; Kramer-Johansen, J.; Myklebust, H.; Sorebo, H.; Svensson, L.; Fellows, B.; Steen, P.A. Quality of Cardiopulmonary Resuscitation During Out-of-Hospital Cardiac Arrest. JAMA 2005, 293, 299–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunziker, S.; Tschan, F.; Semmer, N.K.; Zobrist, R.; Spychiger, M.; Breuer, M.; Hunziker, P.R.; Marsch, S.C. Hands-on time during cardiopulmonary resuscitation is affected by the process of teambuilding: A prospective randomised simulator-based trial. BMC Emerg. Med. 2009, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Marsch, S.C.; Muller, C.; Marquardt, K.; Conrad, G.; Tschan, F.; Hunziker, P.R. Human factors affect the quality of cardiopulmonary resuscitation in simulated cardiac arrests. Resuscitation 2004, 60, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Marsch, S.C.; Tschan, F.; Semmer, N.; Spychiger, M.; Breuer, M.; Hunziker, P.R. Performance of first responders in simulated cardiac arrests. Crit. Care Med. 2005, 33, 963–967. [Google Scholar] [CrossRef]
- Tschan, F.; Vetterli, M.; Semmer, N.K.; Hunziker, S.; Marsch, S.C. Activities during interruptions in cardiopulmonary resuscitation: A simulator study. Resuscitation 2011, 82, 1419–1423. [Google Scholar] [CrossRef]
- Marsch, S.; Tschan, F.; Semmer, N.K.; Zobrist, R.; Hunziker, P.; Hunziker, S. ABC versus CAB for cardiopulmonary resuscitation: A prospective, randomized simulator-based trial. Swiss Med. Wkly. 2013, 143, w13856. [Google Scholar] [CrossRef] [Green Version]
- Crowley, C.P.; Salciccioli, J.D.; Kim, E.Y. The association between ACLS guideline deviations and outcomes from in-hospital cardiac arrest. Resuscitation 2020, 153, 65–70. [Google Scholar] [CrossRef]
- Honarmand, K.; Mepham, C.; Ainsworth, C.; Khalid, Z. Adherence to advanced cardiovascular life support (ACLS) guidelines during in-hospital cardiac arrest is associated with improved outcomes. Resuscitation 2018, 129, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Aw, S.J.; Cheong, M.A.; Chew, J.; Ler, A.C.; Yong, L.P.; Chan, Y.H.; Win, M.T.M.; Suppiah, N. A randomised control trial to compare retention rates of two cardiopulmonary resuscitation instruction methods in the novice. Resuscitation 2016, 103, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Wik, L.; Hansen, T.B.; Fylling, F.; Steen, T.; Vaagenes, P.; Auestad, B.H.; Steen, P.A. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out-of-hospital ventricular fibrillation: A randomized trial. JAMA 2003, 289, 1389–1395. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.; Kessler, D.; Mackinnon, R.; Chang, T.P.; Nadkarni, V.M.; Hunt, E.A.; Duval-Arnould, J.; Lin, Y.; Cook, D.A.; Pusic, M.; et al. For the International Network for Simulation-based Pediatric Innovation, R. a. E. I. R. G. I. Reporting Guidelines for Health Care Simulation Research: Extensions to the CONSORT and STROBE Statements. Simul. Healthc. 2016, 11, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Christenson, J.; Andrusiek, D.; Everson-Stewart, S.; Kudenchuk, P.; Hostler, D.; Powell, J.; Callaway, C.W.; Bishop, D.; Vaillancourt, C.; Davis, D.; et al. The Resuscitation Outcomes Consortium. Chest Compression Fraction Determines Survival in Patients With Out-of-Hospital Ventricular Fibrillation. Circulation 2009, 120, 1241–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledesma, R.D.; Macbeth, G.; Cortada de Kohan, N. Computing Effect Size Measures with ViSta—The Visual Statistics System. Tutor. Quant. Methods Psychol. 2020, 5, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, C.; Iwami, T.; Kawamura, T.; Ando, M.; Yonemoto, N.; Hiraide, A.; Nonogi, H. Effectiveness of simplified chest compression-only CPR training for the general public: A randomized controlled trial. Resuscitation 2008, 79, 90–96. [Google Scholar] [CrossRef]
- Weichert, V.; Sellmann, T.; Wetzchewald, D.; Gasch, B.; Hunziker, S.; Marsch, S. Two minutes CPR versus five cycles CPR prior to reanalysis of the cardiac rhythm: A prospective, randomized simulator-based trial. Resuscitation 2015, 96, 142–147. [Google Scholar] [CrossRef]
- Andersen, L.W.; Granfeldt, A.; Callaway, C.W. Association between tracheal intubation during adult in-hospital cardiac arrest and survival. JAMA 2017, 317, 494–506. [Google Scholar] [CrossRef]
- Benger, J.R.; Kirby, K.; Black, S.; Brett, S.J.; Clout, M.; Lazaroo, M.J.; Nolan, J.P.; Reeves, B.C.; Robinson, M.; Scott, L.J.; et al. Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA 2018, 320, 779–791. [Google Scholar] [CrossRef]
- Wang, H.E.; Schmicker, R.H.; Daya, M.R.; Stephens, S.W.; Idris, A.H.; Carlson, J.N.; Colella, M.R.; Herren, H.; Hansen, M.; Richmond, N.J.; et al. Effect of a Strategy of Initial Laryngeal Tube Insertion vs Endotracheal Intubation on 72-Hour Survival in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2018, 320, 769–778. [Google Scholar] [CrossRef]
- Granfeldt, A.; Avis, S.R.; Nicholson, T.C.; Holmberg, M.J.; Moskowitz, A.; Coker, A.; Berg, K.M.; Parr, M.J.; Donnino, M.W.; Soar, J.; et al. Advanced airway management during adult cardiac arrest: A systematic review. Resuscitation 2019, 139, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Breen, C.J.; Kelly, G.P.; Kernohan, W.G. ECG interpretation skill acquisition: A review of learning, teaching and assessment. J. Electrocardiol. 2019, 18, 30641. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.K.; Cattermole, G.N.; Mak, P.S.K.; Graham, C.A.; Rainer, T.H. Nurse-initiated defibrillation: Are nurses confident enough? Emerg. Med. J. 2012, 29, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, S.; Wakelam, A. Leadership of resuscitation teams: “Lighthouse Leadership”. Resuscitation 1999, 42, 27–45. [Google Scholar] [CrossRef]
- Cooper, S. Developing leaders for advanced life support: Evaluation of a training programme. Resuscitation 2001, 49, 33–38. [Google Scholar] [CrossRef]
- Fernandez, C.E.; Russo, S.G.; Cremer, S.; Strack, M.; Kaminski, L.; Eich, C.; Timmermann, A.; Boos, M. Positive impact of crisis resource management training on no-flow time and team member verbalisations during simulated cardiopulmonary resuscitation: A randomised controlled trial. Resuscitation 2011, 82, 1338–1343. [Google Scholar] [CrossRef]
- Fernandez, C.E.; Russo, S.G.; Riethmuller, M.; Boos, M. Effects of team coordination during cardiopulmonary resuscitation: A systematic review of the literature. J. Crit. Care 2013, 28, 504–521. [Google Scholar] [CrossRef]
- Fernandez, C.E.; Boos, M.; Ringer, C.; Eich, C.; Russo, S.G. Effect of CRM team leader training on team performance and leadership behavior in simulated cardiac arrest scenarios: A prospective, randomized, controlled study. BMC Med. Educ. 2015, 15, 116. [Google Scholar] [CrossRef] [Green Version]
- Hunziker, S.; Buhlmann, C.; Tschan, F.; Balestra, G.; Legeret, C.; Schumacher, C.; Semmer, N.K.; Hunziker, P.; Marsch, S. Brief leadership instructions improve cardiopulmonary resuscitation in a high-fidelity simulation: A randomized controlled trial. Crit. Care Med. 2010, 38, 1086–1091. [Google Scholar] [CrossRef]
- Hunziker, S.; Johansson, A.C.; Tschan, F.; Semmer, N.K.; Rock, L.; Howell, M.D.; Marsch, S. Teamwork and leadership in cardiopulmonary resuscitation. J. Am. Coll. Cardiol. 2011, 57, 2381–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunziker, S.; O’Connell, K.J.; Ranniger, C.; Su, L.; Hochstrasser, S.; Becker, C.; Naef, D.; Carter, E.; Stockwell, D.; Burd, R.S.; et al. Effects of designated leadership and team-size on cardiopulmonary resuscitation: The Basel-Washington SIMulation (BaWaSim) trial. J. Crit. Care 2018, 48, 72–77. [Google Scholar] [CrossRef]
- Bogenstatter, Y.; Tschan, F.; Semmer, N.K.; Spychiger, M.; Breuer, M.; Marsch, S. How accurate is information transmitted to medical professionals joining a medical emergency? A simulator study. Hum. Factors 2009, 51, 115–125. [Google Scholar] [CrossRef]
- Truhlar, A.; Deakin, C.D.; Soar, J.; Khalifa, G.E.; Alfonzo, A.; Bierens, J.J.; Brattebo, G.; Brugger, H.; Dunning, J.; Hunyadi-Anticevic, S.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation 2015, 95, 148–201. [Google Scholar] [CrossRef] [PubMed]
- Maconochie, I.K.; de Caen, A.R.; Aickin, R.; Atkins, D.L.; Biarent, D.; Guerguerian, A.M.; Kleinman, M.E.; Kloeck, D.A.; Meaney, P.A.; Nadkarni, V.M.; et al. Part 6: Pediatric basic life support and pediatric advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2015, 95, e147–e168. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rifai, S.; Sellmann, T.; Wetzchewald, D.; Schwager, H.; Tschan, F.; Russo, S.G.; Marsch, S. Hands-On Times, Adherence to Recommendations and Variance in Execution among Three Different CPR Algorithms: A Prospective Randomized Single-Blind Simulator-Based Trial. Int. J. Environ. Res. Public Health 2020, 17, 7946. https://doi.org/10.3390/ijerph17217946
Rifai S, Sellmann T, Wetzchewald D, Schwager H, Tschan F, Russo SG, Marsch S. Hands-On Times, Adherence to Recommendations and Variance in Execution among Three Different CPR Algorithms: A Prospective Randomized Single-Blind Simulator-Based Trial. International Journal of Environmental Research and Public Health. 2020; 17(21):7946. https://doi.org/10.3390/ijerph17217946
Chicago/Turabian StyleRifai, Sami, Timur Sellmann, Dietmar Wetzchewald, Heidrun Schwager, Franziska Tschan, Sebastian G. Russo, and Stephan Marsch. 2020. "Hands-On Times, Adherence to Recommendations and Variance in Execution among Three Different CPR Algorithms: A Prospective Randomized Single-Blind Simulator-Based Trial" International Journal of Environmental Research and Public Health 17, no. 21: 7946. https://doi.org/10.3390/ijerph17217946
APA StyleRifai, S., Sellmann, T., Wetzchewald, D., Schwager, H., Tschan, F., Russo, S. G., & Marsch, S. (2020). Hands-On Times, Adherence to Recommendations and Variance in Execution among Three Different CPR Algorithms: A Prospective Randomized Single-Blind Simulator-Based Trial. International Journal of Environmental Research and Public Health, 17(21), 7946. https://doi.org/10.3390/ijerph17217946